Peculiarities
According to European and American criteria, the syndrome can manifest itself for no more than 2 weeks, however, in Russian medical practice there are often cases when concomitant symptoms of post-infarction angina were observed in patients within a month after a previous heart attack.
According to statistics, men are more at risk of developing this disease due to poor lifestyle and abuse of bad habits.
Post-infarction angina, unlike other forms of this syndrome, is considered the most dangerous because it is characterized by instability of manifestations. It is the main provoking factor in the development of recurrent myocardial infarction. According to statistics, a similar syndrome develops in 27% of patients who were hospitalized due to a heart attack.
Post-infarction angina syndrome is usually divided into early (symptoms appear no later than 2 weeks after the infarction) and late (the first manifestations of the syndrome occur at a later period). The early form of angina pectoris primarily signals a serious heart condition. In this case, the probability of death increases from 2% to 20 - 50%.
First aid
First aid during an attack of RPS does not differ from that which must be provided for typical angina. However, it cannot be removed with conventional medications, so you must immediately call an ambulance. Before visiting doctors:
- sit the patient comfortably - if the attack began in a lying position, help the person sit up and hang his legs off the bed;
- unbutton his collar, and it is better to take off his clothes with a narrow neck;
- ventilate the room;
- give the victim a Nitroglycerin tablet, and five minutes later - another one.
People with low blood pressure are not recommended to take Nitroglycerin, but Aspirin helps alleviate the condition. Those patients who have recently suffered a heart attack should not refuse hospitalization and examination, even if the pain in the heart was short-lived.
to the point ↑
Reasons for development
Post-infarction angina develops both against the background of general provoking factors and against the background of specific features. The development of angina is preceded by such diseases as:
- atherosclerosis of the coronary arteries;
- arterial hypertension;
- obesity;
- diabetes;
- hyperlipidemia;
- physiological tendency to form blood clots;
- regular stressful conditions.
Specific factors for the development of this syndrome include the following:
- the occurrence of acute stenosis of the coronary arteries as a consequence of drug or spontaneous thrombolysis;
- lesions of the coronary vessels;
- systolic dysfunction of the left ventricular cavity;
- instability of diastolic pressure;
- acute infarction without ST-segment elevation.
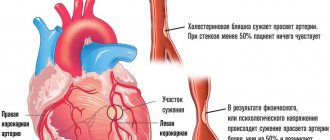
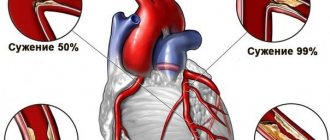
The pathological mechanisms of early post-infarction angina are determined by damage to the coronary arteries by lipid deposits. There is also destruction of cholesterol plaques and progressive stenosis of the coronary vessels. This is characterized by the following functional shifts:
- coronary spasm;
- hemocoagulation is impaired;
- damage to the vascular endothelium.
Coronary spasm
Coronary spasm plays a huge role in the development of coronary artery obstruction. The development of coronary spasm is caused by endothelial dysfunction and the influence of vasoconstrictor substances secreted by platelets during thrombus formation.
Dysfunction of the endothelium of the coronary arteries consists of a decrease in the production of vasodilating substances (nitrogen oxide, prostacyclin, hyperpolarizing factor) and a significant increase in the synthesis of vasoconstrictors (endothelin, angiotensin-2 - formed on the surface of the endothelium with the participation of angiotensin-converting enzyme).
The development of coronary spasm increases the degree of obstruction of the coronary artery caused by atherosclerotic plaque and thrombus, and converts non-occlusive obstruction into occlusive one, causing myocardial necrosis.
Pathomorphology
Depending on the prevalence of necrosis, MI is divided into forms.
2. Non-transmural – subepicardial, subendocardial, intramural.
Symptoms of post-infarction angina
The key symptom of this syndrome is the resumption of anion attacks. The symptom may appear 2-3 days after a heart attack (early form) or 2-4 weeks (late form). In addition, the post-infarction state is characterized by intense pain in the chest. As a rule, to neutralize the pain syndrome, intravenous administration of analgesics, including those containing narcotic substances, is required. This symptom can manifest itself both during bed rest and during low physical activity and stressful conditions. In the first case, exacerbation of the pain syndrome is usually accompanied by an increase in blood pressure.
The atypical course of post-infarction angina may be accompanied by minor chest pain. In some cases it may be completely absent. This condition is characterized by signs of arrhythmia and heart failure. These factors are provoking for the recurrence of myocardial infarction.
The following accompanying symptoms are characteristic of post-infarction angina:
- feeling of heaviness in the chest;
- pain in the heart often radiates to the left arm, neck or under the shoulder blade;
- burning sensation in the chest.
Clinical picture of repeated
1) high frequency among men;
DETAILS: Treatment of hypertension using the Myasnikov method
2) the beginning of the acute period with collapse and dynamic cerebrovascular accident;
3) frequent development of thromboembolic complications and hypostatic pneumonia;
4) the predominance of heart failure, cardiogenic shock, and cardiac arrhythmias in the clinical picture;
5) protracted or recurrent course, long-term persistence of increased rates of resorption-necrotic syndrome.
ECG symptoms of repeated MI can be clear and characteristic, while signs of previous scar changes in the myocardium remain, but sometimes ECG signs of repeated infarction are unconvincing; in this case, a special role in diagnosis belongs to dynamic analysis of the ECG, echocardiography, and determination of biomarkers of necrosis in the blood myocardium.
Diagnostics
Diagnostic methods for confirming post-infarction angina include laboratory, clinical and instrumental studies. The diagnosis is determined by the attending physician using the following data:
- previous heart attack;
- ECG - monitoring;
- coronary angiography;
- stress tests.
- Ultrasound of the heart muscle;
- daily ECG monitoring;
The ECG records ST-segment depression of 1 mm. and more. Painful attacks are characterized by inversion of the T wave. These indicators may also indicate the development of ischemia, as well as changes due to the patient’s heart attack. This reduces the effectiveness of this method in determining post-infarction angina.
Different degrees of sensitivity are noted in the following diagnostic methods:
- with an accuracy of 58% it is possible to correctly diagnose this syndrome thanks to stress tests;
- Holter monitoring determines the development of the syndrome with an accuracy of 27%;
- Carrying out tests with hyperventilation makes it possible to determine post-infarction angina with only 11% probability.
Coronary angiography is performed using CT or MSCT. This makes it possible to accurately identify stenoses of the coronary arteries, as well as damage to the trunk of the left eternal artery (8 - 12%). Often, patients suffering from this post-infarction condition may be diagnosed with multivascular lesions.
Diagnosis
The diagnosis of myocardial infarction in most patients is not difficult and is based on the classic diagnostic triad: a typical clinical picture, ECG data, and determination of blood biomarkers of myocardial necrosis.
When using the above diagnostic criteria, one should remember the possibility of developing a heart attack with atypical clinical manifestations, as well as diseases that can produce symptoms similar to myocardial infarction.
Therefore, a thorough analysis of the clinical picture of the disease and the mandatory presence of the 2nd and 3rd diagnostic criteria are very important. A particularly important role is played by the increase in the blood level of biomarkers of myocardial necrosis, primarily troponin T or I, followed by the characteristic dynamics of their decrease.
Diagnostic criteria for myocardial infarction
- severe and prolonged attack of chest pain ({amp}gt;30-60 minutes), accompanied by weakness, cold sweat, sometimes nausea, vomiting
- the appearance of a pathological Q wave
- changes indicating myocardial ischemia - elevation or depression of the ST interval
3. Typical dynamics of the rise and further decrease in the blood level of biomarkers of myocardial necrosis (troponins T, I or CPK-MB, CPK-MB mass, if determination of troponins is impossible)
4. Interventions on the coronary arteries (for example, angioplasty) with a subsequent increase in the level of troponins or CPK-MB in the blood
Treatment methods for post-infarction angina
Therapeutic and surgical methods of treating this syndrome are aimed at reducing the risk of recurrent infarction, as well as stopping anion attacks. The therapeutic course also includes a set of preventive measures. Depending on the general physiological condition of the patient, the attending physician recommends the following measures:
- bed or semi-bed rest for at least 1 month;
- abstinence from physical activity;
- lack of emotional experiences and mental stress;
- exclusion of high-calorie foods from the diet;
- regular monitoring of the cardiovascular system.
The therapeutic course consists mainly of medications, such as:
- B - adrenergic blockers;
- potassium antagonists;
- nitrates;
- anticoagulants.
Some cases require complex treatment through conservative therapy and cardiac surgery (balloon angioplasty, coronary bypass surgery, stenting).
If there is intense pain in the heart area, the doctor may prescribe nitroglycerin drips. In addition, it is recommended to take medications for complex therapy and prevention. These include drugs that prevent the formation of blood clots, as well as direct anticoagulants. The duration of treatment depends on the nature of the further course of the disease, as well as on the individual physiological characteristics of the patient.
Early manifestations of post-infarction angina syndrome can provoke a re-exacerbation of the heart attack, which can lead to fatal consequences. After coronary angiography, if anion attacks are repeated frequently, a decision may be made to use surgical treatment methods.
The most common ones include coronary aortic bypass surgery, angioplasty and stenting of the damaged artery. Such methods of surgical intervention will significantly reduce the risk of recurrent infarction, as well as provide a high probability of survival for a patient with early post-infarction angina syndrome. In this form, treatment with medications is primarily aimed at maintaining the patient’s current condition, since in this case it does not have a significant therapeutic or preventive effect.
Important! Planned cardiac surgical procedures are carried out mainly 3-4 weeks after a heart attack.
Symptoms of the disease
The first symptom is pain behind the sternum, sometimes on the left, in the region of the heart. The pain can be pressing, burning, cutting, squeezing, boring or pulling. They give to the left shoulder or arm. It happens that the recoil goes to the lower jaw or can shoot into the left shoulder blade, into the stomach, even into the legs. The pain can be insignificant or unbearable, terrifying the sick person, causing fear of death. In general, the manifestations of angina pectoris are individual in nature.
Most often, pain occurs during movement, but can also occur at night. There is a lack of air, the skin becomes pale, the hands become cold, and they feel numb. You can alleviate the condition by taking medication - nitroglycerin. It is better to take a sitting or standing position and follow the recommendations of your doctor.
In general, a characteristic symptom of the post-infarction form of the disease and its difference from other types is the reappearance of attacks, perhaps even in a more acute form, after a heart attack. This type of disease is classified as unstable angina, one of its most dangerous forms.
Important! When acute symptoms appear, the risk of recurrent myocardial infarction increases significantly, which the person may no longer survive. It is worth understanding how dangerous this type of disease is for the patient. That is why seeing a doctor and constantly monitoring one’s own condition is a prerequisite for a normal subsequent life for the patient. Early post-infarction angina is a complex disease that, fortunately, can be corrected.
Forecast
The early form of post-infarction angina is characterized by disappointing prognoses, since it indicates a severe condition of the heart muscle. This increases the risk of another heart attack, which in turn can cause sudden death. In this case, there are usually no warning symptoms. Since early manifestations of the syndrome are associated with high risks, even in a hospital setting, doctors can make a decision regarding surgical intervention aimed at myocardial revascularization.
This measure allows you to achieve a stable state of the cardiovascular system in 90% of cases. Early post-infarction angina syndrome disappears in 60% of patients after successful surgery. The probability of death during surgery, according to statistical data, is less than 1%. After the operation, the patient must be under constant supervision of a qualified cardiac surgeon.
Late manifestations of post-infarction angina are more sensitive to conservative treatment. With an effective therapeutic course, the likelihood of a re-exacerbation of a heart attack is minimal. In some cases, experts may recommend coronary artery bypass grafting.
It is extremely important to follow all the recommendations of your doctor, especially regarding rest and nutrition. Traditional medicine recipes can help in prevention, but only after prior consultation with your doctor.
Medicines to prevent heart attack
To solve the first problem, three groups of drugs are used.
The first is acetylsalicylic acid . Just like that, for prevention, a healthy person or even a hypertensive person does not need to take aspirin. But if we have established a diagnosis of “coronary heart disease,” then constant use of acetylsalicylic acid is mandatory. This drug prevents platelets from sticking together and therefore prevents the formation of blood clots. He seems to act as a policeman who walks around the square and commands “not to gather more than three.”
Some patients refuse to take acetylsalicylic acid because it affects the stomach. Yes, it works - but, of course, it does not directly corrode the stomach. Acetylsalicylic acid is absorbed into the blood and blocks the production of substances that form a protective layer of stomach mucus. And in this case, the risk associated with taking aspirin is much lower than the benefit, which is the prevention of myocardial infarction.
Well, if you have had an ulcer in the past and are afraid to take acetylsalicylic acid, your doctor will recommend gastric acid blockers such as omeprazole .
The second group of drugs is statins . These drugs have the ability to stabilize cholesterol plaque, reduce cholesterol deposits on the walls of blood vessels and prevent this plaque from rupturing.
According to global practice, statins for coronary heart disease must be prescribed to all patients, regardless of the initial cholesterol level. Reducing cholesterol once a diagnosis of coronary artery disease has been established using diet alone, as is often attempted, is a very serious mistake.
Patients with coronary heart disease should have very low cholesterol levels. When adjusting the dose of the drug, it is better to focus on the so-called “bad cholesterol” or LDL cholesterol, the level of which should be <1.8 mmol/l.
Let us briefly recall the main myths and legends associated with statins. Myth 1. Statins are addictive and should not be stopped. Truth: you should not stop taking statins not because they cause addiction, but because if you stop taking them, the plaque will grow further, the symptoms of angina will progress, and the likelihood of myocardial infarction will increase. Myth 2. We treat one thing, we cripple another. Statins cause changes in the liver and kidneys. Is it true. Significant changes in the liver while taking statins occur in one to two patients out of a thousand. During this time, it is possible to prevent 4–5 heart attacks. As for the kidneys, on the contrary, statins protect the kidneys even in renal failure.
The third group of drugs that increase life expectancy in patients with coronary artery disease are ACE inhibitors . These drugs are successfully used to lower blood pressure. However, back in the last century, their ability to prevent the development of heart failure in patients at high risk of complications was discovered. Therefore, if your doctor recommends taking these medications even with normal blood pressure, do not refuse. However, since ACE inhibitors do reduce blood pressure, they are prescribed in small doses in people with normal blood pressure.
Possible complications and prognosis
RPS syndrome indicates that in the area of necrosis of the heart muscle there are still functional cells: if they die, the heart attack will recur. One of the possible complications of RPS is coronary artery thrombosis.
The general prognosis of the disease depends on whether the heart attack was primary or repeated. Other factors:
- patient's age;
- severity and extent of heart damage;
- timeliness of thrombolytic therapy;
- presence/absence of seizures before a heart attack.
Late manifestations respond better to conservative therapy, and with adequate treatment, the likelihood of a repeat disaster is minimal.
Early and atypical forms of the syndrome have a less favorable prognosis: the first indicates significant damage to the myocardium, and the atypical form is difficult to diagnose - in the absence of pain, arrhythmias progress, and heart failure develops and becomes chronic.
to the point ↑