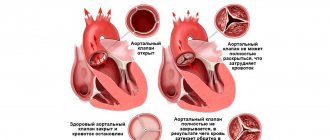
If left untreated, heart defects often lead to serious consequences, including death. The most common disorder is considered to be aortic valve insufficiency, in which the valves do not close completely. According to ICD 10, non-rheumatic lesions have code I35.0 (1,2,8,9). Until recently, his aortic valve replacement was considered a serious operation, and it was performed in exceptional cases. Today, such manipulations are carried out regularly, making life easier for many patients. To minimize the risk of complications and shorten the rehabilitation period, experts give preference to minimally invasive techniques.
Aortic valve and its purpose
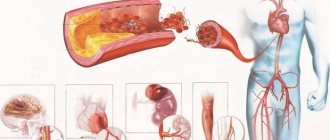
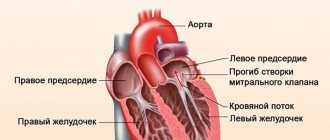
The aortic valve is an element of the internal frame of the heart. It is located on the border of the left ventricle and the largest coronary vessel of the circulatory system, carrying oxygen-enriched blood throughout the body. The design consists of a fibrous ring and three semilunar valves, which swing open when a portion of blood is pushed into the aorta and prevent its return. As a result of this process, the cameras are able to take turns resting.
It is important to know! When the valve fails to cope with its function, hemodynamics are disrupted, which leads to overload of the myocardium and its premature wear. Heart failure causes a slowdown in blood circulation, which causes stagnation that negatively affects the functioning of internal organs and systems.
Carrying out the operation
Once the patient is on the operating table, he is given general anesthesia and falls asleep. If the operation is performed with an opening of the chest, then in the middle the surgeon makes an incision and pushes the chest apart so that the heart can be reached.
Cardiac arrest is required to allow replacement, so the patient is connected to a heart-lung machine. The doctor makes an incision in the aorta, removes the worn or damaged valve and installs a new one in its place. After this, the aorta is sutured, the heart muscle is started, the chest is connected and sutured.
Aortic valve replacement surgery
Doctors talk about replacing the aortic valve when it is no longer able to function properly and there is a risk of circulatory problems. Thanks to innovative technologies, the operation is performed quickly with minimal risks for the patient. A large selection of prostheses allows you to choose the ideal option and prolong human life.
Indications for the procedure and consequences of inaction
Aortic valve dysfunction can occur for many reasons. First of all, this is a congenital defect - the deformation is observed from the moment a person is born. This often happens in adulthood, when, against the background of many years of uninterrupted functioning, incomplete closure of the valves occurs, which increases the load on the heart muscle. In this case, we are talking about an acquired pathology. Indications for surgery:
- Infectious or bacterial endocarditis. Vegetation of microorganisms on valve leaflets and the inner lining of the myocardium.
- Symptoms of heart failure after coronary artery bypass surgery.
- An aortic aneurysm, which is characterized by a bulging sac and leads to deformation of the valve.
- Aortic stenosis. The narrowing prevents the septum from fully opening, which slows down the ejection of blood from the ventricle.
- Degenerative processes. Changes in structure and shape are caused by age-related aging.
Some diseases that are accompanied by characteristic symptoms of cardiovascular failure - shortness of breath, chest pain, and fainting - can also affect the functioning of the valve.
Limitations for the intervention
Mitral valve replacement is not always prescribed by a doctor for existing problems. In some situations there are contraindications to its implementation.
- Myocardial infarction.
- Stroke is an acute disorder of cerebral circulation.
- Infectious diseases in acute form.
- Chronic pathologies during exacerbation (diabetes mellitus, bronchial asthma).
Surgery is contraindicated in severe cases of heart failure, when the question of a heart transplant arises.
Different prostheses and their characteristics
Since the end of the last century, aortic prostheses have undergone significant changes. Valves based on ball joints are considered obsolete. They were replaced by more convenient and modern designs in the form of double-hinged prostheses.
- Mechanical. They are made of hypoallergenic material that is not rejected by the body. They have the shape of a real organ and have a long service life.
- Biological. When there is an increased risk of thrombosis, xenografts made from the pericardium of calves or the heart of pigs, as well as tissue from some other animals, are used to replace the damaged septum.
- Allografts. They are removed from the donor heart and implanted into the patient's muscle.
In rare cases, a dysfunctional valve is replaced with a similar one, which is located in the pulmonary trunk, and a prosthesis is already installed in its place.
Surgical options
Today, replacing the aortic valve without opening the chest is performed quite often, especially with minor injuries. Like replacing the mitral valve of a diseased heart, the operation takes a long time - approximately 5-6 hours. Most often, they try to carry out the procedure using minimally invasive methods, and only in rare cases, in severe cases of the disease, do they resort to open intervention.
- Minithoracotomy. It is performed under general anesthesia. Several small incisions are made below the patient's chest. The aortic valve prosthesis is implanted in the usual way using a heart-lung machine.
- Endovascular method. This type of operation is performed using local anesthesia and X-rays. It involves introducing a microprosthesis using a catheter through small incisions in the brachial artery, but more often in the femoral vessel of the lower limb. It is placed in place, after which the auxiliary tube is brought out through the leg.
- MitraClip. It is translated into Russian as correction of the mitral valve for damage of any complexity. The operation is performed according to the traditional procedure.
It is important to know! The most common option is open heart surgery, which allows you to eliminate the most complex pathologies.
Pre-operation stage
After deciding to undergo surgery, the patient is required to undergo a series of studies, which, in addition to examination by a doctor, include the following procedures.
- A blood test is done for all the necessary indicators.
- An electrocardiogram is performed to determine the heart rhythm.
- An echocardiogram is performed to detect movement of the myocardium and its valves.
- Cardiac catheterization is done: a contrast agent is injected through a thin tube to determine the problem of the functioning of the aortic valve.
If necessary, it is recommended to consult a gynecologist, urologist, dentist, or ENT doctor to rule out infection. Some time before the planned operation, the patient is advised to do the following:
- exclude the use of anticoagulants;
- stop using aspirin and anti-inflammatory drugs;
- on the eve of the appointed date, eat only light meals;
- refrain from eating on the day of the event;
- wear comfortable, loose underwear.
The patient must have with him a passport, insurance policy, SNILS, a referral from the attending physician, and examination results. After all instructions have been followed, the doctor will schedule the surgery.
Technique of the procedure
Open heart surgery is a classic procedure and is performed under general anesthesia. Its progress is determined in several stages.
- A median stenotomy is performed - a large incision in the chest.
- The patient is connected to a heart-lung machine.
- The heart is cooled to slow down its beating.
- The surgeon removes the damaged valve and then installs a prosthesis.
- Stitches are being applied.
- The patient is gradually disconnected from the device.
Due to its prevalence and accessibility, the procedure is considered familiar and relatively uncomplicated. After just a few days, the patient can gradually return to normal life, where the only reminder of the surgery will be the scar.
Possible complications
In rare cases, surgery to replace the mitral and aortic valve can lead to the development of some complications. The most common are thromboembolic. To prevent the formation of blood clots, anticoagulants and antiplatelet agents are prescribed, that is, drugs that prevent rapid blood clotting and promote blood thinning. These include Aspirin, Warfarin, and Heparin injections. In the future, medications should be taken for any surgical treatment or minimally invasive intervention for urogynecological problems, in dentistry.
The development or recurrence of infective endocarditis is considered no less dangerous, and the risk increases several times with the installation of a biological prosthesis. As a preventive and therapeutic measure during the postoperative period, the patient is prescribed a course of antibiotics. The characteristic signs of the beginning process are:
- chills, fever;
- increased body temperature;
- the appearance of symptoms of heart failure due to valve dysfunction.
In rare cases, complications manifest themselves in the form of the following phenomena:
- bleeding after taking anticoagulants;
- growths of scar tissue;
- hemolytic anemia.
Timely detection of these conditions allows for rapid re-operation or other measures to eliminate them.
Recovery period
After the operation, patients are required to stay 5-8 days in a medical institution to undergo cardiac rehabilitation and general recovery of the body, which represents a set of effective measures:
- course of medication;
- physiotherapeutic procedures;
- moderate physical activity for dosed heart training;
- detailed consultation with a specialized doctor regarding lifestyle changes;
- nutritionist recommendations for nutrition correction.
During the postoperative period, a person should try to avoid visiting baths, saunas, and swimming pools.
Features of certain types of operations
Transaortic implantation of the aortic valve with a bioprosthesis is a hybrid minimally invasive surgery. Indications for such intervention are:
- young age of the patient;
- relative contraindications to surgery under artificial circulation;
- dysfunction of external respiration;
- lack of adequate access for transcatheter prosthetics.
- low surgical risk for postoperative complications;
- anatomical features of the aortic root.
Transcatheter TAVI aortic valve implantation is performed through the femoral artery using CoreValve (Medtronic) and SAPIEN ST (Edwards) bioprostheses.
Constant monitoring of the operation on the angiographic monitor screen is necessary. All important parameters are assessed by continuous ultrasound of the heart.
Patients after prosthetics with access through the artery are discharged for 2–4 days. The operation is performed on patients with the following indicators:
- symmetrical calcified aortic stenosis;
- sufficient area of the aortic mouth;
- the diameter of the aortic valve annulus is less than 16 mm or more than 28 mm;
- sufficient width of the lumen of the common femoral artery;
- severe concomitant pathology that does not allow transthoracic surgical access.
Transcatheter intervention is contraindicated in the following cases:
- Supravalvular aortic stenosis.
- Congenital heart defects.
- Hypertrophic cardiomyopathy.
- The need for concomitant coronary artery bypass grafting.
- Severe deformation of the chest.
- Infectious endocarditis.
- Intracardiac thrombi.
Despite a number of contraindications, transcatheter aortic valve replacement is the latest achievement in cardiac surgery.
This operation allows the implantation of the safest biological grafts, which significantly facilitates the life of patients and their further management.
Transthoracic access with subsequent aortic valve replacement requires long-term hospitalization, rehabilitation and massive drug therapy. Therefore, in recent years there has been a trend towards minimally invasive operations.
Cost of surgical treatment
In most cases, aortic valve replacement surgery is free of charge. This is due to the presence of quotas provided by the Russian healthcare system under the compulsory medical insurance system. But if it is not possible to use such a quota, or for some reason the patient is refused, he has the option of performing the operation at his own expense. Surgical interventions of this kind are considered quite accessible to ordinary citizens and are carried out in all major cities of Russia.
The cost of surgical treatment varies in the range of 90-200 thousand rubles. In Moscow, this figure is slightly different and amounts to 65-600 thousand. Moreover, the increase in price directly depends on the volume and complexity of the manipulations.
The standards for heart valve replacement abroad are much higher, so patients often choose foreign clinics. In different countries, the cost of replacement surgery varies significantly.
| A country | Cost/euro |
| USA | 120000 |
| Israel | 50000 |
| Singapore | 30000 |
| Spain | 24000 |
| Poland | 20000 |
| Türkiye | 10000 |
| Mexico | 9000 |
| India | 4000 |
Taking into account numerous reviews from patients, we can conclude that treatment both abroad and in the Russian Federation is of high quality and is carried out at a decent level.
Types of valves
Even the capabilities of modern science and technology still do not allow us to create an ideal valve. The varieties that are used now have their pros and cons. For replacement, surgeons use several types of prostheses:
- Mechanical valves. They are created from modern high-strength alloys. Their advantage is that they function indefinitely, but the patient will have to take anticoagulants throughout his life to prevent the formation of blood clots.
- Biological prostheses are made from animal valves. After their installation, taking blood thinning drugs is not required, but the life of the prosthesis is only 10-15 years, and then a second operation is required.
- Donor valves are obtained from a deceased person. Such valves also cannot last forever.
When aortic valve replacement is required, the choice of type depends on several factors:
- Age group of patients.
- General health.
- Why does the valve need to be replaced?
- Presence of other chronic diseases.
- Does the patient have the opportunity to take anticoagulants for life?
Once the type of valve has been selected, a complex operation is required to replace it.
Life after valve replacement: reviews, forecasts, recommendations
The prognosis after any type of heart valve replacement surgery is considered favorable. The risk of disability and mortality from heart failure is significantly reduced, and life expectancy, on the contrary, increases significantly.
Attention! The fatal outcome of the operation is 0.2%, and it is almost always associated with the formation of blood clots or the development of infective endocarditis.
After replacing the valve, the patient is asked to radically change his living conditions. During the first year after the operation, he must visit the doctor monthly, in the second year much less - once every six months. At all other times, you need to contact a specialist for an examination at least once a year. It is recommended to undergo an ECG and EchoCG at each visit.
Regardless of the period that has passed since the operation, it is recommended to follow simple rules for the rest of your life.
- Avoid drinking strong drinks, including coffee.
- Get rid of bad habits.
- Adjust your diet and follow a gentle diet.
- Periodically take vitamin and mineral complexes to maintain their optimal balance in the body.
It is necessary to create a correct daily routine: allocate no more than 8 hours for work, no less than the specified period for rest and sleep. Divide the rest of the time between meals, walking in the fresh air and doing therapeutic exercises, which are aimed at strengthening the heart muscle.
According to reviews of patients who underwent aortic or mitral valve replacement, most of them returned to their previous lifestyle. The discomfort disappeared, the heart function was completely restored. Many women with pathology of the heart frame were able to find the happiness of motherhood after surgery.
results
In the early postoperative period, 4 (4.7%) patients died in the BioPr group, and 1 (1.1%) in the MehPr group. The cause of mortality was multiple organ failure (2 from the BioPr group) and heart failure (2 - BioPr; 1 - MechPr).
Long-term survival
The average follow-up period was 57.0±6.0 months (from 1.8 years to 9 years). In the long-term period, 66 (89%) patients were observed in the BioPr group, and 72 (84%) in the MehPr group. Long-term survival by the 9th year was not statistically different in both groups and was 88% in the BioPr group and 95% in the MechPr group (Fig. 2). In the BioPr group, 5 (6.3%) patients died: from stroke - 1, progression of CHF - 2, oncology - 1; from an unknown cause - 1; in the MechPr group - 2 (2%): from pulmonary embolism - 1, progressive heart failure - 1.
Rice. 2. Long-term survival.
Reoperations
In the BioPr group, freedom from reoperations by the 9th year was 98%, in the MehPr group - 99% ( p
<0.05). 4 years after the operation, 1 patient with the Carpentier-Edwards Perimount Magna 19 biological prosthesis required re-intervention due to the development of infective endocarditis. The prosthesis was replaced with a biological one of the same diameter. A year after surgery, a patient with a mechanical prosthesis Carbonics 20 developed thrombosis of the prosthesis (the Carbomedics-21 prosthesis was re-implanted).
Thromboembolism and bleeding
There were no episodes of “massive” bleeding in either group. The number of thromboembolisms in the BioPr group was 2 (2.5%), in the MechPr group - 1 (1.1%) ( p
<0,05).
Hemodynamic parameters
In the long-term period, a significantly significant decrease in peak and average gradients and regression of myocardial mass were observed in both groups (see Table 2). According to echocardiography, in the BioPr group the peak and average gradients were 27.0±11.0 and 14.0±8.0 mmHg (in the early postoperative period 23.0±8.0 and 12.0±4 .0, respectively), in the MechPr group - 27.0±9.0 and 13.5±5.0 mmHg. (in the early period 28.3±9.0 and 15.2±7.0 mmHg, respectively) ( p
<0.05) (Fig. 3).
Myocardial mass index (MMI) in the BioPr group was 104.0±35.0 g/m², in the MechPr group - 98.0±21.0 g/m² ( p
<0.05) (see Table 2). High transprosthetic gradients (∆Pmax >40 mmHg, ∆Pav. >20 mmHg) were noted in 4 patients from the BioPr group and 2 from the MechPr group. Despite the high gradients, half of the patients showed a decrease in IMM in the long-term period: 2 patients with Carpentier-Edwards Perimount biological prostheses and 1 with a Carbonix-20 mechanical prosthesis. The worst results were observed in patients with Mitroflow prostheses, in whom the highest transprosthetic gradients and increased myocardial hypertrophy were observed.
Rice. 3. Dynamics of transprosthetic gradients in the long-term period.
Postoperative period
For several days after valve replacement surgery, patients receive painkiller injections to reduce pain. But after a while they are canceled. In addition, the patient may encounter the following problems:
- Swelling of the limbs.
- Pain in the incision area.
- Inflammatory process in the place where the incision was made.
- Nausea.
- Attachment of infection.
If all these manifestations continue for too long, then you should tell your doctor. Surgeries to replace the aortic valve (patient reviews indicate this) bring noticeable improvements within a couple of weeks. Significant positive changes occur within a few months.
After the operation, doctors recommend observing a work-rest schedule and strictly dosing physical activity.
It is best if the patient spends the recovery period not at home, but in a specialized institution, for example, in a sanatorium or in a cardiac rehabilitation center.
There, under the supervision of doctors, the body is being restored, and an individual program is selected for everyone. Rehabilitation may take varying lengths of time. It all depends on the general condition of the patient, the complexity of the operation and the body’s recovery abilities.
The doctor must prescribe medications to the patient after surgery. They must be taken strictly according to the scheme and cannot be canceled independently.
If various physiotherapeutic procedures or medical interventions are required, then you should definitely inform that there is an artificial aortic valve.
If there are concomitant heart diseases, valve replacement will not cure them, so it is necessary to visit a cardiologist and carry out appropriate therapy.
Complications after surgery
For any surgeon, not only the operation process itself and its outcome are important, but also the recovery period, which can also be accompanied by serious complications:
- Proliferation of scar tissue. There are cases when, after surgery, fibrous scar tissue quickly grows at the site of valve replacement in a patient. This process does not even depend on the type of valve and can lead to thrombosis. But thanks to modern surgical techniques, this complication is quite rare.
- Bleeding while taking anticoagulants. Moreover, it can occur not only in the valve area, but also in any organ, for example, in the stomach.
- Thromboembolism. It can be recognized by the following manifestations:
- The patient experiences shortness of breath.
- Blurred consciousness.
- Vision and hearing are lost.
- Numbness and weakness in the body.
- Dizziness.
4. Infection of the supplied valve. Even the most sterile valve, once inside, can become infected. That is why, if your body temperature suddenly rises or respiratory problems appear, you should urgently inform your doctor in order to conduct tests and rule out infection of the valve.
5. Hemolytic anemia. When it occurs, a large number of red blood cells are damaged during contact with the valve material. Severe weakness and fatigue appear that does not go away after rest.
As a rule, if there is a heart defect, the patient has one or another disability group. All this is determined by a special commission of doctors. If the aortic valve has been replaced, disability can be lifted if the council of doctors considers that you are healthy and you do not require special payments from the state. In some cases, group 3 is left.
Methods for correcting heart valves
For the heart to function successfully, all four valves of the human heart (tricuspid, pulmonary valve, mitral valve, aortic valve) must flawlessly perform their functions as conductors of circulating blood.
If the valve is only partially damaged, it is possible that your doctor may be able to prescribe drug therapy without the need for surgery. If the damage is severe, surgery may be required to correct or replace the valve.
Valve repair is commonly performed for congenital valve defects and has a good treatment success rate.
Commissurotomy is a method that is used for a narrowed valve. This occurs when its valves thicken and possibly peck. In case of such damage, the surgeon opens the valve, eliminating the bonding area.
Valvuloplasty – strengthening of the valve leaflets to achieve its tight closure. It is performed using special ring-shaped devices that the surgeon places around the external opening of the valve.
Changing the shape of the valve - with this procedure, part of the valve leaflet is resected. The surgeon then performs proper suturing of the leaflet, causing the valve to close properly.
Decalcification is the removal of calcium buildup from the leaflets, making the valve close tightly.
Correction of chordae tendineae and papillary muscles – the correct length of chordae and muscles is restored, at which the valve closes properly.