Development mechanism
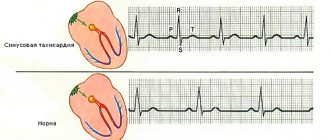
Normally, the impulse generator that controls the contraction of the heart is the sinus node. While it is functioning normally, backup sources of impulse are suppressed.
An extrasystole indicates that such a (secondary) source of impulse has intensified its activity.
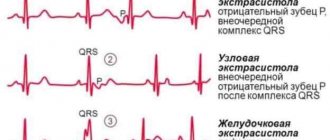
It is in the intraventricular system (Purkinje fibers, trunk of the His bundle, its branches or legs) that extraordinary impulses arise, causing the ventricles to contract without prior contraction of the atria. This can be seen on the electrocardiogram: there is no full-fledged P wave, indicating the functioning of the atria.
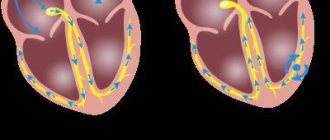
Experts have given a name to this phenomenon – the reentry mechanism. This means that the impulse conducting the excitation passes along a closed path and repeats its action. This mechanism, according to scientists, often causes various forms of arrhythmias.
During an extraordinary contraction, the ventricles do not pump blood, and the transient function does not occur. This is a fruitless waste of the strength of the heart, which at that moment should have been “resting”, but as a result – “working for wear and tear”.
There are relative norms for the number of extrasystoles outside sinus rhythm occurring during the day:
- 600-950 - are considered a non-life-threatening condition if there are no other abnormalities in the heart and disturbing symptoms (tachycardia, causeless shortness of breath).
- 1000-1200 are polymorphic extrasystoles. They are accompanied by a noticeable failure of the heart, which is not only displayed on the ECG, but also felt by the patient himself.
- 1200 or more extraordinary contractions of the ventricles per day are a direct threat to human life and health.
In healthy people, up to one hundred rare extraordinary extrasystoles can occur during the day, which do not in any way affect the overall functioning of the heart or the person’s well-being. In a child, PVCs and other heart rhythm disturbances (abbreviated as HRS) are often observed during puberty.
conclusions
Ventricular extrasystole is a common heart disease in which myocardial automatism is disrupted. If individual extraordinary contractions are functional in nature and can be present in healthy people, an increase in frequency and the appearance of several foci indicates an organic type of lesion.
For the purposes of differential diagnosis, prognosis and choice of treatment, a simple and effective Lown classification was proposed, which has been successfully used since 1975 to this day.
Causes of extrasystole
The general list of causes of ventricular extrasystole can be divided into 2 groups:
- functional disorders - contractions of the ventricles that arose under the influence of short-term physiological factors;
- organic disorders - intercalary extrasystoles, provoked by pathological changes (diseases of the heart and blood vessels).
Neurogenic factors
They are also called idiopathic (non-cardiac) causes of extrasystoles.
These include:
- smoking;
- alcohol consumption;
- passion for strong coffee (increased tone of the sympathetic nerve);
- frequent stay in a state of stress, depressive tendencies;
- insomnia, overeating or mental work (irritation of the vagus nerve occurs;
- great physical activity.
Neurogenic factors provoke increased activity of the sympathetic-adrenal system. As a result, extraordinary contractions of the ventricles of the heart occur.
Heart diseases
A number of pathologies of the cardiovascular system can be a direct trigger for ventricular extrasystoles:
- Coronary heart disease (CHD).
- Myocardial infarction, post-infarction cardiosclerosis.
- Arterial hypertension.
- Atrial tachycardia.
- Inflammatory pathologies (endocarditis, myocarditis).
- Heart defects in the stage of decompensation.
- Cardiomyopathies.
- Supraventricular extrasystole.
- Heart failure (chronic and acute).
- Mitral valve prolapse.
- The presence and activation of excess electrical impulse-conducting beams (James or Kent beam).
Pathological conditions also include ventricular extrasystoles caused by an overdose of cardiac glycosides.
Other diseases
Among other pathologies of a non-cardiological nature, experts note:
- Thyroid gland dysfunction. This is excessive or low production of necessary hormones.
- Vegetovascular dystonia (VSD), neurocirculatory dystonia, vagotonia.
- Pulmonary diseases (PVS are provoked by many drugs used in treatment - Eufillin, Berodual, Salbutamol and others).
- Cervical osteochondrosis of the spine.
- Diseases for which diuretics, antidepressants, and ß-agonists are used.
Reasons for development
Irregularities and heart diseases are the main reasons why PVCs develop. Also, ventricular arrhythmia can be triggered by heavy physical work, chronic stress and other negative effects on the body.
From cardiac pathologies:
| Heart failure | Negative changes in the muscle tissue of the heart muscle, leading to disruption of the inflow and outflow of blood. This is fraught with insufficient blood supply to organs and tissues, which subsequently causes oxygen starvation, acidosis and other metabolic changes. |
| Coronary heart disease (CHD) | This is damage to the heart muscle due to impaired coronary circulation. IHD can be acute (myocardial infarction) or chronic (with periodic attacks of angina). |
| Cardiomyopathy | Primary myocardial damage, leading to heart failure, atypical beats and heart enlargement. |
| Heart disease | Defect in the structure of the heart and/or major outflow vessels. Heart disease can be congenital or acquired. |
| Myocarditis | An inflammatory process in the heart muscle that disrupts impulse conduction, excitability and contractility of the myocardium. |
Taking certain medications (incorrect dosage, self-medication) can also affect the functioning of the heart:
| Diuretics | Medicines in this group increase the rate of urine production and excretion. This can provoke excessive excretion of the “heart” element - potassium, which is involved in the formation of the impulse. |
| Cardiac glycosides | The drugs are widely used in cardiology (they lead to a decrease in heart rate and an increase in the force of myocardial contraction), but in some cases they cause side effects in the form of arrhythmia, tachycardia, atrial fibrillation and ventricular fibrillation. |
| Drugs used for heart blocks (M-anticholinergics, sympathomimetics) | The side effects of the drugs manifest themselves in the form of stimulation of the central nervous system, increased blood pressure, which directly affects heart rhythm. |
Also, the development of PVCs can be affected by other pathologies not associated with disruption of the cardiovascular system:
- Diabetes mellitus type 2 . One of the serious complications of the disease associated with carbohydrate imbalance is diabetic autonomic neuropathy, which affects nerve fibers. In the future, this leads to a change in the functioning of the heart, which “automatically” causes arrhythmia.
- Hyperfunction of the thyroid gland (moderate and severe thyrotoxicosis). In medicine, there is such a concept as “thyrotoxic heart,” which is characterized as a complex of cardiac disorders - hyperfunction, cardiosclerosis, heart failure, extrasystole.
- In diseases of the adrenal glands, there is an increased production of aldosterone, which in turn leads to hypertension and metabolic disorders, which is interconnected with the work of the myocardium.
Ventricular extrasystole is not of an organic nature (when there are no concomitant cardiac diseases), caused by a provoking factor, often has a functional form. If you remove the negative aspect, then in many cases the rhythm returns to normal.
Functional factors of ventricular extrasystole:
- Electrolyte imbalance (reduction or excess of potassium, calcium and sodium in the blood). The main reasons for the development of the condition are changes in urination (rapid production or vice versa, urinary retention), malnutrition, post-traumatic and postoperative conditions, liver damage, and surgery on the small intestine.
- Substance abuse (smoking, alcohol and drug addiction). This leads to tachycardia, changes in material metabolism and disruption of myocardial nutrition.
- Disorders of the autonomic nervous system due to somatotrophic changes (neuroses, psychoses, panic attacks) and damage to subcortical structures (occurs with brain injuries and pathologies of the central nervous system). This directly affects the functioning of the heart and also provokes surges in blood pressure.
Ventricular extrasystoles disrupt the entire heart rhythm. Pathological impulses over time have a negative effect on the myocardium and the body as a whole.
Classification
The classification of ventricular extrasystoles covers all the characteristics of the phenomenon that has arisen.
This is necessary for specialists in order to adequately assess the threat to health, prescribe effective treatment (if necessary) and make a prognosis.
Consequently, according to the source of occurrence of PVCs there are:
- Monotopic - with one ectopic focus of the impulse (in one ventricle).
- Polytopic - with several secondary foci of impulse (left ventricular and right ventricular at the same time).
According to the duration of the compensatory pause:
- A complete compensatory pause means that the sum of the pre- and post-ectopic interval is equivalent in duration to the two main cardiac cycles.
- Incomplete compensatory pause - if the sum of the intervals is less than the duration of the two main cardiac cycles.
According to Lown-Wolf-Ryan (B. Lown, M. Wolf, M. Ryan), ventricular extrasystoles are divided into 5 degrees to take into account the risk of developing fibrillation:
- 1st degree – monomorphic extrasystoles (less than 30 per hour allowed).
- 2nd degree – monomorphic, more than 30 per hour.
- 3rd degree – polymorphic (group, paired) extraordinary contractions.
- 4th degree - divided into subcategories “a” - twin, “b” - salvo.
- Grade 5 – volley polymorphic PVCs (3-5 in half a minute), fixing paroxysmal supraventricular tachycardia. In such a situation, a person needs emergency help.
There is also a 0 (zero) degree. It means the complete absence of extrasystoles (single).
Gradation by time of occurrence:
- Early - occurring during the passage of an impulse through the atria.
- Interpolated - simultaneous contraction of the right and left ventricles with the atria occurs.
- Late - extrasystoles during the “rest” of the upper chambers of the heart.
Circadian types of extrasystoles:
- mixed;
- daytime;
- nocturnal
According to their rhythm, they are divided into allorhythms (periodic) and sporadic (single, irregular) extraordinary contractions.
Allorhythmia is divided into:
- Bigeminy - for every second normal contraction there is 1 extrasystole.
- Trigemy - every third.
- Quadrigeminiy - every fourth contraction is interrupted by an extraordinary contraction.
Classification of extrasystoles according to Bigger
Bigger's classification provides for the formation of groups of patients according to the degree of increase in the risk of complications.
It includes the following course of extrasystole:
- malignant;
- potentially malignant;
- benign.
With benign extrasystoles, the risk of complications is extremely low. Moreover, such patients have no signs of pathology of the cardiovascular system in the anamnesis and during examination (normal left ventricular ejection fraction, no hypertrophy or cicatricial changes in the myocardium). The frequency of ventricular extrasystoles does not exceed 10 per hour and there is no clinical picture of paroxysmal ventricular tachycardia.
A potentially malignant disease is characterized by a moderate or low risk of sudden death. The examination reveals structural changes in the heart in the compensation stage. Ultrasound of the heart reveals a decrease in LV ejection fraction (30-55%) and the presence of scar or myocardial hypertrophy. Patients complain of a feeling of interruptions in the work of the heart, accompanied by short-term episodes of ventricular tachycardia (up to 30 seconds).
Malignant extrasystoles are those whose manifestation causes a disturbance in the general well-being of the patient (palpitations, fainting, signs of cardiac arrest). Patients exhibit a critical decrease in ejection fraction - less than 30%. Persistent ventricular tachycardia is also noted.
The most dangerous ventricular ecstasystoles include 3 gradations in the Lown classification - 4a, 4b and 5 classes.
Symptoms
If the patient does not have underlying cardiac pathologies, then, paradoxically, ventricular extrasystole is more difficult for them to tolerate than with the presence of diseases.
This is due to some compensatory capabilities of the body.
In a young, relatively healthy person, VES will manifest itself:
- A feeling of “cardiac arrest” followed by a series of palpable beats. Trying to describe their condition, patients say that their heart is sinking.
- Several strong heartbeats against the background of a calm state.
Women during pregnancy also often experience a sensation of extraordinary shocks in the heart area. This is due to hormonal changes, but if the symptoms are alarming, you need to consult a doctor and measure all indicators.
Even in the presence of all the above symptoms and signs, it is possible to assert the presence of ventricular extrasystole only on the basis of diagnostic results.
Important: if any interruptions in the functioning of the heart occur, you must consult a general practitioner or cardiologist.
Treatment of extrasystole
If extrasystoles are detected, there is no need to self-medicate. First of all, you need to find out the reason. During the interview, it is found out what diseases the patient has, heredity, and the presence of heart disease.
If extrasystole can not be treated, then it is advisable not to treat it.
The choice of treatment for extrasystoles depends on which heart they occurred on. If a person does not have organic heart pathology, this is one case. If extrasystoles occur due to heart disease, the approach is completely different. Therefore, the most important thing is to determine whether there is heart disease or not. What is organic heart pathology? These are a history of myocardial infarction, low ejection fraction, and valvular heart disease. When treating extrasystoles, you need to take into account the type of extrasystoles (ventricular or supraventricular).
Recommendations from Academician A. Revishvili
Here are the approaches to treatment offered by the famous academician A. Revishvili:
- it is considered dangerous and therapy is necessary for extrasystole more than 20,000/day and if there is heart disease;
- no treatment is required for extrasystole less than 20,000/day and the person does not feel them;
- Treatment is required if there are 100 extrasystoles per day. A person feels each of them as a “blow to the chest.”
- also, treatment is not required if 200 extrasystoles per day are detected and when there is no heart disease.
Treatment of extrasystole in patients without cardiovascular pathology
So, let's consider the treatment of extrasystoles in a person without heart pathology. Most of these extrasystoles are safe. With functional extrasystoles, treatment of the underlying disease is important.
Observation by a doctor and monitoring of extrasystoles using echocardiographic examination twice a year are recommended. Sedatives can be used. If symptoms are severe, antiarrhythmic drugs . These are mainly 2 classes of antiarrhythmic drugs - beta-blockers and class I drugs (Propafenone, Allapinin). The main role of beta-blockers is their effect on the characteristics of extrasystoles, but they do not eliminate the symptoms of the disease. And class I drugs reduce the number of extrasystoles.
Treatment of extrasystole due to heart disease
If extrasystole is associated with heart disease, then potassium, magnesium, and metabolic agents (omega-3 PUFAs) are used. Among the antiarrhythmic drugs for the treatment of ventricular extrasystoles, beta-blockers (Metoprolol, Bisoprolol) in combination with Amiodarone are used. Amiodarone may be recommended to relieve symptoms of arrhythmia. It must be remembered that patients after myocardial infarction should not take class I drugs.
Calcium antagonists (Verapamil, Diltiazem) are used primarily for supraventricular arrhythmias. Also, beta-blockers and class I drugs (Allapinin, Propafenone) are effective for supraventricular extrasystole. If the patient has bradycardia, then the dosage of drugs must be carefully selected.
Surgery
If drug treatment does not help, then the question of surgical treatment . This is the so-called radiofrequency ablation of ectopic sites. In later stages of the disease, heart transplantation is necessary.
Photo: https://pixabay.com/illustrations/pill-capsule-medicine-medical-1884775/
ECG and other diagnostic methods
The following methods are used to diagnose the disease:
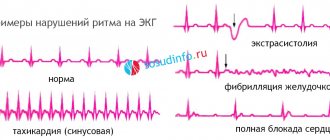
- ECG. Allows you to record everything that happens to the human heart during systole (contraction) and diastole (relaxation). When deciphering the cardiogram, the appearance of an expanded and deformed ventricular QRS complex, a complete compensatory pause, the absence of a P wave before an extraordinary contraction, and a change in the refractory period are observed.
- ECG monitoring according to Holter. This is a diagnostic method during which a special device with sensors is attached to a person, with which he must live his normal day. It is this daily observation that gives specialists the opportunity to track the periods and frequency of occurrence of extraordinary contractions of the ventricles. Holter monitoring is the main method for diagnosing PVCs.
- Bicycle ergometry. The method is used to confirm or refute the relationship between pathology and physical activity.
Additional diagnostic methods are used:
- General and biochemical blood test (to detect cholesterol levels, which could trigger the development of atherosclerosis).
- Blood test for thyroid hormones.
- Treadmill test.
- Echocardiography.
- Polycardiography.
- Rhythmocardiography.
- Transesophageal ECG.
- Sphygmography.
Usually, to determine the correct diagnosis, the patient only needs to undergo an ECG and a Holter study, but in some cases a detailed blood test and stress tests may be required.
Diagnostics
The diagnosis of ventricular extrasystole is made based on the patient’s complaints, as well as laboratory and instrumental examination.
During the collection of anamnesis, complaints about well-being, the time and frequency of their occurrence are clarified, and information about the patient’s bad habits, previous diseases, heredity, and lifestyle is also collected.
Laboratory diagnostics - laboratory tests and examinations are prescribed to establish the cause of extrasystole. The body is checked for hormonal disorders, changes in electrolyte balance, the presence of toxins, infections, and ischemic disorders in the myocardium of the heart.
Instrumental diagnostics are aimed at identifying and assessing the degree of damage to the left ventricle due to extrasystoles. ECG is important in the diagnosis of ventricular extrasystole. Its correct decoding makes it possible not only to detect extrasystoles, but also to determine where the impulses are coming from. With a left ventricular extrasystole, the ECG shows a premature contraction of the heart, reminiscent of a right bundle branch block; with a right ventricular extrasystole, a left bundle branch block.
A stress test is also useful for diagnosis. The patient is given an ECG, then given a little exercise, and then the ECG is taken again. Idiopathic ventricular extrasystole goes away after exercise. If it occurs due to heart disease, then the load only intensifies it.
An ECG can also reveal the time of occurrence of extrasystoles. With early or late extrasystoles, a complete compensatory pause usually follows. With interpolated, that is, the so-called intercalary ventricular extrasystole, there is no such pause. It is called intercalary because it is inserted between two normal contractions of parts of the heart.
However, with single extrasystoles that do not occur so often, the ECG may not give the desired result. Then Holter monitoring comes to the rescue. Electrocardiographic readings are recorded throughout the day, from which one can already judge the frequency of occurrence of extrasystoles, as well as the degree of electrical instability of the heart.
In addition, the following instrumental diagnostic methods are used:
- Echocardiography – it allows you to find out structural changes in the heart;
- Electrophysiological study - a special catheter is inserted into the cavity of the heart, which, using electrical impulses, stimulates contraction of the heart muscle. At the same time, a cardiogram of the heart is recorded. This method is used when the ECG does not give clear results, and also to assess the functioning of the conduction system of the heart.
- MRI of the heart is rarely performed, mainly when the data obtained from echocardiography turned out to be not very informative.
Therapy for ventricular extrasystole
Depending on the cause of the pathology, the specialist individually selects a method of treating the patient.
There is one general rule: therapy must be comprehensive. This is the only way to relieve symptoms.
General recommendations
First of all, patients should exclude idiopathic factors that provoke ventricular extrasystoles and possible complications:
- Quit smoking (completely).
- Reduce the amount of coffee and strong tea to 1 cup per day.
- Abstain from drinking.
- Do simple exercises (exercises) every day.
As for athletes, if they feel tremors in the heart after physical activity and this is visible on electrocardiography, it should be moderated or eliminated for a while. If the symptoms of PVCs do not manifest themselves in characteristic episodes, or they are single, then you can play sports.
Diet is what doctors prescribe for almost any disease. Indeed, properly organized nutrition at home will help the cardiovascular system cope with pathology faster.
You should refuse:
- fat;
- fried;
- products with synthetic food additives (yogurt, chips);
- salty (salt increases blood pressure, which can increase the frequency of extrasystole attacks).
Overeating is strictly prohibited. Eating should be slow, you should leave the table with a feeling of pleasant satiety, not heaviness.
It will be useful to include in your diet:
- bananas;
- dried fruits;
- natural dairy products;
- raw vegetables, nuts.
Drug treatment
If pathological contractions of the ventricles of the heart occur more than 30 times per hour, and lifestyle and nutrition adjustments have not helped, and the patient complains of a palpable, sharp heartbeat, doctors prescribe medication.
Its goal is to eliminate symptoms and prevent the development of severe types of arrhythmias:
- Stage 1 - sedative herbal medicines, ß-blockers (Obzidan, Anaprilin, Nebilet), blood thinners (Aspirin, Cardiomagnyl), Panangin, Asparkam.
- Stage 2 – administration of antiarrhythmic drugs (if there is no effect of treatment at stage 1). According to cardiologists, class 2 antiarrhythmics are considered the safest. These are Allapinin, Amiodarone, Propranolol, Metoprolol, Verapamil. "Etatsizin" (1st class), "Lidocaine", "Mexarithm".
- Stage 3 - taking class 3 antiarrhythmic drugs (Amiodarone, Cordarone) - the drugs of choice to prevent ventricular fibrillation.
- Stage 4 – use of a combination of drugs (ß-blockers, antiarrhythmics).
Important: these medications have a pronounced cardiac effect, so only a doctor can take into account all the risks and prescribe it to the patient. The choice of medication and dosage should be entrusted to a cardiologist; self-medication with antiarrhythmics is unacceptable.
Surgical methods
The opinions of cardiologists regarding surgical intervention for this pathology agree on one thing - it is indicated for the patient only if it was not possible to get rid of extrasystole with the help of medications.
The most commonly used method is called radiofrequency ablation (RFA). During the procedure, with the help of radio waves, sources of pathological impulses are destroyed.
A contraindication to surgery in adults may be that the patient is not able to tolerate general anesthesia.
Forecast and prevention of frequent ventricular extrasystole
The prognosis for the course of ventricular extrasystole depends on its form, the presence of morphological pathology of the heart tissue or hemodynamic disorders. Functional idiopathic and single extraordinary contractions of the myocardium do not pose a threat to the health or life of the patient. Extrasystole, which develops against the background of organic damage to the heart, in the absence of treatment, significantly increases the risk of developing organ failure, sudden death due to the development of tachycardia, atrial fibrillation and supraventricular arrhythmias, and fibrillation.
To prevent the development of frequent extraordinary contractions of the myocardium of the lower part of the heart, it is recommended to carry out the following measures:
- If you have a genetic predisposition to heart disease, you should start seeing a cardiologist as early as possible.
- Use medications with caution that affect heart rate and blood electrolyte composition (diuretics, glycosides).
- If you have endocrine pathologies (diabetes mellitus, hyperfunction of the adrenal glands or thyroid gland), you should be examined for the development of cardiac pathologies.
- Stop smoking and drinking alcohol.
Forecast
Even if the patient has been diagnosed with ventricular extrasystole due to heart disease, treatment should be started as early as possible, not deviate from the pill regimen prescribed by the doctor, and lead a healthy lifestyle. Only in this case will the prognosis be favorable and the person will be able to cure the pathology and live a long, fulfilling life.
Even if the heart is not bothered by interruptions in its work, it is very important to understand that many pathologies occur hidden and are detected too late (especially in men). Therefore, it is extremely important to undergo a routine medical examination and an ECG every year.
Author of the article: Yulia Dmitrieva (Sych) - In 2014, she graduated with honors from Saratov State Medical University named after V. I. Razumovsky. Currently working as a cardiologist at the 8th City Clinical Hospital in the 1st clinic.
Complications and probable prognosis
The consequences of ventricular extrasystole are monotonous:
- Heart failure. Requires urgent resuscitation. There are only a few minutes. In an inpatient setting, the chances of recovery are greater.
- Tachycardia. Significantly reduces the quality of life, worsens the outcome of the pathological process significantly.
- Ventricular arrhythmia. Joins almost instantly. Aggravates the development of the underlying disease.
All of these phenomena, one way or another, lead to the death of the patient. It's a question of time. Therefore, there is no point in delaying treatment and diagnosis.
The forecast data is something like this:
- With single extrasystoles, there are almost no risks. The likelihood of complications is about 2-5% for 5 years or more.
- The opposite phenomenon with group contractions is accompanied by severe problems in 65% of situations without therapy, one and a half to two times less with supervision.
A complete cure never occurs, but there are chances to improve the quality of life and prolong one’s existence. From a prognostic point of view, types 3,4,5 of the process are the least favorable. 1 and 2 do not pose a danger to life and health.