If, in acute coronary insufficiency, the area of necrosis is located in the posterior wall, closer to the atria, then this type is called posterobasal myocardial infarction. The difficulty in identifying it is due to the fact that there may be no signs in standard ECG leads, and if the pain syndrome is atypical, then the diagnosis is not carried out in a timely manner. To determine ischemia, additional leads are required when taking a cardiogram, blood tests, and ultrasound.
Briefly about anatomy and physiology
First, let's try to figure out what the posterior wall of the left ventricle is.
The heart is a hollow muscular organ that circulates blood throughout the body. It consists of 4 chambers: 2 ventricles and 2 atria. The main component of the muscle pump is the left ventricle, which supplies oxygenated blood to all tissues of the body. The thickness of the left ventricular myocardium is approximately 2-3 times greater than other parts of the organ and averages from 11 to 14 mm. Therefore, due to its large size, this part of the heart requires a larger volume of blood, which it receives through the right coronary artery and its circumflex branch. Any damage to the vessels bringing fresh oxygen quickly affects functional activity and can lead to the death of cardiomyocytes.
Due to the features described above, myocardial infarction in 99.9% of cases affects exclusively the left ventricle.
About 10-15% of vascular accidents occur in the posterior wall, which, for the convenience of doctors, is divided into two main sections:
- diaphragmatic;
- basal.
Recent scientific research works of cardiac surgeons, as well as my personal experience, have made this problem more urgent. If myocardial infarction of the posterior wall of the left ventricle develops, it is practically invisible on the ECG and is often hidden under the mask of angina pectoris. As a result, the patient does not receive the necessary range of treatment measures. Organ cells continue to die, and many adverse consequences are observed in the future.
Fortunately, in 60-70% of cases, infarction of the posterior wall of the heart is combined with necrosis of neighboring areas (posteroinferior, posteroseptal, posterolateral), which is clearly reflected in the electrocardiogram curve.
Posterior diaphragmatic myocardial infarction ecg
Myocardial infarction of the posterior wall of the left ventricle
Myocardial infarction of the posterior wall is more difficult to diagnose electrocardiographically than myocardial infarction of the anterior wall. According to ECG and autopsy comparisons, almost half of these infarctions are not visible on the ECG.
The posterior wall of the left ventricle is conventionally divided into 2 parts:
- diaphragmatic section of the posterior wall, - basal section of the posterior wall.
Posterior phrenic (posterior) myocardial infarction.
Causes
In fact, there is a huge list of factors leading to damage to the coronary arteries, but the most significant are:
- Atherosclerosis. Occurs in most people over 60 years of age due to lipid metabolism disorders (increased total cholesterol, LDL and TAG, decreased HDL). As a result of the formation of pathological deposits on the walls of blood vessels, their obstruction occurs. The condition is further aggravated by the sedimentation of thrombotic masses. I have not met cardiac patients without signs of this disease.
- Migration of blood clots from distant sites. This phenomenon is most typical for people suffering from varicose veins of the lower extremities, and is much less common against the background of prolonged physical inactivity (severe somatic diseases) in the absence of antiplatelet therapy. As a rule, middle-aged and elderly people generally do not pay attention to changes in the venous bed in the legs. However, young girls who worry about their attractiveness care much more about it.
- Vasospasm. May occur against the background of disorders of the central nervous system (neuroses, systematic stress).
Factors that predispose to the development of myocardial infarction include:
- arterial hypertension;
- obesity (increased BMI more than 30 kg/m2);
- physical inactivity (WHO recommends walking at least 8,000 steps daily);
- lipid profile disorders;
- presence of bad habits (smoking, systematic use of alcoholic beverages and drugs);
- male gender;
- age from 45 years.
You can assess the presence of risk factors yourself. If there are at least 3 of the above, then the likelihood of a fatal complication from the cardiovascular system increases by 2.5 times. It's not too late to change everything and secure a healthy future for yourself.
Consequences
An attack that has been suffered has a negative impact on the condition of the entire body. Scars form at the site of necrosis on the heart muscle. They are made of connective tissue and cannot contract. Therefore, the area of the myocardium on which they are located permanently loses its functions.
Even properly administered therapy and compliance with all recommendations during the rehabilitation period will not help to completely restore heart function. Most patients develop tachycardia and arrhythmias after an attack.
An extensive infarction is often accompanied by the formation of an aneurysm. In this case, the damaged wall protrudes under pressure and there is a risk of its rupture. Therefore, you cannot do without the help of a doctor.
Thromboembolism, Dressler's syndrome, and heart failure are considered severe complications of the pathology.
Clinical manifestations
It is quite possible to suspect an impending posterior myocardial infarction and other vascular complications (for example, a stroke or hemorrhage in the eyeball) at home.
As a rule, they are preceded by conditions such as:
- hypertensive crisis;
- attack of unstable angina (with a history of coronary artery disease);
- episodes of arrhythmias;
- change in general condition and behavior (sudden sharp headaches, increased sweating, weakness, chills).
Pain
Pain and discomfort behind the sternum are the only things that unite all people with developed myocardial infarction.
Pain has specific characteristics:
- duration over 15 minutes;
- localization behind the sternum;
- lack of effect from nitroglycerin and other nitrates;
- possibility of irradiation to the left scapula, shoulder, forearm and little finger.
It is extremely rare that a “silent picture” is revealed, when pain is completely absent, and only weakness and increased sweating are observed.
Therapy
At the beginning, if possible, conservative treatment is carried out, in which drugs are used to dissolve the blood clot and reduce the heart's need for oxygen, as a result of which it is possible to stop the necrotic process.
They also make sure to use medications to relieve pain, which further aggravates the condition of the heart attack victim.
If treatment with conservative methods is useless, then surgical intervention is performed for myocardial infarction. This treatment gives quick results and allows you to normalize blood circulation in the heart in the shortest possible time.
One of four types of surgery is used:
- Coronary artery bypass surgery. During such an intervention, a new vessel with normal patency is created. For this purpose, a vessel taken from another part of the patient’s body is most often used.
- Installation of a special ring that prevents compression of the artery and restores its normal patency.
- Strengthening the heart walls at the risk of developing their protrusion using special polymer frames.
- In such a situation, suturing the heart wall if it is catastrophically thinned and there is a high risk of its rupture. The wall is strengthened by stitching with a special seam.
Which method of surgical treatment of the pathology will be used is determined by the attending physician. If the risk that the patient will not undergo surgery is high, then it is usually not performed, regardless of the severity of the condition.
Expert advice
An important sign is the duration of pain. Stable angina pectoris never lasts so long. If you have discomfort in the chest for more than 15 minutes, urgently call a team of doctors, since the heart cells are already experiencing acute hypoxia, which may soon enter an irreversible stage (necrosis).
Violation of the functional activity of the heart
Important pathways do not pass through the posterior wall of the left ventricle, therefore, rhythm disturbances are not typical, but sometimes occur (in my memory, such situations have never been observed). By shutting down significant masses of the myocardium from work, stagnation phenomena can be detected from the small (shortness of breath, cough with streaks of blood) and large (swelling in the legs and body cavities, enlarged liver, pallor of the skin with a bluish tint in the distal parts) circles blood circulation
Posterior phrenic myocardial infarction
With this location of the infarction, the lower parts of the posterior wall are predominantly affected. Often the process also extends to the posterior part of the interventricular septum. Signs characteristic of such a myocardial infarction are determined in leads III, aVF, Dorsallis along the Sky, as well as in standard lead II. The Q wave in leads III, aVF is considered pathological if it is more than half the amplitude of the R wave in these leads or wider than 0.03 s.
However, in lead aVF with an undoubted infarction, a Q QI wave may be observed (normally QI>QII). In the cicatricial stage of the infarction, the qII wave may be slightly pronounced or even absent. In the cicatricial stage of a posterior diaphragmatic infarction, sometimes the ECG in leads II, III and aVF and in the Dorsalis lead may look like rS or rSR. If RaVF>RIII is normal, then scar changes in the posterior wall may be indicated by the raVF ratio. Hemorrhagic teeth in the leads, myocardial infarction, may be
Diagnostics
The fundamental method of diagnosis is electrocardiography.
Acute basal isolated myocardial infarction cannot be detected under any circumstances. Damage to the diaphragmatic part of the posterior wall can be recognized by indirect signs. There are no changes in the ECG characteristic of the stages of vascular pathology (acute, acute, subacute, scarring).
So, the doctor will suspect a heart attack based on the following criteria:
- an increase in the amplitude of the R wave in V1 and V2;
- decrease in the depth of the S waves in the 1st and 2nd chest leads;
- the voltage of the S and R waves in the first two leads is the same;
- bifurcation of the R wave (often diagnosed as right bundle branch block);
- T wave elevation in V1-V
The national guidelines for physicians describe variants of small-focal diaphragmatic infarction with the appearance of a characteristic pathological Q wave and ST segment elevation. However, in personal practice it has never been possible to record such changes on a cardiogram, although the clinic was present.
Instrumental diagnostics
Echo-CG is used to establish cardiac wall dysfunction. Ultrasound waves accurately identify areas of myocardial hypo- or akinesia, allowing one to suspect necrotic or cicatricial transformations in them.
Coronography is widely used to locate the source of coronary artery obstruction. After the administration of a contrast agent, a series of x-rays are taken, in which the areas of narrowing are clearly visible.
Laboratory diagnostics
To confirm the diagnosis, the following may be used:
- Complete blood count (increased number of leukocytes and ESR);
- Troponin test - increases in the presence of necrosis of the heart or any skeletal muscle. Damage to the posterior wall is always minor, which is why the troponin level may not increase, leading to diagnostic errors.
Both methods allow you to confirm myocardial infarction only after 6-7 hours. And the golden window in which the cause of occlusion can be eliminated and “barely alive” cardiomyocytes can be restored is only 3 hours. An extremely difficult choice, isn't it? Echo-CG and other highly informative methods (MRI) are not available at all medical institutions.
Myocardial infarction of the posterior wall of the left ventricle
MI of the posterior wall of the left ventricle is much more difficult to diagnose using an ECG than MI of the anterior wall.
According to statistics, in approximately half of cases there are no signs of posterior wall infarction on the ECG. The posterior wall of the left ventricle is conventionally divided into two parts:
1. The diaphragmatic section of the posterior wall includes the lower sections of the posterior wall adjacent to the diaphragm. Myocardial infarction in this area is called posterodiaphragmatic (inferior) infarction.
2. The basal sections of the posterior wall cover the upper sections of the wall adjacent to the base of the heart. Myocardial infarction in this area is called posterobasal (posterior) infarction.
Posterior diaphragmatic MI
Inferior myocardial infarction is caused by blockage of the descending branch of the right coronary artery, which, with the left type of blood supply, can arise from the left circumflex artery. With this localization of the infarction, the lower parts of the posterior wall are affected, often affecting the posterior part of the interventricular septum.
Characteristic signs of posterior phrenic infarction are determined in leads III (II), aVF, Dorsalis (along the Sky):
- the QIII,aVF wave is considered pathological if it is more than half of the RIII,aVF wave or wider than 0.03c;
- in the cicatricial stage of the disease, a QaVF not exceeding half of the RaVF may be observed;
- in case of a heart attack, the QIII wave is necessarily combined with a pathological QaVF wave whose width exceeds 0.02 s;
- the qII wave should exceed 0.1RII, especially in the acute stage (in the cicatricial stage, qII may be absent);
- a heart attack is characterized by the ratio QII>QI (normally, it’s the other way around);
- in the scar stage of the lower infarction, the ECG in leads II, III, aVF looks like rS, rSR'.
If a pathological Q wave is recorded in only one of the leads, then this is not a diagnostic sign of a heart attack. Waves QIII, aVF, not caused by a heart attack, disappear with a deep breath or standing position. Therefore, in doubtful cases, an ECG should always be taken under such conditions.
In the absence of a pathological Q wave, a sign of a posterior phrenic infarction can be pronounced jaggedness of the QRS complex in leads II, III, aVF (the diagnostic value of jaggedness increases if it is in the middle or end of the QRS complex). It should be noted that notching can also be observed with hypertrophy of the ventricles of the heart.
In the acute stage of a heart attack, changes in the ST segment and T wave are also observed in leads II, III, aVF, Dorsalis. In an uncomplicated heart attack, the ST segment returns to the baseline after 2 weeks.
Reciprocal changes (decreased ST segment, high positive T wave) in the acute stage of lower MI are observed in leads V1-V3(V4) and Anterior (along the Sky).
Transmural MI is reliably indicated by the presence of QSIII,aVF. However, with transmural inferior MI, the ECG in these leads may appear as Qr. However, in this case, it is often impossible to make a reliable conclusion about the depth of damage to the ventricular wall based on one ECG.
Posterior diaphragmatic MI (especially in the scar stage) should be distinguished from blockade of the anterior branch of the LAP or from a sharp deviation of the EOS to the left. Sometimes similar ECG changes are observed in idiopathic subaortic stenosis, individual cardiopathy, acute pericarditis, and pulmonary embolism.
Posterobasal MI
Posterior myocardial infarction is caused by obstruction of the right posterior descending artery or left circumflex artery. Such MI of the high parts of the posterior wall of the left ventricle is very difficult to diagnose and is often not detected on the ECG, since there are no signs of infarction in the 12 usual leads. In these cases, the diagnosis of posterobasal MI is made by reciprocal ECG changes.
In some cases, direct signs of posterior MI are detected in additional leads V7-V9 and lead Dorsalis (along the Sky) - pathological Q wave, ST segment elevation in the form of a monophasic curve in the acute stage, followed by the formation of a negative T wave.
Characteristic ECG changes in posterobasal myocardial infarction:
- the RV1, V2 wave increased in amplitude (normally there should be a small amplitude r wave followed by a deep S wave);
- tooth SV1,V2 reduced in depth (SV1,V2 QI.
Characteristic reciprocal changes in leads V1-V3, V3R, Anterior (along the Sky), caused by damage to the basal parts of the posterior wall:
- increased RV1,V2;
- reduced SV1,V2;
- RV1/SV1≥1;
- extended initial RV1≥0.04 s;
- in leads V1, V2, V3R the ECG looks like R, RS, Rs, rR', RSR';
- decrease in the STV1-V3(V4),aVR segment below the isoline;
- high positive TV1-V3 and V3R.
The appearance of permanent or transient bundle branch block or atrioventricular conduction disturbance in the presence of extensive MI in the posterior wall indicates the spread of the infarction to the posterior part of the interventricular septum. In approximately every fourth patient with posterior wall MI, it spreads to the posterior wall of the right ventricle.
Emergency help
If you happen to meet a person with a myocardial infarction, the procedure will be as follows:
- Call an ambulance immediately.
- Place the patient on the bed, raising the head end of the body.
- Provide fresh air flow (open windows).
- Make breathing easier (remove tight outer clothing).
- Every 5 minutes, give any nitro drug (“Nitroglycerin”) under the tongue, simultaneously measuring blood pressure and heart rate before a new dose. When the heart rate increases more than 100 beats per minute or blood pressure decreases below 100/60 mm. rt. Art. therapy is stopped.
- Suggest taking Acetylsalicylic acid (0.3 g) orally.
It is impossible to attempt to eliminate coronary pain with conventional analgesics. Is a painkiller capable of preventing necrosis of heart cells? In addition, the clinical picture may be erased, which will complicate diagnosis.
Features of the disease
The heart wall consists of three layers:
- Endocardium is connective tissue up to 0.5 mm thick. Lines the cavity of the main organ, exactly repeating its relief.
- The myocardium is the thickest membrane formed by striated striated muscle, consisting of tightly connected cells - cardiomyocytes. They are interconnected by jumpers, forming a narrow-loop network that ensures rhythmic contraction of the atria and ventricles.
- The epicardium is a smooth and thin outer layer. Constructed from a connective tissue plate that has collagen and elastic fibers. In close contact with the myocardium.
During ischemia, necrosis can spread to more than just one layer.
Depending on the depth of the lesion, several types are distinguished:
- Transmural - all layers of the heart are involved in the process. The necrotic focus penetrates the wall of the organ through and through.
- Non-transmural - the area of pathology is limited to one endocardium or epicardium in combination with the myocardium.
- Subendocardial - necrosis is located in a narrow strip near the inner lining of the left ventricle.
- Intramural - the affected areas are localized in the thickness of the muscle wall. In this case, the boundary layers are not affected by necrosis.
Treatment
Immediately after diagnosis, emergency treatment with the following drugs is carried out:
| Name of the medication | Dose |
| Aspirin (if not given previously) | 0,3 |
| Metoprolol | 0,0250 |
| Morphine 1% | 1 ml |
| Heparin | Up to 4000 units |
| Clopidogrel | 0,3 |
| Oxygen therapy (40% O2) | Until signs of heart failure are eliminated |
The patient is urgently hospitalized in the cardiac intensive care unit. Systemic or local thrombolysis is performed (if less than 6 hours have passed since the onset of the disease). In the long term, stenting or coronary artery bypass grafting is indicated.
The main directions of therapy are as follows:
- Prevention of rhythm disturbances. Beta blockers (Metoprolol, Carvedilol, Bisoprolol) and calcium channel antagonists (Amlodipine, Verapamil, Bepridil) are used.
- Antiplatelet and anticoagulant therapy (Clopidogrel, Xarelto, Pradaxa).
- Relieving pain symptoms.
- Statin therapy (Rosuvastatin, Atorvastatin, Simvastatin).
Complications
The consequences of a heart attack can be significant. Typically, several life support systems are affected at once.
Heart failure
Dead heart cells are no longer able to pump blood in full. The fluid begins to actively move from the vascular bed into the surrounding tissues with the development of multiple edema. Organs suffer from hypoxia, against the background of which foci of dystrophic changes form. As experience shows, the brain is the first to take the hit (a decrease in all functions is observed: attention, memory, thinking, etc.). Episodes of loss of consciousness, dizziness, and staggering when walking appear.
The most dangerous is pulmonary edema. It can be acute (occurs instantly) or chronic (increases over several days or months). Exudate begins to leak into the lower parts of the paired organ, as a result of which a large number of alveoli cease to perform the respiratory function.
Progression of IHD
As you know, our body has a wide ability to adapt. Efficient heart tissue undergoes hypertrophy (gain of muscle mass), which significantly increases the volume of required oxygen, but the functionality of the remaining segments of the coronary bed is not unlimited. The frequency of angina attacks increases, they become more pronounced and prolonged. The risk of recurrent myocardial infarction increases 3-5 times.
Myocardial remodeling
Against the background of inadequate load and hypertrophy of the myocardium, after a few years, dilatation is observed - thinning of the walls with the formation of bulges - aneurysms. The consequence is always the same - tissue rupture with cardiac tamponade (outflow of blood into the pericardial cavity). This complication is fatal in 8 out of 10 patients.
ECG for myocardial infarction of the true posterior wall
The ECG changes described above
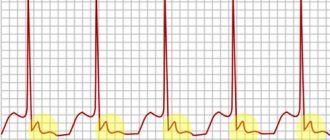
are observed, as already mentioned, with the so-called MI of posterior localization, i.e. essentially with an inferior infarction. However, if the infarction is truly localized in the posterior wall, then they speak of a posterior MI. The resulting LV EMF vector is directed to the left and from bottom to top and forward. The ECG shows a peculiar picture: a high R wave in leads V1 and V2, depression of the ST segment and a negative or positive T wave.
Features of the ECG in myocardial infarction of the posterior (lower) wall
: • Occlusion of the right coronary artery or the circumflex branch of the left coronary artery • Necrosis of the myocardium of the inferior wall • In the acute stage: ST segment elevation and positive T wave in leads II, III and aVF • In the chronic stage: deep negative T wave and large Q wave • Positive blood test result for creatine kinase and troponins
Note the tall R waves and ST segment depression in leads V1-V3.
Forecast
The prognosis for infarction of the posterior wall of the heart in the absence of emergency assistance in the first hours after development is conditionally unfavorable. There will be a gradual increase in dysfunction of the heart muscle, which will ultimately lead to the death of a person. To avoid any undesirable consequences, you should try your best to prevent a heart attack, especially if you are at risk.
The process of aneurysm formation
Posterior diaphragmatic myocardial infarction ecg
• Myocardial infarction (MI) of the posterior wall occurs due to occlusion of the right coronary artery or the circumflex branch of the left coronary artery.
• ECG changes during myocardial infarction (MI) of posterior localization, in contrast to MI of anterior localization, appear mainly in the limb leads.
• In acute posterior myocardial infarction, ST segment elevation and a high positive T wave (monophasic ST segment deformation) are recorded in leads II, III and aVF, especially in lead III. Often, even with a “fresh” MI, a large Q wave is recorded.
• With “old” myocardial infarction (MI) of posterior localization, there is no longer ST segment elevation and positive T wave in leads II, III and aVF. In lead III, a large Q wave is recorded and, in addition, a pointed negative T wave and ST segment depression.
• The result of a blood test for serum markers of myocardial necrosis (creatine kinase activity and its MB fraction, troponin I or T concentration) in acute myocardial infarction (STEMI) is positive.
Clinical case
In conclusion, I would like to cite an interesting case from personal experience, which proves the complexity of recognizing ischemic damage to the posterior wall of the left ventricle.
Patient D., 66 years old. He was repeatedly admitted to our cardiology department by ambulance with a diagnosis of Acute Coronary Syndrome. For reference, I would like to say that this term refers to two pathologies. This is a myocardial infarction and an episode of unstable angina. Only after an examination (ECG, troponin test) is the exact nosology determined.
The patient complained of pain in the chest, lasting 35-50 minutes. Each time an examination was carried out (ECG, CBC, troponin detection test), which did not reveal signs of necrosis. Nitroglycerin in the form of a 1% solution and Aspirin were used.
Unfortunately, a few days ago the patient died in a car accident. At autopsy, it was discovered that the patient had suffered 3 small-focal myocardial infarctions during his life, caused by damage to the circumflex branch of the posterior coronary artery. More than 2 years have passed since the last one.
Thus, infarction of the posterior wall of the left ventricle represents a huge problem for modern cardiology due to the almost complete lack of timely diagnosis. Although such a vascular complication is extremely rare, the likelihood of its development cannot be ignored. Prevention is always based on a healthy lifestyle and adequate treatment of any diseases (especially those related to the cardiovascular system).
Posterior diaphragmatic myocardial infarction (or infarction of the inferior wall of the left ventricle)
With this localization of MI, the lower parts of the posterior wall adjacent to the diaphragm are predominantly affected, therefore this location of the infarction is often called an infarction of the lower wall. Sometimes, with a posterior phrenic infarction, the process spreads to the posterior part of the IVS. Posterior diaphragmatic (inferior) MI develops when the proximal parts of the right coronary artery are occluded.
ECG signs of posterior diaphragmatic (lower) MI are:
· the presence of direct signs of infarction (pathological Q or QS wave, decreased amplitude of the R wave, elevation of the ST interval, negative coronary T wave) in leads II, III, aVF, D along the Sky, and the greatest role in the diagnosis of posterior diaphragmatic infarction belongs to lead aVF;
· the appearance of reciprocal ECG changes in leads I, aVL, V1 -V3 (ST segment depression, high positive T wave);
· increase in the amplitude of the R wave in lead aVR>1 mm (not a constant sign).
The most important role in the ECG diagnosis of posterior diaphragmatic (inferior) MI is played by the correct assessment of the Q wave in leads III and aVF
Criteria for a pathological Q wave in leads III and aVF (V.N. Orlov, 1983):
· tooth width Q>0.03 s;
· depth of the Q wave> 1/2 of the amplitude of the R wave in the same leads, however, a Q wave of 10% RII can be observed in lead aVF;
· QIII and QaVF waves. caused by the presence of MI in the posterior diaphragmatic region, never disappear or decrease during deep inspiration and in the vertical position of the patient; on the contrary, deep QIII and QaVF. not caused by myocardial infarction, disappear or decrease significantly during inspiration and in the patient’s upright position;
· pathological wave Q III, aVF is often jagged or split;
· a pathological QIII, aVF wave is most likely pathological if it is combined with a negative T wave or ST interval elevation, or if the following R wave is jagged or split.
Rice. Posterior phrenic (lower) infarction. Direct signs of a heart attack (pathological Q wave, elevation of the ST interval, formation of a negative T wave) in leads II, III, aVF, reciprocal changes (depression of the ST interval, high positive T wave) in leads I, aVL, V1, V2, V3.
Rice. Acute large-focal myocardial infarction of the inferior wall of the LV.
Rice. Acute large-focal myocardial infarction of the inferior wall of the LV, complicated by 1st degree AV block.