Pulmonary heart (cor pulmonale) is dilatation of the right ventricle secondary to lung diseases, which are accompanied by the development of pulmonary artery hypertension. Right ventricular failure develops. Clinical manifestations include peripheral edema, jugular venous distension, hepatomegaly, and sternal bulge. Diagnosis is made clinically and echocardiographically. Treatment involves eliminating the cause.
Cor pulmonale develops as a result of lung diseases. This condition does not include right ventricular (RV) dilatation secondary to left ventricular failure, congenital heart disease, or acquired valvular disease. Cor pulmonale is usually a chronic condition, but can be acute and reversible.
ICD-10 code
Acute cor pulmonale usually develops during massive pulmonary embolism or mechanical ventilation used for acute respiratory distress syndrome.
Chronic cor pulmonale usually develops with COPD (chronic bronchitis, emphysema), less often with extensive loss of lung tissue due to surgery or trauma, chronic pulmonary embolism, pulmonary veno-occlusive disease, scleroderma, interstitial pulmonary fibrosis, kyphoscoliosis, obesity with alveolar hypoventilation, nervous -muscular disorders involving the respiratory muscles, or idiopathic alveolar hypoventilation. In patients with COPD, a severe exacerbation or pulmonary infection can cause strain on the right ventricle. With chronic cor pulmonale, the risk of venous thromboembolism increases.
Lung diseases cause pulmonary arterial hypertension through several mechanisms:
- loss of capillary beds (eg, due to bullous changes in COPD or pulmonary thromboembolism);
- vasoconstriction caused by hypoxia, hypercapnia, or both;
- increased alveolar pressure (for example, with COPD, during artificial ventilation);
- hypertrophy of the middle layer of the arteriolar wall (a common reaction to pulmonary arterial hypertension caused by other mechanisms).
Pulmonary hypertension increases right ventricular afterload, leading to the same cascade of events that occurs in heart failure, including increased end-diastolic and central venous pressure, ventricular hypertrophy, and dilatation. The load on the right ventricle may increase with increased blood viscosity due to hypoxia-induced polycythemia. Sometimes right ventricular failure leads to left ventricular pathology when the interventricular septum bulges into the left ventricular cavity and prevents filling of the left ventricle, thereby creating diastolic dysfunction.
The presence of clinical, laboratory and instrumental symptoms of chronic obstructive and other lung diseases indicated in the article “Pulmonary heart - Causes and pathogenesis” already suggests a diagnosis of chronic pulmonary heart disease.
Cor pulmonale is initially asymptomatic, although patients usually have significant manifestations of the underlying lung disease (eg, shortness of breath, fatigue on exercise). Later, as right ventricular pressure builds, physical symptoms typically include systolic pulsation in the sternum, a loud pulmonary component of the second heart sound (S2), and murmurs of tricuspid and pulmonary valve insufficiency. Later, the gallop rhythm of the right ventricle (III and IV heart sounds), intensifying with inspiration, swelling of the jugular veins (with a dominant wave a, if there is no blood regurgitation due to tricuspid valve insufficiency), hepatomegaly and edema of the lower extremities join.
Causes
Impaired pulmonary ventilation and the development of respiratory failure can be caused by various acute and chronic diseases of the bronchopulmonary system (bronchiectasis, pneumonia, atelectasis, cavernous cavities, disseminated processes in the lung, abscesses, etc.), central nervous system lesions, anemia, hypertension in the pulmonary circulation, vascular pathology of the lungs and heart, tumors of the lungs and mediastinum, etc. Respiratory failure is classified according to a number of characteristics: 1. According to pathogenesis (mechanism of occurrence): • parenchymal (hypoxemic, respiratory or pulmonary failure type I). Respiratory failure of the parenchymal type is characterized by a decrease in the content and partial pressure of oxygen in the arterial blood (hypoxemia), which is difficult to correct with oxygen therapy. The most common causes of this type of respiratory failure are pneumonia, respiratory distress syndrome (shock lung), and cardiogenic pulmonary edema. • ventilation (“pumping”, hypercapnic or type II respiratory failure). The leading manifestation of ventilation-type respiratory failure is an increase in the content and partial pressure of carbon dioxide in the arterial blood (hypercapnia). Hypoxemia is also present in the blood, but it responds well to oxygen therapy. The development of ventilation respiratory failure is observed with weakness of the respiratory muscles, mechanical defects in the muscular and rib cage of the chest, and disruption of the regulatory functions of the respiratory center. 2. By etiology (reasons): • obstructive. Respiratory failure of the obstructive type is observed when it is difficult for air to pass through the airways - the trachea and bronchi due to bronchospasm, inflammation of the bronchi (bronchitis), foreign bodies, stricture (narrowing) of the trachea and bronchi, compression of the bronchi and trachea by a tumor. In this case, the functionality of the external apparatus is affected breathing: full inhalation and especially exhalation are difficult, breathing frequency is limited. • restrictive (or restrictive). Respiratory failure of the restrictive (restrictive) type is characterized by a limitation in the ability of the lung tissue to expand and collapse and occurs with exudative pleurisy, pneumothorax, pneumosclerosis, adhesions in the pleural cavity, limited mobility of the rib frame, kyphoscoliosis. Respiratory failure in these conditions develops due to the limitation of the maximum possible depth of inspiration. • combined (mixed). Respiratory failure of the combined (mixed) type combines signs of obstructive and restrictive types with a predominance of one of them and develops with a long course of cardiopulmonary diseases. • hemodynamic. The cause of the development of hemodynamic respiratory failure can be circulatory disorders (for example, thromboembolism), leading to the inability to ventilate the blocked area of the lung. Right-to-left shunting of blood through a patent foramen ovale due to heart disease also leads to the development of hemodynamic-type respiratory failure. In this case, a mixture of venous and oxygenated arterial blood occurs. • diffuse. Respiratory failure of the diffuse type develops when the penetration of gases through the capillary-alveolar membrane of the lungs is impaired due to its pathological thickening. 3. According to the rate of growth of signs: • acute. Acute respiratory failure develops rapidly, within a few hours or minutes, is usually accompanied by hemodynamic disturbances and poses a danger to the lives of patients (emergency resuscitation and intensive care are required). The development of acute respiratory failure can be observed in patients suffering from a chronic form of DN during its exacerbation or decompensation. • chronic. The development of chronic respiratory failure can occur over several months and years, often gradually, with a gradual increase in symptoms; it can also be a consequence of incomplete recovery after acute DN. 4. In terms of blood gas composition: • compensated (blood gas composition is normal); • decompensated (presence of hypoxemia or hypercapnia of arterial blood). 5. According to the severity of symptoms of respiratory failure: • DN I degree – characterized by shortness of breath with moderate or significant exertion; • DN II degree – shortness of breath is observed with minor exertion, the involvement of compensatory mechanisms at rest is noted;
What's troubling?
The classification of pulmonary hypertension in COPD by N. R. Paleev successfully complements the classification of cor pulmonale by B. E. Votchal.
- In stage I (transient), an increase in pulmonary arterial pressure occurs during physical activity, often due to an exacerbation of the inflammatory process in the lungs or worsening bronchial obstruction.
- Stage II (stable) is characterized by the existence of pulmonary arterial hypertension at rest and without exacerbation of pulmonary pathology.
- At stage III, stable pulmonary hypertension is accompanied by circulatory failure.
An examination to diagnose cor pulmonale should be carried out in all patients who have at least one of the reasons for its possible development. Chest radiographs demonstrate right ventricular enlargement and proximal pulmonary artery dilatation with distal attenuation of the vascular pattern. ECG signs of right ventricular hypertrophy (eg, right axis deviation, QR wave in lead V, and dominant R wave in leads V1-V3) correlate well with the degree of pulmonary hypertension. However, because pulmonary hyperventilation and bullae in COPD lead to cardiac remodeling, physical examination, radiography, and ECG may be relatively insensitive. Cardiac imaging using echocardiography or radionuclide scanning is necessary to assess left and right ventricular function. Echocardiography helps assess right ventricular systolic pressure, but is often technically limited in pulmonary disease. Right heart catheterization may be required to confirm the diagnosis.
Read also: Acute arterial hypotension
Treatment
General aspects are given in the article: respiratory failure
Treatment for this condition depends on the cause that led to its development. In case of a foreign body or spasm of the glottis, a conicotomy is performed. For pneumothorax, the pleural cavity is sealed. In case of poisoning with hemic poisons, specific antidotes are used. For severe bronchospasm, glucocorticosteroids are used. If you are unsure of the cause of this condition, you should not do anything until emergency medical services arrive.
What needs to be examined?
This condition is difficult to treat. The main importance is to eliminate the cause, especially to reduce or slow the progression of hypoxia.
In the presence of peripheral edema, diuretics may be indicated, but they are effective only in the presence of simultaneous left ventricular failure and fluid overload of the lungs. Diuretics may worsen the condition, since even a small decrease in preload often worsens the manifestations of cor pulmonale. Pulmonary vasodilators (eg, hydralazine, calcium channel blockers, dinitrogen oxide, prostacyclin), which are effective in primary pulmonary hypertension, are not effective in cor pulmonale. Digoxin is effective only in the presence of concomitant left ventricular dysfunction. This drug should be prescribed with caution because patients with COPD are very sensitive to the effects of digoxin. In case of hypoxic cor pulmonale, it has been proposed to perform a venotomy, but the effect of reducing blood viscosity is unlikely to offset the negative consequences of reducing the volume of blood carrying oxygen, except in cases of significant polycythemia. In patients with chronic cor pulmonale, long-term use of anticoagulants reduces the risk of venous thromboembolism.
I28 Other pulmonary vascular diseases
I28.0 Arteriovenous fistula of the pulmonary vessels
I28.1 Pulmonary artery aneurysm
I28.8 Other specified pulmonary vascular diseases
I28.9 Pulmonary vascular disease, unspecified
Add a comment Cancel reply
List of classes
- Class I. A00-B99. Some infectious and parasitic diseases
Excludes: autoimmune disease (systemic) NOS (M35.9)
disease caused by the human immunodeficiency virus HIV (B20 - B24) congenital anomalies (malformations), deformations and chromosomal disorders (Q00 - Q99) neoplasms (C00 - D48) complications of pregnancy, childbirth and the postpartum period (O00 - O99) certain conditions arising in the perinatal period (P00 - P96) symptoms, signs and abnormalities identified during clinical and laboratory tests, not classified elsewhere (R00 - R99) trauma, poisoning and some other consequences of external causes (S00 - T98) endocrine diseases , eating disorders and metabolic disorders (E00 - E90).
Note. All neoplasms (both functionally active and inactive) are included in class II. The corresponding codes in this class (for example, E05.8, E07.0, E16-E31, E34.-) can, if necessary, be used as additional codes to identify functionally active neoplasms and ectopic endocrine tissue, as well as hyperfunction and hypofunction of the endocrine glands, associated with neoplasms and other disorders classified elsewhere.
Excluded: certain conditions arising in the perinatal period (P00 - P96), some infectious and parasitic diseases (A00 - B99), complications of pregnancy, childbirth and the puerperium (O00 - O99), congenital anomalies, deformities and chromosomal disorders (Q00 - Q99 ), diseases of the endocrine system, nutritional disorders and metabolic disorders (E00 - E90), injuries, poisoning and some other consequences of external causes (S00 - T98), neoplasms (C00 - D48), symptoms, signs and deviations from the norm identified in clinical and laboratory studies, not classified elsewhere (R00 - R99).
Read also: Severe arterial hypotension
Chapter IX Diseases of the circulatory system (I00-I99)
Excluded
: diseases of the endocrine system, nutritional disorders and metabolic disorders (E00-E90) congenital anomalies, deformations and chromosomal disorders (Q00-Q99) some infectious and parasitic diseases (A00-B99) neoplasms (C00-D48) complications of pregnancy, childbirth and postpartum period (O00-O99) certain conditions arising in the perinatal period (P00-P96) symptoms, signs and abnormalities identified during clinical and laboratory tests, not classified elsewhere (R00-R99) systemic connective tissue disorders (M30- M36) trauma, poisoning and some other consequences of external causes (S00-T98) transient cerebral ischemic attacks and related syndromes (G45.-)
This chapter contains the following blocks
: I00-I02 Acute rheumatic fever I05-I09 Chronic rheumatic heart diseases I10-I15 Hypertensive diseases I20-I25 Ischaemic heart diseases I26-I28 Pulmonary heart disease and diseases of pulmonary circulation I30-I52 Other forms of heart disease I60-I69 Cerebrovascular diseases I70 -I79 Diseases of arteries, arterioles and capillaries I80-I89 Diseases of veins, lymphatic vessels and lymph nodes, not elsewhere classified I95-I99 Other and unspecified disorders of the circulatory system
Links
Wikimedia Foundation. 2010.
See what “Acute respiratory failure” is in other dictionaries:
- ICD 10 N17.17. ICD 9 584584 DiseasesDB ... Wikipedia
Acute respiratory failure ICD 10 J96.96. ICD 9 518.81518.81 DiseasesDB ... Wikipedia
I Respiratory failure is a pathological condition in which the external respiratory system does not provide a normal blood gas composition, or it is provided only by increased work of breathing, manifested by shortness of breath. This definition is... ... Medical Encyclopedia
The human respiratory system is a set of organs that provide the function of external respiration (gas exchange between inhaled atmospheric air and blood circulating in the pulmonary circulation). Gas exchange takes place in the alveoli of the lungs,... ... Wikipedia
RESPIRATORY FAILURE
- honey Respiratory failure is a violation of gas exchange between the surrounding air and the circulating blood with the development of hypoxemia, which consists of 2 stages. Ventilation - exchange of gases between the environment and the lungs. Oxygenation intrapulmonary... ...Reference book on diseases
ENZYME DEFICIENCIES
- honey Syndromes of inborn errors of metabolism are rare, but have a significant impact on physical, intellectual, mental development and quality of life (for example, phenylketonuria, homocystinuria, glycogenosis, fragile syndromes ... ... Disease Reference
I Renal failure Renal failure is a pathological condition characterized by a violation of the renal regulation of the body's chemical homeostasis with partial or complete disruption of the formation and (or) excretion of urine. Pronounced P. n.... ... Medical encyclopedia
ICD 10 I ... Wikipedia
ICD 10 N17.17. N19.19. ICD 9 584 ... Wikipedia
Liver failure is a complex of symptoms characterized by a violation of one or more liver functions, resulting from damage to its parenchyma. Portosystemic or hepatic encephalopathy is a symptom complex of central nervous system disorders,... ... Wikipedia
Books
- Emergency care at the prehospital stage. Textbook, Lychev Valery Germanovich, Babushkin Igor Evgenievich, Andrienko Alexey Vladimirovich. The textbook is devoted to emergency therapy as an independent field of medicine. The most common urgent syndromes are described: acute respiratory failure, acute...
Respiratory failure
- disruption of gas exchange between the surrounding air and the circulating blood with the development of hypoxemia. Gas exchange consists of two stages. Ventilation is the exchange of gases between the environment and the lungs. Oxygenation - intrapulmonary gas exchange; venous blood releases CO2 and is saturated with O2.
Code according to the international classification of diseases ICD-10:
CHRONIC PULMONARY HEART
• Lesions of the bronchial tree and lung parenchyma: • COPD • Diffuse interstitial lung diseases: pneumoconiosis, silicosis, idiopathic pulmonary fibrosis, radiation fibrosis • Granulomatous diseases: pulmonary tuberculosis, sarcoidosis, eosinophilic granuloma • Bronchiectasis • Cystic fibrosis • Malignant tumors • Lung resection • Pulmonary pathology blood vessels: • Primary pulmonary hypertension • Damage to the pulmonary vessels in diffuse connective tissue diseases (rheumatoid arthritis, SLE) • Hemoglobinopathies • Parasitic lung diseases • Limitation of chest excursion: • Obesity (Pickwick's syndrome) • Kyphoscoliosis • Neuromuscular diseases • Thoracoplasty • Syndrome sleep apnea • Chronic hypoxia (for example, during prolonged stay at high altitude).
• Mechanisms of pulmonary hypertension • Hypoxia and acidosis. The vasoconstrictor effect of hypoxia is a strong stimulus for the development of pulmonary hypertension; it can be enhanced by acidosis, which also has a direct, although less pronounced effect on the pulmonary vessels. The most important aspect of hypoxic vasoconstriction is the possibility of reversal with increasing oxygen content in the inspired air • Obliteration or obstruction of the pulmonary vasculature is a less common mechanism of pulmonary hypertension, occurring in recurrent pulmonary embolism, primary pulmonary hypertension (a rare disease of unknown etiology) and pulmonary fibrosis . Significant obstruction of the pulmonary vascular bed can also occur with emphysema and lung surgery • Development of cor pulmonale • Each attack of pulmonary hypertension leads to a progressive increase in pressure that persists after the attack • Pulmonary hypertension causes hypertrophy of the SMCs of the pulmonary arteries, and then of the peripheral pulmonary vessels. As a result, the pulmonary vascular bed becomes more rigid and loses its ability to respond to changes in cardiac output • Changes in the vascular wall impair the functioning of the right ventricle, causing its hypertrophy and failure of the right heart (ie, cor pulmonale).
Pathomorphology
• Signs of the underlying disease (see.
) • Hypertrophied right atrium and ventricle with dilatation of cavities • Enlarged liver.
Clinical picture
depends on the underlying disease • Shortness of breath, fainting (especially during physical exertion) • Cyanosis • Swelling of the neck veins • Dry or productive cough • Accent of the second tone over the pulmonary artery • Chest pain (dilatation of the pulmonary artery, myocardial ischemia) • Crackles in the lungs • Hepatomegaly and ascites, sometimes peripheral edema.
Laboratory research
• Ht is often increased (secondary erythrocytosis) • p02 is decreased.
Special studies
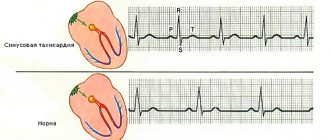
• ECG • Sinus tachycardia, possible atrial and ventricular extrasystole • Deviation of EOS to the right (angle a >[+110°]) • Right ventricular hypertrophy - most often with primary pulmonary hypertension • Right atrium hypertrophy - P-pulmonale (sawtooth wave P>2 .5 mm in standard leads II, III, aVF) • Complex Rs or rSR in lead V, • Ratio of the size of the r wave in v6 to the size of the S wave in V6 <1 • Appearance of flat or inverted T waves in the right chest leads • Decreased segment ST in leads II, III and aVF • Right bundle branch block (partial or complete) • Chest X-ray - signs of primary disease (often - saucer-shaped atelectasis, unilateral elevation of the diaphragm and minor pleural effusion), enlargement of the right atrium and ventricle, pulmonary artery • Echocardiography • Catheterization of the right heart - determination of pressure in the right ventricle and pulmonary artery in order to exclude congenital heart diseases as the cause of right ventricular failure.
Read also: Heart anatomy diagram
Lead tactics
• Outpatient mode. Regular oxygen inhalations are indicated (if possible at home) • Physical activity should not be limited • Moderate limitation of salt intake • Smoking cessation • Intensive antibiotic treatment of acute infectious diseases of the respiratory tract • Careful administration of drugs that reduce pulmonary ventilation (sedatives, tranquilizers, hypnotics), - only if there is an urgent need
heart failure • Phlebotomy to normalize Ht • Improvement of alveolar ventilation in COPD • Hydration • Bronchodilators • Oxygen inhalation. It should be taken into account that the only stimulator of the respiratory center in patients with severe hypercapnia is hypoxemia. Prolonged uncontrolled oxygen therapy, eliminating hypoxemia, causes a decrease in minute volume of respiration and increased hypercapnia • In advanced chronic cor pulmonale • Intravenous infusion of 1 -2 ml of cordiamine, 10 ml of 2.4% aminophylline solution, 1 ml of 0.025% strophanthin solution in 100-150 ml of 5% glucose solution • Intubation, mechanical ventilation, aspiration of sputum from the respiratory tract, intrabronchial administration of antibiotics, bronchodilators, glucocorticoids • Anticoagulants • Progestins • If indicated (long-term treatment, exclusion of anatomical dead space) - tracheostomy.
Drug therapy
• Drugs of choice • Bronchodilators, for example metapro-terenol (orciprenaline), albuterol (salbutamol), - every 6 hours or more often • Diuretics, for example furosemide • Vasodilators, for example hydralazine (apressin) nifedipine, diltiazem, prazosin - when lack of effect of conventional treatment methods. Efficacy is assessed only with invasive hemodynamic monitoring to reduce pulmonary vascular resistance by more than 20% with reduced or constant pulmonary artery pressure and increased or constant cardiac output. When administering these drugs, constant monitoring of blood pressure should be carried out to avoid severe arterial hypotension • Contraindications depend on the presence of the underlying disease; in all cases, the use of sedatives and drugs that depress the respiratory center should be avoided
Precautionary measures
. Constant monitoring of electrolyte levels is necessary when prescribing diuretins (especially ethacrynic acid), because increased excretion of potassium and chlorine ions can lead to metabolic alkalosis. • Alternative drugs. Digoxin 0.125-0.25 mg/day in the later stages - the effectiveness is questionable. Arrhythmias may occur as a result of electrolyte imbalance. Complication: hypercapnic coma. The course and prognosis depend on the underlying disease and the degree of pulmonary hypertension. 10-50% of patients live over 5 years (this figure increases with regular oxygen inhalation). In COPD with the development of cor pulmonale, mortality within 3 years reaches 30-50%. Pregnancy. Monitoring by a cardiologist is necessary (increasing load on the right ventricle). See also Chronic obstructive pulmonary diseases, Heart failure, Obesity, Bronchiectasis, Primary pulmonary hypertension, Secondary pulmonary hypertension
• 126.0 Pulmonary embolism with mention of acute cor pulmonale • 127.9 Pulmonary heart failure, unspecified
Primary ARF
Dysfunction of the external respiratory apparatus and its regulating systems
- 1. pain syndrome with suppression of external respiration (rib fracture, thoracotomy)
- 2. violation of the patency of the upper respiratory tract, bronchitis and bronchiolitis with hypersecretion of mucus and the development of obstructive atelectasis
- laryngeal edema
- foreign body
- aspiration
- massive bronchopneumonia
- electrical injury
- polio, tetanus, botulism