#!KardioNA4ALO!#
Heart disease, one of the most common causes of premature death in Russia, can be caused by completely different reasons, among which a certain place belongs to inflammation. The heart muscle, the body's main blood pump, is vulnerable to a range of infections and toxins, making inflammation extremely dangerous. What do you need to know about inflammatory diseases of the heart and blood vessels in order to seek medical help in time?
Inflammatory heart diseases: causes
Among the causes of inflammatory heart diseases, the following are usually identified:
- infectious - diseases can be caused by a wide variety of viruses, microbes, rickettsia, fungi and protozoa; In recent years, increasing importance has been attached to viral infections, with Coxsackie A and B viruses, enteroviruses and influenza viruses coming to the fore;
- toxic - inflammation occurs as a reaction to various toxins, toxins can be very different. This also includes a number of medications (most often used for chemotherapy).
- allergic (immunopathological) - a secondary reaction to the use of certain medications, serums, vaccines, reactions after transplantations;
- infectious-toxic, infectious-allergic - with simultaneous exposure to several different infections, when one of them creates conditions for myocardial damage, and the other is the direct cause of the disease;
- autoimmune - the body’s reaction to the accumulation of antibodies in the tissues of the heart (with rheumatism, connective tissue diseases);
- metabolic – for metabolic disorders (uremic pericarditis with gout);
- physical - trauma or the presence of a tumor (metastatic lesion) - characteristic of pericarditis.
Treatment[edit | edit code]
The basis for the treatment of subacute bacterial endocarditis is the earliest and sufficiently long (at least 4 weeks) administration of effective bactericidal doses of adequate antibiotics, the most reliable choice of which is determined by the sensitivity of microorganisms isolated from the blood. If the results of microbial isolation from the blood are negative, an analysis of the situation is carried out to suggest the most likely pathogen and thereby determine its sensitivity to antibiotics.
In most cases caused by viridans streptococcus, treatment begins with the use of moderate doses of benzylpenicillin (about 4,000,000 - 6,000,000 units per day) intravenously for 4 weeks. In elderly people, as well as if the disease is caused by enterococcus, high doses of benzylpenicillin are prescribed (12,000,000 - 24,000,000 units per day), often in combination with gentamicin (3-5 mg/kg) or amikacin (10-15 mg/kg) per day intramuscularly[4]. Doses are indicated for adults.
For staphylococcal endocarditis, the drugs of choice are semisynthetic penicillins (oxacillin, ampicillin, methicillin, amoxicillin, etc.) 10 g per day in combination with cephalosporins (cephaloridine, cefamizin, claforan) or aminoglycosides. If you are intolerant to penicillins, you can prescribe macrolides (erythromycin, oleandomycin, etc.), as well as aminoglycosides. The same treatment is indicated when identifying gram-negative bacteria ( Escherichia, Proteus
and etc.).
Inflammatory heart diseases: symptoms
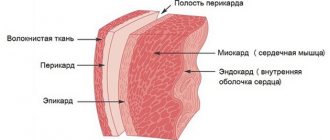
The clinical picture of inflammatory heart disease depends on which tissues are involved in the pathological process: inflammation of the heart muscle itself (myocarditis), inflammation of the inner lining of the heart (endocarditis) or inflammation of the pericardial sac (pericarditis). Common symptoms may be prolonged pain in the heart, shortness of breath, palpitations, and often (with an infectious process), an increase in body temperature to febrile levels. At the first suspicion of heart problems due to any infectious disease, you should contact a cardiologist
. Some forms of inflammatory heart disease are acute and lead to very serious consequences.
Forecast[edit | edit code]
The prognosis is conditionally unfavorable; before the introduction of broad-spectrum antibiotics into practice, in most cases the disease ended in death, but even now death occurs in 30% of cases. Death can occur from heart or kidney failure, thromboembolism, or intoxication.
Early vigorous antibiotic therapy, provided the pathogen is correctly identified and its sensitivity, makes possible an almost complete cure (with more or less pronounced residual sclerotic changes in the valves). Working capacity is slowly restored, and irreversible morphological changes in the valvular apparatus of the heart often develop.
Recurrence of endocarditis usually occurs within 4 weeks after the end of treatment. Their development is a reflection of the inadequacy or insufficient activity (low doses) of antibiotics, or (less often) is an indication for surgical treatment. Relapses lead to severe valve damage and progression of heart failure. The appearance of symptoms of endocarditis later than 6 weeks after the end of treatment does not indicate a relapse, but a new infection.
Inflammatory heart diseases - myocarditis
Myocarditis - what is it? Inflammatory damage to the heart muscle, which is manifested by impaired cardiac activity (excitability, conductivity and contractility). Most often it is of a viral nature (half of all cases of myocarditis). The disease affects middle-aged people (30–40 years old, slightly more often women). By origin, myocarditis is:
- rheumatic;
- infectious (viral, bacterial, etc.);
- allergic (medicinal, post-vaccination, transplant);
- for diffuse connective tissue diseases;
- due to exposure to physical factors (trauma, burns, exposure to ionizing radiation);
- idiopathic (unexplained nature) Abramov-Fiedler myocarditis.
The course of myocarditis can be acute, subacute, chronic (recurrent).
#!KardioSeredina!#
Myocarditis: symptoms and diagnosis
Symptoms of myocarditis are often associated with an infectious disease - ARVI, tonsillitis, etc. (in the background or shortly after it). The most common signs of the disease are malaise, weakness, fatigue, shortness of breath, palpitations, heart rhythm disturbances, sometimes discomfort and pain in the chest, and rarely, pain in the joints. In infectious myocarditis, symptoms of an infectious disease usually dominate (fever, increased body temperature, general signs of intoxication). The onset of myocarditis can be asymptomatic, with low-grade or normal temperature; palpitations, “interruptions” in the heart’s function, and shortness of breath are often noted. The severity of symptoms depends on the prevalence and severity of the inflammatory process. Without treatment, signs of heart failure will increase. It is necessary to urgently consult a medical specialist! Timely diagnostic studies ( ultrasound of the heart
,
ECG
, radiography) can reveal:
- increase in heart size;
- heart rhythm disturbances (tachycardia, less often bradycardia, various arrhythmias);
- intracardiac conduction disorders.
Diagnosis of myocarditis often requires an integrated approach. In addition to physical examination, the following are usually used:
- clinical and biochemical blood test;
- electrocardiography
(ECG); - echocardiography
(ultrasound of the heart); - chest x-ray
; - isotope study of the heart;
- MRI of the heart;
- endomyocardial biopsy;
- cultures of blood and other biological fluids;
- comprehensive study of immunological parameters.
By contacting the Energo clinic for help, you will have the opportunity in one place to undergo all the tests necessary for the correct diagnosis of inflammatory heart diseases. You can make an appointment at the Energo clinic using the form on the website or by calling the phone number listed on the page.
How to treat myocarditis?
Mild myocarditis, which occurs without complications, can be treated on an outpatient basis. In more severe cases, hospitalization, mandatory bed rest, etiotropic, anti-inflammatory and symptomatic therapy are required. Etiotropic therapy - treatment of the infection that caused myocarditis (viral, bacterial, fungal, etc.), and maintenance therapy of the primary disease (rheumatism, SLE, thyrotoxicosis, etc.).
Risk factors for developing myocarditis
The development of inflammatory heart diseases is provoked by:
- decreased immunity;
- viral infections and acute infectious diseases (ARVI, tonsillitis);
- foci of chronic infection (caries, tonsillitis);
- hereditary predisposition to inflammatory heart diseases;
- parasitic and fungal diseases.
Inflammatory heart diseases - endocarditis
Endocarditis - what is it? Inflammation of the inner lining of the heart (endocardium), including the heart valves, most often caused by infection. Acute and subacute bacterial endocarditis (infective endocarditis), caused mainly by a bacterial infection, is of independent importance. Endocarditis is often of a secondary nature (it is a consequence of the development of another disease). Secondary endocarditis develops as an inflammatory reaction to immune complexes localized in the endocardium, often combined with myocarditis (characteristic of diffuse connective tissue diseases, rheumatism and other damaging factors). Infective endocarditis is a very dangerous disease. Without treatment, mortality approaches 100%. Infectious endocarditis is often associated with the problem of intravenous drug addiction, when a bacterial agent enters the blood during an intravenous injection, with a complete lack of compliance with the rules of asepsis and antisepsis.
Endocarditis: symptoms
The clinical picture of the disease consists of symptoms of an infectious process, immune disorders and signs of damage to the heart valves:
- with acute onset of endocarditis - symptoms of general intoxication: fever, temperature 38.5 - 39.5 ° C), chills, profuse sweating, pain in joints and muscles, weakness, weight loss;
- with a long course, a grayish with a slight yellowish color of the skin appears (the color “coffee with milk”), on the hands and feet - Osler’s nodes, small hemorrhages in the mucous membranes, a symptom of “drum fingers” - the terminal phalanges of the fingers and toes thicken, the nails become similar with watch glasses;
- development of hepatosplenomegaly is characteristic; possible manifestations of kidney damage (hematuria, proteinuria);
- rough heart murmurs associated with damage to the valve apparatus are heard; later signs of heart failure appear, usually as valvular heart disease progresses;
- characteristic changes develop in the clinical and biochemical blood test (leukocytosis, acceleration of ESR, increase in acute phase indicators - CRP, fibrinogen).
Endocarditis: diagnosis
The diagnosis can be made by a medical specialist when signs of damage to the valvular apparatus of the heart are combined with fever, enlarged liver and spleen, hematuria, skin hemorrhages, anemia, and increased ESR. To verify the diagnosis, blood cultures, ECG and echocardiography are prescribed. Comprehensive examination and treatment is possible only in a hospital setting.
Endocarditis: treatment
The basis of treatment for bacterial endocarditis is early and long-term administration of effective doses of antibiotics, in parallel, symptomatic treatment is carried out. In some cases, it is necessary to resort to surgical treatment methods - valve replacement. It is possible to cure endocarditis with early, properly selected antibiotic therapy, but irreversible changes in the valvular apparatus of the heart can still develop. Prevention of endocarditis consists of timely and correct treatment of infectious diseases, timely sanitation of foci of chronic infection, and compliance with medical recommendations for people with heart defects.
Risk factors for developing endocarditis
The development of inflammatory diseases of the endocardium is provoked by:
- decreased immunity;
- foci of chronic infection in the body (dental caries, periodontitis, chronic tonsillitis, chronic pyelonephritis, chronic thrombophlebitis, furunculosis);
- history of rheumatism;
- history of heart disease;
- bad habits (drug addiction, alcohol abuse, smoking).
Traditional treatment of pathology
Considering the multifactorial etiology of the disease, therapeutic measures should be organized depending on the cause that caused the inflammatory process. The main method is drug therapy offered by official medicine. Home methods for improving the heart muscle are well complemented by medicinal effects.
Drug therapy includes the following areas:
- Fighting the pathogen.
Chronic sources of infection in the body are often caries and tonsillitis, prostatitis and sinusitis, as well as various abscesses. Therefore, the first step towards eliminating pathogenic flora should be the sanitation of the sources of inflammation. In addition, the patient is prescribed a course of antibiotics (cephalosporins, fluoroquinolones, macrolides). To treat autoimmune and allergic disorders, drugs containing hormones are used.
- Reducing the inflammatory process.
Taking immunosuppressive drugs is mandatory for severe stages of the disease and in the treatment of autoimmune myocarditis. Such medications include glucocorticosteroids “Metypred”, “Prednisolone”, “Dexamethasone”.
In other cases, it is advisable to use non-steroidal anti-inflammatory drugs: Ibuprofen, Ibusan, Diclofenac, Voltaren.
Antihistamines are used for severe allergy symptoms (Tavegil, Suprastin, Delagil).
- Relieving symptoms of myocarditis.
It is carried out with antiarrhythmics, coronary lytics, hypertensive drugs, anticoagulants, diuretics, cardiac glycosides, antipyretic drugs.
- Elimination of metabolic disorders.
To maintain the heart during such a difficult period, substances are needed that improve metabolic processes and provide additional nutrition to the myocardium. All this can be provided by vitamins, as well as drugs called: Mexicor, Riboxin, ATP, Asparkam, Potassium Orotate, Panangin, Mildronate.
Inflammatory heart diseases - pericarditis
Pericarditis - what is it? Inflammation of the pericardium, the serous membrane of the heart; occurs most often as a complication of one or another disease, less often as an independent disease. The causes of pericarditis are as varied as with other inflammatory heart diseases. In principle, infectious (bacteria, viruses, protozoa and even some types of fungi) and non-infectious (connective tissue diseases, tumors, injuries, post-operative) are distinguished. In form - acute (dry, exudative, with or without cardiac tamponade) and chronic. Pericarditis is manifested by an increase in the volume of fluid in the cavity of the pericardial sac or the formation of fibrous strictures that impede the functioning of the heart.
Pericarditis: symptoms
There are no specific symptoms of pericarditis; in the acute process, heart failure develops. Pericarditis usually causes pain in the chest and left arm, vaguely reminiscent of myocardial infarction, but on the ECG with pericarditis, sufficient R amplitude remains, there is no pathological Q wave, changes concern the final part of the ventricular complex (ST segment and T wave). In addition to pain, there are complaints of shortness of breath, palpitations, general weakness, weight loss, a dry cough may develop, in severe cases - hemoptysis, a feeling of heaviness in the right hypochondrium, an increase in abdominal circumference (a consequence of the progression of heart failure). Acute dry pericarditis often occurs suddenly - with a sharp increase in temperature, stabbing pain in the heart area, and a feeling of heart failure. Exudative pericarditis can develop gradually; the more fluid accumulates in the pericardial sac, the more pronounced the symptoms of pericarditis are: swelling of the neck veins, swelling in the legs, cyanosis of the face, suffocation, swallowing disorders, ascites (accumulation of free fluid in the abdominal cavity), tachycardia .
Pericarditis: diagnosis
If there is any suspicion of cardiac dysfunction, you should urgently consult a specialist. Cardiologist
can make a presumptive diagnosis already during a physical examination.
Auscultatory confirmation of the diagnosis will be the absence or displacement of the apical impulse and percussion expansion of the borders of the heart, muffled heart sounds or pericardial friction noise (with dry pericarditis). Instrumental diagnostics - ECG
,
echocardiography
- will allow you to verify the diagnosis. Pericardial diseases are dangerous, so it is unacceptable to self-medicate or drink “something for the heart.” Without correct and quick diagnosis of the disease, serious consequences are possible.
Pericarditis: treatment
Treatment of inflammatory heart diseases is carried out under the supervision of a doctor, usually in a hospital. Only in some mild cases, outpatient treatment is acceptable. The priority direction of therapy for pericarditis is treatment of the underlying disease. Diuretics may be prescribed to reduce the volume of fluid in the pericardium. If there is a threat of tamponade (compression of the cavities of the heart), a percutaneous puncture is performed and the contents are evacuated. Treatment of compressive (constrictive) pericarditis is only surgical.
Risk factors for developing pericarditis
The development of inflammatory diseases of the serous membrane of the heart is provoked by:
- rheumatism;
- systemic autoimmune diseases;
- severe pneumonia;
- chronic renal failure;
- tuberculosis, brucellosis;
- tendency to allergic reactions.
Prevention of inflammatory heart diseases
Primary prevention of most inflammatory heart diseases consists of two simple rules:
- increasing the body's resistance to infections (hardening, healthy lifestyle);
- timely treatment of focal infections (tonsillitis, caries, sinusitis, furunculosis, etc.).
Secondary prevention of inflammatory heart diseases consists of preventing relapses of the disease, taking measures to monitor patients, and following the recommendations of the attending physician for the treatment of the underlying disease (if any). #!KardioKONEC!#