The replacement of elastic fibers of the connective tissue of the heart valve apparatus with rough ones is called fibrosis. It occurs under the influence of ischemia, inflammation or age-related changes. The mitral and aortic valves are most often affected. An acquired heart defect with circulatory failure is formed. Treatment requires cardiac surgery.
What happens with fibrosis of the leaflets?
fibrosis of the aortic heart valve
Normally, the leaflets of all four heart valves contain loose connective tissue. Its fibers are ordered, and the nutrition of cellular structures is carried out by the smallest blood vessels from the muscle tissue of the heart. When pathological factors influence the valve, as well as due to age-related characteristics, the connective tissue is replaced by coarser tissue, which is not able to maintain the elasticity and flexibility of the valves. The number of capillaries in the valves decreases, the valve tissue receives less nutrients, and some of the cells simply die off, being replaced by fibrous tissue. In fact, valve fibrosis resembles a scar at the site of exposure to a negative factor on delicate connective tissue. Often the concept of fibrosis is identified with sclerosis, which is also true. But sclerosis is more typical for the heart muscle itself, for example, post-infarction or post-myocardial cardiosclerosis. Although often in the conclusion of echocardioscopy you can read about sclerosis of the aortic root, or sclerosis of the mitral valve leaflets.
As fibrous tissue grows, the function of the valve leaflets becomes impaired. They are no longer able to close tightly when blood is expelled from the ventricle, for example, and then some of the blood “leaks” back into the atrium, gradually overstretching it and leading to further hemodynamic disturbances. Or, conversely, fibrous tissue from the valve ring grows towards the valves, leading to their fusion with each other, which sooner or later will provoke the formation of stenosis (narrowing) of the valve opening.
Symptoms
Grade 1 aortic valve regurgitation can occur in an acute form, and sometimes in a chronic form. Signs of pathology occur more often in the first case. If the disease is of a chronic type, then symptoms appear during periods of exacerbation. It should be noted that with each episode of renewed activity, the severity of the disease increases. Often the disease is not accompanied by symptoms for many years.
Signs:
- Shortness of breath that occurs at complete rest and even during sleep.
- When performing any sports activities accompanied by certain loads, difficulty breathing occurs.
- Heart rate increases.
- Migraine that bothers a person systematically.
- Fever.
- Pain appearing in the sternum area. It is observed rarely, only in 7-8 cases of such violations.
- Loss of body weight.
- Manifestations of anemia.
- Violation of the function of the heart ventricle, its left chamber.
- General weakness.
- Decreased blood pressure levels.
In the chronic course of the disease, the absence of symptoms is recorded, but as soon as an exacerbation of the pathology occurs, signs appear one after another, worsening the person’s well-being.
How is fibrosis different from heart disease?
It must be remembered that the concept of cardiac fibrosis as such is not a diagnosis. That is, these are anatomical and morphological changes that can cause stenosis (in particular, mitral stenosis, aortic stenosis) or valve insufficiency. The last two concepts are precisely diagnoses that require certain additional examination and treatment.
Fibrosis, sclerosis or calcification is just a substrate for the development of a heart defect, and whether a defect will develop or not cannot be predicted in advance. But you can regularly see a doctor, and in case of the slightest signs of a defect or chronic heart failure, receive timely treatment. Here we are talking about the fact that the earlier risk factors for the development of heart disease are identified in a patient, the more often he will perform an ultrasound of the heart, and, accordingly, time will not be lost.
Causes of cardiac fibrosis
the mitral valve is most commonly affected . In second place in frequency is the aortic valve . Infection, inflammation, calcium deposition, congenital features, etc. can lead to the replacement of normal valve tissue with fibrous tissue.
Most often, fibrosis of the heart valves is caused by the following conditions and diseases:
- Age-related changes in valve leaflets. Thus, in patients over 60 years of age, due to age-related changes in collagen and elastic fibers, the number of vessels feeding the latter decreases. As a result, the fibers in the heart valves acquire a coarse fibrous structure, which affects the function of the valves.
- Previous acute rheumatic fever, especially with repeated attacks (previously called rheumatism). When the valve is affected by bacteria (usually streptococci, hemolytic, viridans, etc.), infective endocarditis develops with an inflammatory process on the valves. When the valve is influenced by antibodies to this group of bacteria (usually GABHS - group A beta-hemolytic streptococcus), an inflammatory process on the valve is also formed, but of an autoimmune nature. People most often affected by rheumatism are those who often suffer from sore throats, tonsillitis, caries, chronic diseases of the ENT organs and those who have had scarlet fever. Infective endocarditis also develops in this category of patients, but it is more common in injection drug users.
rheumatic vegetations on the mitral valve
- Congenital features, for example, connective tissue dysplasia, Marfan syndrome, mitral valve prolapse. With these anomalies, initially the connective tissue in other organs differs from normal, and often leads to loss of function by the organ. For example, with Marfan syndrome, there is a disturbance in the anatomical and functional structure of other internal organs, including the heart. Mitral valve prolapse causes the leaflets to “sag” into the lumen of the heart chamber, and if linear fibrosis develops on such leaflets, the patient is likely to experience disturbances in intracardiac hemodynamics.
- Atherosclerosis of the aorta. The deposition of cholesterol plaques, in addition to harm to the coronary arteries and, in connection with this, a high risk of myocardial infarction, poses another danger. This is a lesion of the aortic root with subsequent deposition of calcium in the plaque. In addition to the wall of the aorta itself, its valves are affected, and aortic fibrosis develops.
- Previous myocardial infarction and acute inflammation of the heart muscle (myocarditis). Necrosis (cell death) or inflammation near the valve ring leads to the proliferation of sclerotic tissue in place of dead cardiomyocytes - a “scar on the heart” is formed. If in place of this tissue there were tiny vessels feeding the valve leaflets, naturally, they can no longer perform their function. Due to chronic hypoxia, fibrous tissue forms directly in the valve leaflets.
Treatment
Fibrous changes affecting organ tissue are an irreversible process. Therefore, it is necessary to treat the underlying pathology.
In extreme cases, if diagnostics and a high-quality examination are not carried out in time, there is a need to turn to surgical methods of treatment, including valve replacement.
If the disease is not treated over several years, heart failure develops over time, threatening the person’s life. The most effective methods of treatment are drugs that affect the restoration of heart rhythm and restore functions in heart failure.
The treatment regimen is a diet with limited intake of fatty foods and salt. Limiting physical activity, eliminating stress and bad habits.
The most common drug therapy is the use of beta-blockers and antiarrhythmic therapy. To stop the process, angiotensin-converting enzyme inhibitors (ACEIs) are used.
To improve the functioning of the heart muscle, the use of potassium and magnesium supplements and amino acids is useful.
| Name of institution | Address(Moscow and St. Petersburg) | Telephone | Procedure (or appointment with a specialist) | Cost, rub) |
| "Heart and Vascular Clinic" | Moscow, st. Shchepkina, 35 | (495) 933-66-55 | Appointment with a cardiologist | 13813 |
| "SM-Clinic" | Moscow, st. K. Zetkin, 33 | (495)241-89-41 | Appointment with a cardiologist | 1450 |
| Nearmedic Clinic | Moscow, 2 – Botkinsky proezd, 8 | 8(499)558-33-21 | Appointment with a cardiologist | 1000 |
| "Center for Endosurgery and Lithotripsy" | Moscow, Enthusiastov Highway, 62 | Appointment with a cardiologist | 2000 | |
| MMC "Union Clinic" | St. Petersburg, Marata street, 69 | +7 | Appointment with a cardiologist | 1500 |
| Network of medical centers and laboratories "MedLab SPb" | St. Petersburg, Obukhovskoy Oborony Avenue, 51 | +7 812 600–22–10 | Appointment with a cardiologist | 1000 |
Author of the article:
Elena Demidova
about the author
Did you like the article?
Let us know about it -
rate
How does heart valve fibrosis manifest?
Due to the fact that the mitral and aortic valves are most often susceptible to the growth of fibrous tissue, it makes sense to dwell in more detail on the clinical manifestations of these valves.
Fibrosis of each valve may not be clinically evident if the valve ring is narrowed slightly (so-called non-critical valve stenosis). If fibrosis leads to valve insufficiency, regurgitation is formed - a reverse flow of blood into the atrium (with damage to the mitral valve) or into the left ventricle (with fibrosis of the leaflets or aortic root). Regurgitation can be moderate or significant, and depending on this, the patient may experience certain symptoms.
Signs of mitral valve fibrosis
fibrosis, calcification and stenosis of the mitral valve
In most cases, fibrosis of the mitral valve leaflets occurs over several years, during which the patient feels satisfactorily, without noting any subjective complaints from the heart. Subsequently, with further involvement of the connective tissue of the valve in the fibrotic process, the patient develops the following symptoms:
- Increased fatigue during normal physical activity, previously well tolerated by the patient,
- The occurrence of attacks of shortness of breath, suffocation, a feeling of lack of air, periodically or constantly noted at rest,
- Feelings of interruptions in the work of the heart (usually like extrasystole or atrial fibrillation),
- Pain in the chest, reminiscent of angina pectoris,
- Periodically occurring swelling of the lower extremities, especially in the morning, after a long horizontal position of the body.
aortic valve fibrosis
What happens with aortic valve fibrosis?
Damage to the aortic valve, whether it is stenosis of the leaflets or aortic root due to fibrosis of the aortic valve, or insufficiency of its leaflets, causes less than normal flow of arterial blood to other organs, including the brain. This provokes general severe weakness, attacks of loss of consciousness, attacks of angina pectoris due to depletion of coronary blood flow, and can also lead to the development of pulmonary edema.
Symptoms
Mitral valve fibrosis can manifest itself in the form of different symptoms and with different intensities.
It all depends on the degree of development of the disease and the extent to which the valve leaflets are affected.
As a rule, the following signs of the disease can be identified:
- with increased physical activity, coughing or shortness of breath begins;
- loss of ability to work;
- fatigue;
- hypertension.
If treatment for fibrosis is not started on time or is ineffective, the patient’s symptoms of the disease worsen and manifest themselves in the form of the following signs:
- heart rhythm disturbance;
- dizziness;
- noise in ears;
- chest pain;
- blood stagnation in the liver;
- a sharp change in blood pressure.
I would like to note that the disease can last for a year or more. In this case, the symptoms change periodically.
Diagnosis of heart valve fibrosis
In cases where fibrosis is mild and occurs without significant symptoms, the doctor can rely on these minor manifestations and on examination data to prescribe a specific follow-up plan for the patient. Routine diagnostics (blood tests, urine tests, ECG) and instrumental research methods are usually prescribed. These include the following:
- Ultrasound of the heart is the most informative study, as it allows you to visualize the smallest internal structures in the heart and reliably assess the degree of fibrosis, the degree of narrowing of the valve ring or the degree of regurgitation. The contractile function of the left ventricle and the ejection fraction are also assessed, that is, the amount of blood that actually enters the aorta, and how much it differs from the proper amount.
- X-ray of the chest organs. Informative in case of venous congestion in the pulmonary tissue, when the configuration of the heart changes, for example, with an enlargement of the atrium or ventricle. An experienced radiologist can always tell which camera is supposedly expanding the cardiac shadow in the image.
- Coronary angiography (CAG, or the so-called “coronary angiography”) is not performed on all patients, but only on those who are planned for surgical treatment for valve replacement. In addition, CAG is indicated for patients with concomitant ischemic heart disease, but the corresponding indications are identified.
Any of the research methods is prescribed by a doctor based on the results of an in-person examination. It happens that a patient notes characteristic complaints of weakness, fatigue, shortness of breath, etc., and the doctor does not see any indication for examination, since such symptoms can be caused by anything, from chronic fatigue syndrome and overload at work to pathology nervous system. In this case, the patient can perform an electrocardiogram and ultrasound of the heart at his own expense in paid clinics, even if only for self-soothing, since there will definitely be no harm from these techniques.
Diagnostic methods
The primary diagnosis is made at an appointment with a cardiologist. Anamnesis, examination of the patient and instrumental diagnostics are carried out. These include:
- Doppler method, which allows you to determine the magnitude of the regurgitant flow.
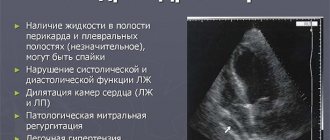
- Two-dimensional echocardiography. During the diagnosis, the aortic root, features of the anatomical structure of the valve and the performance of the ventricle of the left chamber are assessed.
- EchoCG makes it possible to analyze the severity of the disease, identify vegetation and make a prognosis.
The figure below shows images that determine the signs of the disease during echocardiography.
- X-ray of the sternum cavity makes it possible to classify an increase in the volume of the heart and the aortic root.
- Coronography. Rarely used as a diagnostic method, because it is carried out immediately before the operation.
If the disease has a high severity, then signs such as swelling of the lungs of the respiratory tract and failure of the heart organ appear. In this case, physical exercise studies can be carried out in order to analyze the pathology clinic. This method can also be used if there are questionable symptoms.
How to treat cardiac fibrosis and can it be cured completely?
If the fibrosis of the valves is not so severe as to lead to significant stenosis or regurgitation, the patient does not require treatment. Annual monitoring by a cardiologist with regular echocardioscopy is sufficient. But if the patient has other diseases of the heart and blood vessels - arterial hypertension, atrial fibrillation, myocardial ischemia, selection of therapy is required according to the nature of the disease.
If the fibrosis is significant and has led to the development of severe heart failure, in most cases it is necessary to take cardiac glycosides and diuretics (diuretics). Digoxin is usually prescribed at a dosage of 0.25 mg, 1/2 tablet twice a day, five days a week (two days off) continuously or until the clinical situation improves. Of the diuretics, preference is given to indapamide (1.5 or 2.5 mg in the morning), and in more pronounced stages - veroshpiron (25 or 50 mg in the morning), diuver (5 or 10 mg in the morning) and furosemide (20-80 mg in the morning).
When a patient has significant fibrosis leading to grade 2, 3 and 4 valve ring stenosis, valve replacement surgery or surgical dissection of adhesions (commissurotomy) is necessary. Currently, operations can be performed both on the open heart using a heart-lung machine, and through intravascular access, through large peripheral arteries (inguinal, femoral, etc.). Typically, modern mechanical prostheses made of synthetic materials are used. Biological prostheses (from pig valves) are used less frequently. When valve leaflet insufficiency develops, either surgical valve repair with suturing of non-closing leaflets or valve replacement is indicated.
Unfortunately, fibrosis of the heart valves cannot be cured permanently with medications, since it is almost impossible to treat scar tissue with medications. The consequences of fibrosis can be eliminated surgically, but the indications for surgery must be determined strictly individually. In the case where the patient has minor fibrosis that does not lead to stenosis or insufficiency, it is recommended to lead a healthy lifestyle, eat well, regularly see a cardiologist (or cardiac surgeon) and take all prescribed medications, and then it is likely that the operation will be successful. won't be needed for the next few years.
Types and degrees of pathology
The initial stage of the formation of heart valve fibrosis is considered focal. It is characterized by the growth of fibers in a local area. This mechanism serves to limit the focus of inflammation or destruction of the myocardium, which is a compensatory-adaptive reaction.
With the progression of pathological processes in the body, the zones of sclerosis spread, and the second stage begins - diffuse changes.
Any formation of scar tissue in the myocardium is irreversible; muscle fibers lose their functional properties and inhibit the functioning of the entire organ.
Heart valves
Are there possible consequences?
Yes, with cardiac fibrosis, there is a high probability of adverse consequences sooner or later. The likelihood of their occurrence is determined by the reason why fibrosis initially occurred. Thus, the formation of heart defects after rheumatism is more common than the formation of failure or stenosis due to myocardial ischemia and a heart attack. Again, atherosclerosis of the aortic walls with the deposition of calcium in them more often leads to the formation of non-rheumatic heart disease than previous myocarditis, for example. Therefore, it is possible to predict whether valve stenosis or insufficiency will develop after a particular disease, but with great caution.
Prevention of the development of defects in valve fibrosis is the correct and timely treatment of the underlying disease that led to fibrosis or cardiosclerosis.
Forecast
The prognostic value of valve fibrosis is determined primarily by the presence or absence of consequences. Thus, fibrosis without pronounced stenosis or without regurgitation has a favorable prognosis, while hemodynamically significant heart defects resulting from fibrosis and leading to severe heart failure have an unfavorable prognosis. In the latter case, everything depends on the timeliness of the operation - if the operation is performed on time, and the surgeon has caught that fine line when the operation is already indicated, but not yet contraindicated - the duration and quality of life of the patient increases.