Home » Heart disease or cardiac disease » Heart failure: concept, forms, pathogenesis, manifestations
October 24, 2020 No comments
Heart failure is a severe pathological process that in some cases leads to death within a matter of hours (acute heart failure), and in others progresses over many years (chronic heart failure). This syndrome develops as a consequence of many diseases of the cardiovascular system and requires intensive complex treatment. In chronic heart failure, the five-year and ten-year survival rates are 50 and 10%, respectively, from the time of diagnosis.
Definition of the concept and classification
Heart failure is a condition characterized by a decrease in the reserve capacity of the heart.
This definition was proposed by professors V.A. Frolov, T.A. Kazanskoy, G.A. Drozdova and other employees of the Department of General Pathology and Pathological Physiology of the RUDN University on the basis of many years of research into this process. We believe that it is applicable to both acute and chronic heart failure and takes into account even those forms that in the initial stages occur only with a decrease in the functional reserves of the myocardium caused by certain types of functional load.
Diagnostics
Diagnosis of chronic heart failure involves the use of a set of methods aimed at timely detection of symptoms and immediate initiation of treatment.
First, doctors need to know the duration of symptoms. Emphasis is also placed on researching the family tree to find the possibility of a genetic predisposition to the disease. Important information is the possibility of patient contact with toxic substances, the use of various drugs, the presence of tumors or HIV infection.
Conducting urine and blood tests, as well as biochemical analysis, is aimed at determining the stage of chronic heart failure, cholesterol levels, and identifying the process of damage to internal organs.
When using diagnostic methods using ECG, MRI, echocardiography, phonocardiogram, specialists receive information about the degree of performance of the heart, the correct functioning of the valves, ventricles, wear and tear of the vascular system and muscles. When examining the structures and functions of internal organs, such as the kidneys and thyroid gland, doctors rule out the possibility that the development of chronic heart failure was the result of damage or deterioration in the functioning of internal organs.
Classification of heart failure
The classification of heart failure can be based on several different criteria.
I. According to the clinical course:
• Acute;
• chronic.
Acute heart failure is characterized by rapid development and increasing severity of hemodynamic disorders. It can lead to the death of the patient in a very short time (from a few minutes to several hours).
Chronic heart failure usually develops over many years and is characterized by alternating periods of exacerbation and periods of compensation.
II. According to cardiac output:
• with a reduced cardiac output - in most cases, heart failure is accompanied by a decrease in cardiac output due to a violation of the contractile activity of the left or right ventricles;
• with increased cardiac output - in case of certain diseases (thyrotoxicosis or beriberi disease), chronic heart failure, despite a decrease in myocardial contractile function, is characterized by an increase in cardiac output due to sinus tachycardia. It should be noted that this type of failure has a more unfavorable course, since in this case the energy resources of the myocardium are depleted very rapidly.
III. According to the part of the heart that is involved in the pathological process.
- left ventricular;
- right ventricular;
- total (both ventricles of the heart are in a state of failure).
IV. According to the etiopathogenetic principle:
- myocardial heart failure, which develops as a result of direct damage to the heart muscle (for example, with myocardial infarction, cardiomyopathies, myocarditis, etc.); overload heart failure - in this case, the pathological process is caused by a chronic significant increase in hemodynamic load, exceeding the ability of the corresponding part of the heart to overcome it (with arterial hypertension, heart defects);
- mixed form - develops, as a rule, in the later stages of overload heart failure, when myocardial damage occurs as a result of prolonged hemodynamic stress. In this case, the overload is also maintained.
Heart failure (HF) is a typical form of pathology of the cardiovascular system, characterized by the fact that the pumping function of the heart does not provide a level of systemic hemodynamics adequate to the metabolic needs of the body [uncompensated form of HF] or maintains it due to the implementation of pre-existing and/or newly formed compensatory mechanisms of the body [ compensated form of heart failure].
CHF. Clinic, diagnosis and treatment of biventricular heart failure. Prevention of CHF
HF is a pathophysiological symptom complex based on ↓ pumping function of the heart with normal venous return adequate to tissue needs.
Absolute – heartache
Relative – tissues require more (hyperthyroidism, pregnancy, anemia, hypoxia).
CHF is a SYNDROME characterized by weakness, shortness of breath, edema, caused by various pathological changes in the heart, leading to systolic and (or) diastolic dysfunction of the ventricular myocardium, manifested by both hemodynamic disorders and disorders of neuroendocrine regulation.
CHF of a bilateral nature, i.e. from the small side and BCC - biventricular HF, which is a diagnostic sign of dilated cardiomyopathy, in which the primary source is difficult to determine.
after myocarditis, CHF develops, often of a bilateral nature, i.e. from the small and large circles of blood circulation. This is biventricular heart failure, which is diagnostic of dilated cardiomyopathy, in which the primary source is difficult to determine.
Left ventricular failure is characterized by symptoms associated with stagnation in the pulmonary circulation: inspiratory shortness of breath during physical exertion, cough that worsens in a horizontal position, paroxysms of suffocation at night, orthopnea, moist rales during auscultation of the lower parts of the lungs, as well as a decrease in cardiac output: increased fatigue, decreased performance. Along with this, cardiomegaly is noted due to the left ventricle; a weakening of the 1st tone, a gallop rhythm, and an accent of the 2nd tone over the pulmonary trunk can be heard.
The skin is usually pale and cold to the touch due to peripheral vasoconstriction, and acrocyanosis is characteristic, associated with an increase in reduced hemoglobin in the venous part of the capillaries due to increased extraction of oxygen from venous blood. In severe heart failure there may be an alternating pulse.
On X-ray examination, in addition to enlargement of the left chambers of the heart, signs of pulmonary venous hypertension are observed: dilation of the upper lobe veins, perivascular and interstitial edema, and in severe cases, the presence of fluid in the alveoli. There may be pleural effusion, most often right-sided.
Echocardiography, Doppler echocardiography can reveal an increase in the size and volume of the left ventricle and left atrium, left ventricular hypertrophy, signs of segmental or diffuse impairment of its contractility, systolic and diastolic dysfunction, a decrease in ejection fraction and cardiac index. Radionuclide examination of the heart (ventriculography and myocardial scintigraphy) reveals a decrease in the ejection fraction of the left ventricle and regional disturbances in the movement of its walls.
Catheterization of the left ventricle and pulmonary artery characterizes changes in cardiac output, end-diastolic pressure and myocardial contractility. The use of ECG for diagnosing CHF is not very informative. With left ventricular failure, there may be signs of left ventricular and left atrium hypertrophy (P mitrale), decreased voltage, and impaired intraventricular conduction.
Right ventricular failure is characterized by hepatomegaly, edema, effusion in the pleural, abdominal and pericardial cavities, swelling and pulsation of the jugular veins, and high venous pressure. Pain in the right hypochondrium may occur due to stagnation of blood in the liver and an increase in its volume, loss of appetite, nausea, vomiting. Abnormal pulsation in the epigastric region can be detected, which can be caused by hypertrophy and dilatation of the right ventricle or pulsation of the liver with absolute or, more often, relative insufficiency tricuspid valve.
When pressure is applied to the liver area, the pressure in the jugular veins increases (jugular reflux, Plesch's symptom). Peripheral edema first appears in the evening and is localized on the feet, legs, and later covers the thighs and abdominal wall, lumbar region, up to anasarca.
Upon percussion, a displacement of the borders of the heart to the right is determined. X-ray and echocardiographic examination reveals an enlargement of the right ventricle and right atrium. The electrocardiogram may show signs of hypertrophy of the right ventricle and right atrium (Ppulmonale), blockade of the right bundle branch.
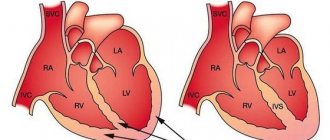
Biventricular heart failure is a combination of symptoms of left and right ventricular failure.
MAIN GOALS OF THERAPY FOR CHRONIC HEART FAILURE. 1. ↓LETHALITY, ↑life expectancy
2. ↓ CLINICAL SYMPTOMATICS - maintaining and improving quality of life
3. PREVENTION of the development of diseases leading to impaired cardiac function and the development of CHF (MI, hypertension, valvular heart disease, etc.).
- prevention of the progression of CHF in cases where there are already cardiac dysfunctions (↓myocardial ischemia, elimination of the toxic effects of alcohol, etc.).
Biventricular (total) heart failure develops when both ventricles are simultaneously affected by the pathological process (for example, with myocarditis) or when only the left parts of the heart are affected, which leads to a persistent increase in pressure in the left atrium, pulmonary hypertension and overload of the right ventricle with resistance and, in as a result, to right ventricular failure. In the latter case, chronic retention of Na + and water also plays a certain role. Regardless of which chamber of the heart experiences hemodynamic overload, biochemical changes in the myocardium characteristic of heart failure (depletion of norepinephrine, decreased activity of myosin ATPase, etc.) develop simultaneously in both ventricles. Left ventricular failure is the most common cause of right ventricular failure.
BASIC PRINCIPLES OF CHF TREATMENT - GENERAL MEASURES, DRUG THERAPY, TECHNICAL DEVICES, SURGICAL TREATMENT METHODS
GENERAL RECOMMENDATIONS: Advisory work: explaining to patients and their relatives what symptoms of CHF they need to pay attention to; the need for regular monitoring of body weight.
— Social activity and ability to work: social isolation is undesirable; social activity is encouraged as part of daily work, adapted to the patient’s physical capabilities.
— Travel: air transport is preferred (except for patients with NYHA class III and IV).
— Vaccination: vaccination against influenza and pneumococcal diseases is advisable.
— Contraception: 3-4 generation hormonal drugs and intrauterine devices are used to prevent pregnancy.
— Diet: (fighting excess weight, moderately limiting salt and liquid intake to 1-1.5 liters per day).
- To give up smoking.
— Alcohol: the amount should not exceed 40 g per day; in patients with alcoholic cardiomyopathy - complete refusal.
— Physical activity: moderate physical activity such as 20-30 minute walks 2 to 5 times a week is recommended.
— Rest: only for the period of occurrence of AHF, or worsening of CHF.
DRUG THERAPY ACE inhibitors and angiotensin II receptor antagonists, Diuretics, Beta-adrenergic receptor blockers, Cardiac glycosides, Peripheral vasodilators, Drugs with positive inotropic effects.
MAIN EFFECTS OF ACE INHIBITORS AND ARB-II IN CHF
1. ↑ LIFESPAN OF PATIENTS WITH CHF and ↓LETALITY
2. ↓ SEVERITY OF CLINICAL SYMPTOMS.
3. PREVENT THE PROGRESSION OF CHF.
DIURETICS 1. Thiazide diuretics: hydrochlorothiazide (hypothiazide)
2. Loop diuretics: furosemide (Lasix),
3. Potassium-sparing diuretics: spironolactones (veroshpiron)
PERIPHERAL VASODILATORS isosorbide dinitrate (nitrosorbide, isoket, isomac)
— ↓preload. With relatively preserved LV function and overload of the ICC.
Prevention: Equally important is the identification and elimination of some provoking factors - the direct causes of deterioration in the condition of patients with CHF. The most common of them include: non-compliance with medical recommendations (excessive consumption of salt, liquid, violation of the medication regimen, etc.); violation of individual physical/activity regime; infections; alcohol consumption; acute MI, unstable angina; TELA; transient disorders of electrolyte metabolism (hypokalemia, hypophosphatemia, hypocalcemia, etc.); pregnancy and childbirth; the occurrence of paroxysms or a permanent form of atrial fibrillation; thyroid dysfunction.
Iatrogenic factors are of great importance, in particular, taking medications that cause sodium and water retention (estrogens, androgens, chlorpropamide, glucocorticoids, minoxidil, NSAIDs, etc.) and having a negative inotropic effect (verapamil, diltiazem, some class I antiarrhythmic drugs, β-blockers in inappropriately large doses), inhibiting the formation of vasodilatory prostaglandins and endothelial factors (NSAIDs, glucocorticoids), excessive reduction of preload (large doses of diuretics, ACE inhibitors, etc.).
Pathogenesis
Acute heart failure
The cause of the development of acute heart failure is excessive hemodynamic overload of the myocardium. This occurs with severe damage to the heart muscle, for example, with a large-focal left ventricular infarction, accompanied by a sharp decrease in its contractile function.
Serious hemodynamic disorders occur. Overcoming the resulting overload of the heart muscle is possible only with a significant increase in the activity of intact myofibrils, which requires a significant increase in their energy supply.
Under these conditions, mitochondrial hyperfunction occurs. At the same time, the energy generated in them is almost completely spent on ensuring contractile activity, which allows the myofibrils to function in an enhanced mode for a certain period of time. However, as a result of mitochondrial hyperfunction, their damage and even destruction can occur, which obviously leads to an increase in energy deficiency in the myocardium and, as a consequence, to a weakening of protein synthesis, which is necessary, among other things, for the formation of new mitochondria.
Thus, the deepening energy deficit develops according to the principle of a vicious circle. Ultimately, energy exhaustion occurs, a sharp weakening of myocardial contractility up to fatal decompensation of cardiac activity.
Chronic heart failure
In chronic heart failure, the myocardium is exposed to a less pronounced pathogenic factor than in acute heart failure. Under these conditions, part of the energy generated in hyperfunctioning mitochondria can be spent to support protein synthesis processes. As a result, a very important sanogenetic mechanism is activated - the development of myocardial hypertrophy, which allows overcoming excess load for a long time.
At the same time, myocardial hypertrophy also contains significant pathogenetic potential, which begins to manifest itself especially sharply in the later stages of its development. The fact is that the development of hypertrophy is accompanied primarily by an increase in the mass of myofibrils (contractile elements experiencing hemodynamic overload), while the increase in the number of mitochondria and the mass of microvessels lags behind.
Thus, per unit myocardial mass, the number of mitochondria and the number of vessels in the hypertrophied myocardium become relatively smaller compared to the heart muscle of a healthy person. All this sooner or later leads to a deficiency of energy production, which becomes chronic. In the myocardium, the so-called wear complex of the hypertrophied heart develops, characterized by a deficiency (of oxygen, death of myofibrils, their replacement by elements of connective tissue, and a lack of mitochondria.
Complications
Complications of chronic heart failure can arise both during the natural development of the disease and as a result of the low effectiveness of the patient’s treatment. In the worst case, this can be fatal. Less bad complications include:
- heart rhythm failure;
- deterioration of throughput;
- organ enlargement;
- blood clot formation;
- liver dysfunction.
It is also cardiac cachexia, caused by decreased appetite, poor absorption of fats and increased metabolism. All this can lead to weight loss and the formation of ulcers on thinned skin.
Diastolic heart failure
It has been established that diastolic heart failure always includes diastolic dysfunction, but its presence does not indicate heart failure. Diastolic heart failure is diagnosed much less frequently than diastolic dysfunction, and is observed in no more than 1/3 of patients with CHF.
There are 3 stages of transition from diastolic dysfunction to diastolic heart failure. At the 1st stage, under the influence of various damaging agents (overload, ischemia, heart attack, left ventricular hypertrophy, etc.), the process of active relaxation of the myocardium and early filling of the left ventricle is disrupted, which at this stage is fully compensated by the activity of the left atrium, and therefore does not manifest itself even under load. The progression of the disease and an increase in the rigidity of the LV chamber is accompanied by a forced increase in LV filling pressure (the atrium can no longer cope!), especially noticeable during exercise. An even greater difficulty in blood flow to the left ventricle and a pathological increase in pressure in the pulmonary artery are observed, which reduces exercise tolerance (2nd stage). A further increase in LV filling pressure (3rd stage) completely “incapacitates” the left atrium; blood flow to the ventricle (blood outflow from the lungs) is critically reduced, which is accompanied by a drop in cardiac output, a sharp decrease in tolerance and congestion in the lungs, i.e., the formation of a detailed picture of CHF.
Thus, the transition from left ventricular diastolic dysfunction to diastolic heart failure is due to the classic development of congestion caused by a decrease in blood outflow from the lungs, a deterioration in the active relaxation of the myocardium and an increase in the stiffness of the LV chamber. The key to solving the problem is considered to be improving active relaxation and increasing the compliance of the left ventricular chamber.
Another feature of diastolic heart failure compared to the traditional (classical) variant of its development is a relatively better prognosis - the level of one-year mortality in the diastolic variant is approximately two times less than in “classical” systolic chronic heart failure. However, experts believe that such “well-being” is deceptive, since mortality from systolic CHF is constantly decreasing, and from diastolic heart failure remains at the same level from year to year, which can be explained by the lack of sufficiently effective treatments for patients with diastolic form of chronic heart failure.
When the pumping function of the ventricles of the heart deteriorates, an increase in preload can maintain cardiac output. As a result of this, remodeling of the left ventricle occurs over a long period of time: it becomes more elliptoid, expands and hypertrophies.
Although initially compensatory, these changes ultimately increase diastolic stiffness and wall tension (myocardial stress), impairing cardiac function, especially during exercise. Increased cardiac wall tension increases oxygen demand and accelerates apoptosis (programmed cell death) of myocardial cells.
Manifestations of hemodynamic disorders
Developed acute heart failure (or exacerbation of chronic) is characterized by a number of disturbances, first in intracardiac and then in systemic hemodynamics.
Tachycardia. This manifestation of heart failure occurs reflexively due to excessive stretching of the vena cava and plays a compensatory role: increased blood flow to organs and tissues is ensured by increasing cardiac output.
Increase in residual systolic volume of the heart . Residual systolic volume is the amount of blood that normally remains in the ventricles of the heart after the end of systole. Against the background of a decrease in myocardial contractility, the residual systolic volume increases in the cavity of the left (or right) ventricle.
Increased end-diastolic pressure . This indicator depends on the residual systolic volume. Obviously, an increase in this volume will be accompanied by an increase in end-diastolic pressure.
An important clinical criterion for assessing the state of contractile function of the left ventricle is the ejection fraction. Ejection fraction is a coefficient that reflects the proportion of left ventricular blood volume expelled into the aorta during each contraction (ratio of stroke volume to end-diastolic volume). Normally, the ejection fraction in an adult should be 55-75%.
Dilatation of the ventricles of the heart . Dilatation of the chambers of the heart develops as a result of an increase in systolic blood volume and an increase in end-diastolic pressure. There are two forms of dilatation of the ventricles of the heart: tonogenic and myogenic.
With tonogenic dilatation, the contractile and elastic properties of the myocardium are sufficiently preserved, which in this case obeys the Frank-Starling law, according to which the corresponding chamber of the heart contracts more effectively in systole, the more it stretches in diastole.
Myogenic dilatation is characterized by a sharp violation of this pattern due to a profound decrease in the elastic properties of the heart muscle. In this case, the myocardium begins to obey the Frank-Starling law to a much lesser extent.
Increased pressure in the veins through which blood is delivered directly to the decompensated part of the heart. Against the background of dilatation, when the corresponding ventricle of the heart does not provide the required volume of cardiac output, a sharp increase in pressure in the atria occurs. When the contractile activity of the left ventricle is decompensated, the pressure in the left atrium increases and, as a result, the pressure in the veins of the pulmonary circulation increases. With decompensation of the right ventricle, the pressure in the veins of the systemic circle increases accordingly.
Edema . Severe failure of the left ventricle of the heart can lead to pulmonary edema due to stagnation of blood in the pulmonary circulation. In addition, the development of general edema is possible, since a decrease in the release of blood into the aorta serves as a factor initiating the retention of sodium, and then water in the body. Right ventricular failure is accompanied by stagnation of blood in the systemic circulation, resulting in the development of peripheral edema. They begin to spread from below (from the feet) upward at a constant speed. Swelling of the subcutaneous tissue is more pronounced in the evening.
Hepatomegaly and liver failure . These manifestations are explained by venous congestion in the liver. Hepatomegaly is one of the early symptoms of right ventricular failure and precedes the development of edema. Prolonged venous hyperemia of the liver leads to irreversible morphological changes, which begin to impair its functional activity. Liver failure syndrome develops.
Cyanosis . This symptom occurs due to insufficient oxygenation of the blood and more intensive utilization of oxygen by tissues with weakened blood circulation.
Ascites . In the later stages of chronic heart failure, fluid containing protein may accumulate in the abdominal cavity. Ascites is one of the components of the general edematous syndrome, and the appearance of transudate in the abdominal cavity is explained by increased pressure in the peritoneal veins.
Hydrothorax . This symptom, which, like ascites, is one of the manifestations of the general edematous syndrome, can occur with both left and right ventricular heart failure. This is due to the fact that the veins of the visceral pleura belong to the pulmonary circulation, and the parietal veins belong to the large circle.
Cardiac cachexia . A sharp decrease in body weight and even exhaustion can be observed in the later stages of heart failure.
Firstly, when the heart is decompensated, it requires significantly more energy to overcome any load.
Secondly, with right ventricular failure, stagnation of blood in the systemic circle is accompanied by venous hyperemia of the intestine, leading to edema of its wall. Under these conditions, the process of absorption of nutrients is sharply disrupted.
About the operation
In most cases, CHF is associated with the pumping function of the heart.
The left ventricle acts as the main pumping chamber when it cannot contract with sufficient force, blood circulation is disrupted, the heart cannot contract normally and eject blood in order to provide the organs and tissues of the body with a sufficient amount of useful elements. In this case, both ventricles can contract almost simultaneously, or the contraction of the left ventricle or part of it is greatly delayed in relation to the right. To treat the disease, special pacemakers are used. Resynchronization therapy or biventricular stimulation is performed in patients with severe heart failure with a left ventricular ejection fraction of less than 35% that is not amenable to drug therapy. The purpose of the operation is to stimulate the ventricles from several points at once to restore simultaneous contraction and improve the pumping function of the heart.
A resynchronization device is a type of pacemaker. It consists of a generator and electrodes that are installed in the right atrium, right and left ventricles. When the ventricles contract out of sync, the device sends an electrical impulse, restoring their simultaneous rhythm. All indicators are sent from the pacemaker to the desktop computer of the institution where the implantation was performed. The doctor remotely monitors the operation of the device and the patient’s well-being. The battery of the device lasts up to 8 years of continuous operation. The pacemaker is then completely changed.
Two methods are used to perform SRT:
- endocardial - electrodes are installed into the heart cavity through a puncture (puncture) of the subclavian or brachiocephalic vein. The pacemaker is implanted under the skin in the chest area;
- epicardial – open heart surgery. It is performed less frequently due to anatomical conditions or other reasons. The electrodes are attached to the surface of the ventricles or to the surface of the endocardium (the inner lining of the heart).
Changes in respiratory system functions
In addition to hemodynamic disorders, changes in the functions of the respiratory system also appear in heart failure.
Shortness of breath . This symptom is caused by stagnation of blood in the pulmonary circulation, as well as impaired blood oxygenation.
Orthopnea . In case of heart failure, the patient takes a forced position of the body - sitting or lying with the head of the chair raised. This helps to reduce blood flow to the right side of the heart, resulting in a decrease in pressure in the pulmonary capillaries.
Cardiac asthma . Patients suffering from heart failure often experience attacks of shortness of breath and suffocation, mainly at night, accompanied by coughing with phlegm and bubbling breath.
Pulmonary heart
Cor pulmonale is a clinical syndrome in which there is an enlargement and expansion of the right chambers of the heart as a result of increased blood pressure in the pulmonary circulation due to chronic diseases of the lungs or bronchi.
According to the clinical course, cor pulmonale can be acute or chronic.
Acute cor pulmonale can be caused by two reasons. Firstly, this is an embolism of the pulmonary circulation, in which emboli block more than half of the pulmonary arteries (for example, with thromboembolism or pulmonary embolism). Secondly, massive thrombosis of the small capillaries in DIC syndrome can lead to the occurrence of this syndrome.
Chronic cor pulmonale develops as a result of a long-term increase in resistance in the pulmonary circulation, which accompanies various chronic lung diseases, including emphysema and broncho-obstructive diseases (chronic obstructive bronchitis, bronchial asthma, bronchopulmonary dysplasia, etc.).
These diseases are characterized, among other things, by the appearance of pneumosclerosis of varying severity. In chronic pulmonary heart disease, a combination of right ventricular and respiratory failure syndromes is observed. Against this background, combined (circulatory and respiratory) hypoxia occurs. Cor pulmonale does not respond to effective therapy. Nevertheless, treatment should, if possible, be aimed at correcting disorders caused by the underlying disease. Otherwise, it is symptomatic.
( 1 votes, average: 5.00 out of 5)
Indications for Biventricular pacemaker implantation
- Moderate to severe heart failure (HF). — The more pronounced the degree of heart failure, the better the results.
- QRS duration > 130ms. — Left bundle branch block or interventricular dissociation.
- Long-term drug therapy for heart failure, including the ineffectiveness of drug therapy.
During normal heart function, both ventricles of the heart work simultaneously with each other with a slight delay after the atria contract.
With CHF, many patients experience a disturbance in the conduction of excitation to the ventricles (bundle branch block or disturbance of intraventricular conduction). As a result, the left and right ventricles lose synchrony in their work.
Also, the walls of the left ventricle (responsible for delivering blood to the organs of the body) contract asynchronously, reducing the efficiency of the pumping function of the heart, and causing the blood to literally “splash” inside the chamber.
In such cases, the heart increases its rate of contraction to ensure that blood is delivered to the organs to meet the body's demand. This increases the load on the heart, which contributes to its premature exhaustion.
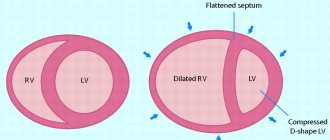
One of the manifestations is dysynchrony (asynchrony)
both ventricles of the heart,
which is caused by pathological changes in the myocardium:
Electric
: disturbance of intraventricular conduction.
Bundle branch block. Structural
: changes in the collagen matrix of the pathways.
Mechanical
: local myocardial asynchrony detected during stress - echocardiography.
to the top of the page