Description of the pathology
Depending on the specifics of the pathology, aortic heart defects in ICD-10 are designated by codes I35.0-I35.9. This pathology is the most common heart defect and consists of a violation of the process of closure of the aortic valve. The pathology is associated with a disruption of the normal anatomical structure of the valve located between the left ventricle and the aorta.
The function of the valve is to remove oxygenated arterial blood into the aorta. Accordingly, disruption of the functioning of this structure leads to changes in the systemic circulation, as a result of which a number of complications develop from the cardiovascular system, negatively affecting the functioning of the entire body.
Regardless of the type and causes of aortic heart disease, the disease must be diagnosed in a timely manner. Therapy in the early stages is based on taking medications that prevent the development of hypertrophy of the heart chambers, which occurs against the background of progressive heart failure. In advanced cases, valve replacement (prosthetics) is practiced.
Aortic (valvular) stenosis code according to ICD 10 2020
Valvular defects never develop primarily. The causes of acquired heart defects are usually rheumatism (the main cause, the most common), infective endocarditis, syphilis and atherosclerosis. Damage to the valve begins with the deposition of specific structures on it: a cholesterol plaque, a bacterial colony or auto-antibodies, which have a direct damaging effect on it.
The result of destruction is deposits of calcium and connective fibers (fibrosis), as a result of which the valve loses its elasticity and correct configuration - its folds decrease and shift. This leads to a gradual loss of its function and disruption of the heart.
Usually this disease affects the mitral valve, the others (tricuspid, aortic and pulmonary valve) are affected less frequently. Most common
rheumatic heart defects
.
Prevention of PPS:
- Cholesterol level control;
- Elimination of harmful occupational factors;
- Mandatory treatment of streptococcal infection to avoid rheumatism;
- Therapy of chronic diseases;
- Hardening;
- Registration with a cardiologist in the presence of any heart disease.
Classification
| Localization | View | Incidence of cases per 100,000 population |
| Mitral valve disease | Stenosis | 1500 |
| Failure | 400 | |
| Aortic valve disease | Stenosis | 2000 |
| Failure | 1000 | |
| Tricuspid valve | Stenosis | 300 |
| Failure | 400 | |
| Pulmonary valve | Stenosis | 200 |
| Failure | 300 | |
| Combined defects | Stenosis of 2 or 3 valves | 25-30 |
| Insufficiency of 2 or 3 valves | Isolated cases | |
| Combination of stenosis and insufficiency of 2 or 3 valves | ||
| Combination of stenosis and insufficiency in 1 valve | 400-1000 |
Non-rheumatic defects (codes for the rest are below in the description):
- Mitral: I34.0, I34.1, I34.2.
- Aortic: I35.0, I35.1, I35.2.
- Tricuspid: I36.0, I36.1, I36.2.
- Non-rheumatic lesions of the pulmonary valve: I37.0, I37.1, I37.2.
Description of common defects:
- Mitral insufficiency (I05.1). It is characterized by inadequate closure of the bicuspid valve, resulting in the return of blood to the left atrium. A blue defect with excessive blood supply to the lungs, manifested by blueness of the skin, increased breathing and rapid exhaustion.
- Mitral stenosis (I05.0). The defect is represented by a decrease in the mitral orifice, as a result of which insufficient blood flows into the left ventricle. The atrium experiences increased pressure and hypertrophies. Blue defect with enrichment of pulmonary blood supply, manifested by cyanosis, shortness of breath, dizziness.
- Aortic insufficiency (I06.1). A defect caused by a loose connection of the semilunar aortic folds, due to which, at the time of diastole, blood moves back into the left ventricle, causing its overflow and hypertrophy. White defect with depletion of blood supply to internal organs, arterial hypertension, chilliness.
- Aortic stenosis (I06.0). Represented by narrowing of the aortic opening. The lesion is manifested by insufficient blood flow into the aorta during systole, which leads to left ventricular hypertrophy. White defect with depletion of the large circle, hypertension, chilliness, physical weakness.
- Triscupidal insufficiency (I07.1). It manifests itself as incomplete or untimely connection of the leaflets of the right atrioventricular valve, resulting in the reflux of blood into the right atrium. Blue defect, manifested by blueness of the skin, swelling of the legs, swelling of the neck veins, and weakness.
- Triscupidal stenosis (I07.0). It is represented by narrowing of the tricuspid ring and poor blood supply to the right ventricle at the moment of cardiac relaxation. Blue defect with insufficient blood supply to the lungs, shortness of breath, enlarged liver.
- Pulmonary valve insufficiency (I37.1). The defect is caused by incomplete connection of the valve leaflets between the right ventricle and the pulmonary artery, as a result of which the blood partially returns to the ventricle, causing its hypertrophy. Blue defect with depletion of pulmonary blood supply, shortness of breath, cyanosis, fainting.
- Pulmonary valve stenosis (I37.0). The lesion consists of a narrowed opening of the pulmonary valve, resulting in insufficient blood flowing into the lungs. Blue defect, accompanied by right ventricular hypertrophy, cerebral hypoxia, edema, and enlarged liver.
It is an irreversible form of pulmonary hypertension acquired due to a congenital cardiac abnormality. It is a combination of a ventricular septal defect, right ventricular hypertrophy and reverse aortic position.
Eisenmeiger syndrome manifests itself with pulmonary edema and cyanosis in adulthood in unoperated individuals with pronounced right-to-left shunting.
General symptoms
At an early stage of the disease, symptoms may be minor or absent altogether, so the patient does not take them into account. Here is a list of the first signs of cardiac muscle dysfunction:
- heartbeat becomes rapid;
- a dry cough appears;
- the voice becomes hoarse;
- shortness of breath bothers you;
- pain and feeling of fullness in the chest;
- the patient may cough up blood;
- loss of consciousness;
- dizziness;
- a blush may appear on the cheeks;
- swelling of the legs.
PPS rarely reveal themselves at the initial stage. Vivid symptoms appear already during the period of active development of the disease, so you should undergo examination at the first signs of disruption of the heart muscle.
Acquired defects in children
- Questioning: history of previous infectious disease or atherosclerosis, complaints of weakness and fatigue, interruptions in heart function, shortness of breath, fainting.
- Examination: cyanosis (blue blemishes) or pallor (white blemishes) of the skin; visible pulsation and swelling of the neck veins, rapid breathing, swelling of the legs, cold skin.
- Measurement of pressure, pulse and respiratory rate: indicators can be either altered or within normal limits.
- Palpation: displaced apical impulse, presence of cardiac impulse, dense swelling of the legs.
- Percussion: increase in cardiac and hepatic boundaries.
- Auscultation: detection of heart murmurs, additional 3rd and 4th sounds, “ri”, specific murmurs (systolic, diastolic, mixed).
- Laboratory data: anemia, increased levels of alkaline phosphatase, aminotransferases, cholesterol, sugar.
- ECG: arrhythmias, blockades, prolongation of repolarization (change in T wave), non-simultaneous excitation of the cardiac chambers (bifurcated and widened P and R waves).
- X-ray: enlargement of the atria or ventricles, depletion of the pulmonary pattern, displacement of the vascular bundle and dome of the diaphragm.
- Echocardiography: location, type and degree of valve displacement.
- Dopplerography: recording the strength and magnitude of reverse blood flow.
- Probing, CT and MRI help confirm the diagnosis in controversial cases.
PPS can develop at any age. In children, pathology occurs much less frequently (in 0.5% of cases), since primary diseases are more typical for the adult population.
The clinical manifestations of the acquired defect in a child are the same as in adults (shortness of breath, blue or pale skin, swollen veins, arrhythmia, enlarged liver), but they appear more clearly and are accompanied by crying, refusal to eat, rapid weight loss, and dystrophy.
Detection of the disease occurs faster (more often - in the first year of the disease, while in adults - in 2-4 years).
The leading diagnostic methods for children are ECG, radiography and ultrasound of the heart.
Is treatment always necessary?
PPPs can be compensated, subcompensated and decompensated.
The compensated form is slightly expressed, and therefore treatment of acquired heart disease is limited to taking medications. Subcompensation requires mandatory surgical treatment, and decompensation, as a rule, inevitably causes death (patients need palliative therapy).
Cases when treatment is not required are extremely rare, since all valve defects are characterized by a steadily progressive course.
Types of surgical interventions:
- Commissurotomy - dissection of adhesions between the valves;
- Balloon valvuloplasty – expansion of the valve using a pressurized balloon;
- Prosthetics – complete valve replacement.
Types of operations depending on the location of the lesion:
- Mitral stenosis – prosthetics, commissurotomy, valvuloplasty.
- Mitral insufficiency – valvuloplasty, prosthetics.
- Aortic defects - installation of a prosthesis.
- Tricuspid stenosis – commissurotomy, valvuloplasty, prosthetics.
- Tricuspid insufficiency – valvuloplasty and prosthetics.
- Pulmonary artery defects – prosthetics.
Forecast
The prognosis without treatment is unfavorable. The disease inevitably leads to heart failure, and acute decompensation leads to the death of the patient. Working capacity is significantly reduced, even to the point of loss.
After treatment, the patient must adhere to the following rules:
- taking medications regularly;
- adherence to diet and regimen;
- maintaining normal weight;
- absence of bad habits;
- exclusion of all harmful foods from the diet;
- frequent walks;
- constant monitoring by the attending physician.
Kinds
The disease is more often diagnosed in elderly patients
Aortic heart disease is quite common. In addition to congenital pathology, older people also face aortic disease. The frequency of occurrence among patients over 80 years of age is more than 15% of all types of cardiac pathologies.
One of the types of congenital pathology is the bicuspid valve (normally it has 3 leaflets). This disorder is a developmental anomaly and is accompanied by valve stenosis.
There are three types of pathology:
- stenosis;
- aortic insufficiency;
- combined aortic disease.
Each type has a number of features that you need to become familiar with.
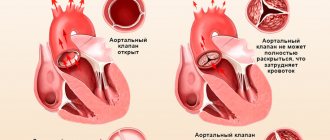
Aortic stenosis
Aortic stenosis, like other heart defects, can be a congenital or acquired pathology. The term “stenosis” refers to a narrowing of the aortic mouth, which leads to poor circulation.
Associated disorders:
- bicuspid valve;
- valve calcification;
- fusion of valve leaflets.
Due to the narrowing of the aortic valve, the process of pushing blood out of the left ventricle is disrupted. As a result, compensatory mechanisms are launched and the pressure inside the valve increases, which entails ventricular hypertrophy. This occurs due to the fact that blood cannot penetrate into the aorta in full due to significant narrowing of the valve, so some of it stagnates in the ventricle, provoking hypertrophy.
Aortic stenosis is characterized by slow progression. On the one hand, thanks to this, the pathology is successfully treated with medication in the initial stages, but on the other hand, the symptoms are very mild and stenosis is difficult to diagnose in a timely manner. The main symptom is impaired cardiac output and changes in systolic pressure.
Aortic heart valve stenosis has ICD-10 code I35.0.
The aortic orifice in a healthy person measures about 2.5 sq. cm. With stenosis, it narrows to 1.5 - 2 sq. cm (1st degree), 1-1.5 sq. cm. cm (2nd degree), and less than 1 sq. cm (3rd degree). The smaller the size of the orifice, the more severe the degree of the disease and the more impaired the functioning of the heart. If with grade 1 stenosis there is a slight disturbance in cardiac output, then grade 3 is diagnosed with severe left ventricular hypertrophy. The effectiveness of drug treatment for aortic heart disease directly depends on the degree of stenosis.
Aortic insufficiency
At an early stage, the disease does not manifest itself in any way, the person is not in pain or bothered by anything
Code I35.1 in ICD-10 indicates aortic valve insufficiency. This pathology is characterized by the return of blood to the left ventricle due to impaired closure of the valve leaflets. Aortic insufficiency is incomplete closure of the valves and a decrease in stroke volume of the heart. The direct consequence of this disease is cardiac ischemia. This is explained by the expansion of the left ventricle and an increase in myocardial oxygen demand. The disease is accompanied by stagnation of blood in the left ventricle.
Like stenosis, it has several stages:
- mild (grade 1) – no more than 15% of the blood is thrown from the aorta into the heart;
- moderate (grade 2) – 15-25% of the blood returns back;
- medium (grade 3) – 25-50% of the blood comes back;
- severe (grade 4) – reflux accounts for more than half of all blood.
As in the case of stenosis, the mild form goes unnoticed by the patient, since it does not have specific symptoms, but it is the one that is most amenable to treatment. The disease can be diagnosed by an increase in the shadow of the heart on an x-ray.
Combined aortic disease
Combined aortic heart disease is a pathology that is simultaneously accompanied by changes characteristic of stenosis and aortic insufficiency. As a rule, this is a disease of rheumatic origin.
With combined aortic heart disease, left ventricular hypertrophy quickly develops and venous blood stagnation is observed.
Note! Acquired combined aortic heart disease is more often diagnosed in men rather than women.
This pathology can also be congenital or acquired. It manifests itself as severe shortness of breath and swelling, and is quite easily diagnosed. Combined aortic heart disease is manifested by two characteristic disorders:
- during systole (contraction of the ventricles), not all the blood enters the aorta;
- During diastole, some of the blood returns to the ventricle (in addition to that which did not enter the aorta).
Such aortic valve defects are the most severe. Moreover, in most cases, either stenosis or aortic insufficiency predominates. Thus, the degrees of these disorders may differ significantly (for example, severe stenosis and moderate failure).
What it is?
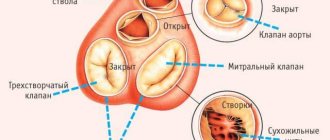
Aortic heart disease is usually understood as a congenital or acquired change in the normal anatomical structure of the aortic heart valve, which is located at the border of the left ventricle and the aorta.
This is a tricuspid valve, the main task of which is to carry out a portioned release of oxygenated arterial blood into the aorta. The functioning of the systemic circulation, the same one that supplies all the internal organs of a person, largely depends on its coordinated work.
There are two main types of aortic valve defects:
- The valve leaflets, which normally close tightly after each pumping of blood from the ventricle into the aorta, for various reasons, cease to close tightly with each other.
As a result, part of the blood intended to enter the aorta is returned back to the left ventricle, which becomes overfilled and begins to stretch, enlarge and act under overload.
- Due to organic damage, valve the doors lose their elasticity and stop opening completely. In this case, the lumen of the valve, which is normally an opening with an area of about 3 cm2 in an adult, decreases.
As a result, the throughput of such a valve also becomes smaller: not all the blood from the ventricle enters the aorta, some of it simply does not have time to get there during the cardiac impulse and remains in the ventricle.The result is gradual stretching and hypertrophy of the left ventricle and heart failure. Narrowing of the aortic valve or stenosis is another type of heart defect.
If this happens for quite a long time, left ventricular failure occurs. This condition of loose closure of the valve leaflets is called aortic valve insufficiency.
Frequency of occurrence
Prevalence of aortic stenosis (AS):
- From 3 to 7%;
- The increase in the amount increases with age up to 20% (in patients over 80 years of age);
- In the young age group, men are more susceptible – 2.4:1.
The incidence of other aortic valve defects is much lower.
ICD-10 codes
- I35.0 AC stenosis
- I35.1 AC insufficiency
- I35.2 Combined aortic heart disease - stenosis and insufficiency
- I35.8 Other AK lesions
- I35.9 AK lesion, unspecified
What does degenerative disease mean?
This type of valve defect is characterized by the presence of inflammation, lipid deposition and valve calcification. Unlike congenital or rheumatic APS, a more rapid progression may occur . Therefore, all cases of mild and moderate aortic stenosis are observed by cardiologists.
It is also necessary to pay attention to the presence of shortness of breath, attacks of angina (“angina pectoris”) and fainting during physical exertion.
Is it congenital?
The most common congenital pathology is aortic stenosis. It accounts for 6% of all cases of congenital heart defects.
Since the stenosis progresses slowly and the clinical picture is not pronounced, its diagnosis may be delayed. However, all children undergo echocardiography to exclude APS . And already at this planned event, if the degree of severity is sufficient, a defect of the aortic mouth can be diagnosed.
Bicuspid aortic valve
A bicuspid valve is a congenital type of AV insufficiency in which it has only two cusps. About 1-2% of the world's population have a bicuspid valve; in newborns it occurs on average in 20 cases out of 1000. BAV often causes the development of aortic stenosis : in children with AS, in 70-85% of cases the valve has only 2 leaflets.
With this diagnosis, doctors try to use valve-sparing operations, because Prosthetics in childhood are undesirable.
Causes of pathology
Medicines can have side effects on the unborn child's body
The cause of congenital concomitant heart disease is an intrauterine disorder in the formation of the aorta, as a result of which the valve has only two leaflets instead of three.
Among the probable causes of intrauterine development disorders:
- intrauterine infections;
- mother's bad habits;
- the effect of medications taken by a pregnant woman;
- living in regions with poor ecology, etc.
Congenital aortic valve insufficiency is a heart defect that can go undetected for years. Aortic stenosis or valve narrowing and aortic insufficiency are defects with slow progression. As a rule, pathology first makes itself felt during a period of rapid growth of the body - in adolescence. However, the symptoms in this case are so mild that they do not pose a danger. People with congenital aortic disease encounter serious manifestations of pathology at a later age. A predisposing factor for the rapid progression of the disease may be secondary pathologies of the cardiovascular system or complications of other diseases.
Acquired heart disease can be a complication of the following diseases:
- syphilis;
- lupus erythematosus;
- endocarditis;
- rheumatism;
- atherosclerosis of the aorta;
- hypertonic disease.
In addition to syphilis, other serious infectious diseases can provoke disruption of the myocardium. Often, heart disease is a complication of severe influenza, usually suffered in old age.
Few people know that chronic tonsillitis can affect cardiac dysfunction, but advanced disease of the tonsils is one of the most common causes of aortic disease in young and middle-aged people.
Heart defects are the most dangerous complications of autoimmune diseases such as lupus and rheumatoid arthritis. Chronic inflammatory processes can spread to the heart, causing endocarditis, which leads to disruption of the aortic valve.
Another cause of the development of pathology is arterial hypertension (hypertension). This pathology is accompanied by high blood pressure, and can also occur in children. This disease results in cardiac complications such as aortic valve stenosis and left ventricular hypertrophy.
A heart defect can be the result of a chest injury that ruptures a valve leaflet. This happens with strong impacts, for example, due to an accident. A feature of aortic disease in this case is the rapid increase in symptoms.
Causes
Etiology • Rheumatism, including cases of secondary infective endocarditis (46.5%) • Medionecrosis (18%) • Primary infective endocarditis (12.8%) • Congenital anomalies (flapping cusp syndrome, isolated aortic valve insufficiency, annulo-aortic ectasia , abnormalities in the number of aortic valve cusps), including cases of secondary infective endocarditis - 13.5% • Syphilis (2.1%) • Aortitis in Reiter's disease, ankylosing spondylitis, rheumatoid arthritis (2.1%) • Connective tissue diseases, such as syndrome Marfana et al. (1.9%) • Traumatic and spontaneous rupture of aortic valves (1.3%) • Atherosclerosis (0.9%) • Arterial hypertension (0.9%).
Pathophysiology • Hemodynamic disturbances are caused by regurgitation of blood from the aorta into the left ventricle during diastole. The volume of regurgitation depends on the area of the defect, the magnitude of the diastolic pressure gradient between the aorta and the left ventricle, the duration of diastole • An increase in the diastolic volume of the left ventricle leads to its tonogenic dilatation • According to the Frank-Starling law, the left ventricle ejects an increased volume of blood into the aorta, which, together with regurgitation, leads to a decrease in diastolic blood pressure, an increase in systolic and pulse blood pressure • As myogenic dilatation develops, the end-diastolic volume and end-diastolic pressure of the left ventricle increase, which leads to stagnation of blood in the pulmonary circulation • Congestion in the pulmonary circulation increases with the development of relative insufficiency mitral valve due to dilatation of the left ventricle • Compensation mechanisms: decreased peripheral vascular resistance, tachycardia, left ventricular hypertrophy.
Symptoms of aortic disease
If a person repeatedly loses consciousness, this may be a sign of a heart defect.
The left ventricle is the largest and strongest part of the heart with excellent compensatory abilities. Because of this, aortic defects do not make themselves felt for a very long time, since the heart tries to cope with the disorder “on its own,” due to hypertrophy and stretching of the walls of the left ventricle. Symptoms appear only when the walls of the ventricle are severely overstretched. Valvular heart disease, aortic valve insufficiency and stenosis have the following symptoms:
- a feeling of pressure and fullness in the heart area;
- pain in the left side of the chest;
- dizziness and weakness;
- frequent fainting;
- swelling of the lower extremities;
- dyspnea;
- change in heart rate;
- change in blood pressure.
Heart rhythm disturbances depend on the type of disease. With aortic insufficiency, tachycardia is observed, which is manifested by a rapid pulse. This is due to the fact that the heart has to beat faster to quickly remove excess blood from the left ventricle. But with stenosis, the rhythm slows down and bradycardia is observed. Changes in rhythm are accompanied by pallor of the skin, a feeling of blood pulsation in large veins (characteristic of tachycardia), weakness and spots before the eyes (bradycardia).
A characteristic symptom of aortic heart defects is a change in pulse pressure - the difference between diastolic and systolic values. Normally this value is 35-40. A decrease in pulse pressure to 25 or below, or an increase in the difference between the upper and lower readings to 50 or more may indicate aortic heart disease.
Short description
Aortic valve insufficiency is a pathological condition characterized by retrograde blood flow from the aorta into the left ventricular cavity through a defective aortic valve.
Code according to the international classification of diseases ICD-10:
- I06.1 Rheumatic aortic valve insufficiency
- I06.2 Rheumatic aortic stenosis with insufficiency
- I35.1 Aortic (valve) insufficiency
- I35.2 Aortic (valvular) stenosis with insufficiency
- Q23.1 Congenital aortic valve insufficiency
Frequency. Among those who died from various heart pathologies, aortic valve insufficiency was detected in 14% of cases, of which in 3.7% - in isolated form, and in 10.3% - in combination with other defects. Since 1999, more than 80% of heart valve surgeries have involved aortic valve replacement.
Diagnostics
To make a diagnosis, you must consult a doctor. Aortic defects are characterized by the appearance of murmurs that are easily audible during a standard examination by a family doctor. Thus, the doctor can make a preliminary diagnosis based on the results of a physical examination and blood pressure measurement. To accurately diagnose the type of heart defect and the degree of pathology, the following is prescribed:
- Ultrasound of the heart;
- chest x-ray;
- ECG;
- MRI.
Additionally, you need to do biochemical and immunological blood tests, since these examinations can exclude or confirm the autoimmune and infectious nature of myocardial dysfunction.
Treatment
You can’t lift weights: neither in the gym nor at home.
People live with aortic heart disease for decades, but without timely and adequate drug therapy, the chance of rapid development of complications increases. Therapy is symptomatic, prescribed on an individual basis, depending on which symptoms predominate.
The following drugs can be used for treatment:
- Calcium antagonists. Used in cases of vascular calcification. These drugs prevent the penetration of calcium ions into the myocardium, reduce the heart's need for oxygen, and reduce afterload. They have an antiarrhythmic effect.
- Beta blockers. Medicines for hypertension are used in cases where aortic valve disease is caused by increased vascular tone. These medications suppress the excess release of adrenaline.
- Angiotensin-converting enzyme inhibitors. They reduce blood pressure, dilate arteries, eliminating spasm, and normalize coronary blood flow. For patients with heart disease, in whom pathologies of the aortic valve are not accompanied by an increase in blood pressure, drugs of this group are prescribed in minimal doses. In this case, there is a decrease in myocardial oxygen demand and normalization of coronary circulation without a significant effect on pressure.
- Diuretics. Diuretics are widely used for heart failure and venous congestion due to aortic disease. Medicines in this group can eliminate swelling of the lower extremities.
The drugs are prescribed without fail, but each patient is given an individual treatment regimen. However, drug treatment is ineffective without radical lifestyle changes. A patient with aortic disease, both congenital and acquired, must:
- maintain a daily routine;
- do not overexert yourself;
- Healthy food;
- limit salt intake;
- normalize the drinking regime;
- exclude physical activity.
Aortic heart disease and bad habits are mutually exclusive concepts. If a violation is detected, you should immediately stop smoking and drinking alcohol.
Treatment tactics
An important factor when choosing treatment tactics is the stage of the defect and the degree of heart failure. Conservative treatment is mostly used as symptomatic therapy. The main method of treatment remains surgical replacement of the aortic valve.
Conservative
The main principles in therapeutic treatment are a diet that limits the consumption of table salt and fatty foods, limiting physical activity to avoid worsening defects, as well as drug treatment of heart failure that occurs.
Conservative drug treatment is in demand in the early stages and when preparing the patient for subsequent surgery. The directions of drug therapy are presented in the table.
| Pursued goal | Groups of drugs used |
| Prevention of infectious complications | antibiotics |
| Prevention of relapses of the provocateur-rheumatism | antirheumatic |
| Elimination of characteristic “heart” symptoms in patients for whom surgery is contraindicated | symptomatic therapy with diuretics, nitroglycerin and drugs to lower blood pressure |
| Normalization of heart rate | antiarrhythmic |
| Prevention of progression of valve narrowing due to atherosclerosis | statins |
| Treatment of chronic heart failure | vasodilators |
With the help of conservative treatment, it is possible to maintain a state of compensation and subcompensation of AC defects for a long time . Complete cure can only be achieved with aortic valve replacement.
The gold standard for the treatment of aortic valve disease in most cases is radical intervention.
Operation
Indications for surgical treatment of patients with aortic stenosis:
- Severe symptoms;
- Pressure difference - 50 mmHg;
- AK hole area is less than 0.75 square meters. cm;
- Increased brain natriuretic peptide.
Indications for AA deficiency:
- The presence of NAC, which does not depend on LV function;
- Impaired LV function is combined with the absence of clinical symptoms;
- Other AV lesions or coronary artery disease (CHD).
When assessing risk factors and the patient's condition before surgery, an interdisciplinary approach is used, which is important in older people. After all, they have contraindications that are not typical for young people (for example, senile asthenia). Their cognitive function, mobility, dependence on assistance, risk of falls, malnutrition (discrepancy between nutrient intake and requirements), and transplant compatibility are also assessed.
Prevention
To prevent the development of heart disease, you should lead a healthy lifestyle, not have bad habits and exercise. In the case of congenital heart disease, prevention is aimed at preventing the progression of the disease. In this case, it is necessary to follow the doctor’s recommendations, undergo a comprehensive examination every six months, and avoid infectious diseases that can potentially lead to heart complications. If you have a congenital heart defect, bad habits and addictions are unacceptable.
Related Articles
Ebstein's anomaly: causes of development, symptoms and treatment in children and adults
Ventricular septal defect (VSD): classification, treatment and prognosis
Transposition of the great vessels: treatment and prognosis of pathology
Coarctation of the aorta in children: ICD-10 code, causes, symptoms and treatment
Mitral heart disease: causes of pathology and treatment methods
VSD of the hypertensive type: ICD code, symptoms and treatment