A pathology such as paroxysmal tachycardia in newborns and older children is a sudden increase in heart rate. It can last a few minutes or 2-3 hours. Mostly, such an attack passes abruptly and without drug relief. In young children, heart rate reaches 200 beats per minute, and in older children - 160.
Why does the disease occur?
Paroxysmal tachycardia in children is divided into 2 types:
The first type of disease is provoked by the following factors:
- hydrocephalus of the brain;
- neurotic diseases;
- Wolff-Parkinson-White syndrome;
- vegetative-vascular dystonia;
- organic heart lesions.
Supraventricular tachycardia in young patients is provoked by the following reasons:
- carditis;
- heart defects;
- cardiomyopathy;
- increased or decreased levels of potassium in the body;
- poisoning with drugs that contain digoxin and quinidine;
- thyrotoxicosis;
- physical and emotional fatigue.
Return to contents
Causes
Attacks of pathology appear in children for no apparent reason.
Paroxysmal ventricular tachycardia can be provoked by the following factors:
- carditis;
- cardiomyopathy;
- heart disease;
- autonomic dysfunction;
- hypo- or hyperkalemia;
- thyrotoxicosis;
- overdose of a heart drug (usually with digoxin or quinidine);
- overwork in physical or psycho-emotional terms.
Paroxysmal tachycardia in the supraventricular form occurs for other reasons. It can be called:
- hydrocephalus of the brain with high blood pressure;
- organic damage to the heart muscle;
- damage to the central nervous system that caused a neurotic disease;
- Wolff-Parkinson-White syndrome with a congenital anomaly of the heart structure;
- vegetative-vascular dystonia accompanied by sympathetic-adrenal crises.
In addition to provoking factors, the occurrence of pathology can be caused by a predisposition to it. The reason may be an unfavorable course of pregnancy and childbirth.
Paroxysmal tachycardia can occur in both adolescents and infants. Most often, children aged 4-5 years are exposed to attacks of this pathology.
Diagnostic measures
If parents suspect that tachycardia has occurred in teenagers or younger children, it is important to visit the hospital as soon as possible. First of all, the doctor conducts a survey, during which he finds out how long ago the heart rhythm disturbances appeared and what additional symptoms are present. The doctor then begins to listen to the heart. To confirm the preliminary diagnosis, the child is sent for electrocardiography. Sometimes a transesophageal electrophysiological study or 24-hour monitoring using the Holter method is required.
Urgent Care
When a child has an attack of paroxysmal tachycardia, it is important to immediately give him a sedative. Then intravenous administration of antiarrhythmic drugs is required, which normalize the heart rate. If medication measures do not bring the required therapeutic effect, emergency care includes electropulse therapy.
Small patients suffering from supraventricular tachycardia are hospitalized in a hospital, and ventricular tachycardia are admitted to the intensive care unit.
Treatment goals:
- Relieving an attack of supraventricular tachycardia.
- Prevention of subsequent attacks of SVT.
- Rhythm control or heart rate (HR) control in chronic SVT.
- Radical elimination of the electrophysiological substrate of SVT.
Indications for hospitalization
- Primary diagnosis of supraventricular tachycardia
- Relief of tachycardia attacks when therapy is ineffective at the prehospital stage.
- Selection of antiarrhythmic therapy.
- Performing endocardial EPI and RFA.
How is the treatment carried out?
Therapy of paroxysmal tachycardia in children initially involves simple techniques that are equally effective for both supraventricular and ventricular disease. Doctors advise using carotid sinus massage. You can also strain your stomach during maximum inhalation, while holding your breath for 40 seconds. Provocation of the gag reflex is effective during an attack of tachycardia. Rubbing your face with cold water will also help cope with the disease.
As a rule, Phenibut prescribed by a doctor has minimal negative consequences for the child’s body.
If using these methods it was not possible to stop an attack of paroxysmal tachycardia in a small patient, you will need to use medications that affect the cortical-subcortical relationship. The child is prescribed gentle medications that have minimal side effects. Phenibut and tincture of hawthorn or valerian are often used.
When such drug treatment turns out to be ineffective, the child in the hospital is given intravenous medications that reduce heart contractions. Verapamil and Digoxin can be used. If the injection of drugs does not help, electropulse therapy is prescribed. They resort to her help when an attack lasts for 24 hours and there is a risk of heart failure.
Heart rhythm disturbances in children: supraventricular (supraventricular) tachycardia
Supraventricular (supraventricular) tachycardia (SVT) is three or more consecutive heart contractions with a frequency exceeding the upper limit of the age norm in children.
Figure 1. Gradual onset and cessation of ectopic atrial tachycardia
Table 1. Pulse rates
for children and adults
ICD-10 code
I47.1
Supraventricular tachycardia.
Etiology and pathogenesis
Basic electrophysiological mechanisms:
- pathological automatism;
- trigger activity;
- re-entry.
In most cases, children with SVT do not have congenital heart defects or organic myocardial diseases.
The most common cause of paroxysmal tachycardia in children is the presence of an additional conduction pathway.
Tachycardia occurs more often in boys.
Epidemiology
The incidence of SVT in the pediatric population: 0.1-0.4%.
Prevention
There is no specific primary prevention of SVT.
ECG screening allows us to identify children with phenomena of ventricular preexcitation and asymptomatic chronic tachycardias.
Clinical and electrophysiological classification (Kruchina T.K., Egorov D.F., 2011)
- Clinical variants of NVT
- paroxysmal tachycardia:
- stable (duration of attack 30 s or more);
- unstable (duration of attack less than 30 s);
- constant;
- permanently returnable.
- sinus tachycardia:
- sinus tachycardia (functional);
- chronic sinus tachycardia;
- sinoatrial reentrant tachycardia;
- focal (focal);
- multifocal or chaotic;
- incisional;
- atrial flutter;
- atrial fibrillation;
- AVNRT (atrioventricular nodal reentrant tachycardia): typical; atypical;
- focal (focal) tachycardia from the AV junction: postoperative; congenital; "adult" form;
- paroxysmal orthodromic AVRT (atrioventricular reciprocal tachycardia) with the participation of APP;
- chronic orthodromic AVNRT with the participation of “slow” AP;
- paroxysmal antidromic AVNRT with the participation of DPP;
- paroxysmal AVNRT with the participation of the DPP;
Diagnostics
Paroxysmal SVT is characterized by complaints of repeated attacks of palpitations that suddenly begin and end, often accompanied by weakness, dizziness, and sometimes presyncope and syncope.
In young children, paroxysmal tachycardia is manifested by episodes of sudden weakness, lethargy or anxiety, refusal to feed, and with prolonged manifestations, manifestations of heart failure increase.
Chronic SVT is characterized by an asymptomatic course, up to the development of arrhythmogenic myocardial dysfunction (dilation of the heart chambers with a decrease in contractility).
Examination plan:
- ECG in 12 leads;
- 24-hour ECG monitoring (CMECG);
- test with dosed visual load;
- transesophageal EPI (electrophysiological study).
Endocardial EPI in children is rarely performed for diagnostic purposes, usually only as a stage of RFA (radiofrequency ablation).
Additionally, research is carried out:
- EchoCG to exclude structural heart diseases;
- clinical blood and urine analysis;
- blood electrolytes;
- thyroid hormone levels (according to indications).
If a connection between SVT and current myocarditis is suspected, a complex of biochemical, immunological, bacteriological and virological studies is carried out to confirm or exclude it.
Treatment goals:
- Relieving an attack of supraventricular tachycardia.
- Prevention of subsequent attacks of SVT.
- Rhythm control or heart rate (HR) control in chronic SVT.
- Radical elimination of the electrophysiological substrate of SVT.
Indications for hospitalization
- Primary diagnosis of supraventricular tachycardia
- Relief of tachycardia attacks when therapy is ineffective at the prehospital stage.
- Selection of antiarrhythmic therapy.
- Performing endocardial EPI and RFA.
Relief of an attack of supraventricular (supraventricular) tachycardia
- In case of severe hemodynamic disorders, electrical pulse therapy is administered at a dose of 0.5-1 J/kg.
- Stopping an attack of supraventricular tachycardia with stable hemodynamics begins with vagal techniques.
For young children, the cold test (diver effect) is most effective; for school-age children, the Valsalva test is most effective.
It is also possible to massage the carotid sinus (for school-age children) or analogues of the test - turning the child upside down (for young children).
Children and their parents should be taught the technique of vagal techniques.
Pressure on the eyeballs (Aschner-Danyini test) is NOT RECOMMENDED for use in children (risk of eye damage, retinal detachment).
- If vagal techniques are ineffective, drug relief begins with intravenous administration of ATP (in a stream, quickly, without dilution, starting from 0.1 mg/kg).
If tachycardia persists, then after 2 minutes the injection is repeated, and the dose should be increased to 0.3 mg/kg or to an adult dose of 6-12 mg.
Age dosage for intravenous ATP administration:
- up to 6 months – 0.5 ml;
- 6-12 months – 0.7 ml;
- 1-3 years – 0.8 ml;
- 4-7 years – 1 ml;
- 8-10 years – 1.5 ml;
- 11 years and over 2 ml;
- repeated administration - in a double dose.
Efficiency is 90-100%.
However, due to the short half-life (5-10 seconds), relapse of tachycardia is possible in up to 1/3 of cases.
Side effects of adenosine (ATP) are short-term: hypotension, bronchospasm, facial flushing, sinus bradycardia, sinus arrest, AV block.
- To relieve SVT, it is possible to use TES (transesophageal electrical stimulation of the heart).
- If, after repeated administration of ATP, supraventricular tachycardia persists, verapamil or procainamide is used to stop the attack.
VERAPAMIL is administered intravenously slowly at a dose of 0.1 mg/kg in 10-20 ml of 0.9% NaCl (not used in children of the first year of life, with WPW syndrome, together with or after the use of beta-blockers).
PROCAINAMIDE (novocainamide) is administered at a dose of 10-15 mg/kg IV slowly in 10 ml of 0.9% NaCl (given the frequent development of hypotension during the administration of the drug, 1% mezatone (phenylephrine) is administered at a dose of 0.1 ml at the same time IV per year of life, but not more than 1 ml).
If tachycardia persists, use AMIODARONE intravenously at a dose of 5-10 mg/kg (up to 150 mg) in a 5% glucose solution for 30-60 minutes.
Amiodarone is the drug of choice in children with reduced EF when the use of other antiarrhythmic drugs is undesirable due to negative inotropic effects.
Protective antiarrhythmic therapy
Long-term antiarrhythmic therapy is justified:
- in children of the first year of life;
- in young children with frequent seizures, with clinical manifestations or with chronic SVT;
- in older children if it is impossible to perform or refuses RFA.
Antiarrhythmic therapy is recommended to begin in the hospital.
Rhythm control will delay the onset of arrhythmogenic myocardial dysfunction and allow you to wait for the recommended timing of RFA.
To prevent recurrent attacks of supraventricular tachycardia
- PROPAFENONE at a dose of 8-15 mg/kg/day in 3 divided doses,
- VERAPAMIL at a dose of 3-7 mg/kg/day in 2-3 doses,
- AMIODARONE at a maintenance dose of 5 mg/kg/day in 1-2 doses,
- SOTALOL 2-6 mg/kg/day in 2 divided doses.
To control the rhythm frequency in children with chronic supraventricular tachycardia, digoxin and beta-blockers are also used.
Interventional treatment of supraventricular (supraventricular) tachycardias
RFA of tachyarrhythmias in young children is performed according to vital indications:
- pronounced clinical symptoms;
- hemodynamically significant arrhythmia;
- decreased LVEF;
- ineffectiveness of all antiarrhythmic drugs (including amiodarone).
- Indications for RFA in children over 10 years of age are comparable to indications for RFA in adults.
Forecast
Children with supraventricular tachycardia without congenital heart defects and organic myocardial diseases have a favorable prognosis.
The effectiveness of RFA is 85-98%.
Source
Source: https://www.cardioplaneta.ru/expert/cardiology/pediatrics/208-narushenie-ritma-serdca-u-detey-nadzheludochkovaya-supraventrikulyarnaya-tahikardiya.html
Preventive actions
To prevent the risk of seizures in young patients, doctors recommend that parents monitor the child’s lifestyle. They need to spend more time in the fresh air and engage in gentle sports, for example, swimming. A healthy diet is considered an important preventive measure. You will need to remove fried, spicy, fatty, salty and sweet foods from the menu. The main emphasis in the diet is on a sufficient amount of fruits and vegetables, products that contain potassium and magnesium. In addition, you can get useful substances from vitamin-mineral complexes, which are sold in pharmacy chains.
It is important to protect the child from stressful situations, to ensure that he does not become overtired, both physically and emotionally. If a small patient suffers from frequent attacks of paroxysmal tachycardia, he needs to be given antiarrhythmic and sedative medications prescribed by a specialist. In this case, under no circumstances should you change the dosage and regimen of taking the medication. If the disease occurs against the background of other heart pathologies, their therapy is mandatory, after which the tachycardia goes away on its own.
Read also: Tachycardia with cervical osteochondrosis
Paroxysmal tachycardia in a child
A heart rhythm disturbance, which is characterized by a rapid heartbeat and appears in the first 3 days of a child’s life, is called paroxysmal tachycardia in newborns. In this condition, the infant's heart rate reaches from 180 to 250 beats per minute. Also, such attacks can occur in young children, schoolchildren and adolescents. Attacks of paroxysmal tachycardia can cause serious complications from the cardiovascular system in a child, so when the first signs of pathology appear, you should immediately contact a specialist.
Symptoms
The most common symptoms are diseases of the genitourinary system, excess weight and even bad teeth. The heart muscle, not receiving proper nutrition and constantly being in a “stressful” state, quickly becomes unusable - this is the cause of rhythm disturbances.
In a child, this pathology may not have pronounced symptoms. But with more serious signs of damage, heaviness in the heart area, slight pain, attacks of irregular heartbeats, dizziness, and nausea are felt. This condition may cause the child to faint. With severe symptoms, disturbances in the blood supply to organs appear.
Paroxysmal tachycardia can cause ventricular fibrillation and circulatory failure. This is especially true for premature babies.
However, in young children, approximately one year old, signs of tachycardia, namely, rapid heartbeats, are not always symptoms of the disease. Most children tolerate attacks of tachycardia calmly. In a one-year-old child, these attacks are considered normal.
Symptoms of tachycardia
With paroxysmal tachycardia in children with the ventricular form, the following symptoms appear:
- interruptions in heart function;
- chest discomfort;
- the appearance of weakness and dizziness;
- strong fear;
- fainting;
- rapid breathing;
- the appearance of shortness of breath;
- pale or bluish skin;
- lethargy;
- increase in liver size;
- swelling of the body.
For the supraventricular form:
- pale skin;
- the appearance of severe sweating;
- frequent urination;
- the appearance of nausea and vomiting;
- protrusion of the neck veins;
- rapid heartbeat;
- popping and loud heart sounds;
- the appearance of lack of air.
Return to contents
Features of development in newborns
Paroxysmal tachycardia in infants is characterized by a sudden development of rapid heartbeat, which lasts at least a few minutes and at most several hours.
Tachycardia can manifest itself in the womb, as well as after birth.
This pathology can appear in the womb. It is characterized by the appearance of a heartbeat with a frequency of up to 200 beats per minute. If an attack occurs frequently and lasts a long time, it can easily provoke heart failure. Even during an attack, the newborn develops rapid breathing, bluish skin, the child becomes restless and cries. As a result of a prolonged attack, signs of insufficient blood supply appear - the development of encephalopathy and necrotizing inflammation of the intestine. It also leads to the formation of cardiomyopathies and fibrosis of the heart muscle.
Paroxysmal supraventricular tachycardia: treatment
Any malfunction of the heart muscle affects the human condition, and paroxysmal supraventricular tachycardia is no exception. This pathological condition manifests itself in the form of palpitations, which often begin suddenly. The main indicator of the painful state of the heart muscle is its contraction within the range of 120-250 beats/min.
The disease is paroxysmal in nature and can last from several minutes to several days.
Symptoms
Paroxysmal supraventricular tachycardia is most often observed. This species is distinguished by its striking manifestations. The onset of the attack occurs suddenly. The heart beats at a frequency of about 150 beats. Before this, interruptions in the functioning of the organ are noticed.
The attacks have different durations. For some, tachycardia continues for several minutes, while for others it lasts for many days. The condition can normalize without medical help.
Also read: Features of the development of ventricular parasystole
Increased heart rate is accompanied by vegetative symptoms:
- chills and trembling;
- sweating;
- feeling of lack of air;
- redness and blanching of the skin.
If a person suffers from a severe form of heart disease, or has a heart attack, he may lose consciousness. There is also a significant decrease in arterial pressure and the development of arrhythmogenic shock.
With functional disorders without serious cardiac pathologies and in young people, tachycardia is accompanied by slight weakness and dizziness, as well as interruptions in heart function.
Contributing factors and clinical manifestations
Like any ailment, painful palpitations have their own reasons for their development. All of them can be divided into two groups.
| Heartfelt | caused by ailments and structural elements of the cardiovascular system. These include pathologies of the development of the conduction system, diseases resulting from insufficient blood supply to the heart muscle, and pathological changes in the structure of the organ. Inflammation of the muscle layer, changes in its structure and functional deviations, as well as inadequate contraction can also provoke rhythm disturbances |
| Extracardiac | manifest themselves in ailments of organs not related to the cardiovascular system. We are talking about diseases of the endocrine gland, blockage of large branches of the pulmonary trunk with a blood clot, inflammation of the respiratory system, unbalanced functioning of the nervous system |
Smoking, alcoholism, stress, and intense physical activity can also trigger symptoms.
As for the clinical manifestations of supraventricular tachycardia, they are expressed in rapid heartbeat, chest discomfort, general weakness, nausea, shortness of breath, anxiety, dizziness, and fainting. It is noteworthy that the patient may be bothered by frequent urination.
Prevention methods
To avoid the development of tachycardia, it is necessary to promptly treat pathologies that are accompanied by such disorders. For example:
- coronary disease, in which the heart is insufficiently supplied with blood, can be prevented through a balanced diet, moderate exercise, and avoidance of alcoholic beverages and smoking;
- myocarditis is prevented by the same measures as other heart diseases.
Supraventricular tachycardia can be prevented by:
- Elimination of excessive psycho-emotional stress. Stress and conflict situations should be avoided.
- Giving up bad habits.
- Moderate physical activity.
- Rational and balanced nutrition. It is important to give up fried, fatty foods, salt, and introduce more vegetables and fruits into your diet.
- Controlling body weight and blood glucose levels.
In the case of a hereditary predisposition to pathology, it is necessary to undergo periodic examinations in order to detect the development of disorders in time and stop the process.
Classification of tachycardia and its manifestation on the ECG
This form of arrhythmia has several varieties.
- Atrial paroxysmal form is divided into focal and multifocal.
- Atrioventricular is divided into nodal, reciprocal and ectopic.
Manifestations of paroxysmal supraventricular tachycardia on an ECG are of particular importance in the diagnosis of the disease. The essence of the non-invasive research method, which is the most informative and safe, is to check the electrical conductivity of the heart muscle.
The main method of confirming or refuting a diagnosis is an ECG.
So, paroxysmal supraventricular tachycardia has the following ECG signs:
- a paroxysmal attack begins abruptly and also abruptly ends;
- heart rate exceeds 140 beats per minute;
- it is characteristic that the regularity of the heart rhythm is maintained;
- QRS complexes retain their normal appearance.
As for the P waves, they are different in visual diagnostics. For example, in conditions of the atrioventricular form of AT, the waves of group P are noted after each QRS complex, sometimes they overlap. But the atrial form of arrhythmia of the paroxysmal type is manifested in the fact that P waves are recorded before the complexes. Moreover, they are characterized by a noticeably deformed appearance.
Basic classification, differences between species by localization
Depending on the course, acute, permanent recurrent (chronic) and continuously relapsing forms . The latter type of course is especially dangerous, since it causes circulatory failure and arrhythmogenic dilated cardiomyopathy.
There are the following forms of paroxysmal tachycardia :
- ventricular - persistent (from 30 seconds), unstable (up to 30 seconds);
- supraventricular (supraventricular) - atrial, atrioventricular.
Supraventricular
The atrial form is the most common. The source of increased impulse production is the atrioventricular node. Brief seizures are often not diagnosed on an electrocardiogram .
The atrioventricular form is characterized by the fact that it arises at the atrioventricular junction.
For this form, the heart rate reaches 250 beats per minute, stopping paroxysmal tachycardia is performed using the vagal method.
Ventricular
The focus of excitation in the ventricular form is in the ventricles - the bundle of His, its legs, in the Purkin fibers . The ventricular form often develops against the background of cardiac glycoside poisoning (approximately 2% of cases). This is a dangerous condition that sometimes develops into ventricular fibrillation.
Heart rate usually does not “accelerate” more than 180 beats per minute . Tests with awakening of the vagus nerve show a negative result.
PNT therapy
As mentioned, the main way to diagnose the disease is an ECG. But besides this, a physical examination, general and biochemical (in the case of blood) analysis are required. Additional research may be required, for example:
- daily monitoring;
- transesophageal stimulation;
- electrophysiological study of the heart muscle;
- EchoCG.
Treatment of paroxysmal supraventricular tachycardia is prescribed after receiving the results of all studies. To provide first aid to someone having a seizure, you need to:
- throw back his head;
- lightly press on the eyeballs;
- If possible, immerse your face in cold water for 10-35 seconds.
An ice collar applied to the neck is effective. Straining the abdominal muscles can be used as a vagal technique.
After the patient contacts a doctor or an ambulance, conservative or surgical treatment may be prescribed.
Drug therapy is aimed at preventing attacks, for which antiarrhythmic drugs are prescribed. They are able to restore normal heart rhythm.
The doctor always prescribes medications based on the patient’s current condition and the presence of underlying diseases.
Today the most effective medications are:
| Beta blockers | Atenol, Metoprolol, Quinidine |
| Foxglove Products | Isoptin |
| Antiarrhythmic drugs | Procainamide, Aymalin, Verampil, Propaphenone, etc. |
Surgery
If drug therapy is ineffective, then surgery is prescribed to combat paroxysmal tachycardia. This method of treatment is resorted to if irreversible changes of a sclerotic nature have occurred in the main organ of the cardiovascular system or defects have been identified.
Source: https://gpk1.ru/zabolevaniya/nzht-serdca.html
Emergency care for paroxysmal tachycardia in children
Emergency care for the supraventricular form consists of the following steps:
- Massage the carotid node for up to 15 seconds, starting from the left side.
- Take a strong breath, hold your breath and strain. Stay in this state for up to 40 seconds (Valsalva maneuver).
- Mechanically tease the throat (gag reflex).
- Sedatives (Seduxen).
- Products containing magnesium (Panangin, Asparkam).
- Antiarrhythmic drugs (Diltiazem, Amiodarone).
- Cardiac glycosides - Digoxin.
- If there is no effect of drug therapy, electropulse therapy is used.
For ventricular form:
- vein catheterization is used;
- “Novocainamide” and “Mezaton” are administered;
- If the drugs are ineffective, electropulse therapy is used.
Return to contents
Diagnostic features
When the first signs of an attack of paroxysmal tachycardia appear in a child, you should urgently contact a pediatrician, cardiologist, neurologist and endocrinologist. They will collect all complaints, conduct an examination, differential diagnosis with other diseases and make a preliminary diagnosis. You will also need:
- general blood analysis;
- general urine analysis;
- blood chemistry;
- blood test for electrolytes;
- hormone tests;
- EchoCG;
- ECG;
- monitoring using the Holter method.
Return to contents
Treatment of paroxysmal tachycardia
A child with the supraventricular form is hospitalized in the somatic department, and with the ventricular form - in the intensive care unit.
The doctor prescribes an examination and the necessary treatment.
If an attack of paroxysmal palpitations occurs in a child, you should immediately consult a doctor. In the somatic department or intensive care unit, specialists will examine the patient and draw up an examination plan. After the diagnosis is made, medication or surgical treatment is prescribed, and recommendations are given on proper nutrition.
Drug therapy methods
The following drugs are prescribed to treat attacks:
- beta blockers (Sotalol, Metoprolol);
- calcium channel blockers (Verapamil, Diltiazem);
- antiarrhythmic drugs (“Amiodarone”, “Propafenone”);
- preparations containing magnesium and potassium (“Asparkam”, “Panangin”);
- cardiac glycosides - (“Strophanthin”, “Digoxin”).
Read also: Idiopathic tachycardia
Return to contents
Surgical treatment
An attack of paroxysmal tachycardia in a child is an emergency condition, therefore in some cases it involves the use of surgical treatment. Surgery is performed in children if drug therapy is ineffective or if such an attack lasts a long time and leads to serious complications from the cardiovascular system, gastrointestinal tract, brain and kidneys.
Signs of paroxysmal tachycardia
The onset of the disease is sudden. Attack duration:
- few seconds;
- several days
The frequency of arrhythmia is increased. According to clinical signs, the disease is divided into:
- essential type;
- extrasystolic type;
- supraventricular lesion;
- ventricular lesion
But the electrocardiogram does not give a clear clinical picture. Characteristics of the essential form of the lesion:
- an attack of an unexpected type;
- sudden end of attack
The extrasystolic type of lesion is a type of paroxysmal tachycardia. In this case, extrasystoles can be short-term or long-lasting. Tachycardia of the supraventricular type has a regular rhythm.
Patient complaints relate to the following:
- malaise;
- the phenomenon of paroxysm;
- squeezing;
- chest pain;
- breathing disorder
If the attacks are prolonged, then impaired breathing is a consequence. The following complications exist during prolonged attacks:
- blood stagnation;
- blood stagnation in the liver
The heart rhythm is disturbed with the ventricular type of lesion. The heartbeat has the form of a push. The following signs are revealed:
- dizziness;
- noise in the head;
- heart compression
Rare phenomena of the disease:
- phenomenon of hemiparesis;
- phenomenon of aphasia
Signs of vascular dystonia are also revealed. After an attack, the phenomenon of polyuria occurs. In this case, urine is released in large quantities. Signs of the patient's condition:
- hypotension;
- asthenia;
- fainting
A complex course of the disease is observed with cardiopathy. Complications with ventricular fibrillation are possible.
go to top
Preventing an attack
To prevent an attack, children are advised to lead a healthy lifestyle, eat right and get enough sleep. It is imperative to exclude physical and mental stress, and also follow all medical recommendations regarding drug therapy. Pregnant women are advised to regularly consult an obstetrician-gynecologist and monitor the condition of the fetus to avoid the occurrence of paroxysmal tachycardia in the newborn. If your child has repeated signs of an attack, you should immediately consult your doctor.
General characteristics of the pathology
Paroxysmal tachycardia is characterized by a sharp increase in heart rate. In young children the figures reach 200 beats per minute; for older children the numbers are lower - 150-160 beats per minute.
Paroxysmal tachycardia is usually divided into two forms:
- Ventricular. Pathology is caused by organic disorders of the heart muscle. This option is rare in children but is life-threatening.
- Supraventricular. It is also called supraventricular. In this case, the pathology is caused by impaired functioning of the autonomic nervous system, which controls cardiac activity.
Attacks of pathology appear in children for no apparent reason.
Paroxysmal ventricular tachycardia can be provoked by the following factors:
- carditis;
- cardiomyopathy;
- heart disease;
- autonomic dysfunction;
- hypo- or hyperkalemia;
- thyrotoxicosis;
- overdose of a heart drug (usually with digoxin or quinidine);
- overwork in physical or psycho-emotional terms.
Paroxysmal tachycardia in the supraventricular form occurs for other reasons. It can be called:
- hydrocephalus of the brain with high blood pressure;
- organic damage to the heart muscle;
- damage to the central nervous system that caused a neurotic disease;
- Wolff-Parkinson-White syndrome with a congenital anomaly of the heart structure;
- vegetative-vascular dystonia accompanied by sympathetic-adrenal crises.
In addition to provoking factors, the occurrence of pathology can be caused by a predisposition to it. The reason may be an unfavorable course of pregnancy and childbirth.
Seminar “SUPRAVENTRICULAR TACHYCARDIA IN CHILDREN: CLINICAL, DIAGNOSIS, TREATMENT METHODS”
Recommended pediatricians, family doctors, pediatric cardiologists, pediatric neurologists, neonatologists.
Relevance of the problem. Tachyarrhythmias are the most common and clinically significant cardiac arrhythmia (CHD) in children. The frequency of supraventricular tachycardias (SVT) in children without heart defects ranges from 1 in 250 to 1 in 1000; SVT accounts for 95% of all tachycardias in children. In approximately 50% of children, SVT is diagnosed in the neonatal period.
In most cases, SVT is not a life-threatening disorder; however, once it occurs, it persists for many years, significantly worsening the child’s quality of life. In some children, attacks of tachycardia have a severe clinical course and are accompanied by hemodynamic disturbances and syncope. A number of supraventricular tachycardias are associated with a risk of sudden cardiac death. Life-threatening conditions occur in children with Wolff-Parkinson-White syndrome, when tachycardia is combined with structural heart pathology, with chronic tachycardias, or when an arrhythmogenic effect occurs during the period of taking antiarrhythmic drugs (AAP) used to treat supraventricular tachycardias.
Currently, radiofrequency ablation (RFA) is a radical treatment method and is highly effective in most SVT. At the same time, antiarrhythmic therapy (AAT), used to relieve attacks of tachycardia, as well as to prevent repeated paroxysms or treat chronic forms in young children, remains effective. The clinical course, prognosis of the disease and the choice of treatment method are primarily determined by the mechanism of tachycardia, the age of the child and concomitant heart pathology.
General goal: to be able to diagnose and determine management tactics for a child with paroxysmal tachycardia.
Specific goals: to identify the main clinical and electrocardiographic signs of paroxysmal tachycardia, to draw up a plan for examining the patient, to make the most likely clinical diagnosis, to determine a plan of treatment and preventive measures.
Training content
Theoretical issues
- Definition of paroxysmal tachycardia (PT). Etiopathogenesis of PT in children. Clinical and electrocardiographic signs of various types of PT in children. Modern methods of examining children with PT. Principles of treatment of PT in childhood. Prognosis of the clinical course of PT in children. Measures to prevent PT in children.
Indicative basis of activity
During preparation for the lesson, it is necessary to familiarize yourself with the main theoretical issues using literature sources.
DEFINITION, CLASSIFICATION
Supraventricular (supraventricular) tachycardia (SVT) is three or more consecutive heart contractions with a frequency exceeding the upper limit of the age norm in children, with the localization of the electrophysiological mechanism above the bifurcation of the His bundle - in the sinus node, atrial myocardium, atrioventricular junction, orifices of the hollow and pulmonary veins, as well as arrhythmia with circulation of excitation waves between the atria and ventricles.
ICD X contains the following codes:
I 47.1 – paroxysmal supraventricular tachycardia, AV nodal tachycardia, ectopic (focal) atrial tachycardia;
I 45.6 – Wolff-Parkinson-White syndrome;
I 48 – atrial fibrillation-flutter.
M.A. Shkolnikova proposed the currently most widespread clinical and electrophysiological classification of supraventricular tachycardias:
- Clinical options for SVT:
- Paroxysmal tachycardia:
- stable (duration of attack is 30 s or more) unstable (duration of attack is less than 30 s)
- Chronic tachycardia:
- constant constant-return
- Clinical forms of SVT:
- Sinus tachycardia:
- Sinus tachycardia (functional). Chronic sinus tachycardia. Sinoatrial reciprocal tachycardia.
- Atrial tachycardia:
- Focal (focal) atrial tachycardia. Multifocal or chaotic atrial tachycardia. Incisional atrial tachycardia. Atrial flutter. Atrial fibrillation.
- Tachycardia from the AV junction:
- Atrioventricular nodal reciprocal tachycardia. Focal (focal) tachycardia from the AV junction.
- Tachycardias involving accessory pathways (APP):
- Paroxysmal orthodromic AV reciprocating tachycardia with the participation of AP. Chronic orthodromic AV reentrant tachycardia involving slow AP. Paroxysmal antidromic AV reciprocating tachycardia with the participation of AP. Paroxysmal AV reciprocal tachycardia with preexcitation (involving several APs).
METHODS AND ALGORITHMS FOR DIAGNOSIS OF SUPRAVENTRICULAR TACHYCARDIA IN CHILDREN
Diagnosis of SVT is based on its documented confirmation on an ECG. If tachycardia is registered, then the diagnostic search is primarily aimed at identifying its source, i.e. type of tachycardia, which is of fundamental importance for the scope of further examination, prognosis and choice of treatment method. If there is only an assumption that the child may have SVT, then the main task becomes confirmation of its presence.
The reason for the examination is complaints from the child or his parents about:
- repeated attacks of palpitations; syncope and presyncope of unknown etiology; repeated episodes of sudden weakness, lethargy in infants and young children; high pulse rate when examining the child.
- When analyzing the anamnesis, the age of the first attack, the connection with past diseases, and vaccination are essential; factors provoking SVT; seizure circadianity; their duration; cupping features; frequency of paroxysms during the month; Heart rate during an attack; subjective sensations during an attack. A clinical analysis of blood and urine is important to exclude an inflammatory process and anemia. When conducting a biochemical blood test, blood electrolytes, the level of “muscle breakdown enzymes” (troponin-I, creatine phosphokinase MB-fraction, lactate dehydrogenase-1), blood lipid spectrum (cholesterol, triglycerides; according to indications - high and low density lipoproteins), activity liver enzymes (AST, ALT), glucose; thyroid hormones (TSH, free T4, antibodies to thyroid peroxidase, including when prescribed and during treatment with cordarone). Standard resting ECG. ECG in 12 leads (or at least one lead) during an attack of tachycardia. Holter 24-hour or longer ECG monitoring. assessment of the state of the basic rhythm during the day and night, the presence of concomitant rhythm and conduction disorders, percentage of heterotopic rhythm, circadianity of arrhythmia, indicators of heart rate variability, assessment of the effectiveness of AAT. Stress tests (bicycle ergometry, treadmill test, psychological tests): study of the reaction of rhythm, myocardium and blood pressure to psycho-emotional and physical stress, identification of presumably blood-dependent and sympatho-dependent arrhythmias, determination of adaptation of the QT interval under load. Echocardiography (EchoCG) with Doppler analysis and color mapping: exclusion of structural heart pathology, assessment of morphometric parameters, identification of signs of arrhythmogenic dysfunction, assessment of the hemodynamic significance (efficacy) of tachycardia. Ultrasound of the thyroid gland. exclusion of organic changes in the thyroid gland, including when prescribed and during treatment with cordarone. EEG study. assessment of the state of bioelectrical activity of the brain, disturbances in the state of structures at the meso- and diencephalic level, identification of paroxysmal readiness of the brain, EEG patterns. Transesophageal electrophysiological study. reproduction and registration of tachycardia, conducting topical diagnosis of arrhythmia.
Symptoms of paroxysmal tachycardia in children
In half of the cases, the pathology manifests itself in the child in the evening or at night and lasts on average half an hour. Symptoms appear more clearly during evening attacks. The child becomes restless, feels general weakness, and his vision darkens. A pulsation begins in the temples, there is a feeling that the heart is about to jump out of the chest, there is not enough air. The child may feel dizzy, feel nauseous, and begin to gag.
Paroxysmal tachycardia is expressed by the following symptoms:
- pulsation of cervical vessels;
- pale skin;
- sweating;
- mild cyanosis of the lips and mucous membranes;
- emotional instability.
The child may develop a low-grade fever accompanied by chills. Urination often increases, and the urine is light in color.
In older children, this pathology can manifest itself as anxiety-depressive feelings and phobias. In most cases (90%), an attack is provoked by emotional rather than physical stress.
Tachycardia in a newborn
The expectant mother should pay special attention to the fetus in the womb. Constant and mandatory examination can help identify tachycardia in a child in the womb. The treatment methods used in this case will prevent the development of tachycardia in an infant.
During pregnancy, expectant mothers experience double stress. This means they need additional emergency care.
Supraventricular tachycardia developing during pregnancy can have serious consequences. That is why during pregnancy a woman is obliged to monitor her diet and physical health. Such care will help avoid the birth of a premature baby.
Doctors, both a cardiologist and a pediatrician, through joint efforts, will be able to prevent the development of tachycardia even in premature infants. Independent use of medications or folk remedies for pathologies during pregnancy should be excluded.
Diagnostics
It is quite simple to identify paroxysmal tachycardia. After a standard examination, the specialist prescribes electrocardiography and echocardiography. Each form of pathology has its own characteristics.
Ventricular tachycardia can be identified by the following signs:
- registration of outbreaks of sequential extrasystoles (formation occurs in the ventricles);
- there are 5 or more extrasystoles, and short periods of sinus rhythm are observed alternately with them;
- deformation of the QRS complex and widening from 0.1 seconds;
- the opposition of T waves to the main wave in the QRS complex;
- The R wave is difficult to determine due to its overlap with other elements.
Read also: Supraventricular tachycardia in children
With tachycardia of the panventricular type, 4-5 consecutive extrasystoles are also formed, but they are formed in the atria. Heart rate exceeds 160 beats per minute. The conduction of electrical impulses from the atria to the ventricles may be impaired, that is, atrioventricular block occurs (I, II degree).
Additionally, the Holter method, that is, daily monitoring, can be used. Instead, a transesophageal electrophysiological study may be prescribed.
Classification
Clinical and electrophysiological classification (Kruchina T.K., Egorov D.F., 2011)
- Clinical variants of NVT paroxysmal tachycardia: sustained (attack duration 30 s or more);
- unstable (duration of attack less than 30 s);
- constant;
- sinus tachycardia: sinus tachycardia (functional);
- focal (focal);
- AVNRT (atrioventricular nodal reentrant tachycardia): typical; atypical;
- paroxysmal orthodromic AVRT (atrioventricular reciprocal tachycardia) with the participation of APP;
Read also: Allergy tachycardia
Treatment of paroxysmal tachycardia in children
Features of treatment depend on the form of pathology.
Vagal tests
Vagal tests are of particular importance, as they make it possible to stop an attack of any type of pathology. The following manipulations must be performed:
- Massage the carotid artery area for 10-15 seconds on both sides.
- Perform the Valsalva maneuver. To do this, the child must inhale as much as possible and hold his breath for 10 seconds, holding his nose. While holding your breath, you need to strain your stomach.
- Provoke a gag reflex. For younger children, apply pressure to the stomach or wash with ice water. In this case, severe bradycardia or asystole may occur. Such consequences require treatment.
- Give a sedative. Usually they resort to valerian, Corvalol, Valocordin.
Stopping heart palpitations
During an attack, it is necessary to normalize the rapid heartbeat. The choice of drugs in this case depends on the form of the pathology.
In case of ventricular tachycardia, the attack is stopped by the following means:
- Trifosadenine;
- Gilurithmal;
- Amiodarone;
- sodium chloride solution;
- Lidocaine;
- glucose solution;
- Procainamide;
- Phenylephrine.
The use of the listed antiarrhythmic drugs is possible if the electrocardiogram showed a wide QRS complex. If such a study cannot be carried out, then Trifosadenine and Lidocaine are not used.
Antiarrhythmic drugs in the case of supraventricular tachycardia are used if vagal tests do not provide the desired effect. In this case, Trifosadenine, Digoxin, Verapamil are administered intravenously. When using antiarrhythmic drugs, it is necessary to monitor pulse and blood pressure.
Antiarrhythmic drugs are used sequentially. For example, for ventricular tachycardia, lidocaine is first administered. If there is no effect within 5-10 minutes, then the drug is re-administered, but the dosage is halved. If there is no result, they resort to Giluritmal. If this does not bring the desired effect, then Amiodarone is administered.
It is necessary to take medications that affect the central nervous system, that is, the cortical-subcortical relationship. Therapy with Phenibut, Carbamazepine, tinctures of valerian, hawthorn or peony is possible.
To regulate cardiac activity, taking Asparkam is necessary. This drug contains potassium and magnesium ions. The dosage must be calculated according to age; for young children, a third of the tablet is enough.
Requirements for regime and nutrition
During an attack of paroxysmal tachycardia, the child needs bed rest. The diet should be enriched with potassium and magnesium: it is necessary to include dried fruits (especially dried apricots and raisins), baked potatoes. You should give up chocolate, tea and coffee.
Electropulse therapy
Drug therapy does not always bring the desired effect, so it is necessary to use electrical pulse therapy. This means delivering a shock. The high voltage current interrupts the circulation of the excitation wave, which causes an abnormal heart rhythm. Paroxysmal tachycardia of any form is a relative contraindication to such effects.
Usually, electropulse therapy is used when the duration of an attack is more than a day. This measure is also necessary if there is a risk of developing heart failure.
Tachycardia in children: why does it occur and how to treat?
During childhood, changes occur in the growing body that are considered normal at a certain stage of life.
Parents should be aware of the boundary between the physiological state and the presence of pathology of the cardiovascular system. These include tachycardia in children. In one case it is a manifestation of the disease, and in the other it is a variant of the norm.
Knowing all the causes and accompanying symptoms, parents will be able to suspect pathology in time and consult a doctor.
What is tachycardia?
The term “tachycardia” in children refers to a variant of arrhythmia, the main manifestation of which is considered to be an increase in heart rate of more than 90 beats per minute.
The increased rhythm is associated with the anatomical features of the body. Catecholamines play the role of specific stimulants of myocardial activity. Negatively affect cardiomyocytes and disrupt electrolyte metabolism.
Dysfunction in the functioning of the heart appears when nervous excitability changes.
The myocardium contains a large group of cells that act as pacemakers. They operate at a frequency of 60-80 per minute. When the work of the nervous system increases, a signal is given that travels further along the conduction pathways of the heart.
Pacemakers (drivers) stimulate cardiomyocytes to do more work. This condition may be physiological, and after a short period of time, heart function returns to normal. Normally, sinus rhythm is maintained.
This does not happen under the influence of organic pathology. Already at an early age, arrhythmia appears, the main symptom of which is tachycardia in a child.
Causes of tachycardia in children
A child's cardiovascular system is affected by a number of factors. This often leads to increased heart rate. All reasons are divided into several large groups - external and internal. The first includes the following diseases and conditions:
- anemia;
- heart defects;
- myocarditis;
- endocarditis;
- vascular insufficiency (with fainting, shock).
At any age, stress performs a protective function and helps to adapt to negative external conditions. With its constant exposure, the nervous system is depleted. This often happens to schoolchildren. This is a common cause of tachycardia in childhood.
Physical activity causes a short-term increase in heart rate. Tachycardia in adolescents is associated with intense training and hormonal changes. The following external factors lead to this condition:
- Sudden change in body position.
- Mental disorders.
- Infectious diseases occurring with high body temperature.
- Pathology of the endocrine system – thyroid disease, diabetes, tumors.
- Dehydration of the body. Increased heart rate is the result of exhausting workouts during which the child drinks little water. Some girls follow a strict diet without understanding all its health hazards. An illiterate approach to losing weight is accompanied by a lack of nutrients and fluids.
- Drinking drinks containing caffeine - strong tea, coffee.
- Drinking alcoholic beverages, smoking tobacco. The most dangerous period is adolescence. A child (especially a boy) may fall into bad company. Holidays with such friends are accompanied by a desire to try alcohol or smoke for fun.
- Taking certain groups of medications - hormones, psychostimulants.
- Insect bites - bumblebees, wasps, bees, some arachnids.
In rare cases, it is not possible to establish the exact reason why tachycardia appeared. This occurs when young children are admitted to the hospital. In such a situation, it is difficult to fully collect all the necessary information. For this reason, parents should be more attentive to their baby. If palpitations occur, the diagnosis is clarified and treatment is prescribed.
Symptoms and signs in children of different ages
When tachycardia appears, the symptoms and treatment in children of different ages will be slightly different. It is taken as the norm during the entire period that an unborn baby is in the womb of a woman. After birth, the rhythm continues to be accelerated compared to adults.
As the child grows, it becomes rarer. By the age of 14, a teenager has a frequency of no higher than 90 beats per minute. Age periods at a certain stage of life are characterized by specific features. They appear simultaneously with tachycardia.
Child's age Normal heart rate (beats per minute) Associated signs and symptoms
| Newborn | 110-170 | 1. Pale skin and against its background the appearance of a blue color in the nasolabial triangle, earlobes, and tip of the nose. In more severe cases, the shade becomes more pronounced every month without treatment. Blueness may appear on the fingers and toes. 2. The main symptom is shortness of breath with the participation of accessory muscles. The supra- and subclavian fossae and intercostal spaces begin to sink. 3. A “sailing symptom” appears. It is considered a sign of severe respiratory failure. During the process of inhalation and exit, the cheeks first inflate and then retract. 4. Increased sweating. In some cases, after waking up, the baby's bedding becomes wet. 5. Increased heart rate, tense pulse. |
| Up to 12 months of life | 100-160 | |
| Up to 2 years | 95-155 | 1. The child becomes lethargic, sleeps constantly, and loses interest in games. 2. Increased and accelerated heart rate. |
| Up to 4 years | 92-140 | |
| Up to 6 years | 85-125 | 1. The above symptoms are accompanied by causeless nausea and vomiting. 2. Dizziness, darkening of the eyes and sometimes fainting.3. The appearance of visible veins in the neck. |
| Up to 8 years | 75-115 | |
| Up to 10 years | 65-105 | |
| Up to 14 years old | 60-95 | 1. Pain in the heart area. The child describes them as aching, occurring during physical activity or at rest. 2. Blood pressure below 120/80 mmHg. 3. The teenager feels a strong heartbeat and is sometimes bothered by a feeling of freezing. 4. Severe weakness that does not disappear after rest. |
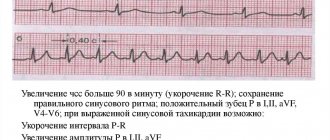
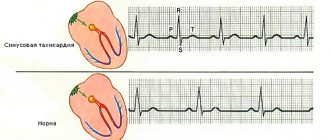
As for sinus tachycardia in children, the ECG image shows the same changes at any age. The gaps between the R-R teeth are reduced. When the causes of such a condition are of organic origin, they will be at different distances. If pathology appears on examination, additional signs will appear.
Diagnostics
Tachycardia is detected by interviewing parents and examining their child. The information obtained helps to establish the cause of this condition. If necessary, treatment is prescribed. The examination includes the following methods:
- ECG (Electrocardiography).
- Holter monitoring ECG.
- Electrophysiological study (EPS) - transesophageal or intracardiac.
- Load tests.
- MRI.
An ECG image for various forms of tachycardia provides data characteristic of a certain spectrum of diseases. Depending on the pathology and heart rate, therapy is prescribed. It is carried out under the supervision of examination and additional research methods.
In childhood, a sinus variant of tachycardia is most often detected on the cardiogram. It does not exceed 150 beats per minute. The rhythm remains within normal limits, and the P wave remains positive.
The supraventricular form differs from that described above. The contraction frequency can be 250 per minute. QRS remains normal. The P wave may have changes in the form of:
- negative option;
- deformed;
- two-phase.
The electrocardiogram with the ventricular form of tachycardia looks altered. The QRS complex is deformed, and the child’s heart rate remains within the range of 160-210 beats per minute. Dissociation may occur when the ventricles contract in their own rhythm, and the atria in their own.
If the child does not have the paroxysmal variant, then the above symptoms will persist. There are differences in the number of heart contractions. Children are characterized by moderate tachycardia in the range of 110-120 beats per minute.
In addition to the electrocardiographic method, Holter monitoring is used. All data is collected within 24 hours. For this reason, it is carried out only among older children. The results, which are obtained within 24 hours, are assessed by a doctor. Sometimes questions remain in clarifying the form of tachycardia or it is difficult to find its cause.
To resolve controversial issues or confirm the diagnosis, a transesophageal examination is performed. The method allows you to evaluate the lesions that provoked the increased rhythm and caused associated symptoms.
For ventricular and supraventricular forms of tachycardia, stress tests are indicated. A treadmill test or bicycle ergometry is used. They are given to older children.
It is important to consider all possible complications and contraindications. If a child has a ventricular variant, then caution is needed. This is associated with a high risk of developing an attack, which occurs during intense physical activity.
In unclear situations (or to obtain complete information about the condition of the heart), a magnetic resonance imaging (MRI) study is performed. A complete examination allows you to get a clear picture and assess the severity of the pathology.
Treatment
In most cases, the heart rate accelerates with excitement, physical activity and hormonal changes in adolescence. If there is no organic pathology, then you need to calm down - this is often enough to normalize the condition. According to indications, the child is prescribed medications, or he is sent to a surgical hospital for surgery.
Drug therapy
Organic pathology is considered the main indication for prescribing medications. Children can be given drugs from the following groups:
- beta-blockers ("Pindolol");
- cardiac glycosides (Digoxin);
- calcium antagonists (“Verapamil”);
If there is no effect from the therapy, if complications arise or the child’s condition worsens, the child is referred for surgery. During pregnancy in girls under 18 years of age, possible contraindications are clarified.
Non-drug therapy
When tachycardia interferes with the quality of life, then, according to the recommendations of Dr. Komarovsky, you need to use therapeutic methods:
- Massage of the carotid sinus in the neck in the area of the carotid artery. It should not be performed for a long time, so as not to lead to an excessive slowdown of the heart rate.
- Short-term straining of the abdominal muscles, lasting 1.5-2 minutes.
- Covering the face with pieces of ice.
- Pressing on the eyeballs while lying down.
If the methods alleviate the condition for a short time or are completely ineffective, then the child is given herbal sedatives. If there are contraindications, they cannot be used. The most popular are motherwort and valerian. In most cases, this is also used for emergency purposes.
When all attempts do not lead to positive dynamics, the patient undergoes surgery. Depending on the disease that causes tachycardia, the child will be treated comprehensively. Before this, medication preparation may be required.
There are several surgical options:
- Radiofrequency ablation of veins (rejection of tissue under the influence of radiation).
- Installation of an artificial pacemaker.
- Replace valves when indicated.
- Heart transplant, depending on the severity of the condition.
After the operation, the child must be under medical supervision. It is necessary to follow a diet excluding harmful foods from the diet, drink more water (1.5-2 liters per day).
Complications
Complications are likely only in severe forms of diseases that cause tachycardia. The main ones are the following:
- arrhythmogenic shock;
- pulmonary edema;
- heart failure;
If help is not provided in time, cardiac arrest and death are possible.
Forecast
With physiological tachycardia there is no threat to health; it does not turn into illness over time. If an abnormal heart rate is caused by a disease, then the prognosis is assessed based on the variant of the pathology. The ventricular form is considered the most unfavorable. With timely treatment and surgical correction, there will be no threat to health in the future.
Parents should remember that following the doctor's recommendations will save the child's life. For this reason, it is important to undergo routine examinations and (if necessary) comprehensive treatment.
Full-fledged drug therapy together with non-drug therapy leads to positive dynamics.
If the disease was identified at an early stage of development, then this approach is sufficient for the patient in most cases.
Consequently, tachycardia in children can develop under the influence of both physiological and pathological processes. To recognize the true provocateur of the pathology, the child needs to undergo a series of diagnostic examinations, and parents need to be attentive to various symptoms and signs that indicate a possible pathology of the cardiovascular system.
Source: https://MirKardio.ru/bolezni/uchashhenie/tahikardiya-u-detej.html