Features of the disease
To understand how and for what reasons intraventricular block develops, it is important to understand that in the myocardial system, which provides consistent, continuous and rhythmic electrical excitation of all cardiac structures, there are separate muscle cells called Purkinje fibers and bundles of His.
The first formation is represented by cardiomyocytes, which are characterized by increased electrical excitability, being located in the ventricles. The left and right branches are called legs, the latter of which has posterior and anterior branches. Decreasing in diameter, they seem to break up into a huge number of small branches, which are Purkinje fibers.
Due to various organic or functional changes in the heart, obstacles appear in the path of electrical signals. In this case, the impulse does not travel further through the ventricles of the heart (in a specific situation). Because of this, the areas located below cannot contract and excite. This becomes visible on the cardiogram.
Sinoatrial blockade
Sinoatrial blockades occur:
- in the sinus node (there is no impulse or it does not have sufficient strength);
- in the transition zone (the signal from the sinus node does not pass to the atrium);
- in the atrium (the part of the heart that does not perceive the impulse).
There are three degrees of pathology, each with characteristic features noticeable on the ECG. The second degree of sinoatrial block is divided into two types - Mobitz 1 (Samoilov-Wenckebach periodicity) and Mobitz 2.
Normally, the sinus node produces an impulse that travels through the transition zone to the atrium. It is excited, and a normal P-wave is recorded on the cardiogram. With the first degree of sinoatrial block, the signal slows down due to problems in the transition zone - this pathology is not visible on the ECG. To identify it, you need to record the potential in the sinus node or electrical stimulation of the atrium.
With a second degree blockade, the electrical signal sometimes does not pass through at all. The number of impulses before the loss of heart contraction can be different, as well as the number of dropouts themselves. III degree of violation is characterized by a complete absence of impulse. But the heart works tirelessly - the role of the sinus node in such cases is performed by its other parts. Ectopic rhythms are recorded on the ECG.
Sinoatrial obstruction visible on the cardiogram:
| Graphic image on a cardiogram | The pathology that caused the change | Characteristic signs |
| Type 2 sinoatrial blockade II degree | Absence of the QRS complex, T-wave and P-wave, they fall out. The distance RR before and after the pulse drop is the same. The dropout interval distance is two RR. The waves are the same, the QRS complexes are the same | |
| Type 1 sinoatrial block II degree | Until the loss of heart contraction, the RR interval progressively decreases. After the impulse falls out, it is restored and gradually decreases again (Samoilov-Wenckebach period). The dropped interval is not equal to twice the RR of the preceding heartbeat. The RR interval after the drop is greater than the interval preceding it | |
| Type 1 sinoatrial block of the second degree with loss of several heartbeats | The RR dropout interval increases in proportion to the number of dropped beats | |
| Type 1 sinoatrial block of the second degree with escape ventricular contraction | Several heartbeats occur, but another part of the myocardium performs the function of pacemaker. The QRS complex has changed. There is no P wave | |
| III degree sinoatrial block | There is not a single impulse. Isoline. The situation is life-threatening, sometimes ending in death | |
| Third degree sinoatrial block with ectopic signal from the atrium | Negative P wave | |
| Third degree sinoatrial block with ectopic signal from the AV junction | Absence of a P wave | |
| Third degree sinoatrial block with ectopic signal from the ventricle | There is no P wave, the altered QRS complex is widened |
Place of manifestation
Intraventricular block can occur anywhere in the ventricles. Therefore, the resulting disorders are divided into nonspecific and bundle block. Each of these subtypes has its own ECG criteria.
It is noteworthy that intraventricular block can develop even in an absolutely healthy person, without affecting his well-being in any way. But this is still considered conduction disorders along the right branch. When registering the left hemiblock, as well as with a two- or three-fascicle blockade of the terminal branches, it is generally accepted that some kind of cardiac pathology is present.
What is heart block?
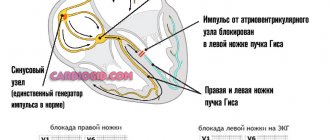
work of the conduction system of the heart
Let's start with the fact that the normal functioning of the heart is facilitated by electrical impulses generated in the sinoatrial node. From it they are distributed throughout the atria, the contractions of which contribute to the transmission of the impulse further, through the atrioventricular node to the atrioventricular His bundle. From there it is distributed into areas through smaller branches. With a decrease in the automaticity of the sinus node, between atrioventricular contractions increases (lengthens)
Sometimes the impulse does not travel through the conduction system at all. In this case, there is no contraction of the atria or ventricles. A long pause occurs (atrial asystole), which is called the Wenckebach period. When it occurs, conductivity is restored again, thanks to the ectopic rhythm, which is called the “rescuing” rhythm. And the next atrioventricular interval is already of normal length. Symptoms with incomplete (partial) heart block are almost completely absent, since it does not disrupt the blood supply to the brain. Most often, partial heart block is accompanied by slight dizziness and slight malaise.
Complete heart block is characterized by the occurrence of bradysystole - a sharp decrease in the number of ventricular contractions (up to 30-40), when the number of atrial contractions remains normal. This almost always causes significant circulatory problems. Patients complain of shortness of breath, dizziness, and their vision suddenly becomes dark.
Sometimes a drop in cardiac activity (a sharp decrease in ventricular contractions to 15 per minute) causes cerebral ischemia. In this case, a Morgagni-Adams-Stokes (MAS) attack occurs: epileptiform convulsions develop, and the person loses consciousness for several minutes. Before it occurs, he begins to feel weak, a feeling of intense heat arises in his head, then he suddenly turns pale and loses consciousness. This condition is called instantaneous blockade . It develops when a violation of sinus rhythm turns into ventricular automaticity. Repeated attacks of MAS often cause death.
Video: heart block on ECG
The video shows an intermittent (alternating) blockade of either the right or left bundle branch
Causes
The causes of blockade of intraventricular conduction, as a rule, appear in childhood. Diseases due to which this disorder develops can occur in both the right and left hemiblock. In addition, blockades of terminal branches can have an effect.
These ailments include: cardiomyopathy, myocarditis, disorders of the heart architecture due to acquired or congenital defects, cardiosclerosis, heart tumors. But there is no need to panic ahead of time, since in both children and adolescents, incomplete and even complete blockade of the right leg is considered a normal condition, often occurring against the background of a healthy heart.
In adults and old age, intraventricular heart block develops for completely different reasons. Almost half of all cases are associated with atherosclerotic lesions of the artery that supplies the myocardium in the area of the conduction bundle. This causes myocardial ischemia. In addition to chronic ischemia, acute myocardial infarction leads to this problem.
About a third of all cases occur due to hypertension. Congenital heart defects and rheumatism can also be common causes of intraventricular block.
Regardless of age, blockades are provoked by alcohol poisoning or its surrogates, hyperkalemia, usually due to renal failure, chest injuries, and excessive use of certain drugs. For example, intraventricular block develops due to poisoning with potassium-containing drugs and some psychotropic drugs.
Etiology
- Basically, the causes of heart block lie in the progression of diseases, such as:
- myocarditis of thyrotoxic, diphtheria or autoimmune type;
- diffuse connective tissue diseases;
- heart defects and tumors;
- sarcodia and amyloidosis;
- myxedema;
- syphilis affecting the heart and myocardial defects caused by rheumatism;
- myocardial infarction or cardiosclerosis.
- No less common causes are drug poisoning caused by exceeding the dosage of certain drugs: quinidine (against arrhythmia), Corinfar, verapamil, digitalis and a number of others. Digitalis preparations are especially dangerous for heart blockades of any kind.
- Incomplete blockade often occurs in completely healthy people. Most often it is caused by overexcitation of the vagus nerve, which is caused by increased stress during training or physical work.
- There have been cases of congenital blockade that occurs as a result of pathology of intrauterine development. In this case, newborns are diagnosed with heart defects, etc.
- Blockade can also be caused by certain types of surgical interventions used to eliminate various heart defects and other anomalies.
Symptoms
Often this disease is asymptomatic. If any signs of intraventricular block occur, they are due to the underlying pathology that led to this block. For example, with myocardial ischemia, headaches appear, usually in the back of the head, and chest pain. Myocarditis is manifested by shortness of breath and chest discomfort.
If a patient exhibits intraventricular block on the ECG, which is accompanied by certain suspicious complaints, the patient should be urgently examined for cardiac pathologies.
Transverse
Transverse (atrioventricular) blockade implies a violation of the conduction of impulses along the pathways between the atria and ventricles. Such blockade can occur randomly or at regular intervals, and can also be of varying duration.
In accordance with the characteristic elements of electrocardiograms and the totality of symptoms, the pathological process is usually divided into 3 types of transverse (AV) blockade:
- 1st degree - atrioventricular conduction through the AV node is slow, but all impulses from the atria are able to reach the ventricles;
- 2nd degree - incomplete, in which atrial impulses selectively reach the ventricles (there are three types according to Mobitz);
- 3rd degree - complete, in which the passage of impulses completely stops.
The totality of symptoms appears only with complete blockade. In other cases, the main organ of the cardiovascular system miraculously adapts so much that the patient practically does not feel any abnormalities.
Signs of complete AV block develop sequentially:
- the patient suddenly experiences a panic attack;
- an “illusion of movement” appears in the head;
- the patient may lose consciousness;
- the skin of the face first turns red and then turns pale;
- rhythmic movements of the arterial walls cannot be felt;
- breathing becomes rare but deep;
- facial spasms spreading to the musculoskeletal system;
- pupils increase in diameter;
- spontaneous act of defecation and urine discharge.
The monitor's sensors are attached to the chest. The examined patient leads a normal, habitual lifestyle. The device continuously records ECG throughout the day, which is then analyzed. This allows us to determine the frequency of blockades, their dependence on the time of day and the patient’s physical activity. Decoding what is recorded on the cardiogram helps to make the correct conclusion.
If the examination showed the transition of the 1st degree of AV blockade to the 2nd degree according to the 2nd type (Moritz 2) into a partial (or complete) block of the 3rd degree, then this means that the patient requires mandatory treatment. The main method of restoring normal heart function is to implant a permanent or temporary pacemaker (PAC) into the patient. Temporary electrical stimulation is necessary, for example, in case of acute heart block resulting from myocardial infarction.
Only when cardiac pathology is detected is individually selected therapy carried out, which can also affect the frequency of blockades. In any case, if any blockades have been diagnosed, then this is a signal from the underlying disease. Such patients should have a cardiogram done at least once every 6 months and be registered with a cardiologist.
Attention in case of complete blockade
Particular attention should be paid to complete blockade if it occurs for the first time and is also accompanied by pain in the left half of the chest or sternum area. The fact is that it is almost impossible to recognize a complete left blockade on a cardiogram. For this reason, if a complete left blockade occurs, which is accompanied by burning or pressing pain in the chest, the patient must be checked for acute myocardial infarction and hospitalized as quickly as possible in a cardiology hospital.
Nonspecific intraventricular block, as a rule, also does not cause discomfort in the patient, but in most cases is accompanied by symptoms that can be attributed to the causative disease.
Sinoatrial
Sinoatrial or sinoauricular block is a lesion of the sinus node in the area of the right atrium. There is a violation of the rhythm of contractions, in which complete contraction of the entire heart muscle occurs. Such a pause can double the time interval between contractions. The frequency may be random or sequential.
This violation is designated CA. It affects females slightly more often than males after the age of 50. It is usually divided into the following types:
The totality of manifestations of pathology depends on the type of SA blockade:
- Degree I disorders are asymptomatic, without objective changes in the functioning of the heart.
- If the pathology has a II degree of manifestation, then disturbances in the vestibular apparatus and interruptions in the functioning of the heart may be observed (untimely depolarization and contraction of the heart or its individual chambers or a pronounced reduction in heart rate).
- A complete blockade can occur in 2 scenarios. In the first case, if the atrioventricular connection becomes the part of the heart muscle in which the impulses that determine the heart rate are generated, then patients may not feel rhythm disturbances at all. And when the AV connection does not manifest itself, then with a short third-degree SA blockade, loss of consciousness can occur, and with a long one, sudden death can even occur.
The prognosis of the pathological condition depends on the probable causes of its occurrence, the duration of the attack, the type of blockade and the general condition of the patient’s cardiac activity. In general, sinoauricular lesions are considered less dangerous than those that occur due to AV conduction disorders.
Diagnostics
In most cases, a diagnosis of this blockade can only be made by doing a cardiogram. A sign of right intraventricular block on the ECG is an expanded and altered M-shaped complex. In this case, a jagged and deep tooth is observed along the left branches. Complete blockade differs from incomplete blockade in the duration of the complex. With complete blockade, the complex will be more than 0.12 s, and with incomplete blockade, it will be lower than this indicator.
A sign of left intraventricular block on an ECG in an adult will be a deformed and dilated ventricular complex along the left chest leads. On the right, a jagged tooth is revealed.
Atrioventricular block
Signs of 1st degree atrioventricular block are prolongation of the PQ interval by more than 180 ms (for adult patients). Atrioventricular block of the 2nd degree is the loss of part of the ventricular complexes. If the loss is preceded by a gradual lengthening of the PQ interval, this is called the Samoilov-Wenckebach periodicity. The next degree of impairment of AV conduction is 3rd degree AV block (AV dissociation), in which the atria contract in one rhythm and the ventricles in another.
↓Atrioventricular block 1st degree. Atrial P waves begin immediately after T waves, and the duration of the PQ interval is impressive.
↓Episode of 2nd degree AV block without Samoilov-Wenckebach periodicity (equal PQ intervals before loss of QRS). “Lonely” P wave without subsequent QRS complex. Escaping contraction from the AV node after blockade (there is no atrial P wave before it). And also - early repolarization syndrome.
↓An episode of 2nd degree AV block with Samoilov-Wenckebach periodicity - a gradual lengthening of the PQ interval before the QRS loss and a return to normal PQ after the loss are visible.
↓Picture of 3rd degree AV block (AV dissociation): atrial P waves occur at one frequency, and ventricular complexes from the AV node are at a completely different frequency. Note the third QRS complex. The atrial P wave is between the complex and the T wave. The maximum PQ interval in this recording is 1.15 seconds.
Local blockade of terminal branches
Local terminal branch block, also called local intraventricular block, may also develop. This type is usually caused primarily by an acute infarction. Focal intraventricular block is characterized by an acute “damage block”, which is represented by necrotic cardiomyocytes. They occur when there are obstacles in the path of electrical impulses, and there is a lack of growth of the R wave towards the fourth thoracic branch.
Intra-infarction local intraventricular block is formed directly inside the zone of myocardial necrosis, manifested by splitting of the pathological Q wave. They are observed in leads that are most characteristic of the affected area. Finally, peri-infarction local intraventricular block on the ECG in an adult can be determined by the focus of cardiomyocyte necrosis. It appears as a jagged and deformed tooth.
It is important to remember that with local intraventricular blockade, it is impossible to see the Q wave on the ECG. Its appearance clearly indicates the presence of acute myocardial infarction, which is veiled on the cardiogram by this very blockade.
Intraatrial block
Normally, the electrical signal from the pacemaker to the AV node travels quite quickly. An obstacle slows him down. On the electrocardiogram, this is manifested by a change in the P wave (widening). There may be no other anomalies. Intraatrial block has the same severity as sinoatrial block. Its main criterion is a P-wave exceeding 0.1 s.
The ECG showed complete intraatrial block. The contraction of the atria and ventricles is noticeable, taking place in their own rhythms.
Visualization of intraatrial conduction disturbances on the cardiogram:
| Graphic image on a cardiogram | The pathology that caused the change | Characteristic signs |
| Intraatrial block I degree | The atrioventricular node suffers slightly, slowing down the conduction of impulses. PQ segment is extended, PQ interval exceeds 0.2 s | |
| Type 2 intraatrial block II degree | The AV node cannot conduct all electrical signals. Absence of QRS complex. All PQ segments are the same (normal or extended). At the point where the impulse drops, RR is twice as large as during the previous contraction | |
| 1 type of intra-atrial block II degree | The AV node “gets tired” gradually. There are several contractions during which the atrioventricular node does not work at full strength. Before the QRS complex drops out, the PQ interval gradually lengthens. The PP interval is the same everywhere | |
| Intraatrial block of the third degree | The AV node stops conducting electrical signals. The ventricles and atria work in different rhythms. For the ventricles, it is set by the AV node. There is no pattern between QRS and P. The P wave can abut the QRS complex and merge with the T wave. Heart rate is correct |
Additional examinations
When diagnosing a blockade, the patient usually requires additional examinations. For accurate and correct diagnosis, cardiologists are recommended to use one or all three of these methods.
Ultrasound of the heart or echocardioscopy. This procedure is prescribed if there is a suspicion of myocarditis, heart disease, or myocardial infarction. If the patient denies the fact of hospital treatment, an Echo-CS is considered mandatory, since otherwise the patient may suffer a heart attack on his legs, which will have a fatal impact on his health.
Another method is coronary angiography. It is done to evaluate in detail the patency of the coronary arteries, and also to determine whether there is a need for bypass surgery or stenting.
Finally, 24-hour Holter ECG monitoring is often prescribed. It is especially useful in case of unstable blockade. This may be due to tachydependent blockade, that is, tachycardia, which manifests itself and worsens during physical activity.
Does the blockage need to be treated?
Considering that this disease is often asymptomatic and does not always indicate cardiac pathology, many wonder whether it is worth treating it at all.
According to the recommendations of doctors, treatment of blockades of this type is required only if the patient actually has a pathology of the cardiovascular system, which leads to this problem.
For example, in case of acute myocardial infarction, surgery or therapy using conservative methods is recommended. In the latter case, nitroglycerin analogs, pain relief with narcotic analgesics, and massive antiplatelet and anticoagulant therapy are prescribed. If myocarditis is established, anti-inflammatory therapy is carried out, and for cardiosclerosis, cardiac glycosides and diuretics are prescribed, especially if the disease develops against the background of chronic heart failure.
When the cause of the blockage is a heart defect, surgical correction is necessary.
Sinoatrial blockade
Strictly speaking, it is impossible to accurately prove the fact of sinoatrial block (failure to conduct an impulse from the sinus node to the atria) due to the absence of ECG events. An indirect sign is an increase in RR quite exactly twice as compared to the previous one and the absence of a P wave at the moment of the pause. Sinoatrial blockade differs from the Holter recording of pronounced sinus arrhythmia according to the rhythmogram (after the blockade, RR becomes the same, and with sinus arrhythmia it decreases gradually.
↓Presumably an episode of sinoatrial block (look at the heart rate numbers at the top of the picture).
↓Another presumptive episode of sinoatrial block (look at the RR duration numbers at the top), after which first-degree atrioventricular block occurred (prolongation of the PR interval).
The danger of blockade
It is worth understanding that not every intraventricular block poses a real danger. For example, if it is incomplete and single-bundle, then you should not pay attention to it at all, especially if it is not provoked by any underlying disease.
A two-bundle block in most cases transforms into a three-bundle block. The latter leads to complete blocking of conduction between the ventricles and atria. In this case, seizures and loss of consciousness are possible. In this situation, the patient's life is at risk. There is a possibility of sudden cardiac arrest and death.
Double-bundle bailey block. DOUBLE BAND BLOCK
DOUBLE BUNCH BLOCK - disruption of the conduction of supraventricular impulses. occurring when 2 bundle branches are affected. Etiology and pathogenesis Excitation emanating from the Gavar node passes through the common trunk and 2 branches of the His bundle and through the branches of the Purkinje fibers. Excitation spreads from the internal to the external parts of the heart in directions perpendicular to the walls. The interventricular septum is activated on both sides, right and left, in the direction from the endocardium inward. In the area of the bundle branches and their branches, lesions are rarely observed. The cause of severe disturbances in the conduction of the His bundle is its organic change in rheumatism, diphtheria myocarditis, and atherosclerosis of the arteries. feeding bundle, syphilitic myocarditis, myocardial infarction. When the His bundle completely loses conductivity, there is a pause in the activity of the ventricles. Clinic Usually in these cases, impulses to contraction are generated in the remaining entire segment of the bundle, resulting in an independent ventricular rhythm: 1) slow (30-40 contractions per minute); 2) correct; 3) almost independent of extracardiac innervation influences. At this time, the atria continue to contract at their own rhythm, more frequent. This is called complete atrioventricular dissociation, or complete block. Complete atrioventricular block may be asymptomatic. Most often, patients experience palpitations, dizziness, and fainting. On auscultation, a systolic murmur is heard, sometimes a cannon tone. Diagnostics is carried out on the basis of ECG, FCG and SV studies. Treatment The underlying disease is treated.
Possibility of death
Therefore, one should be most wary of double-bundle His blockade, which is combined with symptoms of the underlying cardiac disease. In this case, it is necessary to closely monitor the patient's condition, as there is a possibility of death.
If signs of second or third degree AV block appear on the cardiogram, the doctor decides to install a pacemaker. It is important that it be implanted even in patients who do not experience serious attacks, since their lives are still at risk.
It should be noted that, in addition to AV block, intraventricular problems of this nature cause ventricular fibrillation, ventricular tachycardia, which can also lead to a fatal outcome.
Prevention
In this case, a method of preventing sudden death from heart disease due to rhythm disturbances is actively practiced.
Essentially, this type of prevention consists of regular visits to a cardiologist, an electrocardiogram, as well as a timely and prompt decision on the implantation of a pacemaker if necessary.
As a preventive measure against this disease, as well as in order to generally reduce the likelihood of cardiovascular pathologies, it is recommended to avoid unpleasant stressful situations in life, completely stop drinking alcoholic beverages and smoking, strive to lead a healthy lifestyle, and engage in moderate exercise and sports.
You should definitely take medications, but under no circumstances self-medicate, following the recommendations of your doctor in everything.
Visit to the doctor
After a heart attack or other serious cardiac pathology, it is necessary to regularly visit a cardiologist, at least in the first six months. This will allow you to record your condition, identify complications, if any, and promptly eliminate them.
Separately, it is worth noting that any type of this blockade at the initial stage requires increased attention and mandatory consultation with your doctor.
First of all, you should go to a therapist or cardiologist, who can guide you on whether you really should be afraid of this disease, what examinations to undergo, and how to structure your therapy. After all, as we have already noted in this article, this disease can be either completely harmless or seriously threaten your life and health. In the latter case, hospital treatment, possibly surgical intervention, will be required.