Degrees and stages of blood transfusion shock
This type of shock has several degrees of severity. The course of the process depends on the patient’s well-being before the transfusion procedure and the volume of blood infused.
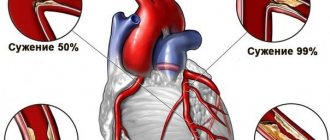
The severity of the pathology is judged by the level of systolic blood pressure:
- First degree - the pressure level is above 90 mm Hg. The first symptoms appear.
- Second degree - systolic pressure drops to 70 - 90 mmHg.
- Third degree - pressure drops below 70 mm Hg.
Most often, transfusion shock is of the first degree. A qualified nurse will notice the deterioration of the patient’s condition in time and prevent the deterioration of his condition.
The clinical course of this pathology has its own periods.
Destruction of red blood cells if the rules are not followed
Classic shock occurs with a sequential change, however, a severe form of transfusion shock occurs so quickly that even an experienced specialist is not always able to determine in which period the patient is.
The following periodization of blood transfusion shock is accepted:
- The period of blood transfusion shock - it is characterized by disseminated intravascular coagulation syndrome, disordered coagulation and destruction of blood elements, as well as a decrease in blood pressure.
- The period of renal disorders - as a result of shock, acute renal failure develops, oliguria or anuria occurs - a sharp decrease in the amount of urine excreted or its complete absence.
- Restoration of renal function - with timely therapy, kidney function is resumed, and the processes of filtration and urine formation are activated again.
- The rehabilitation period is a gradual return to normal of all indicators of the circulatory system: the formation of new red blood cells, replenishment of the lack of hemoglobin, restoration of normal bilirubin levels.
Symptoms of pathology
Symptoms of shock can be either pronounced or confused. The approximate time for the first signs of incompatibility to appear is up to 2 hours from the moment of transfusion.
The most obvious symptoms are:
- periodic agitated state of the patient;
- breathing disorders - heaviness, intermittency, shortness of breath;
- blue tint of skin and mucous membranes;
- chills;
- pain in the back (lower back).
The transfusiologist asks the patient about back pain from the moment the blood transfusion begins until completion. Impaired kidney function is the first sign of the development of transfusion shock.
The development of pathology depends on the patient’s condition before the procedure and the immune system. Changes can begin rapidly with a sharp drop in blood pressure and kidney damage, which requires emergency treatment for transfusion shock.
In other cases, the condition worsens gradually, giving a vague clinical picture.
Etiology of the condition
This pathology is a complication of transfusion, which occurs due to a violation of its technology.
Most often the cause is:
- Errors in determining blood group,
- Violations during medical manipulations with collected blood,
- Errors in determining the compatibility of the blood of the donor and the recipient (the person to whom the blood or its components are infused).
Hemotransfusion shock occurs with incompatibility of the ABO or Rh factor systems. For example, an error in determining the latter can lead to the infusion of Rh-positive blood into a patient who is Rh-negative. This is guaranteed to lead to shock.
Usually, only Rh and blood group according to the A0 system are determined. There are other systems that take into account the compatibility of dozens of antigens (special components on the surface of red blood cells), but they are determined very rarely.
This is due to the fact that in most cases the conflict of these antigens does not have any consequences.
Indications and contraindications for blood transfusion
There are several categories of people who need transfusions. Refusing blood transfusion to people without indications or with contraindications to it is already a prevention of shock.
Indications for transfusion are:
- Massive blood loss during surgery or injury.
- Diseases of the circulatory system (leukemia, etc.)
- Various types of anemia (sometimes transfusion is part of therapeutic measures).
- Severe intoxication leading to the destruction of blood cells.
- Systemic purulent-inflammatory diseases.
Blood leukemia
Contraindications to transfusion are as follows:
- Heart failure during decompensation (irreversible impairment of heart function).
- Septic endocarditis is inflammation of the inner lining of the heart wall.
- Pathologies of cerebral circulation.
- Allergies.
- State of liver failure.
- Glomerulonephritis (kidney disease, with characteristic damage to the glomeruli).
- Tumor neoplasms in the stage of decay.
You can help your doctor by telling him about any allergic reactions you have and your experience with previous blood transfusions. Women should also talk about the difficult course of childbirth and the presence of hereditary blood pathologies in children.
How is a blood transfusion performed?
Blood transfusion is carried out only as prescribed by a doctor, who takes into account the clinical picture of your disease. The procedure itself is carried out by a nurse.
Before performing a transfusion, the doctor checks the blood group and Rh factor, and the correctness of the biological compatibility tests. Only after the doctor is convinced of the safety of the procedure does he give permission to carry out it.
Immediately before the transfusion, the patient is injected with 15 ml of blood three times (with a 3-minute break). The nurse observes the patient’s reaction to each administered portion, monitors the heart rate, blood pressure level, and asks the patient about his well-being.
If the test passed without complications, a full transfusion begins. The entire transfusion process will be documented in the medical record.
The blood container and the test tube with the patient’s blood are stored for two days. In case of complications, they will determine the presence of violations of the procedure on the part of medical personnel.
Monitoring of the condition after blood transfusion is carried out over the next day. Blood pressure, body temperature, and pulse rate are taken every hour. The next day, a control blood and urine test is performed.
A doctor's view of the problem
As complications develop, the pressure drops significantly and the outflow of urine becomes difficult. There are problems with the functioning of the kidneys. If you experience any of the symptoms of shock, it is important to see a doctor immediately. Thanks to timely treatment, you can protect yourself from complications. The patient is treated in a hospital setting under the strict supervision of doctors. Over time, general health is restored. The main causes of citrate shock are negligence in blood storage and improper procedure.
What happens during transfusion shock?
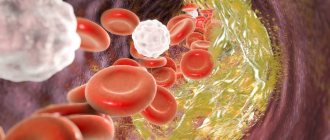
The pathogenesis of this condition is due to the adhesion of blood cells, which occurs due to the incompatibility of the groups or Rhesus of the donor and recipient. Red blood cells gather into large clots, their shell dissolves, and the hemoglobin contained inside comes out, circulating freely in the bloodstream.
The observed reaction is called cytotoxic and is one of the types of allergies.
Hemolytic breakdown of red blood cells in the vascular bed causes many pathological changes. Blood can no longer fully perform its main function - transporting oxygen to the tissues of the body.
This causes oxygen starvation, which only worsens over time and leads to disorders in the central nervous system and other tissues.
Hemolytic breakdown of red blood cells
In response to foreign substances, a reflex vascular spasm occurs. After a short period of time, paresis (paralysis) occurs in them, leading to uncontrolled expansion.
The dilated peripheral vessels take away most of the blood, causing a drop in central blood pressure. Blood cannot return to the heart due to problems with paralyzed intravascular muscles.
The release of hemoglobin from cells leads to changes in blood pressure. As a result, plasma begins to penetrate the walls of blood vessels in large quantities, increasing the viscosity of the blood.
Due to thickening and imbalance of the coagulation and anticoagulation systems, disordered blood clotting (DIC syndrome) begins. It becomes very difficult for the heart to pump the clotted blood.
Metabolic acidosis begins to increase in tissues - an increase in acidity that occurs due to adenosine phosphoric acid entering the blood.
This leads to disturbances in the nervous system (loss of consciousness, stupor).
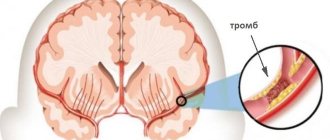
Free hemoglobin begins to disintegrate, turning into hydrochloric acid hematin. This substance, entering the kidneys, leads to blockage of the renal filter. Acute renal failure occurs.
Filtration stops, and more and more oxidizing substances accumulate in the body. This worsens acidosis, which kills nerve cells and affects all tissues in the body.
Poor circulation, worsening hypoxia and acidosis gradually lead to the death of the body. If a patient in shock does not receive emergency care, he will die.
What changes occur in the body?
This condition is characterized by the destruction of donor red blood cells in blood vessels under the influence of antibodies, the release of hemoglobin, biogenic amines, potassium, and tissue thromboplastin. Due to the influence of high concentrations of these substances, the following occurs:
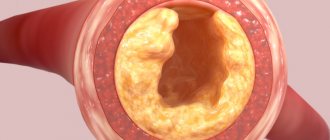
- strong spasm of blood vessels, their rapid transition from narrowing to expansion occurs. As a consequence of this, hypoxia occurs, blood microcirculation is impaired, its viscosity increases, and the permeability of the vascular walls increases.
- Reduced oxygen content and the presence of acidic metabolites lead to disruption of the body systems and their morphological changes. Blood pH decreases.
- The breakdown of hemoglobin has a devastating effect on kidney function. As a result of deposition of hematin hydrochloride in the kidney tubules, as well as spasm and the occurrence of vascular obstruction, acute renal failure develops. This leads to a gradual cessation of the filtering function of the organ, an increase in the level of creatinine and nitrogenous substances in the blood.
Hemotransfusion shock is characterized by the presence of thrombohemorrhagic syndrome. This disorder is provoked by thromboplastins, which penetrate into the blood due to the destruction of red blood cells and activate its coagulation.
With thrombohemorrhagic syndrome, blood clots form in small vessels, causing damage to all organs and systems, especially the lungs, liver, and endocrine glands.
Symptoms
Usually the body reacts quickly to the infusion of incompatible blood. The first signs of transfusion shock begin to appear already at the initial stages of the procedure. However, there are cases when symptoms do not make themselves felt immediately.
That is why during each post-transfusion period the recipient is under the supervision of doctors for 24 hours.
Early symptoms of incompatible blood transfusion:
- Patient agitation. Due to the reflex release of adrenaline, he experiences anxiety and excessive activity.
- Breathing problems. Shortness of breath appears, the patient experiences a lack of air.
- Total cyanosis - change in color of the skin and mucous membranes to pale blue.
- Trembling, feeling of decreased body temperature.
- Pain in the lumbar region (is the main sign of damage to the kidney tissue).
Gradually, signs of shock become more and more obvious due to the increasing phenomena of tissue hypoxia. The heart tries to compensate for the lack of blood circulation by speeding up its rhythm. Tachycardia appears.
The patient's skin gradually becomes more and more pale and bluish, and cold perspiration appears on it. Blood pressure levels constantly drop due to pathological relaxation of peripheral vessels.
Much less often with blood transfusion shock, vomiting and an increase in the patient’s body temperature are observed.
Sometimes there are limb cramps caused by the influence of acidosis (increased acidity of the body) on the nervous tissue.
Emergency care not provided on time causes the development of hemolytic jaundice - yellow discoloration of the skin due to the breakdown of red blood cells, as well as acute renal failure. The latter is a dangerous condition leading to the death of the patient.
If blood transfusion is performed under anesthesia, shock is determined by the following signs:
- A sharp drop in blood pressure.
- Increased bleeding.
- Urine entering the urinal, the color ranges from pink to deep red. This occurs due to a malfunction in the kidney filter, which allows parts of the destroyed red blood cells to pass through.
Clinical picture and symptoms of hemolytic shock
The clinical picture of transfusion shock covers the following signs that appear at the onset of this condition:
- increasing anxiety;
- the occurrence of short-term excitement;
- pain syndrome localized in the thoracic and lumbar region, as well as in the abdomen;
- the patient feels chills and cold;
- rapid and difficult breathing;
- blue discoloration of the skin and mucous membranes.
Pain in the lower back is called a “marker” symptom or pathognostic manifestation characteristic of hemolytic shock. In this condition, circulatory disorders occur, characterized by:
- arterial hypotension;
- the appearance of sticky cold sweat;
- cardiac arrhythmia with signs of acute heart failure;
- rapid heartbeat accompanied by pain.
The state of transfusion shock is characterized by sustained hemolysis due to the breakdown of red blood cells. The acquisition of a brown color in urine and a high protein content (according to tests) is also a characteristic symptom. There is also a violation of the blood clotting process, the clinical manifestation of this symptom is manifested in profuse bleeding.
Rare symptoms are:
- increased body temperature;
- redness or, conversely, paleness of the skin on the face;
- nausea and vomiting;
- marbling of the skin;
- the appearance of seizures;
- fecal and urinary incontinence.
Symptoms during a procedure performed under anesthesia may not appear at all or may be mild. Careful observation by doctors of the blood transfusion procedure and emergency care when such a complication occurs is the key to its successful elimination.
Algorithm of actions for blood transfusion shock
The nurse’s actions at the first manifestations of transfusion shock should be as follows:
- Immediately stop the transfusion. Disconnecting the dropper. The needle remains in the vein for subsequent manipulations.
- An emergency infusion of saline solution begins. The dropper with it is connected to the same needle, since after removing it there is a risk of spending a lot of time inserting a new one.
- The patient is given humidified oxygen through a special mask.
- In an emergency, a laboratory worker is called to perform a rapid blood test, determining the level of hemoglobin, the number of red blood cells, and hematocrit indicators (the ratio of the liquid and cellular parts of the blood).
- A urinary catheter is inserted to monitor urine output. A urine test is sent to the laboratory.
If possible, the patient's central venous pressure is measured, electrocardiography is performed, and the acid-base balance is determined. Hemoglobin in plasma can be quickly detected using the Baxter test.
It is carried out 10 minutes after the start of the transfusion. 10 ml of blood is taken from the patient, the tube is closed and placed in a centrifuge. If, after shaking, the separated plasma is pink in color, destruction of red blood cells can be suspected.
Diagnostics
Instrumental and laboratory tests must be carried out:
- Phlebotonometry - using a phlebotonometer, the pressure exerted by venous blood in the right atrium is measured.
- Colorimetry - determine the content of free hemoglobin in plasma by the color intensity of the solution.
- Goryaev's method of counting - blood is placed in a chamber of a certain volume and the number of red blood cells and platelets is counted using a microscope, after which they are recalculated per 1 microliter.
- Rutberg's gravimetric method - fibrin formed after plasma coagulation is dried and weighed to determine the concentration of fibrinogen in the blood.
- Blood centrifugation - after a strictly defined number of revolutions of the centrifuge, the hematocrit is calculated using a special scale - the ratio of blood cells to plasma.
- Determination of diuresis - calculate the amount of urine that is produced over a certain time period.
If necessary, measure the acid-base state of the blood and the content of gases in it, and make an electrocardiogram.
Treatment
The treatment regimen for transfusion shock depends on the amount of diuresis (the volume of urine produced over a certain period of time).
If more than 30 ml of urine collects in the urinal in an hour, the patient is administered the following within 6 hours:
- Soda solution to restore normal acid balance,
- Reopoliglucin is an anti-shock plasma substitute with 10% glucose content,
- Mannitol is a diuretic.
- Lasix is a diuretic to remove excess fluid.
In just 4-6 hours of infusion therapy, the patient is given up to 6 liters of fluid. However, this volume is only suitable for patients with normal renal function.
In case of acute renal failure (no more than 30 ml of urine is excreted per hour), fluid is administered according to the following formula: 600 ml + volume of diuresis during infusion therapy.
If the patient has pain, it is relieved first. In such cases, the use of narcotic analgesics like Promedol is indicated.
Patients are also prescribed:
- Heparin to thin the blood and normalize clotting.
- Agents that regulate the permeability of vascular walls: ascorbic acid, Prednisolone, sodium ethamsylate, etc.
- Antiallergic drugs (Suprastin).
- Drugs that suppress proteases (enzymes that break down proteins) - Contrikal.
An effective method of eliminating transfusion shock is plasmapheresis - purification of the victim’s blood with special filters, after which it is reintroduced into the vascular bed.
Plasmapheresis
Treatment recommendations
Transfusion shock is a condition that requires emergency care. The algorithm of actions in this situation can be presented as follows:
- Removing the patient from a state of shock.
- Measures to prevent pathological changes in important organs and correct them.
- Relief of developing DIC syndrome.
- Prevention of development of acute renal failure.
If adverse symptoms appear, the first action of the nurse or doctor is to stop the transfusion procedure and replace the system with saline solutions.
It is strictly forbidden to remove the needle from the vessel, since a drop in pressure may make it impossible to perform repeated venipuncture.
The most important factor is time: the faster medical interventions are performed, the better the prognosis for the patient.
Infusion therapy
All shock treatment regimens begin with infusions.
First of all, it is necessary to replenish the circulating blood volume (CBV) and restore hemostatic function (dextrans with a molecular weight of 40–70 thousand units are used - rheopolyglucin, gelatinol).
Early infusion of a 4% solution of sodium bicarbonate or lactosol is also indicated. In this way, compensation for metabolic acidification of the blood is ensured, and the synthesis of hematin hydrochloride does not occur.
Subsequently, a crystalloid infusion is performed (with a solution of 0.9% sodium chloride or Ringer's solution) to reduce the amount of free Hb and prevent the destruction of fibrinogen. The amount of infused drugs must be controlled by the volume of diuresis and pressure values.
Drug therapy
It is necessary to raise the patient's blood pressure, as well as ensure normal renal blood flow. A triad of standard antishock drugs: prednisolone (a glucocorticosteroid to increase blood pressure), furosemide (a diuretic) and aminophylline (a phosphodiesterase inhibitor). Antihistamines and opioid painkillers (fentanyl) are also used.
Efferent methods
An effective method of anti-shock therapy is plasmapheresis - removal of about 2 liters of plasma followed by infusion of fresh frozen plasma and colloid solutions. Symptomatic correction of disorders of the internal organs.
If necessary, medications are prescribed that stimulate the activity of important body systems. If symptoms characteristic of a decrease in the respiratory function of the lungs appear, the patient may be transferred to a ventilator. In case of severe anemia (hemoglobin concentration less than 70 g/l), it is possible to transfuse washed red blood cells compatible in blood group with the patient's red blood cells.
Correction of the hemostatic system
Anticoagulants are used, transfusions of fresh frozen plasma and antienzyme drugs (Gordox) are performed to inhibit fibrinolysis.
Since the development of acute renal failure is possible in the future, treatment of transfusion shock is also aimed at correcting the functional state of the kidneys. Furosemide and mannitol are used and correction is performed with crystalloid solutions.
If there is no effect, hemodialysis may be applicable . During the recovery period, specific symptoms are treated.
Life forecast
Most often, transfusion shock is determined quickly. If first aid and treatment measures are carried out within 6 hours after a failed transfusion, then approximately 2/3 of people make a full recovery.
Associated complications are observed in the case of massive transfusion of incompatible blood. It is worth noting that this is rare.
However, if doctors and nurses are incompetent, violation of blood transfusion technique leads to renal-liver failure and thrombosis of the blood vessels of the brain and lungs. After treatment, patients with such pathologies suffer from chronic diseases throughout their lives.