Myocardial infarction is one of the most severe cardiovascular diseases. It is often complicated by various pathologies, including post-infarction cardiosclerosis. This disease is considered quite severe and requires appropriate treatment.
Post-infarction cardiosclerosis (PICC) is a cardiovascular disease in which myocardiocytes are replaced by connective tissue. Most often, this is facilitated by cell necrosis, which occurs during long-term ischemia of the heart muscle. As a result, the activity of the heart is disrupted, and various forms of arrhythmia can develop.
The disease is included in the International Classification of Diseases (ICD-10), where it is located under code I25.1 and the name “Atherosclerotic heart disease. Coronary arteries: atheroma, atherosclerosis, disease, sclerosis.”
To examine patients with suspected post-infarction cardiosclerosis, various examination methods are used (electrocardiography, cardiac ultrasound, chest X-ray). After an accurate diagnosis has been established, treatment must be prescribed, since without this there is a risk of developing heart failure.
Video What is cardiosclerosis?
Definition
Post-infarction cardiosclerosis is the presence of areas of the heart that died as a result of a myocardial infarction and were replaced by connective tissue.
The transformation of the heart muscle begins 3-4 days after the vascular accident and is completed by the end of 2-4 months. It is impossible to make a diagnosis at an earlier time. Mortality from the pathology, according to personal observations, is about 20% in the first few hours after an attack and about 30-40% in the long-term period (1-5 years). The volume and density of scarring directly depends on the area of myocardial damage and is a determining factor in the prognosis of the disease.
Etiology
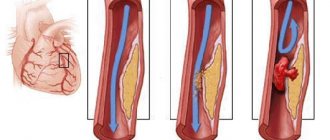
Post-infarction cardiosclerosis has only one cause. This is a myocardial infarction - an acute disruption of the blood supply to the heart as a result of obstruction of the coronary arteries.
The following can lead to blockage of blood vessels:
- migrating blood clots (usually from the veins of the lower extremities);
- application of thrombotic masses to ulcerated atherosclerotic plaques;
- functional disorders of the central nervous system, leading to severe spasm of the coronary arteries;
- anatomical defects of the vascular wall due to the long course of hypertension, diabetes mellitus, etc.
As a result, individual segments of the muscular organ stop receiving blood enriched with oxygen, and after 4-6 hours they begin to die.
Under the influence of enzymes, myocytes are resorbed and replaced by a scar, the existence of which entails many problems in the future:
- rhythm and conduction disturbances;
- decreased cardiac output and cardiac output;
- cardiomyopathy (hypertrophy or dilatation of organ chambers).
Scar changes can affect the valves (the mitral valve is most often involved), leading to their insufficiency. My professional experience shows that in 100% of cases myocardial infarction does not go away without leaving a trace. Complications progress and significantly reduce life expectancy.
The following risk factors significantly increase the incidence of a heart attack:
- male gender;
- age over 45 years;
- arterial hypertension;
- smoking;
- obesity (BMI over 30);
- diabetes;
- low physical activity (WHO recommends walking a distance of 8,000 steps daily);
- alcohol abuse (more than 20 g of pure ethanol per day for women and 40 g for men).
Read more about risk factors here.
In most cases, myocardial infarction develops against the background of a long course of coronary heart disease, although in my practice I have encountered young patients (25-30 years old) with a similar disease who lead an unhealthy lifestyle (overweight, abuse of alcohol, drugs and smoking).
Clinical picture
The symptoms of the pathology are extremely varied. At the initial stages (first six months) the following may be detected:
- Conduction disorders ( AV blockade, slow conduction along Purkinje fibers and His bundles). The phenomena are caused by damage to the conduction system when nerve fibers are transformed into connective tissue. They manifest themselves as sensations of interruptions in work or prolonged cardiac arrest, periodic fainting and dizziness.
- Tachyatrhythmias . Atrial or ventricular fibrillation often occurs, in which the contraction frequency of individual fibers reaches 350-800 per minute. The patient feels an attack of palpitations, weakness, and possible episodes of loss of consciousness due to impaired tissue oxygenation.
When the scar thickens, it can compress other coronary vessels, provoking or aggravating the manifestations of coronary heart disease (angina):
- pain and shortness of breath with little physical activity;
- general weakness, fatigue.
After 6-12 months, the heart tries to compensatoryly return to its previous functional activity. Hypertrophic changes and dilatation of the organ chambers occur. Such phenomena contribute to the increase in signs of heart failure.
When the left half of the heart is predominantly affected, pulmonary edema is observed with symptoms such as:
- discomfort in the chest (tightness, pressure);
- shortness of breath (up to 40-60 respiratory movements per minute) at rest or with little physical activity;
- pale skin;
- acrocyanosis (bluish coloration of the limbs, nasolabial triangle).
All symptoms are relieved in the “orthoptic” position (sitting on a chair with legs down), due to which the patient feels relief.
Insufficiency of the right sections of the muscular organ is manifested by stagnation of blood in the systemic circulation:
- Edema syndrome. Fluid retention can be observed in the lower extremities, liver (enlarged in size, painful on palpation), and less commonly in body cavities (hydrothorax, hydropericardium, ascites).
- Shortness of breath . Caused by tissue hypoxia.
Subsequently, all types of metabolism are significantly disrupted, acidosis and irreversible changes in organs (dystrophy and sclerosis) develop, which is manifested by their failure.
With cardiosclerosis, changes in the heart are irreversible and manifestations of circulatory disorders will steadily increase. I have encountered patients who were practically bedridden and could not exist without oxygen support.
Symptoms
There are no unique symptoms characteristic of cardiosclerosis. For a long time, the pathology may not manifest itself and be asymptomatic.
However, upon careful questioning, patients present the following complaints:
- heaviness in the left half of the chest;
- pain in the heart area of a compressive nature, which occurs and intensifies during physical overload, stress, and is relieved after taking nitrates;
- shortness of breath is often permanent;
- high pulse;
- a feeling of irregular heartbeat, a feeling of freezing during the next contractions;
- weakness, fatigue;
- low performance;
- lack of endurance during physical effort;
- increase or decrease in blood pressure values;
- swelling.
These symptoms have their own severity in each patient. They do not determine the diagnosis, but only indicate the severity of the condition.
Deadly complications
Typical disorders of the body have already been described above, but there are a number of pathologies that pose a direct threat to life and cause death, including sudden death. These include:
- Aneurysm . The wall of the organ becomes thinner and stretched, and rupture with cardiac tamponade can occur at any time.
- Blockade . The impulse is not transmitted to individual parts of the heart, which stop contracting.
- Atrial fibrillation or extrasystole is the uncoordinated work of different parts of the organ. If fibrillation is severe and emergency assistance is not provided, the complication can be fatal.
- Acute heart failure is the final stage of chronic heart failure, when the organ is no longer able to provide adequate blood flow. The cause of death is ischemia.
Diagnostics
All patients who have suffered a myocardial infarction require clinical observation, which includes the following types of laboratory and instrumental studies:
- General blood test (detection of possible changes: leukocytosis, rise in ESR).
- Electrocardiogram . The ECG shows all conduction pathologies, episodes of overload against the background of post-infarction cardiosclerosis, and hypertrophic changes.
- Echo-CG is a key way to recognize abnormalities, allowing you to visualize the volume of muscle tissue involved, the degree of loss of functional activity, and concomitant disorders of the valve apparatus.
- Survey radiography of the chest organs . The parts of the heart are usually dilated, the cardiothoracic index exceeds 50%.
- Coronography . The method allows you to assess the diameter of the lumen of the coronary arteries and, if necessary, refer patients for surgical treatment.
- INR . The study is important for prescribing anticoagulant and antiplatelet therapy, which is a key stage of secondary prevention.
If there are signs of heart failure (they are present in 80% of cases), a thorough assessment of a biochemical blood test is indicated.
The following indicators are determined:
- Lipid profile (total cholesterol, HDL, LDL, TAG, atherogenic index). The values characterize the risk of recurrent myocardial infarction.
- Markers of liver necrosis. Against the background of congestive right ventricular failure, the level of ALT and AST, bilirubin (direct and indirect) often increases, which indicate the death of hepatocytes.
- Renal complex (urea, creatinine, electrolytes). A rise signals CKD.
If there are signs of damage to various organs, enhanced diagnostics are carried out, and algorithms for subsequent compensation of conditions are developed.
Consequences
A patient with the diagnosis in question needs lifelong medical supervision. Knowing what post-infarction cardiosclerosis is, one cannot ignore the situation, as this leads to inevitable complications in the form of the following consequences:
- pericardial tamponade;
- atrial fibrillation;
- thromboembolism;
- blockades;
- pulmonary edema;
- tachycardia;
- decreased automaticity of the sinoatrial node.
These processes negatively affect a person’s quality of life. The patient loses tolerance to physical activity, loses the opportunity to work and lead a normal life. Advanced cardiosclerosis provokes the appearance of an aneurysm, the rupture of which leads to death in 90% of non-operated patients.
Treatment
It should be understood that cardiosclerosis is an irreversible pathology and all therapy is aimed exclusively at slowing the progression of heart failure and correcting rhythm disturbances. Often, patients do not realize this and quickly return to their usual incorrect lifestyle, not realizing that they will soon find themselves on the border with death. Judging by the experience of working in the emergency department, such persons are encountered quite often (about every 5th). Why is this happening? This remains a mystery to me.
Non-drug
Treatment of a pathology such as post-infarction cardiosclerosis involves a complete change in lifestyle. All patients are recommended to do feasible exercise (therapeutic exercises, aerobic exercises, walks in parks, etc.) It is advisable to carry out training daily.
The second condition is giving up bad habits (drinking alcohol and smoking) and correcting your diet. Fatty, spicy, fried foods are completely excluded, table salt is limited to 2 g/day. The basis of the diet is fresh vegetables and fruits, seafood (fish, squid, shrimp), vegetable oils, whole grain bakery products.
Prevention
The practice of the principles of a healthy lifestyle is the prevention of many pathologies, including post-infarction cardiosclerosis. This disease, like any other cardiovascular disorder, is closely related to a person’s diet and lifestyle, so to prevent the development of PICS, you should follow some simple rules:
- It is important to eat a healthy and balanced diet. In particular, you need to eat small meals, but often, about 5-6 times a day. Products should be selected rich in potassium and magnesium.
- Physical activity should be regular, but without overload.
- Adequate rest and adequate sleep are of great importance.
- It is necessary to maintain emotional stability, for which stress should be avoided.
- Moderate spa treatments are beneficial.
- Therapeutic massage has a good effect on the body.
- It is worth maintaining a positive attitude no matter what.
Paying special attention to nutrition, it should be noted:
- It is useful to give up coffee and alcohol.
- It is necessary to minimize the consumption of tonic drinks (cocoa, black tea)
- Salt should be consumed in limited quantities
- Avoid heavy consumption of garlic and onions
- Fish varieties should be low-fat.
The accumulation of gas in the intestines can also have a bad effect on a person’s condition, so it is important to limit the consumption of beans, milk, and fresh cabbage of any variety. Also, in order to prevent the development of atherosclerosis, leading to PICS, it is necessary to exclude the lungs, liver, and brain of animals from the diet. It's better to eat more greens and fruits instead.
4.83 Aug. rating ( 95 % score) – 6 votes – ratings
Expert advice
I always tell patients about the high risk of recurrence of a vascular accident in order to create motivation for lifestyle correction. An important criterion is to bring the body mass index and abdominal circumference to standard values - 18.5-24.9 kg/m2 and 80 cm, respectively. Taking care of your health is a guarantee of a long and happy life!
Drug therapy
Treatment of post-infarction cardiosclerosis in the presence or progression of signs of myocardial ischemia involves the administration of nitrates. Their use is justified both on an ongoing basis and during attacks. Long-acting nitro drugs (“Nitrolong”, “Isosorbide dinitrate”) and symptomatic ones (for chest pain) are recommended. To stop a seizure, Nitrospray and regular Nitroglycerin are indicated.
The presence of arterial hypertension is an indication for antihypertensive therapy, which includes at least 2 groups of drugs from the main ones:
- ACE inhibitors and AARs (“Enalapril”, “Valsartan”, “Captopril”). They act at the level of the renin-angiotensin-aldosterone system, quickly and lastingly reduce blood pressure, and prevent myocardial remodeling.
- Diuretics - reduce blood pressure by removing fluid from the body, indicated for edema. Thiazide (“Indapamide”) and loop (“Furosemide”, “Torasemide”) are usually used.
- Beta blockers (Bisoprolol, Atenolol, Metoprolol, Nebivalol, Carvedilol) - reduce the total peripheral resistance of the vascular bed, reduce heart rate and weaken the strength of contractions of the heart muscle, promoting relaxation and rest of the myocardium. They are a means of preventing tachyarrhythmias.
- Calcium antagonists - relax the muscular wall of the arteries and have a mild diuretic effect. More often, drugs of the dihydroperidine series are prescribed (Nifedepine, Corinfar, Lacidipine).
To reduce the severity of oxygen starvation and increase the functionality of organs, antihypoxants are used. The only remedy with a proven effect is Preductal. My patients already notice an improvement in mental and associative processes, memory activation, and improved mood within 3-5 days. Mexidol has proven itself to be excellent in neurology.
Atherosclerosis occurring in the post-infarction period should be the reason for prescribing statins (Rosuvastatin). Fibrates and blockers of cholesterol absorption in the intestine (Ezetrol) are used less frequently.
For severe heart failure, glycosides are used. Medicines of this pharmacological group increase the activity of myocytes and slightly reduce the frequency of contractions.
Glycosides cause the heart to work to the detriment of its own condition. For some time, heart failure stabilizes, and then the myocardium is completely depleted, circulatory disorders increase and death from cardiogenic shock may occur. Consequently, such medications are used in exceptional cases, or in extremely small doses.
All patients undergo prophylaxis of thromboembolic complications. Anticoagulants are used (Heparin, Xarelto).
Surgical correction
In case of severe rhythm disturbances, when the hollow muscular organ is not able to cope with the load on its own, an electrical pacemaker or cardioverter is installed. They are activated during extrasystole, cardiac arrest, tachyarrhythmias and quickly normalize myocardial function.
The formation of an aneurysm is an indication for resection of the thinned area. The operation requires wide access and lengthy manipulations. Usually not performed in older people.
Clinical example
An important stage in compensating for the general condition is the psychological component of the patient and his adherence to treatment.
I would like to give an interesting example from the experience of my colleague. Patient N., 47 years old. Suffered a large-focal myocardial infarction. The diagnosis was made based on an ECG and troponin test. The lower and lateral walls and the apex of the left ventricle were affected. The typical picture of the disease (acute pain syndrome, circulatory disorders) was absent, and therefore, he sought help only 12 hours after the acute thrombosis.
Thrombolytics were ineffective in the long term (more than 4-6 hours), symptomatic therapy was carried out. The patient felt excellent, refused treatment and the prescription of preventive medications, and left the hospital on his own.
After 3 months, he was readmitted to the hospital with severe signs of left ventricular failure. “The diagnosis was made: IHD. Post-infarction cardiosclerosis. CHF III. FC III. Left ventricular aneurysm.” Full life activity was no longer possible. The patient died from cardiac tamponade on the 10th day. If doctors' instructions were followed, this condition could develop only after several years.
Thus, post-infarction cardiosclerosis is a problem faced by almost every person who has suffered a myocardial infarction. It is necessary to understand that the appearance of any signs of cardiac dysfunction that have not previously manifested is an indication for urgent medical help. Only properly selected therapy will ensure a comfortable life.
Could it be the cause of death?
The risk of sudden clinical death for people with this diagnosis is quite high. The forecast is made based on information about the degree of neglect of the pathology and the location of its foci. A life-threatening condition occurs when the blood flow is less than 80% of normal, and the left ventricle is susceptible to sclerotization.
When the disease reaches this stage, a heart transplant is required. Without surgery, even with supportive drug therapy, the survival prognosis does not exceed five years.
In addition, with post-infarction cardiosclerosis, the causes of death are:
- uncoordinated ventricular contractions (fibrillation);
- cardiogenic shock;
- aneurysm rupture;
- cessation of bioelectrical conduction of the heart (asystole).
To avoid irreversible consequences, the patient after a heart attack needs to carefully monitor the body’s reactions. At the first sign of exacerbation, immediately visit a cardiologist.