Defects of the cardiovascular system are mostly invisible to the patient. But up to a certain point. Many diagnoses are made after the fact, after an autopsy. Some diseases do not produce any symptoms at all and do not affect the anatomical state of the muscle organ.
Sinoatrial block is a disruption of the movement of electrical impulses from the natural pacemaker (sinus node) to the underlying chambers of the heart (atria and ventricles). Several structures of the heart are involved at once, hence the generalized disruption of its functioning.
The signal does not reach the ventricles, so they contract incorrectly (beats are skipped).
With prolonged damage, ventricular fibrillation develops: chambers that do not receive an external impulse begin to generate it independently. This can be fatal in the short term.
Treatment is carried out under the supervision of a cardiologist, preferably in a hospital until all the nuances are identified. Full recovery presents some difficulties: more often, sinoatrial blockade acts as a secondary pathology, occurring against the background of other diseases.
The correct treatment regimen is a simultaneous impact on the cause and symptomatic component.
The essence of the violation
In the normal state of affairs, the muscular organ works autonomously and does not need external stimulation. Uninterrupted functioning is ensured by the presence of a special accumulation of active cardiomyocyte cells - the sinus node. It is located in the right atrium.
The job of this anatomical structure is to generate an electrical impulse that causes the other chambers to contract.
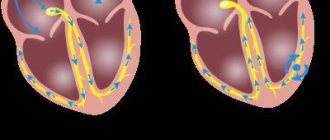
With sinoatrial (SA) blockade, the generation or propagation of an impulse into the underlying chambers of the heart is disrupted. The result is the impossibility of proper stimulation of the ventricles.
Since they do not receive the necessary command, a full reduction does not occur either. The body strives to compensate for this situation. The cameras begin to produce a signal themselves and become spontaneously excited.
But on the one hand, the intensity is not enough for a high-quality release of blood, on the other, the ventricles stop coordinating actions.
The contractions turn out to be chaotic and disorderly. Fibrillation develops, which most likely leads to cardiac arrest.
Another point is the excessive activity of the sinus node itself. This is another compensatory mechanism. The organ begins to produce impulses more often in order to somehow reach the ventricles.
As a result, a patient with advanced sinoatrial block has a history of two dangerous processes: tachycardia as a result of excessive work of the natural pacemaker and fibrillation.
It is difficult not to notice these signs, so diagnosis is prescribed in relatively early stages. Although the situation described is not always so critical. A patient can live with the pathology for years without even suspecting any problems.
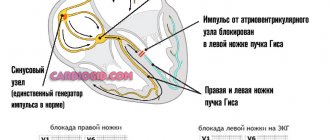
How does the conduction system work?
Conduction system of the heart
This system is represented by a complex of fibers and nodes consisting of specific cells that set the “rhythm” of the entire muscle tissue. It is in these cells that the impulse is generated, and along the underlying fibers and nodes of the conduction system it spreads from the atria to the lower cardiac chambers - the ventricles. Node of the conduction system No. 1 is the sinoatrial or sinus node. It is located in the right atrium. In a healthy heart, normally it is in this node that impulses arise, which then spread through the underlying nodes and tracts throughout the organ. The generation of impulses by the sinus node with a frequency of 60-80 beats per minute is the norm.
From the sinoatrial node, impulses enter the AV node, located between the upper and lower cardiac chambers. In this area, the impulses are delayed by hundredths of a second and further propagate to the underlying cardiac sections - the His bundles and Purkinje fibers. In a healthy organ, only one node of the conduction system is active - the sinoatrial one. The remaining components of the conduction system diligently “follow” instructions to conduct impulses at the frequency specified by the sinus node. When the main pulse generator fails, its responsibilities are assumed by the AV node.
Classification and degrees
Typing is carried out according to the severity of the condition.
- SA blockade 1st degree. Represents the initial phase of the disease. There are no symptoms as such, there are no changes in well-being. The patient is active and goes about his daily activities.
It is possible to detect problems during sports, especially at a professional level. Excessive load leads to increased heart rate, impaired myocardial contractility, and chest discomfort.
Additionally, intense shortness of breath and loss of consciousness similar to superficial fainting are detected. After rest, everything falls into place. The objective picture consists of a slight drop in blood pressure and heart rate.
- 2nd degree SA block is an incomplete disruption of impulse conduction. Contractility is still normal, the activity of the sinus node is normal or slightly reduced.
At this stage, severe tachycardia occurs, but the reverse process is also possible. Shortness of breath, sleep disturbances, poor exercise tolerance. All these are moments inherent in pathology.
Depending on the ECG pattern, two types of the described condition are distinguished:
SA blockade 2nd degree, type 1 - the graph reveals chaotic transmission of contractions, usually two or more in a row, possibly with an increase in the impulse conduction time (Samoilov-Wenckebach periods). Clinically, this form is especially dangerous, since it more often causes spontaneous cardiac arrest without the possibility of urgent resuscitation using routine methods.
SA blockade 2nd degree, type 2 - there are no beats symmetrically: there is an alternation of normal contraction and its omission.
- Sinoauricular block of the 3rd degree is considered terminal stage. It takes from several months to years to develop, depending on the aggressiveness of the condition and its underlying cause.
Electrocardiography shows weak contractions. In severe cases, the indicator degenerates almost into a straight line. There is a high risk of asystole or cardiac arrest. This can happen at any time.
The patient needs to be hospitalized urgently. Third degree sinoatrial block is extremely difficult to treat. Radical measures are required. If you are lucky and there are no abnormalities in other organs yet, transplantation will help, which in itself is difficult to implement due to the lack of donors.
At its core, sinoatrial block is a type of sick sinus syndrome. It is similar to bundle branch lesions in both manifestations and prognosis.
But it flows much more aggressively, gives more complications and carries great danger, since the disorder affects both ventricles at once, and at stages 2-3 the atria also suffer.
Reasons for development
In young people, such conduction disturbances may be associated with increased excitability of the vagus nerve and the predominance of the parasympathetic system. During daily ECG monitoring, pauses are detected, usually during sleep. This condition is not life-threatening, but can limit the professional suitability of a young person.
Extracardiac causes of pathology:
- damage to the sympathetic or parasympathetic nerve trunks during operations on the chest or abdominal organs;
- brain tumor;
- intracranial hypertension (increased cerebrospinal fluid pressure in the cavities of the ventricles of the brain);
- hypothyroidism (insufficient production of thyroid hormones);
- progressive liver diseases (hepatitis or cirrhosis);
- hyperkalemia (increased potassium concentration in the blood, for example, with renal failure).
SA blockade can be caused by heart diseases:
- ischemic cardiomyopathy caused by ischemic heart disease or the consequences of myocardial infarction;
- myocarditis;
- pericarditis;
- myocardial amyloidosis (impregnation with protein masses, for example, in chronic osteomyelitis);
- age-related changes associated with atherosclerosis of the coronary vessels.
This rhythm disturbance is one of the manifestations of sick sinus syndrome (SSNS). The disease is accompanied by a disruption in the production of normal impulses, a slow heartbeat, attacks of tachycardia and the formation of long pauses.
Sinoauricular block can be caused by an overdose of the following medications:
- digoxin;
- quinidine;
- beta blockers;
- verapamil.
In many cases, it is not possible to determine the exact cause of the pathology.
Causes
Development factors are always cardiac. On the one hand, this makes diagnosis easier. On the other hand, it initially worsens the prognosis.
- Poisoning with phosphorus compounds. Usually these are mineral fertilizers. Patients working in hazardous chemical plants are especially at risk. Once the dangerous factor is eliminated, the likelihood of restoring normal health is almost maximum.
Patients with acute intoxication should be immediately hospitalized for specific treatment measures. The prognosis in this case is relatively favorable.
- Congenital and acquired heart defects. What kind doesn't play a big role. This may be stenosis, prolapse of the mitral, aortic valves, disturbances in the anatomical development of the septum and other conditions.
The problem is that it is extremely difficult to detect them if you do not contact a cardiologist every six months or a year for a routine examination.
Findings are mostly accidental, because pathological processes are detected already at irreversible stages. Some cases are even dealt with after the fact, when the person has died.
Sinoatrial blockade of this type is relieved as part of the main surgical treatment.
- Drug overdose. It’s ironic, but drugs designed to lower blood pressure and eliminate arrhythmia, that is, medications aimed at improving the heart, can kill the patient in a matter of hours.
Amiodarone, Quinidine, Digoxin, glycosides in general, and beta blockers are especially dangerous. Third-party drugs include psychotropic drugs, including antipsychotics, antidepressants, and tranquilizers.
It is possible to provoke a similar effect due to the use of oral contraceptives. All drugs should be prescribed only by a specialist after a thorough diagnosis.
- Myocarditis. Inflammation of the heart muscle. It is an infectious, less often autoimmune disease. Requires urgent medical care in a hospital.
Such a dangerous condition cannot be treated on an outpatient basis, since complications are possible, including a heart attack or cardiac arrest. Antibiotics are used in loading doses or immunosuppressants.
As a rule, the condition is secondary. Develops as a complication of colds, rheumatism and others. Sinoatrial blockade after severe myocarditis does not go away on its own.
- Vegetovascular dystonia. Strictly speaking, it does not apply to cardiac problems. However, the normal innervation of the cardiovascular system is disrupted. Hence the deviations in the conductivity of the electrical impulse.
It is a complex symptomatic complex. It manifests itself in many ways: from tachycardia, to dizziness, fainting, shortness of breath and others.
It is not considered an independent diagnosis; you need to look for the cause of this condition. Usually we are talking about hormonal imbalance or pathologies of the cerebral structures themselves.
- Rheumatism. Autoimmune damage to cardiomyocyte cells. The body's protective forces, designed to cover the body, destroy its own tissues. The reasons for this deviation are not fully known. However, rheumatism quite quickly destructs cardiac cells, causing severe scarring and severe heart failure with sinoatrial block.
- Myopathy. Proliferation of the muscle layer, as well as dilatation (expansion) of the chambers of the heart. Restoration is not possible due to the anatomical nature of the deviation. Maintenance therapy under the supervision of a specialist is required. Read more about cardiomyopathy and its types in this article.
- Heart attack and, as a consequence, scarring of the affected areas (cardiosclerosis). It ends with a significant decrease in the conductivity of the natural pathways of electrical impulses. Treatment is required urgently. There is always a risk of death.
In completely healthy people, sinoatrial blockade is also possible. Spontaneous, transient, and transient SA blockades are a consequence of increased activity of the vagus nerve.
Such conditions can be dangerous, but they last only a few minutes, half an hour at most. Patients with no cardiac history and no organic abnormalities in the objective picture are observed by neurologists.
Attention:
There is a chance that the first attack will be the only one, but it is not great. Most likely, we are talking about a disruption of the brain or endocrine system.
In the absence of data for pathologies and functional disorders, they generally speak of an idiopathic form of sinoatrial block. This is a relatively rare option. Typically, diagnostic problems do not arise due to the obviousness of the underlying process.
Treatment options
The first stage blockade is practically harmless, but requires constant monitoring. Sinoauricular blockade 2nd degree, type 2 and 1, as well as 3rd degree - treatment. In the presence of primary pathology, impaired hemodynamics - anticholinergics (Atropine, Saracin, Metacin, Platyfillin), sympathomimetics (Ephedrine, Isoprenaline, Orciprenaline) and nitrates (Olicard, Monizol, Erinit, Nitroglycerin), partial cardiac pacing.
To improve metabolism in the heart muscle - adrenomimetics (Inosine, Cocarboxylase, Isadrin, Mezaton). Therapy with diuretics and hormonal agents is used.
In case of persistent blockade or deterioration of the condition during conservative treatment (pulse below 40, severe depression of consciousness, constant fainting and other signs of heart failure, clinical death), installation of a pacemaker.
Mezaton improves metabolism in the heart, alleviating the condition
If the blockade occurs while taking medications, then their immediate withdrawal and supportive therapy and detoxification of the body are necessary. Temporary electrical stimulation is acceptable, as in myocardial infarction.
If a sudden, but unexpectedly acute blockade occurs, resuscitation is performed: chest compressions and pulmonary ventilation, temporary cardiac stimulation, injection of Atropine and (or) Adrenaline.
The use of β blockers, glycosides and antiarrhythmic quinidine drugs is prohibited!
In addition, some of the approved drugs have many adverse reactions and the risk of individual intolerance to the components, causing ectopic arrhythmia. Therefore, they require strict medical supervision!
Not all medications can be used, so do not take anything without a doctor's prescription
Stage 1 symptoms
At an early stage, there are no manifestations at all or they are scanty. The clinical picture consists of two signs:
- Severe shortness of breath. But only after intense physical activity. The average person is not active enough to notice a deviation from the norm. In part, problems can be suspected based on the results of specialized tests (bicycle ergometry), but such a test is prescribed only when indicated.
- Tachycardia. Acceleration of the heart rate due to excessive generation of an electrical impulse, against the background of incomplete conduction of the signal to the ventricles. The compensatory mechanism is activated. But he is initially flawed, unable to influence the state of things. Both signs are revealed only after intense physical exertion. An ordinary person does not notice the problem, so diagnosis at stage 1 is almost impossible.
Degrees of sinus node blockade
Samoilov-Wenckebach periods
In medicine, there are three degrees of sinoatrial blockade.
I - with the first degree of SA blockade, all impulses from the node pass to the upper cardiac chambers, but more slowly than normal. On an ECG, such a blockade does not manifest itself in anything special; an indirect sign that allows one to suspect a blockade is constant sinus bradycardia - a slowdown in the rhythm.
II - sinoatrial blockade of degree II is characterized by the fact that some impulses from the center of automatism of the 1st order do not cause excitation of the lower cardiac chambers. Omissions of the QRS complex appear on the cardiogram. Periods of a flat line equal to a distance of 2 RR are visualized—the Samoilov-Wenckebach periods. The second degree of SA blockade, in turn, is divided into 3 types, which are characterized by distinctive ECG signs that are accessible to the experienced eye of a functional diagnostics doctor.
III - third degree SA block is characterized by the fact that not a single atrial impulse is conducted to the underlying cardiac tissue. This condition is called complete blockade of the sinoatrial node. The cardiogram shows a long pause, similar to a complete stop of the SA pacemaker. Complete SA blockade can lead to asystole and death of the patient. In some cases, if the first-order pacemaker fails, the AV connection takes on a replacing and dominant role, while the rhythm from the 2nd-order source of impulse is recorded on the ECG.
Symptoms at stages 2-3
Phases 2-3 are accompanied by a number of gross changes in condition:
- Chest pain. Pressing or burning. Unlike angina, the episodes are so small that the patient does not have time to pay attention to them. Discomfort is described as a momentary unpleasant sensation that immediately disappears. Duration - from a couple of seconds to several minutes.
- Dyspnea. Against the background of minimal physical activity or at rest. It is extremely difficult to tolerate, the patient is unable to work or perform daily duties. Even going to the store becomes akin to achievement. It is difficult to correct the condition. Usually such patients are given a disability group.
- Heaviness in the chest. It feels like a huge stone has been sewn up.
- Tachycardia and the reverse process. Increase and decrease in heart rate. One may be replaced by another. In parallel, other arrhythmias occur. Ventricular fibrillation. The number of movements reaches 300-400, but they are visible only on electrocardiography.
- Cyanosis of the nasolabial triangle.
- Increased sweating, especially at night.
- Paleness of the skin.
- Fainting may occur more than once during the same day.
- Headache.
- Vertigo, inability to navigate in space.
- Weakness, drowsiness. Long-term decline in labor activity.
- Apathy, unwillingness to do anything.
Sinoatrial blockade of the 2nd degree is accompanied by all the described manifestations, but treatment still has promise.
Symptoms of pathology
1st degree SA blockade has no clinical manifestations.
Second degree sinoauricular block is usually well tolerated by the patient. Sometimes the patient complains of a feeling of interruptions, a sinking heart, and slight dizziness. Clinical symptoms are associated primarily with the underlying disease (eg, myocarditis).
With complete SA blockade, attacks of weakness, dizziness, and sudden loss of consciousness may occur. In such cases, doctors decide to implant a pacemaker in the patient.
Diagnostics
It is carried out under the supervision of a cardiologist. A group of techniques is assigned:
- Oral questioning of the patient and collection of anamnesis. A way to objectify complaints, formalize symptoms and create a clinical picture.
- Measurement of blood pressure, heart rate.
- Daily monitoring using a special tonometer. Allows you to evaluate both heart rate and blood pressure over 24 hours in natural conditions for the patient.
- Electrocardiography. Study of functional indicators. Used as a basic measure.
- Echocardiography. Ultrasound method of tissue visualization. Defects are diagnosed in this way.
- General blood test, hormones and biochemical.
- MRI as indicated.
As part of an extended examination, a neurologist is involved. It is also possible to schedule a consultation with a specialist who works with hormonal imbalances.
Causes of sinoatrial block
Among the main mechanisms of sinoauricular blockade are damage to the node itself, disruption of the propagation of impulses through the heart muscle, and changes in the tone of the vagus nerve.
In some cases, the impulse is not formed at all, in others it is there, but too weak to cause contraction of cardiomyocytes. In patients with organic damage to the myocardium, the impulse encounters a mechanical obstacle in its path and cannot pass further along the conducting fibers. Insufficient sensitivity of cardiomyocytes to electrical impulses is also possible.
Factors leading to sinoauricular block are considered:
- Heart defects;
- Inflammatory changes in the heart (myocarditis);
- Cardiovascular form of rheumatism;
- Secondary damage to heart tissue due to leukemia and other neoplasms, injuries;
- Coronary heart disease (cardiosclerosis, post-infarction scar);
- Myocardial necrosis (infarction);
- Cardiomyopathy;
- Vagotonia;
- Intoxication with drugs when the permissible dose is exceeded or individual intolerance - cardiac glycosides, verapamil, amiodarone, quinidine, beta-blockers;
- Organophosphorus poisoning.
The operation of the SA is influenced by the activity of the vagus nerve, therefore, when it is activated, impulse generation may be disrupted and SA blockade may occur. Usually in this case they talk about transient SA blockade, which appears on its own and goes away in the same way. This phenomenon is possible in practically healthy people, without anatomical changes in the heart itself. In isolated cases, idiopathic sinoauricular block is diagnosed when the exact cause of the pathology cannot be determined.
In children, conduction disturbances from the sinoatrial node are also possible. Typically, such arrhythmia is detected after 7 years of age, and a common cause is autonomic dysfunction, that is, the blockade is more likely to be transient, against the background of increased tone of the vagus nerve. Among the organic changes in the myocardium that can cause this type of blockade in a child are myocarditis, myocardial dystrophy, in which, along with SA blockade, other types of arrhythmias can be detected.
Signs on ECG
At the first stage there are no changes. Problems cannot be detected. Or the features are so nonspecific that they do not give an idea of the nature of the process.
Grade 2 reveals the most pronounced changes on the ECG:
- Passing several pulses in a row at once. Objectively manifested by the complete absence of PQRST complexes on the graph. This is type 1.
For the 2nd, alternating loss of contractions is typical. Yes, no, and so on. Inadequate movements may occur and appear as minor waves.
- PP extension.
- Acceleration or deceleration of the intensity of work of a muscle organ.
SA blockade on the ECG has features of tachycardia or bradycardia and uneven contractile activity.
The third stage is accompanied by impaired functional activity. The graph degenerates almost into a straight line.
Diagnostic methods
Sinoatrial block is diagnosed on an ECG (electrocardiogram). However, the first stage cannot be defined in this way. Only a slightly abnormal heartbeat (less than normal), that is, a low pulse, can give it away. The only way is auscultation (listening).
At stages 2 and 3, the electrocardiogram shows a number of specific changes. Sinoatrial block 2nd degree: loss of one or more cycles. At the same time, in type 1, there is a shortening of the PP interval with a final pause (shorter than the square of the PP interval) due to the mature blockade. Equal intervals are gradually established, which appear on the cardiogram as the loss of the P wave and the QRS complex. In type 2 – sharp and prolonged pauses (extended interval) against the background of normal equal PP intervals. The ratio can be 2:1 or 3:1, sometimes 5:1 (far gone).
One of the diagnostic options is recording ECG indicators for 72 hours
At stage 3, the ECG shows a slow replacement rhythm. Electrophysiological methods help to more accurately determine pathology.
Diagnostic methods also include:
- Daily ECG monitoring. Lasts at least 72 hours. Allows you to record the slightest fluctuations and changes in the heart rhythm at any time. Used when ECG results are negative, but there is still suspicion of sinoatrial block.
- Atropine test. A drug (1 gram of 0.1% solution) is injected into the body, causing the heartbeat to double (provided the disease is present), and then decrease by the same amount, ending with a blockade. The second degree (when the work of the sinus node is still preserved) is characterized by a gradual increase in frequency. Before and after drug administration, a baseline and control ECG is performed, respectively.
- Additionally, ultrasound is used. It can be used to determine heart defects and other inflammations, muscle size and features (scars).
You also need to do an additional ultrasound of the heart.
Treatment options
The main method of correcting the condition is surgical. Implantation of a pacemaker is indicated, which will artificially control the rhythm.
Medication is a temporary measure and its effect is incomplete.
During acute attacks against the background of autonomic, nervous dysfunction, the following are prescribed:
- Nitroglycerine.
- Atropine or Amizil.
The drugs cannot be abused; they provoke dangerous forms of arrhythmias when used in excess.
In the long term, vitamin and mineral complexes with sufficient amounts of magnesium and potassium, and cardioprotectors (Mildronate) are prescribed.
Attention:
The use of antiarrhythmic drugs is strictly not recommended, as the condition is likely to worsen.
Treatment of pathology
SA blockade of the 1st and 2nd degrees does not require treatment. Treatment is carried out for the disease that caused conduction disturbances.
Treatment of 3rd degree sinoauricular block includes 3 stages:
- therapy of the leading disease;
- taking medications;
- pacemaker implantation.
For suddenly developed SA blockade, atropine is used. This medicine suppresses the activity of the parasympathetic nervous system, speeds up the heartbeat, and increases the efficiency of blood circulation. Ephedrine and norepinephrine stimulate the sympathetic nervous system, increasing heart rate and improving blood flow. These medications are used as emergency measures only.
The main treatment method for 3rd degree SA block is implantation of a pacemaker. It is placed under the skin of the chest and its electrodes are inserted into the heart. They produce electrical impulses, replacing the normal functioning of the sinus node. Cardiac stimulation allows you to completely eliminate the manifestations of arrhythmia.
Forecast
Relatively favorable against the background of systematic drug treatment.
If a pacemaker is implanted and the operation is successful, survival rate increases dramatically to 90-95% over a period of 10 years or more.
Lack of therapy is associated with an almost 100% chance of death within a short period of time.
The pathological process cannot always be cured surgically. For some patients, with severe heart defects, severe concomitant conditions, or old age, surgery may be contraindicated.
However, the chance cannot be neglected. First they try to stabilize the patient, then they still consider radical intervention. Otherwise there is no chance of recovery.
"Failure" of the SA node. Reasons for the blockade
Sinoatrial blockade
Conditions in which there is difficulty in conducting the impulse and a decrease in its production at the level of the SA node are called sinoatrial block. Blockade of impulses at the very beginning of the path can develop with:
- insufficient production, low frequency of impulse production directly in node No. 1 - sinus;
- low impulse strength, which is not enough to cover the atria with excitation and subsequent spread to the underlying nodes;
- blocking the normal impulse by the sinus node and the right atrium.
Cardiac ischemia
All causes of damage to the sinoatrial node can be divided into three main groups:
- Primary. “Breakage” of the node that occurs against the background of its organic lesions, the consequence of ischemic disease, a previous heart attack, the influence of drugs (cardiac glycosides, quinidine, tricyclic antidepressants, Li salts, AK, clonidine) or toxic factors, inflammatory processes in the heart muscle. Primary damage to the sinus node is caused by systemic lesions of the connective tissue, myocardial fibrosis, systemic vasculitis, ankylosing spondylitis, muscular dystrophy, surgical interventions on the lungs and chest, thyrotoxicosis, diabetes mellitus.
- Secondary. Associated with dysfunction of the autonomic nervous system with an excessive increase in n.vagi activity. A physiological increase in the vagus can be observed during sleep, coughing, vomiting, and straining. Physiological changes do not lead to the occurrence of sinoatrial block. This condition can be caused by pathological activity of the vagus nerve with a hiatal hernia, esophageal diverticulum, stroke, brain tumors, disturbances in the electrolyte composition of the blood with an increased concentration of K, sepsis, hypothyroidism, hypothermia.
- Idiopathic. Cases of sinoatrial blockades are characterized when it is impossible to find out the exact cause of their occurrence, in which case they are called idiopathic. Signs of diseases of the heart and other conduction systems cannot be detected with such damage to the SA node.
Heart blocks in children
A B C D E F G H I K L M N O P R S T U V
Heart block in children is a disorder that occurs when conductor cells of the second and third types, which are responsible for transmitting impulses throughout the conduction system and to the contractile myocardium, are poorly functioning.
Blockades by localization:
- sinoatrial
- atrioventicular
- intraventricular
Sinotrial occurs at the level of the atrial myocardium. Atrioventicular is characteristic of the level of the atreoventicular junction and the trunk of the His bundle. Intraventricular block occurs at the level of the branches and branches of the His bundle. Conductivity can be impaired at different levels simultaneously, which indicates widespread damage to the conduction system of the heart.
Types of blockade by completeness:
When complete, there is a complete interruption in the passage of the excitation wave. And if it is incomplete, the impulses are carried out slowly, or some of the impulses may periodically fail to pass through the affected area.
Blockades in relation to the His bundle:
Sinotrial block - in which the impulse slows down or stops as it travels from the sinotrial node to the atria. Types of sinotrial blockade in children: permanent, transient.
Partial sinotrial blockade is characterized by the fact that some impulses do not pass from the SA node to the atria, which is accompanied by periods of asystole.
If several contractions of the ventricles occur one after another, then the child may feel dizzy, fainting, and cardiac “fading” are possible. During auscultation, the doctor listens for a temporary absence of heart sounds.
The ECG shows long diastolic pauses, after which escape contractions or rhythms may appear.
Complete sinotrial blockade is a condition when impulses do not reach the atria in any quantity at all.
Atrioventricular block - in which impulses are poorly conducted through the atrioventricular connection. Blockades are of the first, second and third degree.
Stage I can only be diagnosed using an ECG. Auscultatory methods do not give results. No symptoms appear. The ECG shows a lengthening of the PQ interval compared to the norm adequate for the child’s age. The conduction of impulses through the affected area is slower than it should be.
Grade III is known as complete transverse AV block. Impulses to the ventricles from the atria do not pass at all. Heterotopic rhythm is rarer than sinus rhythm. Auscultation reveals a slow heart rate. The heart rate is less than normal for children of this age.
Intraventricular blocks (bundle branch blocks)
There can be both isolated blockades and combinations of several of them: left, right legs, anterior and posterior left branches. This type of heart block in children can only be diagnosed using the ECG method. According to their expression, they can be complete or incomplete.
Sinotrial blockade is often diagnosed in children over 7 years of age against the background of vegetative-vascular dystonia with vagotonia. In this case, the atopine test will show a positive result.
This means that the blockade is removed by administering atropine. The causes of SA blockade are often myocardial dystrophy or myocarditis in children.
This blockade can develop in parallel with atrial fibrillation, extrasystole, and AV block.
Sick sinus syndrome may have sinotrial block as one of its manifestations. Among the causes of SA blockade in children is also poisoning with certain drugs, for example, cordarone, quinidine, and adrenergic blockers.
Atrioventricular heart block in children of the first degree often occurs due to vegetative-vascular dystonia with vagotonia.
This is confirmed using a functional test with atropine, which shows a positive result. This blockade occurs in a child with an ongoing inflammatory process in the area of the atrioventricular junction.
First degree atrioventricular block can occur even in very young children - it is inherited genetically.
Second degree AV block in most cases occurs with serious damage to the heart muscle. These are MCD, myocarditis, cardiosclerosis, cardiomyopathy. An incomplete blockade can become complete, and a complete blockade can become incomplete.
Acquired complete atrioventricular block often has a cause such as myocarditis. When sclerosis forms, it will be persistent, but during the current process it will be transient.
AV block in children can be caused by heart tumors, atherosclerosis, or narrowing of the vessels that supply the atrioventricular junction.
The cause of intraventricular heart block in children may be ongoing myocarditis. With MCD and cardiosclerosis, as a rule, persistent bundle branch blocks are found.
With congenital heart disease, if surgery is not performed, the child may have intraventricular heart block. They also occur after cardiac surgery.
Also, the cause of intraventricular blockade may be heredity.
Incomplete sinotrial block is very similar to SA node failure. In these two cases, a long pause is recorded on the ECG. Sick sinus syndrome can manifest itself as a failure of the SA node - it cannot generate impulses for a while because the power supply is disrupted.
Type II blockade differs from the first in that there is no consistent prolongation of the PQ interval on the ECG. It is either within the normal range for the child’s age, or persistent lengthening is observed. Ventricular complexes, as with type I blockade, periodically fall out.
Complete transverse block can be either acquired or congenital. Congenital occurs if the child has suffered late congenital carditis. In this case, it is a consequence of post-myocardial sclerosis.
Isolated complete congenital AV block is a consequence of the formation of conduction cells of the atrioventricular node. In this case, symptoms may not appear, except for a rare pulse.
An ECG helps diagnose the disorder.
But then the blood flow inside the heart is disrupted, which leads to stretching of the chambers, a slowdown in general blood circulation throughout the body, and a deterioration in the nutrition of the myocardium and other organs. The result is that a child with such a diagnosis lags behind not only physically, but also mentally. AV block can have complications such as heart failure.
Asystolic pauses are a threat to the child’s life. Short attacks of asystole can be manifested by symptoms such as dizziness, short-term fainting, and weakness. Fainting can occur due to emotional stress or physical overload.
Reliable AV block in children is diagnosed only with the help of an ECG. Atrial P waves and ventricular QRST complexes are recorded independently of each other on the ECG. The P-P interval is shorter than If the heterotoin pacemaker is located in the ventricles, the ventricular complex will be deformed.
To treat sinotrial blockade, it is imperative to cure the underlying disease. For frequent fainting, atropine-like drugs are used to reduce the degree of blockade. Bellatamyal and amizil are effective. Severe cases are treated only in cardiac surgery departments for the treatment of cardiac arrhythmias, and electrical pacing is used.
For first degree AV block, no special treatment is required. The underlying disease is treated. You should not take drugs that slow down conduction, for example, cardiac glycosides and potassium.
Second degree AV block in children is treated depending on the underlying disease in the child. If it is myocarditis, then glucocorticosteroids are prescribed. If this is myocardial dystrophy, then cardiotropic drugs are needed.
For the congenital form of complete AV block, medications are not used, because they have no effect. Children should have a minimum of physical activity. During attacks of asystole and severe bradycardia, only an artificial pacemaker helps.
The acquired form of complete AV block due to myocarditis is treated with glucocorticosteroids and cardiotropic drugs. You cannot take cardiac glycosides or potassium. If the medications do not have the desired effect, frequent fainting occurs, or there is severe bradycardia, then the doctor may prescribe an artificial pacemaker.
There is no treatment for intraventricular heart block in children. Treat the underlying disease. Myocarditis is treated with glucocorticosteroids, MCD is treated with cardiotropic drugs. With intraventricular blockades, the child must not be physically stressed; active games are contraindicated; the child must not be enrolled in sports clubs or involved in agricultural work.
- Treatment of heart diseases
- Timely contact with a pediatrician and cardiologist
- Lack of physical activity if indicated by a doctor
- Annual examinations of healthy children for the purpose of timely detection and treatment of heart diseases
Is something bothering you? Do you want to know more detailed information about heart block in children, its causes, symptoms, methods of treatment and prevention, the course of the disease and diet after it? Or do you need an inspection? You can make an appointment with a doctor - the Euro lab is always at your service! The best doctors will examine you, study external signs and help you identify the disease by symptoms, advise you and provide the necessary assistance and make a diagnosis. You can also call a doctor at home . Euro lab clinic is open for you around the clock.
How to contact the clinic: Phone number of our clinic in Kiev: (+38 (multi-channel). The clinic secretary will select a convenient day and time for you to visit the doctor. Our coordinates and directions are listed here. Look in more detail about all the clinic’s services on its personal page.
If you have previously performed any tests, be sure to take their results to a consultation with your doctor. If the studies have not been performed, we will do everything necessary in our clinic or with our colleagues in other clinics.
You ? It is necessary to take a very careful approach to your overall health. People do not pay enough attention to the symptoms of diseases and do not realize that these diseases can be life-threatening. There are many diseases that at first do not manifest themselves in our body, but in the end it turns out that, unfortunately, it is too late to treat them.
Each disease has its own specific signs, characteristic external manifestations - the so-called symptoms of the disease . Identifying symptoms is the first step in diagnosing diseases in general.
be examined by a doctor several times a year in order not only to prevent a terrible disease, but also to maintain a healthy spirit in the body and the organism as a whole.
If you want to see a doctor, use the online consultation section, perhaps you will find answers to your questions there and read tips on caring for yourself .
If you are interested in reviews about clinics and doctors, try to find the information you need in the All Medicine section.
If you are interested in any other types of diseases and groups of human diseases, or you have any other questions or suggestions, write to us, we will definitely try to help you.
Source: https://www.eurolab-portal.ru/diseases/2634/
Symptoms
Sinoauricular block of the 1st degree is very difficult to identify, since it does not manifest itself in any way. It is determined only if there is no subsequent heartbeat after 2-3 normal cycles.
The frequency of sinus impulse loss influences the clinical signs of second-degree block. If infrequent loss of heart contractions occurs, the patient will suffer:
- dizziness;
- chest discomfort;
- general weakness;
- shortness of breath.
Symptoms of blockade, which is characterized by some absence of heartbeat cycles, will be as follows:
- heart sinking;
- noise in ears;
- bradycardia.
When the disease is accompanied by organic damage to the myocardium, heart failure forms.
Asystole leads to the development of Morgagni-Adams-Stokes syndrome in patients. In this case, there is pallor of the skin, unexpected dizziness, flashing dots before the eyes, convulsions, loss of consciousness, and ringing in the ears.
So, we can conclude that the second and third stages manifest themselves:
- discomfort behind the sternum;
- attacks of dizziness;
- shortness of breath;
- general weakness;
- loss of heartbeat;
- heart sinking;
- pale skin;
- tinnitus;
- convulsions.
Diagnosis of the disease
The main methods that allow us to detect the presence of sinoatrial block are electrocardiography and a similar Holter analysis. The latter method is used if there are no signs of disease on the ECG results. Data collection is carried out over three days. In this case, it is possible to draw reliable conclusions. Holter studies are performed not only for adults, but also for children.
A test with atropine is also used for diagnosis. The essence of the analysis is to introduce into the body a substance that affects the heart rhythm. You can judge the presence of a problem if, after an increase in the pulse, a sharp reduction occurs.
Another effective method is ultrasound. According to this study, it is possible to identify the presence of defects, scars and other pathological changes in the structure of the myocardium.
Description of the disease
Sinoauricular block is a condition in which there is weakness of the sinus node. The conduction of the electrical impulse is blocked between the sinoarterial node and the atria. With this disorder, temporary atrial asystole is observed when one or more than one ventricular complex falls out.
Manifestations of sinoauricular block are rare, and if they develop, they occur most often in the male half of the population (in 65% of cases). The disease is diagnosed at any age.
What is blockade of 1st, 2nd, 3rd degree and type? More on this later.
What is heart block in a child and its degree: causes, symptoms, treatment, prevention
Heart block is a disease that occurs due to an irregular heart rhythm in a child due to a slow or stopped flow of nerve impulses in the conduction system.
Causes
Impulses are generated by the sinus nodal system of the right atrium. The signal then travels to the atria and causes them to contract. After which the impulses reach the ventricle, from which the conduction system branches to other areas. In changing this natural course of impulses lie the causes of heart block.
Violations can take shape during intrauterine development or from heredity. If the mother suffered from lupus during pregnancy, the disease manifests itself as a complication in the child.
The causes of the disease sometimes lie in infectious diseases such as Lyme disease. Sometimes, such a complication begins after surgery, when the child’s heart is injured. Through toxic lesions, the disease can be provoked by certain medications.
Experts define the development of heart block in a child as a pathology arising from other diseases.
Impaired cardiac conduction can be a consequence of: vegetative-vascular dystonia, cardiosclerosis, cardiomyopathy, vagotonia, myocarditis.
Almost any damage to the heart muscles can theoretically lead to problems. Among athletes, they manifest themselves from increased physical activity.
Symptoms
Symptoms of heart conduction disease can be similar to many other ailments, so for an accurate diagnosis you should consult a doctor.
Violation of cardiac conduction in a child is expressed by dizziness and shortness of breath. Pain occurs in the left side of the chest, and sinus arrhythmia appears.
Characteristic fatigue occurs, even to the point of fainting. Its motivating reasons are physical or psychological overload.
Loss of consciousness is accompanied by convulsions, cyanosis and even absence of pulse. The work of the ventricle switches to the heterotopic mode and temporary asystole occurs.
Short asystolic pauses manifest themselves in the form of dizziness and a general low energy tone of the body.
Long asystolic pauses are very dangerous and pose an immediate threat to the child’s life.
The flow of blood in the insides of the heart is disrupted and this is the reason for the stretching of the chambers. The nutrition of the myocardium and other organs is sharply weakened. Slow blood circulation cannot cope with the supply of the body as a whole. Among the complications, the child may develop heart failure.
The disease can affect not only a lag in the level of physical capabilities, but also be an obstacle to the development of the child’s psyche.
Classification
Conduction disturbances appear in various places of the heart (atrium, branches from the left bundle branch, etc.). The method of treatment is based on the location of the disease.
Sinotrial block (atrial) - the nerve signal is slowed down in the muscles of the atrium. The manifestations of atrial block are very similar to bradycardia when a slow heart rate is diagnosed.
Atrioventricular block (atrioventricular block) - when the electrical impulse is disrupted as it passes from the atria to the ventricles in the area of the atrioventricular node. Impaired atrioventricular conduction is expressed by rhythm problems. The severity of cardiac dysfunction is determined by degree.
Atrioventricular block occurs:
- 1st degree – is a mild form of the disease. The electrical impulses transmitted through the heart muscles are slower than normal, but eventually reach the ventricle. The heart rate remains smooth, and symptoms are not evident or dangerous. This blockade requires regular monitoring.
- 2nd degree (the so-called incomplete blockade) - with it, some impulses are not transmitted to the ventricles at all, and the heartbeat has a reduced rhythm. Incomplete blockade does not pose a serious danger if it proceeds without complications. Otherwise, incomplete blockade may continue in the third degree.
- 3 degrees (in other words, complete transverse heart block) is the most dangerous type. Conduction disturbances are the most severe - impulse signals cannot reach the ventricles. Complete blockade forces the ventricles to independently replace impulses, but they cannot fully satisfy the needs, which is expressed in the form of a slow heart rate.
Intraventricular block - expressed in the right or left part of the fasciculus. It can be either complete or partial.
The conduction of nerve impulses is disrupted at the level of the right or left bundle branch, as well as when a branch from the left bundle branch is blocked (posterior and anterior branches).
Usually, it does not pose a threat to life, since nerve signals can pass through the obstacle along an adjacent branch.
Types of intraventricular blockades:
- Right bundle branch – nerve signals travel along the left bundle, but are largely absent along the right one. In some cases, impulses do not pass through the right leg at all.
- Left bundle branch - nerve impulses flow into the ventricle through third-party pathways due to blockage of the left bundle branch.
- The anterior branch of the left bundle branch is a disturbance in the flow of impulses along the branch to the walls of the ventricle (there may be complete or partial blockage).
- The posterior branch of the left bundle branch is detected less frequently than others, it prevents the passage of impulses along the branch on the way to the ventricle.
Diagnostics
Heart disease can be diagnosed by visiting a doctor. At the first symptoms and suspicions, do not delay visiting a specialist.
You should contact a cardiologist or arrhythmologist, who will prescribe procedures to check your heart rhythm and conduction.
The doctor will ask about symptoms, check your medical history, and perform a physical examination of your child. After the doctor’s conclusion, the following types of examinations may be prescribed:
- ECG is the process of recording the activity of the heart, which records the work of the heart muscle; carried out using electric current;
- ECG with atropine tests - an ECG is recorded after the substance atropine is injected into a vein (it changes the heart rhythm);
- Echocardiography is a process in which the shape and size of the heart is analyzed using ultrasound waves, and an idea of its conductivity is formed;
- Holter monitoring is a method of continuous recording of an ECG in everyday life, which will allow one to analyze changes in cardiac conduction on the cardiogram at different times of the day. The method will allow you to create a diary of heart rhythm observations and most accurately characterize the disease.
Prognosis and prevention
It is difficult to talk about prognosis for sinoatrial blockade, since many factors are taken into account. It is necessary to take into account the nature of the course of the underlying illness, the degree of the disease, the presence of other problems, and the age of the patient. The presence of Morgagni–Adams–Stokes syndrome is a factor that allows for an unfavorable prognosis.
Sinoatrial blockade continues to be studied. Experts have not yet been able to formulate a clear plan of preventive measures that would help avoid or reduce the likelihood of the formation of SA blockade. It is important to promptly eliminate the causes that led to the development of the disease and be constantly monitored by a cardiologist.
When the heart worries and sends signals, you need to react sharply, identify the cause and treat it. The consequences of delay can be sad and tragic. In many cases, early diagnosis can completely eliminate the problem.
Sa blockade 2nd degree in a child
SA block (sinoatrial block) is a type of sinus node weakness.
In general, this is a rather rare phenomenon from the category of arrhythmias and is diagnosed mainly in men. There is no age limit for SA blockade as such. In a completely healthy heart, an impulse of electrical charge from the right atrium passes unhindered along this path, creating muscle contraction in the heart.
If, while traveling through our heart, the charge encounters an obstacle, then the contractions themselves automatically fail; it is these obstacles that are the blockade.
With SA blockade, there is a disruption in the creation of a charge and its subsequent distribution. As a consequence, disorganization of ventricular contractions occurs. After a while, the heart begins to systematically skip contractions.
Causes
The problems that SA blockade creates are node deformation and dysfunction of cardiac muscle contraction. It happens that because of it the impulse is too weak or not generated at all.
Reasons leading to blockade:
- Rheumatism of certain forms;
- Heart attack;
- Overdose of drugs;
- Myocarditis;
- Ischemia;
- Heart disease;
- Injury to cardiac tissue;
- Intoxication with organophosphorus substances;
- Cardiomyopathy.
SA blockade appears when the overly active vagus nerve begins to influence the sinus node through activation. In most situations, under such conditions, a transient blockade is performed.
This type of SA blockade resolves over time on its own, without therapeutic or external intervention. Changes in the structure of the heart anatomically do not occur, which allows for the possibility of its manifestation in healthy and strong people.
In very exceptional cases, SA blockade is idiomatic; the factor of its occurrence has not yet been found by scientific doctors.
Degrees of SA blockade
The degree is directly dependent on the intensity of arrhythmias.
- First. At this level, impulses occur, but less frequently than in the normal state. The unit is operating as normal. The only problem is the speed of the pulse. An ECG will not show this degree;
- Second. The heart does not contract every time; the prerequisite is a periodic deficit of impulse;
- Third. Complete SA blockade. There is no necessary impulse, the muscle does not contract.
The first two stages are not complete because, although poorly, the sinus node performs its functions. With the latter, complete, the impulse does not reach the atrium at all.
SA blockade and ECG
What will the ECG show in the second degree:
- Longer intervals between impulsive muscle contractions (PP);
- Decrease in P-P over time after a pause;
- If the intervals are large, the impulses come from another source;
- When there are several impulses and contractions in a row, the pause R-R is long, as in the normal state.
With the third degree, any absence of electrical charges is observed. It is not uncommon for a person to die in such a situation.
How does SA blockade manifest and methods for diagnosing it
In the first degree, a person does not experience discomfort and there are no symptoms. The body becomes accustomed to frequent bradycardia and the person does not feel changes within himself and lives quite comfortably.
The latter degrees already have symptoms that are easily recognizable. These are unpleasant sensations in the chest area, periodic noise and ringing in the ears, shortness of breath, and frequent dizziness. Weakness throughout the body also occurs due to rare rhythmic contractions. If there is a change in the structure of the muscle, signs such as:
- Blue skin;
- Enlarged liver;
- Swelling;
- Shortness of breath;
- Heart failure;
- Decreased ability to work.
The child has the same symptoms. We recommend that you take a closer look at the following: cyanosis of the nasolabial area, decreased performance and severe fatigue. If such symptoms are noticed, go to a cardiologist for check-up.
When the pause between contractions is long, paroxysms appear. Paroxysms are a process in which the brain stops receiving the required amount of arterial blood, its supply is reduced significantly. Symptoms:
- Noise and ringing in the ears;
- Involuntary urination and bowel movements;
- Systematically loss of consciousness;
- Spasm.
The child should also be monitored. Bradycardia for about forty minutes, together with pauses between impulses of three seconds, are an alarm bell. It is common practice to test samples with atropine. If there are problems, the pulse instantly increases several times and just as sharply returns to the original one, or lower, this is a blockade.
In order to be directly convinced of this diagnosis, it is necessary to conduct an ultrasound of the heart to exclude other diseases, for example, myocardial problems.
Treatment of the disease
The first degree does not require intensive treatment. It will be enough to restore the correct daily routine, if it is disrupted, treat the main heart diseases, or stop using heart medications that can affect the performance of the sinus node.
Transient blockade can be treated with medications containing atropine. They are actively used in pediatrics for vagotonia. It should be remembered that reaction therapy is fleeting. Metabolic treatment is more effective with SA blockades. Riboxin, cocarboxylase and vitamin-mineral complexes are the leading fighters in the war against blockades.
SA blockade is a heart disease that is extremely life-threatening; do not forget about routine examinations with a cardiologist.
about heart rhythm disturbances
In this video, Elena Malysheva will tell you how to treat cardiac arrhythmia:
Why does it occur, how is sinoatrial block determined and treated?
Sick sinus syndrome can manifest itself in various forms. One of them is sinoatrial block. This disease is rare and occurs most often in men. Can appear at any age. It is this disease that we will devote this material to.
What is sinoatrial block?
Electrical discharges are born inside the heart and spread throughout its body. They are generated by the sinus node, located in the right atrium. Each impulse that arises is directed to the atrioventricular node and the bundle of His, or rather, to its legs. This mechanism ensures normal contraction of the heart chambers and is the basis for the normal functioning of the heart as a whole.
There may be obstacles along the path of the impulse that disrupt this process. In such a situation, we are talking about blockades, of which there are several varieties.
At some point, the heart misses an impulse and does not respond to it with a contraction.
Reasons for the development of pathology
There are several main mechanisms that can trigger the development of sinoatrial block. This may include damage to the sinus node, disturbances in the process of impulse transmission through the muscle, and changes in the tone of the vagus nerve. The impulse may not occur at all, or may be so weak that cardiomyocyte contraction simply does not occur.
There are many factors that can lead to the development of such a disease. Even the shortened list looks impressive:
- various heart defects;
- myocarditis;
- rheumatism in cardiovascular form;
- leukemia, other formations and injuries leading to secondary damage to the tissue of the heart muscle;
- ischemic disease;
- heart attack;
- vagotonia and cardiomyopathy;
- taking certain medications associated with allergies or overdose;
- effects on the body of organophosphorus substances;
- active work of the vagus nerve leads to the development of a transistor form of the disease, which goes away on its own.
A child may also have sinoatrial blockade, most often this occurs after reaching 7 years of age. Such disorders arise due to autonomic dysfunction.
In this case, in most cases, a transient form of the disease develops, occurring against the background of high tone of the vagus nerve.
In rare cases, the cause of sinoatrial block in children is myocarditis and myocardial dystrophy.
Degrees of manifestation and their features
Sinoatrial block can be expressed in varying degrees. This classification is based on the severity of the disease, its symptoms and complications that may occur in the body.
SA blockade 1st degree
This condition is characterized by the functioning of the sinus node, and even impulses lead to contractile function. Only this does not happen with the frequency that is typical for the normal state.
Negative changes are minimal, the speed of the impulse is slightly slower, and accordingly, the heart contracts less frequently. Sinoatrial blockade of the 1st degree is not detected on the ECG results.
This condition can only be detected by bradycardia.
Source: https://baby-clinic-vozr.ru/narodnaya-medicina/sa-blokada-2-stepeni-u-rebenka.html