5 / 5 ( 2 voices)
Today, doctors have a wide range of diagnostic devices that are absolutely harmless, which allows them to examine infants and young children much more thoroughly than was done before. After an ultrasound examination of the heart, a diagnosis of MARS can be made.
These are abnormal changes in the structural structure of tissues that are not significant and cannot cause harm. Quite rarely, an unfavorable clinical picture is recorded, which does not affect the psychomotor or physical development of children. Special therapy is possible in exceptional cases.
MARS is an anomaly that is not a disease and goes away as the child grows older
A little anatomy
The framework of all the internal organs of the child consists of special connective tissue - it is formed in utero. Connective tissue gives the organ its characteristic shape, helps it perform functions and prevents it from stretching and deforming under impacts. Connective tissue can be presented in two types - coarse fibrous, an example is cartilage, and soft fibrous - this is a kind of sponge, inside of which there are specific cells of a particular organ.
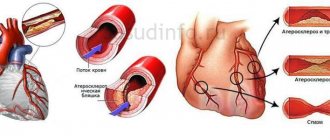
In the structure of the heart, this same connective tissue forms the valves and the heart frame itself, between the fibers of which muscle cells - cardiomyocytes - are located. Due to this, the heart tissue is elastic, but quite strong. In addition, connective tissue also forms the walls of large vessels - the aorta, pulmonary trunk, pulmonary veins and their valves (see figure). Minor cardiac anomalies (or MARS) are one of the manifestations of a condition such as dysplasia (not quite correct development) of this very connective tissue. In this condition, the connective tissue is either too weak or is formed in excess, not in the places where it should normally be. As a result, minor anatomical formations of internal organs, including the heart, appear.
Thromboembolism in small heart defects
The complication is dangerous especially at a young age; the risk of blood clots is relevant for young athletes.
Patent foramen ovale and mitral valve prolapse can cause ischemia, cerebral infarction, peripheral or paradoxical embolism.
Thromboembolism affects young people during periods of intense physical activity; the cause is oxygen deficiency of the arterial blood or an additional chord of the left ventricle.
The risk of thromboembolism due to minor cardiac anomalies increases in people with bronchial asthma.
Causes and mechanisms of development
Minor anomalies in the development of the heart are considered to be the presence of anatomical congenital changes in the heart and its large vessels - that is, a disorder in the structure of the heart itself that forms in the fetus. However, these changes are either insignificant or located in such a way that they do not disrupt the function of the cardiovascular system - the delivery of oxygen to the tissues.
Many MARS are temporary and disappear as the child grows - for example, due to the growth of the heart, prolapse (sagging) of the valves (MVP), pectineal muscles can be normalized, or the oval window can close, the length of the chords and the diameter of the heart vessels can be normalized. Basically, in modern conditions, MARS is detected in the vast majority of cases already in the first 2-3 years of life and has no tendency to progress.
It is believed that the development of MARS is caused by a combination of many factors. There are two large groups - external and internal factors. External factors include environmental influences, the pregnant woman’s diet, her illnesses and medications, radiation, smoking, alcohol intake, stress, etc. Internal factors include genetic, chromosomal abnormalities, and heredity.
Typically, such anomalies in the heart appear at conception (inherited), during pregnancy (congenital), and very rarely at the birth of a child.
The heart is formed in the earliest stages of intrauterine development. At about 5-6 weeks, the main division into chambers is formed and it begins to beat. Around this time and up to 10-12 weeks, the impact of various factors on the expectant mother (and many at this time still do not know about their situation) leads to anomalies. Exposure of a pregnant woman to alcohol, nicotine, toxins, poisons, heavy metal salts, viruses and bacteria in the first trimester can result in the formation of defects or minor anomalies in the development of the heart, because the placenta is still forming, and these substances can more easily penetrate to the fetus.
General symptoms and diagnosis of MARS
Most often, minor anomalies in the development of the heart do not manifest themselves in any way, but in cases where a patient has several such features at the same time, this can affect the functions of the heart. Then a child or adult may experience the following complaints:
- An interesting fact is that in some cases it is possible to assume the presence of MARS in an unborn child even before his birth - through perinatal ultrasound screening of the fetus. Often, one or another minor cardiac anomaly, including accessory or abnormal chordae, provides the basis for an interesting ultrasound phenomenon - a hyperechoic cardiac focus, or golf ball sign.
- In children under one year of age, a characteristic sign of certain heart problems is the appearance of cyanosis. Cyanosis is a bluish or gray discoloration of the skin, including the nasolabial triangle, during sucking, crying, and physical activity.
- Shortness of breath or rapid breathing while eating or doing vigorous exercise.
- In older children and adolescents, during rapid growth of the body and hormonal changes, complaints from the cardiovascular system and vestibular system may appear: rapid heartbeat - tachycardia, “interruptions” in the work of the heart, pain in the chest and in the heart area, the appearance of a “lump” " in the throat, weakness, dizziness, causeless fainting and loss of consciousness, increased sweating.
- Sometimes doctors can observe an increase in the patient's pulse, instability in blood pressure, and when listening to the heart with a stethoscope, the doctor hears various noises. It is these heart murmurs that first force the doctor to prescribe a cardiac ultrasound to the patient.
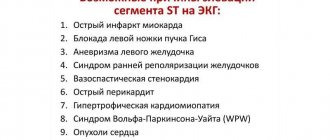
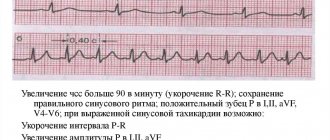
- In quite rare cases, MARS can cause certain changes in the electrocardiogram - sinus tachycardia, shortened PQ interval syndrome, some types of arrhythmias.
These are common symptoms of MARS found on ultrasound and Doppler studies of the heart.
Additionally, in order to assess the effect of a particular MARS on the functioning of the cardiovascular system, other research methods are used:
- Electrocardiography (ECG) – recording of the electrical activity of the heart.
- Holter monitoring is a continuous recording of an ECG throughout the day using a special portable and portable ECG device.
- Functional tests with physical activity - bicycle ergometer, walking and other physical exercises.
- 24-hour blood pressure monitoring (ABPM) is a technique similar to Holter monitoring, only the device measures the patient’s blood pressure at a given time interval throughout the day.
- Pulmonary function tests to assess the fullness of lung function.
- Laboratory research.
Next we will talk in more detail about some of the options for these interesting features of the structure of the heart.
What are they?
There are a lot of minor anomalies in the development of the heart and sometimes they are difficult to distinguish from heart defects with minor changes in blood circulation at an early stage. Therefore, a cardiologist must decide whether they require surgical correction and whether they belong to a defect or to MARS, after a detailed examination. There are borderline conditions in which the classification of a defect into one group or another depends on the size and clinical data.
Minor anomalies are considered to be:
- Heart valve prolapse of the minimal, first degree is a state of pathological sagging, sagging of the valves due to their excessive extensibility or weakness.
- Abnormal (not in the places where it is needed) location of the chords of the heart - peculiar cartilaginous threads that give strength to the heart.
- Disturbances in the structure of special cardiac muscles - papillary muscles.
- Changed number or size of heart valves, their serration.
- Rudimentary sinus valves.
- Small-sized holes in the interatrial or interventricular septum that do not close in the first year and a half of life.
- An open oval window is small in size, up to 2-3 mm.
- A slight increase in the diameter of the outgoing vessels.
- Small aneurysms of the heart septum.
- “Fluttering” or false chords.
MARS and its complications
Despite the apparent harmlessness of minor heart defects, they can also have dangerous consequences; their course and nature depend on the type of anomaly.
Complications most often result from mitral valve prolapse:
- arrhythmias of varying severity;
- disturbance of electrical conductivity;
- infectious endocarditis;
- chronic fatigue syndrome;
- sudden death;
- defeat of the chords;
- blockage of blood vessels in the brain with blood clots;
- Mitral valve insufficiency.
Patients also experience such serious problems: blood clots inside the ventricle, aneurysms of the interatrial septa and sinus of Valsalva.
How are they detected?
Most often, MARS is detected during a routine examination by a pediatrician. Usually, the baby has a heart murmur with a generally satisfactory condition and no complaints. Usually, the doctor at the clinic limits himself to writing on the card - functional cardiopathy, which does not entirely accurately reflect the essence of the phenomena occurring with the baby. By and large, this is not a diagnosis, but simply a statement of fact - there are some minimal deviations from the norm in the heart that cannot be attributed to a specific, more serious diagnosis.
The detected phenomena do not affect the child’s condition, however, to clarify the picture, a full examination and clarification of the clinical diagnosis are required - this is necessary to develop measures for monitoring the baby and his rehabilitation. To do this, you should go to an examination by a pediatric cardiologist - a specialist in heart and vascular diseases.
The doctor will ask you questions. You will tell us how the baby eats, whether he gets tired when he sucks, whether there is any blueness, attacks of shortness of breath, how weight gain occurs. And if the baby can already talk, does he have pain in his heart, is he dizzy, is there a feeling of heartbeat, have he fainted or not?
Then he will carefully examine the baby to see if he has perioral cyanosis (blueness of the nasolabial triangle), count the heart rate and breathing to determine if there is tachycardia and shortness of breath. He will examine the tips of the fingers and nails, the shape of the chest, and percussion (tapping) the borders of the heart to determine its size. The doctor will palpate the abdomen - the area of the liver and spleen, large vessels, pulse.
Then he will begin to listen (auscultate) the heart. The first thing that is usually detected when listening to a baby’s heart is the so-called functional systolic murmur. The word “functional” indicates that the murmur is not caused by some serious heart pathology, such as a defect. The doctor will find out where the noise is coming from, what heart sounds are associated with it, and listen to the baby in front and behind.
Based on all this, he will make a conclusion whether or not the child has a circulatory disorder; with MARS, usually no changes are noted other than noise. Your examination will not end there; you will also have to undergo instrumental examination using various devices.
Let's go to research
To confirm MARS in a child, it is necessary to conduct a number of studies, and the first of them will be an ECG - recording the electrical signals of the heart on a special film. This method can determine the presence of disturbances in heart rhythm, its conductivity and signs of excessive load on different parts. Typically, with MARS, all changes are minimal or do not go beyond age norms.
In addition, it is necessary to conduct a parallel study of noise, called PKG - phonocardiogram. This is a graphic reflection of pathological noise on paper, in parallel with an ECG recording. This study will allow us to differentiate functional noises from organic ones that arise from defects.
The most basic thing in diagnosing MARS is, of course, an ultrasound examination of the heart - ultrasound. This method allows you to visually see both the anomaly itself and the degree of disruption of blood flow that it causes. In addition, ultrasound is very easy to determine whether a given phenomenon relates to a defect or not.
What provokes it?
The reasons for the development of MARS in a child may remain unclear , but in most cases the provoking factor is a disorder in the structure or functioning of connective tissue.
The formation of such a pathology can occur at the stage of intrauterine development of the fetus or be acquired by children in the first years of life under the influence of certain unfavorable factors.
The causes of MARS are the following factors:
- development of dysplasia of connective structures;
- consequences of genetic mutations;
- diseases of chromosomal etiology;
- pathological processes during fetal formation;
- exposure to unfavorable environmental conditions;
- consequences of taking potent medications during pregnancy;
- exposure to radiation on a woman during pregnancy;
- consequences of exposure to harmful chemicals;
- abuse of bad habits during pregnancy;
- complications after an infectious disease.
You will find recommendations for the treatment of bradycardia in children on our website.
So how do MARS manifest itself?
In most cases, MARS does not manifest itself in any way, and children are no different from their peers. Less often, the main complaints of children will be intermittent pain in the heart area, arrhythmias, feelings of interruptions in the heart, and surges in blood pressure.
Often heart anomalies are combined with structural anomalies of the nervous, urinary, digestive system, vision, breathing, skeleton or skin; there may be some structural features of other organs - liver, gall bladder, kidneys.
At the beginning of the material, we said that MARS refers to connective tissue dysplasia, and connective tissue is present in all organs and systems in greater or lesser quantities. Therefore, the manifestations will be so-called systemic, that is, at the level of the entire organism. They can range from very minimal to quite pronounced.
A careful examination of the skeleton can reveal elongation of the limbs relative to the body, depression of the sternum, scoliosis (curvature) of the lower thoracic spine, various forms of flat feet, hypermobility (excessive mobility) of the joints. The most common combinations with MARS are polycystic kidney disease, gastroesophageal reflux (reflux of stomach contents into the esophagus), kinking of the gallbladder, megaureter (dilation of the ureter).
In addition, MARS is often accompanied by so-called neurovegetative disorders - the peripheral and central nervous systems work unbalanced. This can manifest itself as enuresis, speech defects, vegetative-vascular dystonia, and behavioral disorders. However, all these combinations in no case lead to severe dysfunction of organs and systems and do not worsen the overall functioning of the baby’s body.
Could there be complications?
Not always, but in some cases, MARS can be accompanied by cardiac rhythm disturbances, impulse conduction disturbances, which can manifest as minor changes in the ECG and periodic heart pain and palpitations. This requires additional examination by a cardiologist and is quite simply treated by prescribing medications that support heart function. Typically, these disorders are characteristic of mitral valve prolapse. Rhythm disturbances can result from abnormally located chords and trabeculae of the heart, an aneurysm of the interatrial septum, or an enlarged Eustachian valve.
Some MARS may be accompanied by impaired exercise tolerance; such babies have a slightly higher risk of developing infective endocarditis - inflammation of the inner lining of the heart as a complication of ARVI or other infections.
Diagnostics
You can suspect a child has MARS based on heart murmurs, which the doctor can listen to after birth. This is usually a systolic murmur that changes as the child moves and exercises. If it is detected, the baby is sent for a cardiac ultrasound, since this examination most accurately confirms the presence of abnormalities in the heart and their effect on blood flow. Also, children with MARS often undergo an ECG to detect problems with the heart rhythm.
Where to start therapy?
In order for MARS syndrome to manifest itself minimally or not at all, you need to choose an optimal daily routine, an appropriate load for your age and condition, alternating activities and rest. Many parents believe that a child with MARS needs to sharply limit exercise, which is fundamentally wrong. After consulting with a doctor, for the most part, you can not limit the baby’s movement at all. The heart develops correctly when it is given adequate stress. There is no need for restrictions in activity or excessive effort. If the baby expresses a desire to engage in any kind of sport, first consult with a cardiologist to see if the level of stress that sports activities will provide is possible for him. But ordinary daily activities - walking outside, cycling, running - are quite enough for proper development.
For a child with MARS syndrome, it is important to follow a daily routine, get enough sleep, eat properly, and receive all the nutrients and vitamins required by age. It is important to initially prepare yourself for long-term breastfeeding; this will help the baby get sick less and reduce the risk of heart complications at an early age to a minimum. In addition, it is necessary to introduce complementary foods into the child’s diet correctly and in a timely manner, and subsequently monitor the intake of sufficient amounts of protein foods and foods rich in calcium and magnesium.
Children who have neurological problems and are emotionally unstable benefit from working with a psychologist and sedative therapy. Physiotherapy - various baths, spa therapy, massages - also have a calming and restorative effect.
Such babies are monitored jointly by a pediatrician and a pediatric cardiologist. The timing of inspections is selected individually, depending on the type of MARS and the presence or absence of associated violations. Usually, for most children, non-drug measures or infrequent courses of cardiotrophic (supporting the proper functioning of the heart) drugs are sufficient.
Only isolated cases of MARS may require surgical correction. In such cases, the baby will be referred to a cardiac surgeon to decide on the volume and timing of the operation. There is no need to be afraid of this - open heart surgery is very rarely performed for MARS. Usually these are so-called endoscopic operations - an instrument is inserted into the heart cavity through small punctures or through large vessels and the defect is corrected. Usually, babies stay in the clinic for a short time and after discharge they lead the lifestyle of ordinary children.
What if you need pills?
Sometimes there are situations when the doctor will recommend a course of certain medications. The main therapeutic effects are magnesium preparations. This trace element is a component of connective tissue and therefore improves its structure and heart function. The choice of magnesium preparations depends on the age of the patient. There are liquid and tablet forms. Particularly popular are “Magnerot” - in addition it also contains orotic acid, which promotes the absorption and more complete absorption of magnesium, “Magne B6” in the form of syrup or tablets, and “Potassium Orotate”. Usually 1-2 courses per year are recommended.
The second direction of therapy is cardiotrophic - nourishing the heart muscle. These are drugs that improve blood supply and nutrition to the tissue of the heart and other organs, affect metabolism in the body and are active antioxidants. Usually prescribed are “Elkar”, “Ubiquinone” or “Coenzyme Q10”, “Kudesan”, “Cyto-mac”. In addition to these drugs, some vitamins have a similar effect - PP, B2, B1, citric and succinic acids (the drug "Limontar"), biotin. They are prescribed as a multivitamin complex or each separately in courses of 10-14 days twice a year.
In case of infections, the baby is recommended to take preventive courses of antibiotic therapy to prevent heart complications such as endocarditis.
Regular examinations by an ENT specialist and a dentist are indicated to sanitize foci of chronic infection - carious teeth, tonsils, adenoids.
In the presence of arrhythmias, antiarrhythmic therapy is indicated, but it is selected individually in the hospital under the supervision of a physician.
Courses of sedatives are conducted that normalize the functioning of the nervous system, relieve anxiety, increased nervous excitability and treat neuroses.
A little about specific types
The most well-known and common MARS is mitral valve prolapse . This is the sagging of the bicuspid valve at the moment of contraction (systole) of the heart into the cavity of the left ventricle, due to which a slight turbulence of the blood flow in the heart occurs. This turbulence produces systolic murmurs, which the doctor can hear with a phonendoscope. Only the first degree of prolapse is classified as MARS. All other degrees are accompanied by severe circulatory disorders and should be considered heart defects.
Mitral valve prolapse is usually detected by ultrasound or when visiting a doctor with complaints of intermittent pain in the heart. Typically, such babies have periodic heartbeats, poor tolerance to active physical activity, fatigue, asthenia, dizziness, and psycho-emotional instability. Such children have difficulty adapting to a team; they are constrained, shy, and whiny.
False chords in the left ventricle are quite common . This is MARS, which manifests itself in the presence inside the ventricular cavity of additional strands of connective tissue or muscles attached to the walls of the ventricle or interventricular septum. Normally, they should be attached to the leaflets of the atrioventricular valve. This is more often found in boys; false chords can be single or multiple, occurring both separately and in combination with other anomalies. Their location can be along the blood flow, across it or diagonally - the severity of the murmur in the heart will depend on this.
These chords can cause cardiac arrhythmias, so patients require special monitoring by a cardiologist.
The third common MARS is patent foramen ovale (PFO) . A variant of the norm is the presence of a minor defect of up to 2-3 mm under the age of one year. Usually after this age the window closes on its own. But when it is present at an older age, in some cases we are talking about a developmental anomaly (when the size of the defect is up to 5 mm), in others – about a heart defect (when the defect is pronounced and there is a circulatory disorder).
OOO is manifested by pronounced psycho-emotional instability - children are capricious, whiny, they do not adapt well to the team. Babies do not tolerate intense stress well, get tired quickly, they may experience dizziness, interruptions in heart function, and occasionally pain in the heart. On examination, a heart murmur is noted. The diagnosis is usually confirmed by ultrasound.
Causes of MARS
Let's take a closer look at this diagnosis.
MARS in a child, according to experts, occurs due to congenital cardiac changes. This may also apply to large vessels adjacent to the organ, which form during the development of the baby in the mother’s womb. Such changes do not interfere with the functioning of the heart.
The diagnosis of MARS in a child in cardiology is now made quite often.
MARS are temporary in nature; as a rule, symptoms of abnormal development disappear by the age of five years. This is explained by a qualitatively developed medical system for determining such a syndrome at the earliest stages of its occurrence, a large amount of practical knowledge of specialists, and coordination of diagnostic and treatment processes.
For example, a child at a young age was diagnosed with MVP - this is one of the types of MARS - mitral valve prolapse, which has been known in the cardiology field for a long time. During the growth of the body, the heart reached the required size, which corresponds to the patient’s age, as a result of which the diameter of the heart vessels and the length of the chords normalized.
Many people are interested in what is the diagnosis of MARS and LVDC in a child?
It is worth noting that the LVDC is an accessory chord of the left ventricle. This is one of the possible anomalies. Cardiologists and scientists note that the main cause of the syndrome is a combination of a complex of internal and external factors. Internal factors are hereditary changes, genetic predisposition, abnormal distribution of chromosomes. External factors are the state of the ecological and natural environment, the pregnant woman’s history of illness, her diet, the presence of radiation, smoking, stress experienced, and the use of medications or alcoholic beverages.
As a rule, the occurrence of anomalies is due to the stage at which they appeared. After this, the specific reason is determined. For example, if the change appeared at conception, the cause is hereditary; during pregnancy – a congenital feature; after birth - very rare cases.
Regarding hereditary and congenital anomalies, it should be noted that most often they are associated with dysplasia. Such a deviation in development means that the strength of the connective tissue at the genetic level decreases, which is why the following organs are involved in the abnormal process: septa and valves of the heart, subvalvular apparatus, great vessels.
The diagnosis of MARS in a child is not always associated with heart disease.
Summarize
MARS syndrome is not a death sentence, it is a special condition of the child that requires only observation and minor correction. For mothers and fathers, the presence of such a diagnosis is not a reason to limit the child and panic, it is just a reason to change their lifestyle, adjusting it to the capabilities of the baby. Most MARS do not cause any harm to the baby, and his life is no different from his peers. There is no need to treat such a child as a sick person, much less a disabled person - this is groundless. The main thing that parents need to remember is the doctor’s conclusion: “no hemodynamic disturbances are detected.” This suggests that MARS does not interfere with the baby in any way.