Action potential (AP) is a short-term amplitude change in the resting membrane potential (RMP) that occurs when a living cell is excited. Essentially, this is an electrical discharge - a rapid, short-term change in potential in a small area of the membrane of an excitable cell (neuron or muscle fiber), as a result of which the outer surface of this area becomes negatively charged in relation to neighboring areas of the membrane, while its inner surface becomes positively charged in relation to to adjacent areas of the membrane. The action potential is the physical basis of a nerve or muscle impulse that plays a signaling (regulatory) role.
general characteristics
Action potentials can differ in their parameters depending on the type of cell and even on different parts of the membrane of the same cell. The most typical example of differences is the action potential of the heart muscle and the action potential of most neurons. Nevertheless, the basis of any action potential is the following phenomena:
- “The membrane of a living cell is polarized” - its inner surface is charged negatively in relation to the outer one due to the fact that in the solution at its outer surface there is a larger number of positively charged particles (cations), and at the inner surface there is a larger number of negatively charged particles (anions).
- “A membrane has selective permeability” - its permeability to different particles (atoms or molecules) depends on their size, electrical charge and chemical properties.
- “The membrane of an excitable cell is capable of quickly changing its permeability for a certain type of cations, causing a transition of positive charge from the outside to the inside
The first two properties are characteristic of all living cells. The third is a feature of excitable tissue cells and the reason why their membranes are able to generate and conduct action potentials.
The main mathematical model describing the generation and transmission of action potentials is the Hodgkin-Huxley model.
Left ventricular hypertrophy of the heart: treatment, causes, symptoms
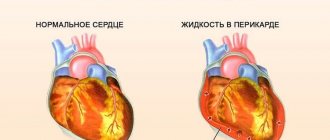
Left ventricular hypertrophy is a syndrome characteristic of most diseases of the cardiovascular system, which consists of an increase in the muscle mass of the heart.
Unfortunately, today there are more and more cases of left ventricular hypertrophy in young people. The danger of this is complemented by a higher percentage of deaths than in older people. Men with left ventricular myocardial hypertrophy die 7 times more often than the fairer sex.
Development mechanism
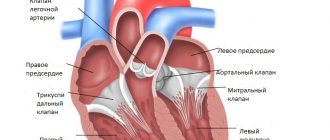
In a normal physiological state, the heart, pushing blood into the aorta, performs the function of a pump. From the aorta, blood flows to all organs. When the left ventricle relaxes, it receives a portion of blood from the left atrium. Its quantity is constant and sufficient to ensure optimal levels of gas exchange and other metabolic functions throughout the body.
As a consequence of the formation of pathological changes in the cardiovascular system, it becomes more difficult for the heart muscle to perform this function. To perform the same amount of work requires more energy expenditure. Then a natural compensatory mechanism is activated - an increase in load leads to an increase in the muscle mass of the heart. This can be compared to how increasing the load on the muscles in the gym results in an increase in muscle mass and volume.
Why can’t the left ventricle “build up” its muscle mass without disturbing its owner? The fact is that in the heart tissue only cardiomyocytes increase. And they make up only about a quarter of the heart tissue. The connective tissue part does not change.
The capillary network does not have time to develop after LV hypertrophy, so rapidly hypertrophied tissue may suffer from oxygen starvation. Which leads to ischemic changes in the myocardium. In addition, the conduction system of the heart remains the same, which leads to disruption of impulse conduction and various arrhythmias.
The tissue of the left ventricle, in particular the interventricular septum, is most susceptible to hypertrophy.
During intense physical activity, the heart has to pump more blood and work harder. Therefore, professional athletes may develop moderate left ventricular hypertrophy, which is physiological or compensatory.
Etiology of hypertrophy
In almost all long-term heart diseases, left ventricular hypertrophy is an obligatory consequence.
Left ventricular myocardial hypertrophy is observed with:
- hypertension;
- aortic valve stenosis;
- hypertrophic cardiomyopathy;
- intense long-term physical activity;
- obesity;
- smoking, drinking alcohol.
Thus, for any heart disease, left ventricular hypertrophy is a mandatory syndrome.
Hypertension, especially persistent and poorly treated hypertension, is the main culprit. If the patient says that high blood pressure numbers are familiar and “working” for him, if hypertension was corrected only occasionally or not treated at all, then he certainly has severe hypertrophy of the left ventricle of the heart.
Excess weight is a risk factor for hypertension, which causes left ventricular hypertrophy. In addition, with obesity, blood supply to an enlarged body requires a lot of work to ensure blood supply to all tissues, which also leads to changes in the myocardium.
Of the congenital diseases, the main place is in heart defects with impaired blood outflow from the ventricle.
However, left ventricular hypertrophy will show the same symptoms for any etiology.
Types of hypertrophy
According to the degree of change in the shape of the left ventricle of the heart and its thickness, eccentric and concentric hypertrophy of the left ventricular myocardium is distinguished.
Concentric hypertrophy of the left ventricle is characterized by thickening of its walls. Its cavity in this case does not change. It is formed when the ventricle is overloaded with blood pressure. This form is typical for hypertension. This etiology accounts for at least 90% and has a high risk of life-threatening cardiovascular complications - more than 35%.
Eccentric left ventricular hypertrophy is characterized by relative preservation of the thickness of the walls of the ventricle, an increase in its mass and the size of the cavity. The risk of severe complications is about 25%. This type develops when there is excess blood volume.
How to suspect a disease
For a long time, left ventricular hypertrophy of the heart has minor symptoms or the heart does not let you know that it is working through force. When compensatory capabilities are exhausted and a person begins to complain, the changes in the myocardium are already significant.
The following signs of left ventricular hypertrophy appear in varying degrees of severity:
- dyspnea;
- tachycardia;
- cardiac pain;
- feeling of weakness and fainting;
- fast fatiguability.
Timely early detection reduces the risk of developing severe complications. ECG signs of left ventricular hypertrophy are easily determined by any therapist. This method is cheap and informative.
Left ventricular hypertrophy on the ECG is manifested by an increase in the pulse transit time, ischemic changes on the ECG, impaired impulse conduction, deviation of the axis to the hypertrophied area, a shift in the electrical position of the heart, and the location of the transition zone.
Treatment
If there is difficulty breathing, there is a desire to stop and catch your breath with the usual load, if there is pressure in the chest, or causeless weakness occurs, then you should consult a doctor.
The cardiologist will prescribe a complete clinical, biochemical and instrumental examination. Upon examination, specific heart murmurs and an increase in its boundaries may be detected. An X-ray examination will show how enlarged the heart is and in what parts. An echocardiogram will help determine the location of disorders and the degree of decrease in heart activity.
Once a diagnosis of left ventricular myocardial hypertrophy has been established, treatment depends on the degree of its severity and the severity of the patient’s general condition.
Changes in heart size are a consequence of other diseases. When treating a patient diagnosed with left ventricular hypertrophy, the causes that led to it are of primary importance.
Depending on the severity of the patient’s condition and how severe the left ventricular hypertrophy is, treatment can be carried out in a hospital or at home.
A prerequisite for successful treatment is a correct lifestyle. If this recommendation is ignored, any therapy is useless.
The diet reduces salt intake. Products that strengthen the heart muscle are recommended.
Constant monitoring of ECG and blood pressure levels and regular examination by a cardiologist are required.
If your condition is satisfactory, regular walks in the fresh air are good. Also, moderate left ventricular hypertrophy does not exclude race walking and swimming at a gentle pace. Excessive physical activity is avoided.
Medicines are taken throughout life. These are calcium channel blockers, beta blockers, antihypertensive drugs, metabolic cardiac medications.
In some cases, surgery may be recommended. During the operation, areas of thickened muscle are excised.
Phases
Five phases of development of PD can be clearly distinguished:
Rising (depolarization)
The occurrence of an action potential (AP) is associated with an increase in the permeability of the membrane for sodium ions (20 times compared to the permeability for K +, and 500 times compared to the initial permeability of Na +) and a subsequent increase in the diffusion of these ions along the concentration gradient into the cell, leads to a change (decrease) in membrane potential.
A decrease in membrane potential leads to an increase in membrane permeability to sodium by opening voltage-gated sodium channels, and an increase in permeability is accompanied by increased diffusion of sodium into the cytoplasm, which causes even more significant depolarization of the membrane. Due to the presence of positive feedback, depolarization of the membrane during excitation occurs with acceleration and the flow of sodium ions into the cell increases all the time. The intensity of the flow of potassium ions directed from the cell outwards in the first moments of excitation remains at the beginning. The increased flow of positively charged sodium ions into the cell first causes the disappearance of excess negative charge on the inner surface of the membrane, and then leads to recharging of the membrane. The influx of sodium ions occurs until the inner surface of the membrane acquires a positive charge sufficient to balance the sodium concentration gradient and stop its further passage into the cell. The sodium occurrence of PD is confirmed by experiments with changes in the external and internal concentrations of this ion. It was shown that a tenfold change in the concentration of sodium ions in the external or internal environment of the cell corresponds to a change in PD of 58 mV. When sodium ions were completely removed from the fluid surrounding the cell, PD did not occur. Thus, it has been established that AP occurs as a result of excess, compared to rest, diffusion of sodium ions from the surrounding fluid into the cell. The period during which the membrane permeability for sodium ions increases when sodium channels open is short (0.5-1 ms), followed by an increase in membrane permeability for potassium ions due to the opening of voltage-dependent potassium channels, and, consequently, increased diffusion these ions out of the cell. The “all or nothing” principle According to the “all-or-nothing” law, the cell membrane of an excitable tissue either does not respond to the stimulus at all, or responds with the maximum force possible for it at the moment. The action of the stimulus usually leads to local depolarization of the membrane. This causes the opening of sodium channels, which are sensitive to changes in potential, and through this increases sodium conductance, which leads to even greater depolarization. The existence of such feedback ensures regenerative (renewable) depolarization of the cell membrane. The magnitude of the action potential depends on the strength of the stimulus, and it occurs only when depolarization exceeds a certain limiting level specific for each cell. This phenomenon is called “all or nothing.” However, if depolarization is 50-75% of the limiting value, then a local response may occur in the cell, the amplitude of which is significantly lower than the amplitude of the action potential. The absence of an action potential at the pidboundary level of depolarization is explained by the fact that sodium permeability does not increase sufficiently to cause regenerative depolarization. The level of depolarization that occurs does not cause the opening of new sodium channels, so sodium conductance quickly decreases, and the resting potential in the cell is again established.
Overshoot
Depolarization of the membrane leads to a reversal of the membrane potential (the MP becomes positive).
In the overshoot phase, the Na + current begins to rapidly decrease, which is associated with the inactivation of voltage-dependent Na + channels (the open state time is milliseconds) and the disappearance of the electrochemical Na + gradient. Refractoriness One of the consequences of the disappearance of the Na + gradient is refractoriness - a temporary inability to respond to a stimulus. If the stimulus occurs immediately after the passage of the action potential, then excitability will not occur either with a stimulus strength at the threshold level or with a significantly stronger stimulus. This state of complete inexcitability is called the absolute refractory period. This is followed by a relative refractory period, when a suprathreshold stimulus can cause an action potential with a significantly lower amplitude than normal. An action potential of the usual amplitude under the action of a threshold stimulus can be evoked only after a few milliseconds after the preliminary action potential. The absolute refractory period limits the maximum frequency of generation of action potentials.
Repolarization
An increase in the potassium ion flow directed outward from the cell leads to a decrease in the membrane potential, which in turn causes a decrease in the permeability of the membrane to sodium ions, which, as indicated, is a function of the membrane potential. Thus, the second stage is characterized by the fact that the flow of potassium ions from the cell outward increases, and the counter flow of sodium ions decreases. This membrane repolarization continues until the resting potential is restored—membrane repolarization. After this, the permeability to potassium ions also drops to its original value. Due to the positively charged potassium ions released into the environment, the outer surface of the membrane again acquires a positive potential relative to the internal one.
Trace depolarization and hyperpolarization
In the final phase, the restoration of the resting membrane potential slows down, and trace reactions are recorded in the form of trace depolarization and hyperpolarization, due to the slow restoration of the initial permeability for K + ions.
What is cardiac repolarization
Each cardiomyocyte has its own membrane, which separates the space inside the cell from the space outside the cell. The potential difference that arises between the internal and external environment is usually called the membrane potential. If the cell is at rest. It is also called resting potential. When a cell is in an excited state, it is called an action potential.
The resting potential is observed at a certain constant concentration of electrolytes inside and outside the cardiomyocyte. When electrolytes begin to move across the cell membrane, the processes of depolarization and repolarization of heart cells begin.
Spreading
Spread into unmyelinated fibers
In unmyelinated (without pulp) nerve fibers, the AP spreads from point to point, since excitation can be registered as one that gradually “runs” along the entire fiber from its point of origin. Sodium ions entering the excited area serve as a source of electric current for the occurrence of AP in adjacent areas. In this case, the impulse occurs between the depolarized section of the membrane and its non-excited section. The potential difference here is many times higher than necessary for membrane depolarization to reach the maximum level. The speed of pulse propagation in such fibers is 0.5-2 m/s
Spread in myelinated fibers
The nerve processes of most somatic nerves are myelinated.
Only very small areas of them, the so-called node interception (interception of Ranvier), are covered with a normal cell membrane. Such nerve fibers are characterized by the fact that voltage-dependent ion channels are located on the membrane only at the interceptions. In addition, this shell increases the electrical resistance of the membrane. Therefore, when the membrane potential shifts, the current passes through the membrane of the intercepting area, that is, by jumping (saltatory) from one interception to another, which allows you to increase the speed of the nerve impulse, which ranges from 5 to 120 m/s. Moreover, the action potential that arose in one of the nodes of Ranvier causes action potentials in neighboring nodes due to the emergence of an electric field, which causes an initial depolarization in these nodes. The parameters of the EMF field and the distance of its effective action depend on the cable properties of the axon. Types of nerve fibers, impulse conduction speed, depending on myelination
| Type | Diameter (µm) | Myelination | Conduction speed (m/s) | Functional purpose |
| A alpha | 12-20 | strong | 70-120 | Mobile fibers of the somatic NS; proprioceptor sensory fibers |
| A beta | 5-12 | strong | 30-70 | Sensory fibers of skin receptors |
| A gamma | 3-16 | strong | 15-30 | Sensory fibers of proprioceptors |
| A delta | 2-5 | strong | 12-30 | Sensitive fibers of thermoreceptors, nociceptors |
| IN | 1-3 | weak | 3-15 | Preganglionic fibers of the sympathetic nervous system |
| WITH | 0,3-1,3 | absent | 0,5-2,3 | Postganglionic fibers of the sympathetic nervous system; sensory fibers of thermoreceptors, nociceptors of some mechanoreceptors |
What happens during depolarization?
What does such an indicator as the critical level of depolarization mean? In physiology, this means that the nerve cells are already ready to work. The proper functioning of the entire organ depends on the normal, timely change of phases of the action potential.
The critical level (CLL) is approximately 40–50 MV. At this time, the electric field around the membrane decreases. The degree of polarization directly depends on how many sodium channels in the cell are open. The cell at this time is not yet ready to respond, but collects electrical potential. This period is called absolute refractoriness. The phase lasts only 0.004 s in nerve cells, and in cardiomyocytes - 0.004 s.
After passing a critical level of depolarization, superexcitability occurs. Nerve cells can respond even to the action of a subthreshold stimulus, that is, a relatively weak influence of the environment.
Action potential propagation between cells
At a chemical synapse, after the action potential wave reaches the nerve terminal, it causes the release of neurotransmitters from the presynaptic vesicles into the synaptic cleft. Transmitter molecules released from the presynapse bind to receptors on the postsynaptic membrane, resulting in the opening of ion channels in the receptor macromolecules. Ions begin to enter the postsynaptic cell through open channels, change the charge of its membrane, which leads to partial depolarization of the membrane and, as a consequence, provoking the generation of an action potential in the postsynaptic cell.
In the electrical synapse there is no “mediator” of transmission in the form of a neurotransmitter. But the cells are connected to each other using specific protein tunnels - conexons, so ionic currents from the presynaptic cell can stimulate the postsynaptic cell, causing the generation of an action potential in it. Thanks to this structure, the action potential can propagate in both directions and much faster than through a chemical synapse.
- Scheme of the process of nerve signal transmission at a chemical synapse
- Diagram of the structure of an electrical synapse
Action potential in different cell types
Action potential in muscle tissue
The action potential in skeletal muscle cells is similar to the action potential in neurons. Their resting potential is typically -90 mV, which is less than the resting potential of typical neurons. The action potential of muscle cells lasts approximately 2–4 ms, the absolute refractory period is approximately 1–3 ms, and the conduction velocity along the muscle is approximately 5 m/s.
Action potential in cardiac tissue
The action potential of the cells of the working myocardium consists of a phase of rapid depolarization, an initial rapid repolarization, which turns into a phase of slow repolarization (plateau phase), and a phase of rapid final repolarization. The phase of rapid depolarization is caused by a sharp increase in the permeability of the membrane for sodium ions, causes a rapid incoming sodium current, when the membrane potential reaches 30-40 mV it is inactivated and subsequently the calcium ion current plays a major role. Depolarization of the membrane causes activation of calcium channels, resulting in an additional depolarizing incoming calcium current.
The action potential in cardiac tissue plays an important role in coordinating cardiac contractions.
Causes
The exact cause of disturbances in repolarization processes is unknown. Pathology can develop under the following conditions:
- Autonomic dysregulation syndrome – better known as vegetative-vascular dystonia;
- organic heart diseases - coronary disease, myocarditis, heart failure, cardiosclerosis, cardiomyopathies, thickening of the interventricular septum;
- the use of drugs that affect the excitability or metabolism of myocardial cells - antidepressants, adrenergic agonists, psychostimulants, cardiac glycosides;
- connective tissue dysplasia is a hereditary pathology characterized by insufficient production of collagen protein and manifested by joint hypermobility, increased skin extensibility, and impaired metabolic processes in the myocardium;
- changes in the blood levels of electrolytes - sodium, potassium, calcium, magnesium;
- Excessive physical activity – SIRD is common among athletes.
Molecular mechanisms of action potential generation
The active properties of the membrane that ensure the occurrence of an action potential, based mainly on the behavior of voltage-gated sodium (Na +) and potassium (K +) channels. The initial phase of AP is formed by the input sodium current, later potassium channels open and the output K + -current returns the membrane potential to the initial level. The initial ion concentration is then restored by the sodium-potassium pump.
During the PD, channels pass from state to state: in Na + channels there are three main states - closed, open and inactivated (in reality everything is more complicated, but these three states are enough for description), in K + channels there are two - closed and open.
The behavior of the channels involved in the formation of PD is described in terms of conductivity and calculated through transfer coefficients.
Carryover coefficients were derived by Alan Lloyd Hodgkin and Andrew Huxley.
Conductivity for potassium GK per unit area
| , |
| Where: |
| an — Transfer coefficient from closed to open state for K+ channels [1/s]; |
| bn — Transfer coefficient from open to closed state for K+ channels [1/s]; |
| n — Fraction of K+ channels in the open state; |
| (1 - n) - Fraction of K + channels in the closed state |
The conductivity for sodium G Na per unit area
is more difficult to calculate, since, as already mentioned, in voltage-dependent Na + channels, in addition to the closed / open states, the transition between which is a parameter, there are also inactivated / not inactivated states, the transition between which is described through a parameter
| , | , |
| Where: | Where: |
| am — Transfer coefficient from closed to open state for Na + channels [1/s]; | ah — Transfer coefficient from inactivated to non-inactivated state for Na + channels [1/s]; |
| bm — Transfer coefficient from open to closed state for Na + channels [1 / s]; | bh — Transfer coefficient from non-inactivated to inactivated state for Na + channels [1 / s]; |
| m — Fraction of Na + channels in the open state; | h — Fraction of Na + channels in a non-inactivated state; |
| (1 - m) - Fraction of Na + channels in the closed state | (1 - h) - Fraction of Na + channels in the inactivated state. |
Story
The main provisions of the membrane theory of excitation were formulated by the German neurophysiologist Yu. Bernstein
In 1902, Julius Bernstein put forward a hypothesis according to which the cell membrane allows K+ ions into the cell, and they accumulate in the cytoplasm. The calculation of the resting potential value using the Nernst equation for the potassium electrode satisfactorily coincided with the measured potential between the muscle sarcoplasm and the environment, which was about -70 mV. According to the theory of Yu. Bernstein, when a cell is excited, its membrane is damaged, and K + ions leave the cell along a concentration gradient until the membrane potential becomes zero. The membrane then restores its integrity and the potential returns to the resting potential level.
This model was developed in their 1952 work by Alan Lloyd Hodgkin and Andrew Huxley, in which they described the electrical mechanisms responsible for the generation and transmission of a nerve signal in the squid giant axon. For this, the authors of the model received the Nobel Prize in Physiology or Medicine for 1963. The model is called the Hodgkin-Huxley model
In 2005, Thomas Heimburg and Andrew D. Jackson proposed the soliton model, based on the assumption that the signal propagates through neurons in the form of solitons - stable waves propagating along the cell membrane.
The effect of certain substances on the action potential
Some substances of organic or synthetic origin can block the formation or passage of PD:
- Batrachotoxin has been found in some representatives of the leaf climber genus. Sustainably and irreversibly increases the permeability of membranes to sodium ions.
- Poneratoxin was found in ants of the genus Paraponera. Blocks sodium channels.
- Tetrodotoxin was found in the tissues of fish of the Skelezubovi family, from which the Japanese delicacy Fugu is prepared. Blocks sodium channels.
- The mechanism of action of most anesthetics (Procaine, Lidocaine) is based on blocking sodium channels and, accordingly, blocking the conduction of impulses along sensitive nerve fibers.
- 4-Aminopyridine - reversely blocks potassium channels, prolongs the duration of the action potential. Can be used in the treatment of multiple sclerosis.
- ADWX 1 - reversely blocks potassium channels. Under experimental conditions, it alleviated the course of acute disseminated encephalomyelitis in rats.