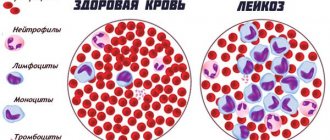
Embolism is a complex pathological process that occurs in the bloodstream, as a result of which the leading vessel is suddenly blocked and the blood supply to organs and tissues is disrupted.
Embolism in the aorta, large arteries occurs with cardiac pathology. Essentially, this is the process of transporting small particles through the bloodstream closer to the central organs. Most often, the material for emboli is formed from broken pieces of blood clots. And blood clots form in the atria. Research shows that up to 40% of cases are associated with atrial fibrillation.
Causes of embolism
The causes of embolism are varied. Blood clots along the walls of the left ventricle occur when the heart muscle is damaged. This is typical for a cardiac aneurysm or extensive myocardial infarction. In the systemic circulation, arterial embolism occurs when a blood clot moves from the heart to the periphery, causing thrombosis in the extremities, in the intestinal mesentery, splenic, renal and cerebral vessels. With heart defects associated with pathological communication between the left and right parts of the heart chambers, emboli can get from the venous bed into the arteries. This type of vascular embolism is called “paradoxical”.
What are emboli formed from?
The types of embolism depend on the “building” material of the detached microparticles.
- Most often, these are glued platelets, leukocytes and fibrin, forming a loose thrombotic mass with increased blood clotting.
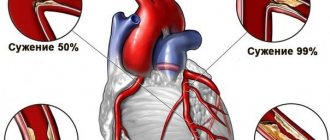
- An atherosclerotic plaque protruding into the lumen of a vessel can break off with a strong wave of blood and move along the vascular bed. It consists of dense deposits of cholesterol.
- Fat embolism occurs in severe injuries with blood loss, multiple fractures, during operations on the bones of the leg, thigh, pelvis, and in overweight individuals. In this case, fatty substances dissolved in the blood turn into an embolus due to a sharp change in their concentration. There is also an opinion about the direct tearing off of small particles of adipose tissue and washing them into the bloodstream.
You can read about air embolism here.
The further fate of the blocked vessel and consequences
Arterial embolism contributes to narrowing or complete obstruction of the vessel. The consequence is a malnutrition of the organ that receives blood through this branch. At the site of blockage of the vessel, the speed of blood flow slows down, this helps the formation of a secondary thrombus. The viability of the affected organ depends on the rate of formation of a network of collaterals, additional vessels bypassing the blocked one. If the possibilities are good, they develop within a few hours and completely replace the lost blood supply.
For this, the following are important:
- the ability of the heart to eject blood under increased pressure to open supporting vessels and increase blood flow;
- properties of the vessels themselves to eliminate spasm.
In case of heart disease with chronic or acute heart failure, severe atherosclerosis, such results cannot be expected.
Drug 93 (39) (7). Phlegmon of subcutaneous tissue.
GE staining.
Micro: Loose connective tissue is abundantly infiltrated with leukocytes. Exudate is diffusely distributed between cellular and stromal elements. The tissue is swollen.
It is a manifestation of purulent inflammation. Purulent inflammation with a predominance of exudation and the formation of exudate in tissues infiltrated by neutrophils.
Cellulitis is a diffuse purulent inflammation in which purulent exudate spreads diffusely between tissue elements, stratifying and saturating them.
Etiology: pyogenic (pyogenic) microorganisms, possibly aseptic purulent inflammation.
Pathogenesis: During inflammation, an exudate rich in neutrophils is formed and infiltrates the thickness of the tissue. In addition to neutrophils, pus contains a certain amount of lymphocytes, macrophages, microbes, and damaged tissue elements.
Outcome: abscess breakthrough, petrification, development of amyloidosis.
Diseases: phlegmon.
Clinical significance: histolysis (tissue destruction), peritonitis (if phlegmon develops in internal organs).
Drug 263 (103). Phlegmanous-ulcerative appendicitis .
GE staining.
Micro: all layers of the process wall are diffusely saturated with exudate containing a large number of leukocytes. Tissue structures undergo purulent melting. The mucous membrane is completely destroyed with the formation of ulcerative defects.
Appendicitis is inflammation of the appendix of the cecum. It is a form of destructive appendicitis.
Etiology: unknown, but there are several theories: caprostasis theory, angioneurotic theory, autoimmune, infectious, etc.
Complications: gangrene of the appendix, perforation, peritonitis, peritiphlitis, empyema of the appendix, periappendiceal abscess, metastatic abscesses in the liver, thrombophlebitis.
Clinical significance: development of local and then diffuse peritonitis, adhesions, typhlitis, empyema of the appendix.
Cause of death: peritonitis (severe intoxication).
Drug 214 (116). Chronic bronchitis with bronchiectasis .
GE staining.
Micro: lung tissue is low in air, sclerotic. In the alveoli and interstitial septa there is an abundance of Lf and foci of acinous pneumonia with a serous-leukocyte infiltrate. (exudate). The wall of the middle bronchus is thickened due to inflammatory edema and sclerotic. In some places, the lumens of the bronchi are expanded (bronchiectasis filled with thick mucus, the epithelium is thickened, the muscle layer is in the stage of atrophy).
Chronic bronchitis is a chronic inflammation of the bronchi that occurs as a result of prolonged acute bronchitis or prolonged exposure to physical or chemical factors on the bronchi.
Etiology: biological factors (causative agents of acute respiratory infections and ARVI), physical and chemical factors (smoking, dust), allergic.
Complications: atelectasis, obstructive emphysema, chronic pneumonia, pulmonary fibrosis. Complications associated with bronchiectasis: amyloidosis, bleeding, cor pulmonale.
Outcomes: see “Complications”.
Causes of death: chronic congestive heart failure, heart failure, abscess formation.
Drug 91 (10) (24). Microbial embolism (embolic kidney abscess).
Micro: microbial emboli in the lumens of small vessels. Around them there is leukocyte infiltration with tissue melting (abscess).
It is a manifestation of microbial embolism.
Definition: microbial embolism - circulation of microbes in the blood and blockage of blood vessels by them.
Etiology: lumps of stuck together bacteria, fungi, animal parasites, protozoa, purulent fusion of a blood clot.
Pathogenesis: With the blood flow, microbes enter the capillaries, the lumen of which is obstructed. Metastatic ulcers form at the site of blockage of blood vessels. In case of embolism of vessels of the pulmonary circulation - in the lungs, of the systemic circulation - in the kidneys, spleen, and other organs.
Diseases: purulent diseases, sepsis, thrombosis.
Outcome: sepsis.
Clinical significance: mechanism of spread of purulent infection.
Macropreparations
Liver abscess.
Macro: on the section there are greenish-yellow lesions (abscesses) and filled cavities
pus.
Microbial embolism is embolism of blood vessels by microbial cell bodies.
Etiology: bacterial inflammation in various organs and tissues.
Diseases: various bacterial and purulent lesions of internal organs
(abscesses, phlegmons, etc.)
Outcome: generalization of the process, intoxication and death.
Amyloid nephrosis.
Macro: the kidney is dense, reduced in size.
These changes are a manifestation of amyloidosis.
Amyloidosis is a mesenchymal dysproteinosis accompanied by deep
disorders of protein metabolism and the formation of a complex substance in tissues - amyloid.
Etiology: dysproteinemia, pathological AG-AT reactions, malignant
neoplasms, chronic inflammatory diseases.
Diseases: tumors, chronic infections (tuberculosis), purulent-destructive
diseases, rheumatic diseases.
Clinical significance: parenchymal atrophy, organ sclerosis, functional
organ failure.
Warty endocarditis of the mitral valve.
Macro: The valve leaflet is thickened, blood clots are visible along the closure line (in the form
warts) with the beginning of the organization
It is a manifestation of rheumatoid endocardial damage.
Complications Development of heart defects, thromboembolism.
Outcome: Sclerosis and hyalinosis of the endocardium.
Clinical significance: myocardial hypertrophy, venous congestion (VC).
Causes of death: decompensated heart disease, thromboembolism.
Typhoid fever (changes in the follicles of the small intestine).
Macro: Peyre's patches protrude into the intestinal lumen. Their surface
wavy, reminiscent of the surface of a GM, gray-pink, juicy in appearance.
Typhoid fever is an acute intestinal infectious disease, anthroponosis.
Etiology: Salmonella typhi.
Stages of changes in the intestines: 1) Stage of group brain swelling
follicles; 2) Stage of necrosis; 3) Stage of ulcer formation; 4) Stage of clean ulcers; 5) Stage
healing.
Complications: bleeding, perforation of ulcers, peritonitis, pneumonia, purulent
laryngeal perichondritis, waxy necrosis of the rectus abdominis muscles, osteomyelitis, abscesses
in other organs.
Clinical significance: bleeding, peritonitis, sepsis, pneumonia.
Brown induration of the lungs with GR infarction
triangle with the base facing the pleura.
It is a manifestation of general venous stagnation.
Venous plethora is increased blood supply to an organ or tissue due to
obstruction of blood outflow, while blood flow is unchanged or reduced.
Etiology: chronic heart failure.
Diseases: ischemic heart disease, heart defects, cardiomyopathies, myocarditis, fibroelastosis
myocardium, post-infarction cardiosclerosis.
Outcomes: progressive pneumosclerosis and hemosiderosis.
Gangrene of the small intestine
Macro: the intestinal wall is edematous, black, the serous cover is dull. In vessels
mesentery red blood clots.
Etiology: thrombosis, thromboembolism, stenosis or compression of mesenteric vessels.
Diseases: atherosclerosis, adhesive disease (with compression of mesenteric vessels),
vasculitis, diseases accompanied by a violation of the rheological properties of blood.
Clinical significance: intoxication - death.
Gangrene of the foot
Macro: black fingers with macerated epithelium and skin ulcers. On
The demarcation zone is clearly visible on the dorsum of the foot.
These changes are a manifestation of artery blockage.
Cause: obstruction of artery patency.
Diseases: atherosclerosis, hypertension, diabetes mellitus, vasculitis.
Possible outcomes: organization and formation of a scar, purulent melting.
Hydronephrosis.
Macro: the volume of the kidney is increased due to the expansion of the pelvis and calyces. Parenchyma
the organ is thinned, transforming the organ into a thin-walled multi-chamber sac.
Diseases: all diseases leading to disruption of the outflow of urine from the kidney
(nephrolithiasis, strictures of the ureters and urethra,
benign prostatic hyperplasia, prostate cancer, kidney and retroperitoneal tumors
spaces with compression of the ureters, etc.)
Clinical significance: development of renal failure, uremia, death.
Previous2Next
Clinical picture
Embolism of a limb vessel
Manifestations of the disease depend on the diameter of the vessel and the organ or part of the body supplied from it. A sign of limb artery embolism is acute pain. The mechanism of pain is considered to be overstretching of the artery wall at the site of the thrombus and irritation of the nerve fibers. Vascular spasm occurs reflexively. At night the pain intensifies.
On palpation, you can feel the absence of a pulse below the site of thrombosis. The skin of the limb turns white and becomes cold to the touch. Blue spots appear on the fingertips. There is a decrease in skin sensitivity.
After 6 - 8 hours from the moment of embolism, if the blood supply is completely stopped, symptoms of tissue necrosis (gangrene) appear. At the same time, the pain becomes very intense. Dry gangrene usually develops.
For fat embolism
Clinical manifestations occur 1–2 days after injury, surgery or other critical condition. There are two types of embolism:
- pulmonary - occurs in 60% of all cases, the patient suddenly develops suffocation, blue face, cough with hemoptysis, possible pulmonary edema;
- cerebral - sudden loss of consciousness or loss of orientation, agitation, delirium, convulsions.
- At the same time, signs of acute heart failure appear: drop in blood pressure, tachycardia, rhythm disturbance.
You can read more about fat embolism in this article.
For pulmonary embolism
Pulmonary embolism is a complication not only of heart disease, but also of surgical interventions. After surgery, it develops unexpectedly during the patient’s recovery against the background of a general improvement in condition, even before discharge from the hospital. Statistics indicate up to 6% of this postoperative complication. The frequency directly depends on the duration of the operation.
In case of heart disease (acute myocardial infarction, aneurysm, defects, atrial fibrillation), embolism into the pulmonary artery is possible. The largest vessel is not always clogged. Most often, the embolus enters the narrower artery of the lower lobe of the right lung. If the main vessel is damaged, death occurs. Clinical symptoms do not have time to develop, but when examining the deceased, attention is paid to the sharp redness of the upper parts of the body.
If the embolus is localized in small branches, it causes a pulmonary infarction. The patient complains of sharp, sudden pain in the side, shortness of breath, cough, sometimes with hemoptysis. Following a heart attack, pneumonia and pleurisy develop.
Three groups of symptoms can be distinguished:
- neurovascular - anxiety, fear, pain in the heart, palpitations, decreased blood pressure;
- pulmonary - pain in the side, hemoptysis, cough, shortness of breath;
- general - fever, yellowness of the skin and sclera, leukocytosis in the blood test.
For abdominal aortic embolism
Embolism of the abdominal aorta is more common in rheumatic heart disease. The embolus is located at the branch of the aorta and leads to subsequent secondary thrombosis. The main symptoms are sudden pain in the legs, their pallor and coldness, and the disappearance of pulsation in the arteries of the foot. The pain radiates to the perineum, lower abdomen, and sacrum.
The consequences of an embolism can be paralysis and numbness of the legs. The patient is in shock. Gangrene develops quickly. If smaller arteries are affected, patients complain of weakness in the legs, lameness and pain when walking. Men experience erectile dysfunction.
With embolism in the renal artery
Renal artery embolism leads to the development of renal infarction. Patients report sharp pain in the lower back in the absence of dysuric phenomena (sharpness when urinating, increased urination). After two days, blood appears in the urine. Possible increase in blood pressure. In severe cases, pain throughout the abdomen, bloating, vomiting, stool and urine retention.
Video about pulmonary embolism:
Types of embolism and its consequences
Embolism (from the Greek embole - wedging, pushing) is a blockage of blood vessels by particles brought by the blood or lymph flow. The particles themselves (body) are called emboli. They can enter blood vessels from the external environment and form in the body itself. Therefore, emboli of endogenous and exogenous origin are distinguished.
According to the location, embolisms of the systemic and pulmonary circulation and portal vein embolism are distinguished.
Embolism leads to ischemia and tissue necrosis.
Embolisms of exogenous origin. An air embolism is caused by atmospheric air entering the blood vessels. More often it occurs with injuries to large veins, especially the jugular. The pressure in the veins is low or negative, the walls of the veins collapse slightly, and conditions arise for air to be sucked in. Air bubbles travel through the bloodstream into the right atrium and right ventricle and cause pulmonary embolism.
The cause may be the accidental entry of air into the vessels during careless intravenous administration of drugs to animals.
Gas embolism develops as a result of blockage of blood vessels by gas bubbles. An increase in atmospheric pressure creates conditions for the dissolution of gases (nitrogen, oxygen, carbon dioxide) in biological fluids. The rapid movement of the body from an environment with increased pressure to an environment with normal pressure leads to a decrease in solubility, desaturation and the formation of gas bubbles in the blood. Gas bubbles, mainly nitrogen, cause blockage of the capillaries of the brain and spinal cord, kidneys, heart and other organs. Gas embolism also occurs when the body is quickly transferred from an environment with normal atmospheric pressure to an environment with reduced atmospheric pressure. Blockage of blood vessels by gas bubbles is also possible with gangrene caused by anaerobes (gas gangrene).
Bacterial embolism occurs when conglomerates of microorganisms enter the bloodstream. The source of bacterial conglomerates can be one of the types of purulent inflammation - empyema, abscess, phlegmon.
Parasitic embolism occurs when larval forms of helminths enter the bloodstream and migrate through the circulatory system, for example, from the intestines to the lungs (roundworms, dictyocaula). Embolism of parasitic origin is also possible as a result of pathogens of mycoses entering the bloodstream (actinomycosis, etc.).
Embolism by foreign bodies entering the bloodstream when the vessels of the systemic and pulmonary circulation are injured. These types of bodies include fragments of mines, shells, bullets, and other objects. The mass of such foreign bodies is high, so they can move retrogradely, against the blood flow.
Embolism of endogenous origin. Based on the material from which emboli are composed, they are divided into several types.
Thromboembolism is caused by pieces of a broken blood clot. This is a fairly common form of embolism, especially in equid animals, occurring during delafondiosis. The larvae of this parasite migrate from the intestine, reach the mesenteric arteries, injure the vessel wall and settle in the resulting blood clot. Loose masses of the thrombus break off and turn into emboli, clogging the small branches of the mesenteric arteries.
Thrombi, as a source of emboli, can form in various parts of the bloodstream (veins, heart, arteries).
Fat embolism follows the entry of fat droplets into the bloodstream during operations on tissues with an abundance of fatty tissue, during fractures of tubular bones, after mechanical crushing of adipose tissue. Due to the negative pressure in the veins, droplets of fat enter the bloodstream through the injured areas of the vessel and stop in vessels of smaller diameter.
Fat embolism is easy to observe under a microscope in the capillary network of the leg or mesentery of an anesthetized frog after vegetable or petroleum jelly is injected into the cavity of its heart.
Tissue embolism occurs when tissue elements from foci of necrosis or ulcerative decay enter the bloodstream. An embolism caused by detached cells of a malignant tumor is possible. Cancer cells move primarily through the lymphatic pathways, while sarcomatous cells travel primarily through the bloodstream. The significance of such an embolus is not only in the disruption of blood and lymph flow, but also in the formation of a new focus of tumor growth (tumor metastasis).
Foreign particles can cause embolism in the pulmonary and systemic circulation and vessels of the portal vein system.
Embolism of the pulmonary circulation. Emboli close the lumen of the pulmonary arteries. Foreign particles enter the pulmonary arteries from the venous vessels of the systemic circulation and the right half of the heart. The consequences depend on the composition, size of emboli, and their total mass. Multiple embolism of small pulmonary arteries is especially dangerous. Blood flow is disrupted. Blood pressure in the vessels of the pulmonary circulation increases, blood flow into the left atrium and ventricle is limited, stroke and cardiac output decreases, and blood pressure drops sharply. Hypotension is a characteristic sign of massive embolism of the vessels of the pulmonary circulation. A decrease in blood pressure negatively affects the functional activity of the heart itself due to myocardial hypoxia. A drop in blood pressure is combined with a significant increase in systemic venous pressure with the development of acute right ventricular failure (acute cor pulmonale syndrome).
Pulmonary embolism is accompanied by changes in blood gas composition. Shortness of breath occurs as a reflex reaction to irritation of the chemoreceptors of the reflexogenic zones of the systemic circulation and as a reaction from the receptor fields of the pulmonary circulation system. Shortness of breath helps to increase blood oxygenation and release it from CO2.
Embolism of the systemic circulation. Emboli enter the vessels of the systemic circulation in various ways. One of them is the passage of air bubbles through the pulmonary capillary network. They stretch out, take the shape of a vessel and flow from the pulmonary circulation into the large one. In a similar way, droplets of fat can penetrate into the bloodstream of the systemic circulation. Lesions of the left half of the heart and its valve apparatus can give rise to thromboembolism, tissue embolism. The formation of blood clots in the arteries of the systemic circulation, which occur in animals after the introduction of parasite larvae, causes thromboembolism. Arteries of the systemic circulation can be the site of localization of tumor cells.
The mesenteric arteries, arteries of the kidneys, spleen, brain, and heart muscle are most often affected by embolism.
Portal vein embolism. Emboli enter the liver portal system from a large number of venous vessels of the abdominal organs. Blockage of the portal vein by emboli is accompanied by severe hemocirculation disorders. Portal hypertension occurs with venous hyperemia of the abdominal organs - the stomach, small and large intestines, kidneys, spleen. This causes disruption of digestion and the main functions of the liver - protein and bile formation, detoxification. Venous hyperemia of the abdominal organs, an increase in hydrodynamic pressure in the veins and a decrease in oncotic pressure are accompanied by the release of transudate into the abdominal cavity and the development of ascites. Portal hypertension is characterized by general circulatory disorders: blood flow to the cavities of the heart is limited, stroke and minute volumes of ejected blood, and blood pressure are reduced. As a reflex, in response to hypoxemia and hypercapnia, shortness of breath develops, followed in severe cases by respiratory arrest.
The severity of the patient's condition is determined by the fact that the portal vein can accommodate up to 90% of the volume of circulating blood and the inability of the remaining part to provide normal blood supply to the animal body.
The consequences of embolism of various origins depend on:
· the functional significance of the organ in which the blood vessels are blocked for the life of the body. Embolism of the coronary, cerebral, mesenteric, and pulmonary arteries can lead to rapid death, which is not observed with embolism of the vessels of striated muscles, bone, and some other tissues;
· composition of foreign particles. Air is relatively easily absorbed, fat is emulsified and saponified, tumor cells form metastases, purulent bodies provoke the formation of a new focus of inflammation, foreign objects are encapsulated, etc.;
· embolus size. The larger it is, the larger the vessel will be blocked;
· reflex spasm of nearby and distant vessels, provoking systemic pathology;
· development of anastomoses in the basin of a blocked vessel. The more there are, the faster blood circulation through the collaterals will be restored.
Diagnostic problems
Diagnosis of embolism is difficult because it is limited in time. Pathological changes develop suddenly and very quickly lead to irreversible conditions. It is important to ask the patient about past illnesses, examine and check the pulse in the extremities.
Information about incipient thrombus formation can be provided by:
- blood clotting test;
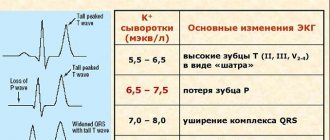
- a set of signs on the ECG;
- chest x-ray;
- Ultrasound examination of large veins and abdominal organs.
Vascular angiography is performed according to clinical indications in large vascular centers and specialized departments.
Catheterization of the heart cavities is possible.
Signs and symptoms
The nature of the symptoms of the pathology depends on the location of the blocked vessel. If the medicinal solution enters the pulmonary arteries, the patient may experience the following symptoms:
- coughing;
- breathing problems;
- short-term attacks of suffocation;
- feeling of squeezing in the sternum;
- blue discoloration of the skin.
At the very beginning of development, oil embolism manifests itself weakly. In this case, the patient experiences pain at the injection site. When necrosis occurs, the symptoms become more complicated: swelling occurs, the skin turns blue, body temperature rises, etc.
If you have an allergy, the patient may develop anaphylactic shock.
Identifying a disorder is difficult because it manifests itself in different ways. If an oil embolism is suspected, the specialist conducts a visual examination and examines the patient's medical history.
Important information: How to treat hemorrhagic diathesis and its symptoms
Additionally, a biochemical blood test, radiography and ultrasound examination are prescribed.
Treatment
It is impossible to know for sure about embolism in advance; however, the likelihood of its occurrence should always be expected with appropriate surgical interventions and treatment of heart disease. Therefore, to prevent embolism, drugs that reduce blood clotting are prescribed, and carious teeth and other foci of chronic infection must be treated before a planned operation.
Treatment of embolism is carried out in four main areas:
- maximum preservation of the ischemic organ;
- anti-shock measures;
- removal of the embolus and restoration of vessel patency;
- prevention of sepsis through the use of antibiotics.
Most often, the measures are equated to resuscitation. The patient is transferred to artificial respiration, large doses of Fibrinolysin, Heparin are administered to dissolve the blood clot, fluids that normalize the properties of blood (Reopoliglyukin), drugs to activate collaterals, and hormonal agents.
Catheterization of large vessels and the heart is possible only in specialized clinics; it will be successful if applied within minutes after an embolism.
One of the newest developments for the prevention of embolism is the installation of special filters in large vessels that do not allow emboli into vital arteries.
To avoid embolism in the future, you need to prevent disease and maintain health now.
More articles on the topic of embolism
Source: icvtormet.ru
What it is
First of all, an embolus is a mass that gets stuck while passing through a blood vessel and causes a blockage. Fat embolism of blood vessels is caused by a conglomerate consisting of fatty acids.
In other words, these are droplets of fat that enter the bloodstream and block the blood vessel. This condition is difficult to diagnose and the prognosis is not always favorable.
Causes
The most common cause of this disease is a fracture of a long bone. When it breaks, fat from the bone marrow can leak into the bloodstream.
In fact, most broken bones cause these droplets to enter the circulatory system. But not all of this fat causes blockages—closed fractures cause more of them than open ones.
Other reasons include major surgeries such as hip and knee replacements. Pancreatitis, burns, childbirth, bone marrow biopsy, and soft tissue damage also contribute to the development of the disease. These also include non-traumatic procedures or conditions such as liposuction, fatty liver disease, or sickle cell disease.
What it is - vascular fat embolism can be found out from your doctor. He will identify the degree of risk of pathology and give the necessary recommendations.
Air embolism
An air embolism
is a blockage of the bloodstream by air bubbles that enter the bloodstream from the external environment. Clinical manifestations depend on the type and size of the affected vessel. The most dangerous is obstruction of the coronary and pulmonary arteries, the blood supply system to the brain.
When the pulmonary artery is damaged, signs of acute respiratory and cardiac failure occur. The cerebral form of the disease occurs with the development of symptoms of ischemic stroke. The diagnosis is established on the basis of the clinical picture, Doppler ultrasound, capnogram, and CVP measurements.
Specific treatment is gas aspiration through a catheter, restoring the integrity of the vascular bed.
Air embolism (AE) is an acute pathological condition that occurs when outside air enters a blood vessel. The amount of gas administered at once must be at least 10-20 ml, otherwise it will dissolve in the blood without causing harm.
The pathology is considered quite rare, accounting for no more than 2% of all possible types of vascular occlusion. It is determined with equal frequency in men and women and is not related to age. Mortality with timely diagnosis and provision of qualified assistance ranges from 10 to 40%.
The lack of medical assistance during embolization of pulmonary and cerebral vessels leads to the death of the patient in 90% of cases.
Air embolism
Spontaneous entry of air into the circulatory system of a healthy person is practically impossible. The pressure in most vessels is excessive in relation to the atmosphere, so the absorption of gases when the vascular wall is damaged is not observed.
The exception is the internal jugular vein, the pressure in which during inspiration is below atmospheric. The situation looks different with dehydrated patients.
Due to a decrease in the bcc, the pressure in the central vessels becomes negative; a violation of the integrity of the vessel wall can lead to the ingress of gases from the environment. Common causes of air occlusion include:
- Traumatization
. Atmospheric gases penetrate into the blood during barotrauma of the lungs (sudden ascent from depth, incorrectly selected ventilator mode), chest injuries, accompanied by rupture of blood vessels. VE is also detected against the background of injuries to other anatomical areas in the absence of timely stoppage of profuse bleeding. - Childbirth
. Penetration of gases becomes possible when the placental venous sinuses rupture. Air is forced into the damaged vessels under pressure during uterine contractions. The disease develops regardless of the value of central venous pressure. Symptoms can occur not only directly during childbirth, but also 1-2 days later. - Medical procedures.
Manipulations with a high risk of developing VE include operations on blood vessels, chest organs, and the brain, if the venous sinus is opened during the intervention. In addition, air can enter the blood supply if there is a loose connection between the infusion system and the central venous catheter or during infusion therapy. This happens with a negative central venous pressure.
Large air bubbles in the bloodstream can lead to occlusion of any vessels. Most often, the pulmonary veins, heart vessels, and arterial trunks that supply the brain are blocked.
When the pulmonary artery is damaged, regional intravascular hypertension, RV overload and acute right ventricular failure are observed. Further, the left ventricle is involved in the process, cardiac output decreases, peripheral circulation is disrupted, and shock develops.
Air embolism of the PA is accompanied by the occurrence of bronchospasm, ventilation-perfusion imbalance, pulmonary infarction and respiratory failure.
When blood flow in the cerebral vessels is disrupted, the formation of pathology occurs as an ischemic stroke. In a certain area of the brain, blood supply is disrupted, neurotissue experiences oxygen starvation and dies.
An area of necrosis forms, and multiple small hemorrhages occur in the brain tissue. The further course of the disease depends on the location of the affected area.
Paresis, paralysis, impaired cognitive functions, and disruptions in the functioning of internal organs may be detected.
There are several criteria for systematizing VE.
Air embolism is classified according to the nature of its course (fulminant, acute and subacute), the path of air penetration into the bloodstream (iatrogenic, traumatic), and the direction of movement of the embolus (orthograde, retrograde, paradoxical). In clinical practice, a division of the forms of the disease according to the type of affected vessel is used, including the following pathology options:
- Arterial
. There is blockage of large arterial trunks (coronary, pulmonary, cerebral). It occurs in 30-35% of cases, develops at lightning speed, is severe, with severe clinical symptoms. The patient dies within a few hours, sometimes minutes. For the formation of AVE, more than 40-50 cm3 of gas is required to simultaneously enter the bloodstream. - Venous
. Detected in 65-70% of cases. Leads to disruption of venous outflow. Symptoms progress relatively slowly, and life-threatening conditions are rarely detected. Prone to subacute course. When small veins and venules are blocked, it can be asymptomatic, while blood flow is ensured by a system of collaterals. An exception is air occlusion of the pulmonary veins, which carry oxygenated blood from the lungs to the heart.
The clinical picture varies depending on the type and size of the affected vessel. When the outflow of blood through large peripheral veins is disrupted, typical signs of thrombosis occur. The affected area swells and increases in size.
When squeezed, severe pain is detected. The skin in the pathology area is cyanotic, and there is local hyperthermia.
The systemic reaction is moderate tachycardia caused by the deposition of a certain volume of fluid and a decrease in blood volume.
Air embolism of small branches of the pulmonary artery causes cough, hemoptysis, episodes of syncope, shortness of breath for more than 20 breaths, tachycardia within 100-120 beats per minute. There are no hemodynamic disturbances.
When large trunks are blocked, a picture of acute cor pulmonale develops. The patient exhibits severe hypotension, swelling of the neck veins, increased liver size, increased central venous pressure, psychomotor agitation, and increased cardiac impulse.
The skin is pale, cold, covered with sticky sweat.
Damage to the coronary arteries leads to acute myocardial infarction. There are typical pains behind the sternum of a compressive nature. The use of nitrates does not give the expected effect.
Blood pressure drops to shock levels. Pulmonary edema of cardiac origin is possible. The typical picture of AMI is not always observed.
In 40% of cases, the disease occurs in an atypical form, manifested by pain in the abdomen, throat, left arm, etc.
Embolization of the brain's blood supply structures causes a stroke. A focus of necrosis forms in the brain tissue, the location of which determines the clinical symptoms.
The most common signs of ischemic stroke include paresis and paralysis, local decrease in muscle tone, paresthesia, speech disorders, blurred vision, dizziness, headache, instability, drop attacks, weakening of skin sensitivity.
During embolization of peripheral arteries, trophic ulcers are formed and zones of necrosis appear. Violation of venous outflow in the extremities leads to edema. Changes in the blood supply system of internal organs cause weakening or complete cessation of their activity.
Acute renal or liver failure, intestinal paresis, and failure of heart and lung function may develop. Damage to cerebral blood structures provokes irreversible disturbances in the functioning of the body.
Paralysis, disturbances in the psychoemotional sphere, and changes in the functioning of internal organs innervated by the damaged area of the brain are observed.
Diagnosis of VE is carried out by an anesthesiologist-resuscitator in tandem with the patient’s direct attending physician. Data from a clinical examination, combined with information obtained from the use of hardware diagnostic techniques, usually leave no doubt about the diagnosis.
Difficulties arise when determining the type of embolism. It is necessary to differentiate between vascular occlusion caused by air, gas bubbles formed endogenously with a sharp change in environmental pressure (caisson disease, gas embolism), thrombus, tumor, foreign body, conglomerate of bacterial cells.
Diagnostic measures include:
- Physical
. They are carried out in the intensive care unit or at the patient’s location. During the examination, indirect signs of thrombosis are identified and a preliminary diagnosis is made. It should be borne in mind that the disease does not always occur with a full set of symptoms; the frequency of occurrence of some of them does not exceed 50-60%. - Laboratory
. At the initial stages of development of VE, laboratory examination is not very informative. Changes in the composition of blood gases, acid-base balance, and electrolyte balance are noted. With damage to internal organs and the development of multiple organ failure, there is an increase in the activity of liver enzymes and an increase in the concentration of creatinine and urea in the blood. Destructive processes in muscle tissue cause an increase in myoglobin levels. - Instrumental
. When performing precordial, transesophageal or transcranial Doppler ultrasound, it is possible to establish the presence of air in the vessels. The study is qualitative; it is impossible to determine the volume of gas using it. The capnogram indicates an increase in the concentration of carbon dioxide at the end of expiration; when measuring CVP, an inadequate increase in indicators is revealed. The ECG reveals ventricular extrasystoles, P wave changes, and ST segment depression.
Elimination of the consequences of air entering the vessels is carried out using medicinal and hardware methods of treatment. The amount of assistance required depends on the patient’s condition, the severity of the impairment of vital functions, and the availability of the necessary equipment in the clinic. Typically, the scheme of restoration measures includes the following methods of influence:
- Nonspecific medications
. Treatment is aimed at minimizing clinical signs of the disease and preventing complications. The patient is prescribed steroid hormones, cardiotonics, loop diuretics, vasodilators, and antioxidants. At the recovery stage, multivitamin complexes and nootropic drugs are used. In case of severe respiratory failure, the patient is transferred to mechanical ventilation in the forced ventilation mode. - Hardware
. Air embolism is treated with hyperbaric oxygen therapy and controlled hypothermia. HBOT is carried out under a pressure of 2-3 atmospheres, the number of sessions varies from 5 to 12. The duration of each of them is 45 minutes. When using hypothermia, the patient's body is cooled to 34°C. Both barotherapy and cold help increase the solubility of gases in the blood, which makes it possible to destroy a blood clot that cannot be removed surgically. - Operational
. The optimal method for removing an embolus during intracardiac VE is its aspiration through a subclavian catheter. This removes several hundred milliliters of blood, which may require massive infusion therapy or blood transfusion. By accurately determining the location of the embolus, it is possible to open the vessel or venous sinus.
The outcome is favorable in cases where the air can be removed using a low-traumatic subclavian approach. If the embolus is intracranial or pulmonary, the prognosis worsens, since it is almost impossible to remove it surgically.
The use of HBOT and hypothermia does not quickly normalize blood flow, therefore, the likelihood of irreversible consequences increases.
When peripheral veins and arteries are damaged, there is usually no threat to life, but the restoration of the affected tissues takes a long time, and complete regeneration is not always achieved.
//www.youtube.com/watch?v=aKsp-LaWk28
Air embolization most often occurs during medical procedures, so measures to prevent it fall entirely on the staff of the medical institution.
When performing interventions on the superior vena cava, the patient should be in the Trandelenburg position; catheterization of the subclavian vein at the moment when the needle remains with an open end (disconnecting the syringe, removing the guidewire) is carried out while the patient exhales deeply.
When the central venous pressure is low, exhausted infusion systems should be shut off in a timely manner.
Source: //www.KrasotaiMedicina.ru/diseases/urgent/air-embolism
How it develops
The appearance of this pathology requires the presence of such factors.
- Systemic vascular obstruction occurs from direct release of bone marrow into the venous system due to fracture.
- Increased intramedullary pressure after injury leads to fat release through patent venous sinusoids.
- Embolized fat clogs the lumens of the capillary network.
Biochemical theory provides an alternative explanation for this process. She suggests that the inflammatory response to injury causes the release of free fatty acids from the bone marrow into the venous system.
Increased concentrations of free fatty acids, as well as inflammatory mediators, cause capillary damage. Such changes cause damage to the brain or lungs.
Regardless of the mechanism that initiates the disease, the end result is an intense inflammatory response. The capillary network becomes more permeable, and inflammatory mediators damage surrounding tissues.
Classification
Doctors classify pathology according to its location.
With pulmonary fat embolism, symptoms usually develop 24 to 72 hours after injury or surgery. Patients often complain of vague chest pain and shortness of breath.
Tachypnea and fever associated with disproportionate tachycardia are common. The syndrome can rapidly progress to severe hypoxemia, which requires mechanical ventilation.
Neurological manifestations include drowsiness, confusion, decreased level of consciousness and seizures. Patients may have petechiae, especially affecting the conjunctiva, oral mucosa, and upper body.
If more than 2/3 of the pulmonary capillaries are blocked, acute pulmonary failure and cardiac arrest will occur.
The cerebral form in the form of a stroke usually occurs a few days after the injury. The clinical features of cerebral embolization depend on the affected areas of the brain. Diffuse embolization may cause encephalopathy or seizures, but more discrete lesions may cause focal neurological deficits.
Peripheral signs that indicate the diagnosis include petechial obstruction visible on ophthalmoscopic examination. Laboratory studies confirm hypoxemia, anemia, lipuria, and bleeding disorders.
The renal form is rare. Typically there is a triad of symptoms:
- oliguria;
- hematuria;
- anuria.
Drowsiness with oliguria is almost pathognomonic.
Symptoms
Sharp pain at the injection site is a possible sign of embolism
The painful manifestations of oil embolism directly depend on which blood vessel the substance initially entered. In cases where an artery is blocked, the following most often occurs:
- Sharp pain localized near the injection site is one of the first signs of pathology;
- Change in skin color - due to blockage of the lumen of the artery, blood does not flow in sufficient quantities, the skin turns pale, while nearby areas sometimes turn red;
- Rapid onset of swelling;
- Changes in the temperature of the affected areas and surrounding tissues - characterized by both cold temperatures due to lack of blood supply and a reflex increase in temperature due to inflammation (occurs later);
- The appearance of signs of tissue death - a change in color to bluish or dark, the addition of an infection;
- Increased body temperature, accompanied by chills;
- Signs of intoxication - nausea, vomiting.
Oil embolism does not go away without a trace
When an oil solution enters the venous network, disturbances in the functioning of the lungs are observed:
- Involuntary increased breathing;
- Feeling of lack of air, suffocation;
- Severe anxiety followed by apathy;
- Depression of consciousness up to fainting;
- Pain in the chest area;
- The appearance of a cough;
- Wheezing audible at a distance;
- Fall in blood pressure.
The appearance of symptoms can occur either immediately after an intramuscular injection (surgery, injury) or after 1-2 days. The greatest difficulty is caused by late-onset symptoms, since they are difficult to associate with previous medical manipulation. In trauma and in the postoperative period, symptoms of oil embolism may be mistaken for the usual consequences of these events.
Manifestations
The appearance of the first signs of the disease varies from 12 to 72 hours after injury. Symptoms appear depending on where the blockage occurs.
The most problematic circulatory problems due to blocked blood vessels occur in the brain, lungs or skin. This is fatal in approximately 10-20% of cases.
Symptoms can appear in different parts of the body, making the disease difficult to diagnose. Typically, 2 of the 3 major symptoms or 1 major symptom and at least 4 minor indicators must be present.
The main signs of a fat embolism include:
- lung damage;
- cerebral (brain) disorders;
- petechial rash (red spots on the skin that do not turn white when pressed).
Minor signs include:
- rapid breathing;
- jaundice;
- fever;
- low oxygen content in the blood;
- kidney problems.
It is very important for the patient to be attentive to changes in his condition. This will help to suspect and carry out diagnostics in time to identify fat vascular embolism.
Possible consequences and complications
Acute massive pulmonary embolism can cause sudden death. In cases where compensatory mechanisms have time to work, the patient does not die immediately, but secondary hemodynamic disorders quickly increase in him, which, in the absence of timely treatment, lead to death. Possible consequences of a pulmonary embolism may include:
- acute cor pulmonale;
- pneumonia;
- pleurisy;
- lung abscess;
- gangrene of the lung.
Possible complications
The development of possible complications is influenced by the speed of provision of qualified medical care and the accuracy of the diagnosis. If these conditions are met, the disease can be treated successfully.
In elderly and weakened people and in cases of fulminant development, the prognosis worsens. Coma and death may develop, observed in 10-20% of cases.
Prevention measures
The main preventive measure is the correct determination of the area for injection under the skin or into the muscles. In addition, you must follow the instructions for the medications. Do not inject oil products into venous vessels.
Drugs are administered into:
- The outer part of the shoulder.
- The lower part of the axillary region.
- The lateral part of the abdominal wall.
- Hips in anterior-outer position.
- Under the shoulder blade.
In these areas, a skin fold is grabbed, then an injection is given. It is worth injecting inside the muscle in the area of the buttocks or the front surface of the thigh.
You should not inject yourself, this will interfere with the injection process. Refer to qualified healthcare professionals or people with extensive knowledge of injections.
Diagnostics
Embolized fat droplets can travel in the bloodstream throughout the body. Thus, the syndrome is a multi-organ disease and can damage any microcirculatory system in the body.
In the absence of specific tests or criteria, the diagnosis of fatty vascular disease depends on the attending physician. This pathology should be suspected in patients with respiratory failure or petechial rash and with injuries to long bones.
Who's at risk
The risk group includes the elderly, those who work in conditions with increased trauma, the weakened, and those who have undergone surgery on tubular bones or liposuction.
Given the increase in road traffic accidents, where victims receive injuries of varying severity, the prevention of fat embolism syndrome is of particular relevance.
Such measures include the timely provision of qualified medical care, including early treatment of fractures and complex anti-shock and drug therapy.
The material was prepared specifically for the website venaprof.ru, edited by doctor N.A. Glushakova. Specialty: therapy, cardiology, family medicine.
Source: venaprof.ru
When do paradoxical embolisms in cerebral vessels occur?
Emboli, called paradoxical, are relatively rare. They arise as a result of the introduction of thrombus particles from the veins of the systemic circulation, usually from the veins of the lower extremities, less often from the cavities of the right heart through a vicious communication between the right and left hearts in the arteries of the systemic circulation. They may linger in the vessels of the brain, kidneys or other organs. In almost all the described cases, a vicious communication between the atria was observed. When opening in such cases, a simple non-closure of the oval foramen is sometimes discovered, i.e., a condition in which the edge of a normally developed valve covering the oval foramen does not fuse along its entire length with the final septum. The condition for the occurrence of paradoxical embolism is an increase in pressure in the right atrium above the pressure in the left atrium and anatomically sufficient patency of the foramen ovale. The most common cause of a sudden increase in pressure in the right atrium, in all likelihood, is pulmonary embolism, which usually precedes the introduction of the embolus into the systemic circulation.
Paradoxical embolism is observed more often with a wide open foramen ovale or with a true atrial septal defect than with simple patent foramen ovale. With a wide open foramen ovale and a true atrial septal defect, more favorable conditions are created for the occurrence of paradoxical embolism, since the vicious communication is larger and the blood of both atria can mix freely in both directions. In such cases, there is an incalculable number of chances of the embolus being introduced through a vicious communication, and not through the pulmonary artery with a blood flow of normal circulation. A ventricular septal defect can result from an embolus from the right heart entering the aorta, such as in tetralogy of Fallot. Paradoxical emboli can cause mycotic abscesses in patients with congenital heart disease. Small emboli brought from non-limited foci of infection and normally retained in the lungs without causing symptoms can cause a brain abscess if there is a right-to-left shunt, even if it is only temporary. This complication is probably rare. Previously, the possibility of paradoxical introduction of fat particles, air, or tumor tissue particles into the systemic circulation was often discussed, but in most observations described in the literature, the evidence is not convincing. Much attention has been paid to the issue of the occurrence of brain abscess in patients with congenital heart disease. The mechanism of occurrence of an abscess without the presence of bacterial endocarditis has not yet been studied in detail. Most authors are of the opinion that the dispersion of pyogenic bacteria, which results in a brain abscess, usually occurs from the systemic circulation through paradoxical embolism (paradoxical brain abscess). However, the source of infection can also be the area of the pulmonary circulation, for example, bronchiectasis or tuberculous cavity. However, the source of infection often remains undetected. The occurrence of brain abscess was also observed in arteriovenous pulmonary malformations. The literature provides statistics that brain abscess in men suffering from congenital heart disease is more common than in women, approximately 1.2:1. The difference in this case is not as significant as with brain abscesses in patients who do not suffer from congenital heart defects. Brain abscesses occur in patients with congenital heart disease usually before the age of 20 years. However, during the first two years of life they occur only in rare cases. In some cases, a brain abscess is preceded by an acute infection, most often of the respiratory system. Occasionally, the occurrence of an abscess has been observed after extraction of carious teeth, after removal of tonsils, or after surgery of the appendix. The pathogenic factor is most often pyogenic streptococci. Other bacteria include Haemophilus influenzae, pyogenic staphylococcus, Escherichia coli, Diplococcus lanceolatus. A mixed infection is found relatively often. It is not uncommon for cultures to give negative results. As already noted, brain abscesses are most often observed with cardiac malformations with a venous-arterial shunt. Bacteria that periodically enter the blood from some source of infection can be carried through the venous blood flow through a vicious communication into the systemic circulation and thus avoid retention in the pulmonary capillaries. Still, the question is controversial whether the presence of microorganisms alone is sufficient for the occurrence of an abscess in the brain tissue without the participation of trauma, local ischemia and concomitant necrosis due to blockage of a vessel by an infected embolus. Using experiments on animals, it was proven that the entry of bacteria into normal brain tissue leads to the formation of an abscess only after preliminary damage to the brain tissue. In patients with congenital heart disease and brain abscess without bacterial endocarditis, polycythemia, increased blood viscosity, slow blood flow, and, consequently, an increased tendency to thrombus formation in the vessels are almost always observed. Blockage of the cerebral vessels or sinuses is, in all likelihood, no less important a factor in the occurrence of an abscess than the presence of the bacteria themselves. With some congenital heart defects, it is likely that small septic emboli may enter the systemic circulation, causing damage to brain tissue as a result of blockage of blood vessels with the subsequent development of an abscess. The almost exclusive localization of the abscess in the brain indicates that brain tissue usually has less resistance to bacterial invasion than other tissues. Paradoxical brain abscesses in patients with congenital heart disease are, in all likelihood, much more common than reported in the literature (3-5%). This complication should be kept in mind in all cases when a patient suffering from a congenital heart defect with the presence of a shunt develops a persistent headache with elevated or normal body temperature, vomiting, drowsiness, or with severe objective signs of damage to brain tissue and swelling of the optic nerve nipple . However, not in all cases there is a mandatory cardiac malformation with the presence of a persistent exclusive or predominant venous-arterial shunt. It is also sufficient to temporarily invert the exclusive or predominant arteriovenous shunt into a venous-arterial one, as, for example, during physical activity. Brain abscesses that occur in patients with congenital heart defects are characterized by a rapid, dramatic course with a slight tendency to form a limiting bursa and a high tendency to early breakthrough into the ventricles of the brain. In some cases, the development of an abscess becomes chronic and may have an intermittent course. In most cases, the formation of a solitary abscess is observed. There are also descriptions of the formation of numerous abscesses in the literature. The results of surgical treatment of abscesses have improved significantly with the use of modern antibiotics and the technique of radical removal of all affected tissue, even before the formation of a bursa. Thanks to the use of antibiotics for any infection that occurs in patients with congenital heart disease, it is usually possible to prevent the formation of a brain abscess. In itself, surgical treatment of congenital heart defects associated with venous-arterial shunt and persistent cyanosis is important for the prevention of brain abscesses, provided that polycythemia disappears after surgery. Among other complications, it is necessary to point out aortic rupture with coarctation of the aorta and with a bicuspid aortic valve. In the past, much attention has been paid to the supposed increased susceptibility to tuberculosis in pure pulmonary stenosis or in combination with the triad or tetralogy of Fallot. The latest large statistical reviews indicate that tuberculosis with pulmonary artery stenosis does not occur as often as previously stated, but in approximately only 2% of patients suffering from this malformation.
Source: alfa-med.su
Course and prognosis
- Depends on the underlying disease, which is complicated by septic thromboembolism
- 40% of patients develop pleural empyema.
Septic embolism in a 25-year-old man suffering from drug addiction.
a Plain chest radiograph taken at the bedside of a patient with a clinical picture of sepsis. Bilateral infiltrative changes in the basal sections, a weak “air bronchogram” on the right, as well as small foci of infiltration with signs of cavitation, more pronounced in the right lung, are visible.
b CT scan confirmed the presence of multiple septic emboli and extensive infiltration of the lungs, especially in the posterobasal regions, more pronounced in the right lung. A small accumulation of fluid in both pleural cavities