5 / 5 ( 1 voice )
What is cardiac asystole, what factors develop it in the rapid pace of a person’s life, what are the probable signs of pathology and how to eliminate them so that clinical death does not occur, many people with and without heart problems want to know. These questions can be answered in our article, where we will talk in detail about the signs of asystole and therapeutic methods to eliminate it.
So, cardiac asystole is, according to ICD-10 code, cardiac arrest when both mechanical and electrical activity of the ventricles - the lower cardiac cavities - ceases. The development of asystole occurs due to prolonged disturbances in heart rhythm or suddenly. The pathology is caused by cardinal factors - severe heart damage, and non-cardiac factors - circulatory disorders.
With asystole, the bioelectrical activity of the heart stops
Pathophysiology
Asystole is divided into primary and secondary. Primary asystole occurs when the bioelectrical system within the heart is unable to depolarize the ventricles. Which may result from ischemia or dysfunction of the sinoatrial node or atrioventricular (AV node) conduction system. Primary asystole is usually preceded by bradydrythmia resulting from sinus node block, complete heart block, or both.
The cause of asystole may be the consequences of ophthalmic surgery, retrobulbar block, eye trauma, direct pressure, maxillofacial surgery, carotid artery syndrome or neuralgia of the glossopharyngeal nerve (glossopharyngeal neuralgia). Episodes of asystole and bradycardia have been documented as manifestations of partial lesions of the left temporal lobe. Patients experienced either dizziness or fainting and loss of consciousness. Sudden death has not been reported, but it is possible if asystole persists.
Secondary asystole occurs when factors outside the cardiac conduction system cause loss of electrical depolarization. In this case, the end result is usually severe tissue hypoxia with metabolic acidosis. Asystole or bradysystole follows cases of ventricular fibrillation and usually occurs after defibrillation attempts have failed. This predicts a pessimistic outcome.
What are the clinical and physiological signs of the condition
The development of ventricular asystole is accompanied by classic symptoms of clinical death:
unconscious state (with sudden development, the person falls);- absence of pulsation in the carotid arteries;
- reaction of the pupil to light (pathological dilation).
- lack of breathing;
- decreased muscle tone;
The pathophysiological mechanisms of the development of symptoms are based on the absence of an electrical impulse, which causes a contraction of the myocardial muscle mass. Stopping blood circulation leads to disruption of the transport of glucose and oxygen to vital organs: lungs, brain and heart.
Due to metabolic changes, the control of the nervous system (central and autonomic) over conscious activity, involuntary breathing and heartbeat is disrupted.
The diagnostic algorithm for suspected asystole includes:
- checking the patient’s response to voice and visual images;
- measurement of pulse on the carotid arteries;
- checking for breathing;
- reaction of the pupil to light (at night a special flashlight is used).
The initial examination of a patient by a paramedic implies the preliminary exclusion of serious injury as the cause of clinical death.
The diagnosis of “asystole” is made according to electrocardiography data, which determines the isoline (a flat line, without teeth or other signs of activity of the conduction system of the heart).
Causes of asystole
Primary asystole
Primary asystole occurs when cellular metabolic functions are damaged and an electrical impulse cannot be generated. With severe ischemia, sinus node cells cannot transport the ions necessary to influence the transmembrane action potential. Failure of an implantable pacemaker can also cause primary asystole.
Proximal coronary occlusion of the right artery can lead to ischemic disease or infarction of both the sinoatrial and atrioventricular nodes. Extensive infarction may result in bilateral ventricular block (eg, intranodal complete heart block).
Idiopathic sinus or atrioventricular node degeneration can lead to sinus block and/or AV node block, respectively. This process occurs slowly and gradually progresses, but symptoms can be intense and asystole may occur. To control these diseases, an implantable pacemaker is usually required.
In some cases, sudden death can occur as a result of congenital heart disease, local manifestation of a tumor, or heart injury due to a contusion of the chest.
Asystole can occur after a direct current shock that disables the pacemaker. Heart rhythm may return spontaneously or after performing cardiopulmonary resuscitation (CPR). In such cases, patients can survive if emergency measures are taken immediately. Alternating current (AC) from artificial sources (generators) of electrical current typically causes ventricular fibrillation.
Derived asystole
Examples of diseases and conditions that can lead to derivative asystole include suffocation, drowning, stroke, massive pulmonary embolism, hyperkalemia, hypothermia, myocardial infarction, complications of ventricular fibrillation or ventricular tachycardia that progress to asystole, post-defibrillation, and sedative overdose or narcotic drugs leading to respiratory failure.
Hypothermia stands apart from these conditions because asystole can occur over a longer period of time and the patient can be saved by cardiopulmonary resuscitation. After which the majority of patients who survive are connected to a heart-lung machine.
Epidemiology
In Russia, according to official statistics, 35% of people die before retirement age. In 80% of cases, blood circulation stops as a result of ventricular fibrillation. In other cases, this occurs as a result of asystole.
Asystole in children
The prevalence of asystole in children is higher than in adults (25-56%). In fact, asystole in children is most likely usually secondary to another underlying noncardiac disease or condition (ie, respiratory retention due to sudden infant death syndrome [SIDS], infectious disease, suffocation, drowning, or poisoning). Infants are statistically more likely to suffer from cardiac arrest than older children.
Children suffering from ventricular fibrillation or ventricular tachycardia were statistically 4 times more likely to suffer cardiac arrest (20%) than patients with asystole (5%), and patients under 20 years of age had better survival than adults when cases of traumatic disorders were excluded .
The frequency of asystole as a percentage of all cases of cardiopulmonary diseases is higher in women than in men; but cardiac arrest itself, in general, as well as cardiovascular diseases, are more often observed in men (under 70 years of age).
Forecast
The prognosis of asystole depends on the etiology of the asystolic rhythm, the timing of medical intervention, and the success or failure of cardiac life support.
Resuscitation measures can only be successful if the primary cause of asystole can be immediately eliminated, for example, in case of cardiac arrest as a result of suffocation due to mechanical asphyxia (a person choked on food) and only if the respiratory tract is free for oxygen to enter. In selected cases, when primary asystole is caused by pacemaker failure (internal or external), support measures may be successful with immediate external stimulation.
As a rule, the prognosis for asystole is poor, regardless of its original cause.
Symptoms of right or left ventricular asystole, fibrillation
Even if cardiac arrest is sudden, in most patients it is preceded by such warning signs as:
- pain behind the sternum,
- rhythm disturbances,
- fainting states,
- frequent dizziness,
- labored breathing.
In other patients, asystole is the outcome of serious illnesses. In this case, a combination of cardiac and extracardiac pathology is often detected. Deterioration in health, in which cardiac arrest is likely, manifests itself:
- a drop in blood pressure;
- frequent and irregular heartbeat;
- increasing swelling;
- accumulation of fluid in the chest and abdominal cavity;
- pain syndrome;
- fever;
- breathing disorders - breaths become rare, short, convulsive, then weaken and stop.
Complications
Complications of asystole include chronic neurological disorders, complications resulting from cardiopulmonary resuscitation (CPR) or invasive surgical procedures (eg, liver injury, gastric/esophageal rupture, rib fractures, pneumothorax, pleural hemorrhage, air embolism, aspiration ). Death is common.
Direct diagnosis of asystole consists of detecting complete cardiac arrest and a confirmed rhythm in the form of a flat ECG line in two perpendicular leads. Asystole, when it follows a bradyarrhythmic rhythm, may be preceded by dizziness or fainting.
If in fact an asystolic rhythm is observed and it is present for more than a few seconds, the patient will not be conscious and will not respond to external stimuli (sound, light). Several agonal (ultimate, rare gasp) attempts to breathe may occur, but there are no heart sounds or palpable peripheral impulses. If asystole persists for 15 minutes or more, the brain is not supplied with oxygen and brain death occurs.
Possible consequences
Complications of asystole can occur for two reasons: due to the progression of the disease itself, and due to the resuscitation measures performed. The most dangerous consequences are the following:
- cerebral ischemia;
- rupture of internal organs;
- fracture of the ribs, which disrupts the integrity of the pleural cavity.
Even professional resuscitators, when carrying out the procedure for bringing a person back to life, often break his ribs - this happens due to the fragility of the bones and the need for strong pressure deep into a certain number of centimeters. And such complications also lead to the death of the patient.
Asystole is a very dangerous condition with a high probability of death. If signs of pathology appear, urgent hospitalization of the patient is necessary. And even with timely application of therapeutic measures, the patient’s prognosis for recovery is not great.
Diagnostics
Bradysystolic or asystolic blockade can be primary or derivative in a patient who has suffered a myocardial infarction. Conditions may also be associated with pacemaker failure directly as a result of decreased blood supply to the sinoatrial (SA) node or atrioventricular (AV) conduction system.
Many patients with myocardial infarction have some degree of autonomic dysfunction (ie, high parasympathetic tone), which occurs indirectly through bradyarrhythmia or heart block. There may also be a lack of sensitivity to sympathetic stimulation. Hypoxia from pulmonary edema or poor tissue perfusion from cardiogenic shock can also lead to secondary asystole.
Doctors consider drug toxicity and hypoxia in the differential diagnosis. Also note that electrocardiograph (ECG) misalignment can simulate asystole (re-check all electrode placements and check the patient's pulse).
Etiology
The heart rarely stops spontaneously. The causes of this phenomenon are varied - injuries, serious pathologies, infections, intoxications. All predisposing pathological conditions are divided into two groups.
Cardiac causes
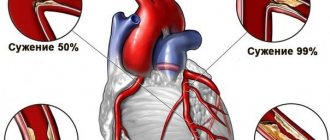
Primary asystole occurs against the background of complete well-being and the absence of heart rhythm disturbances. The main cause of the pathology is myocardial ischemia, which can be provoked by various negative factors:
- obesity,
- bad habits,
- hyperglycemia,
- hypertension,
- hypercholesterolemia.
The process is based on a violation of cellular metabolism and transport of ions necessary for the generation of an electrical impulse.
In addition to myocardial infarction, the following diseases can cause sudden death: congenital heart defects, neoplasms, traumatic injury to the chest. These pathologies are the cause of primary asystole associated with electrical instability of the myocardium itself against the background of oxygen starvation.
ischemia and subsequent myocardial infarction is a typically cardiac cause of sudden asystole due to the inability of the myocardium to contract
- Myocardial infarction is an acute nutritional disorder of the heart muscle caused by ongoing coronary insufficiency, atherosclerosis, and thromboembolism. The heart stops when the affected area becomes extensive - more than 25%. Cardiosclerosis and persistent heart failure are the immediate causes of asystole. Patients with myocardial infarction are prescribed lifelong maintenance therapy and constant monitoring of the condition.
- A decrease in circulating blood volume can cause sudden cardiac arrest. This is usually associated with bleeding as fluid leaves the bloodstream. Blood transfusion measures help save the lives of patients. In more rare cases, there is a decrease in the amount of circulating blood while maintaining its nominal volume. The causes of such changes are serious pathologies - heart valve defects and aortic diseases, in which the blood is not completely released into the systemic circulation. Transfusions in such a situation are pointless, since the problem is of organic origin.
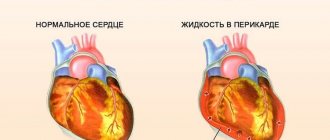
- Cardiac tamponade is a pathological condition caused by the accumulation of fluid between the layers of the pericardium and impairs the contractility of the myocardium. This is the result of injury, swelling, and inflammation. Treatment of the pathology is surgical.
- PE is the occlusion of a vessel by a thrombus that forms directly in the area of damage to the chest or migrates to the pulmonary trunk from distant foci through the systemic circulation. Spontaneous rupture of capillaries is possible under the influence of unfavorable factors - taking medications, blood diseases.
- An extreme degree of left ventricular failure , provoking a sharp decrease in heart rate - cardiogenic shock.
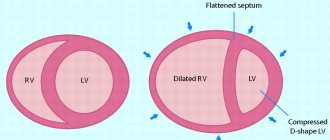
- Hypertrophic and dilated cardiomyopathy with changes in the shape of the heart and myocardial functions.
- Infectious endocarditis and myocarditis caused by viral infection, exposure to nonspecific bacteria, or having diphtheria etiology.
- Malignant hypertension and heart failure.
These conditions lead to a weakening of the pumping function of the heart and disruption of coronary circulation. Asystole is also a complication of coronary angiography, installation of catheters in the cardiac cavities, cardiac stimulation, and heart surgery.
Extracardiac causes
A wide variety of pathological processes lead to secondary asystole. It also develops in young people without damage to the myocardium.
- Pneumothorax is the penetration of air into the chest cavity and disruption of its tightness. It is this condition that is necessary for the adequate functioning of internal organs. Compression of the heart and lungs leads to disruption of hemodynamic processes and dysfunction of cardiovascular structures. The outcome of the pathology depends on the volume of air penetrated.
- Oxygen deficiency in tissues disrupts gas exchange. A severe degree of hypoxia, caused by severe heart or lung disease, often leads to asystole. To restore the functioning of the affected organs, it is necessary to carry out resuscitation measures.
- Electrical trauma disrupts the normal rhythm of the heart - the generation of impulses, their conduction and contraction of muscle fibers. Chaotic excitement sooner or later ends in cardiac arrest. After spontaneous and short-term contraction of the ventricles, asystole occurs.
- Acidosis - a biochemical deviation, which is an increase in the acid level of the blood. This result of metabolic disorders leads to a terrible phenomenon.
- Intoxication of the body , which occurs after taking certain medications, bites of poisonous insects, or penetration of heavy metal salts, leads to disruption of cellular respiration and the development of acute myocardial ischemia. The heart gradually loses its activity. It is unable to withstand negative external influences.
- Asystole may occur in a person with severe hypothermia . A body temperature of 35 degrees or below is considered critical and deadly.
- Hyperkalemia is a serious metabolic disorder not associated with eating habits. In healthy people, excess microelement is eliminated naturally.
- Hyperglycemia and hypoglycemia are common causes of cardiac arrest. A drop in blood sugar levels is especially dangerous - there is little time left for resuscitation.
- Impaired renal function in the decompensation stage and liver failure resulting from cirrhosis or cancer pathology usually result in multiple organ dysfunction and asystole.
- Malignant neoplasms and oncohematological diseases , accompanied by many metastases, lead to general intoxication of the body, destruction of affected organs and cardiac arrest.
In some cases, severe stress can lead to asystole, during which large amounts of adrenaline are released; sudden major stroke; intractable asthmatic attack; sepsis; protein diets; dehydration; asphyxia; shock of various origins - anaphylactic, traumatic or hemorrhagic. In addition to diseases, secondary asystole can be the result of injuries: obstruction of the respiratory organs by a foreign body, burns, extensive damage received in road accidents, man-made disasters, or at home.
The outcome of the pathology largely depends on the underlying process. Organic diseases have the worst prognosis.
Urgent Care
The mainstay of care in the intensive care unit is provided by oxygenation and mechanical ventilation through endotracheal intubation and circulation during cardiopulmonary resuscitation (CPR), attempts at percutaneous or transvenous stimulation, and administration of medications.
An example can be given of the successful resuscitation of a patient with asystole who had elevated serum potassium as a result of renal failure. Treatment consisted of calcium chloride to reverse the physiological effects of hyperkalemia and insulin and glucose to reduce serum potassium levels. However, this therapy cannot be recommended for all cases of asystole.
If rigor mortis is present, further resuscitation measures are stopped.
Electrical defibrillation
Electrical defibrillation should not be used indiscriminately on a patient in asystole. Which is not only ineffective, but also harmful in many cases, leading to the inability to restore the heart rhythm. One caution is that after defibrillation, brief false asystole may occur when defibrillator paddles are used.
Admission to the intensive care unit
The intensive care unit is the appropriate destination for a patient who has undergone bradysystolic cardiopulmonary heart block for further treatment and diagnosis. According to statistics over the past 10 years, patients who were in a stable bioelectrical and hemodynamic state, but were in a coma at temperatures up to 32-34 °C during the first day, showed an improvement in general neurological consequences.
Given that the prognosis for good neurological outcome with return of cardiac circulation is quite poor after cardiac arrest, attempting hypothermia in all adult patients with cardiac arrest, regardless of initial cardiac rhythm, is reasonable.
Prevention of asystole
Prevention of primary asystole in patients who have complete heart block or sinus node arrest may involve the correct use of a pacemaker. Prevention of secondary asystole requires early diagnosis, recognition and treatment of the underlying disease or condition.
Prehospital care
There are two medications recommended by the Association of Cardiology for use in adults for asystole: adrenaline and vasopressin. Atropine is not currently recommended for use in children. Even when taking high doses of atropine (0.03 mg/kg) and adrenaline (0.20 mg/kg) or using vasopressin 40 units, only in some cases do patients manage to avoid neurological disorders as a consequence of asystole.
Atropine is not recommended for preschool children with asystole, but they can be used for adult patients with pulsating electrical activity without a pulse.
Vasopressin
In cases where spontaneous circulation has not been restored, administration of intravenous vasopressin 40 U, followed by epinephrine at the discretion of the physician, may have some promising results.
Although more patients survived to hospital discharge with vasopressin than with epinephrine, there was a subsequent trend toward worse neurological outcome in those treated with vasopressin and epinephrine, with many in a persistent vegetative state.
In a study of 520 patients with asystole, 12 patients treated with vasopressin survived, while 4 patients in the standard treatment group survived.
In another comparative study comparing epinephrine alone and epinephrine plus vasopressin 40, physicians found that there were no significant differences between groups in return of spontaneous circulation, survival to hospital discharge, 1-year survival rate, or good neurological recovery among survivors. discharge from the hospital.
How does cardiac asystole appear on an ECG?
Cardiac asystole on the ECG is detected in the form of an almost straight line reflecting its electrical activity.
Characteristic signs of this condition also include abnormal atrial rhythm and the inability to count the frequency of their contractions when there are no ventricular contractions. In some cases, when the atria continue to contract for some time after the ventricles have stopped, atrial P waves can be detected on the cardiogram.
An auxiliary element for diagnosing asystole can be the arrhythmia preceding this condition. So, if it manifests itself in the form of early polytopic ventricular extrasystoles and ventricular tachycardia, then they will be followed by ventricular fibrillation and flutter, and increasing blockade usually indicates the approach of asystole.
Medications
The clinical benefits and parasympathetic effects on the heart of atropine during cardiopulmonary resuscitation have not been fully confirmed.
Atropine is not currently recommended by the Heart Association for asystole and pulseless electrical activity.
High doses of epinephrine (0.20 mg per kg) improve hemodynamics during cardiopulmonary resuscitation, thereby increasing the rate of return to spontaneous cardiac circulation; however, this drug did not demonstrate an effect on the final clinical outcome. Therefore, high doses are no longer recommended.
Studies have been carried out on the effects of adenosine receptor antagonists such as aminophylline, but there has been no evidence of clinical benefit.
Anticholinergics
The goal of anticholinergic drugs is to increase sinoatrial node activity and improve conduction through the SA node or atrioventricular (AV) node by decreasing vagal tone through muscarinic receptor blockade. This only works if the location of the block is within the SA or AV node. In patients with infranodal block, anticholinergic therapy is ineffective and may increase the second-degree Mobitz II block to a higher degree or third-degree block.
Atropine
Atropine is a parasympatholytic drug used to reverse the effects of the vagus nerve on the SA and AV nodes. This drug is not effective for third-degree infranadal heart block, PEA, and asystole.
Adrenergic agonists
Adrenergic drugs can cause constriction of skeletal and vascular muscles.
Epinephrine (adrenaline)
Adrenaline is considered the most effective drug for cardiac arrest; however, some doctors question its clinical effectiveness. This medication is used to increase coronary and cerebral blood flow during cardiopulmonary resuscitation and may increase automaticity during asystole. Adrenaline can also be used for bradycardia.
Vasopressin
Vasopressin has vasopressor and antidiuretic activity. This drug increases the process of water resorption on the distal renal tubular epithelium (ADH effect) and promotes smooth muscle contraction throughout the vascular bed by stimulating B1 receptors (vasopressor effect). Vasoconstriction (narrowing of the lumen of the vessel) increases in articular, coronary, cerebral, peripheral, pulmonary and intrahepatic vessels.
Recommendations for taking the drug while maintaining the cardiovascular system indicate a single dose of vasopressin in the amount of 40 units. as a treatment option for ventricular fibrillation and asystole. This drug may be given either before epinephrine or after the first dose of epinephrine.
Transcutaneous electrical stimulation
Transcutaneous electrical stimulation (TES), even when used urgently, does not increase the number of patients surviving after resuscitation measures. However, for example, in cardiac arrest preceded by conduction or impulse generation disorder (i.e., primary asystole), immediate use of TENS can save the patient's life.
(No Ratings Yet)