Minkowski-Choffard disease, hereditary spherocytosis and microspherocytic anemia are synonymous with the same pathology. This is a common disease that is transmitted to people only by inheritance. This complicates the issue of its prevention and protection from occurrence.
First, pathology was discovered by a Polish specialist in the field of physiology, Minkowski, and with the help of Shoffar, the data on the disease was supplemented. That’s why they named it after two scientists. An interesting fact is that the disease affects different ethnic groups, but it remains most common in European countries and especially in the northern part. There are no definite patterns regarding the time of onset of the first symptoms. Symptoms can occur at any age.
What is anemia?
Anemia is generally understood as a condition of the body characterized by a sharp decrease in red blood cells and hemoglobin. Some types of the disease cause changes in the shape of red blood cells. Over time, they lose their primary functions.
Anemia often accompanies various diseases, but is never primary. This is why the disorder should not be ignored. It is necessary to find its cause as quickly as possible and try to eliminate it.
Causes
The disease develops when pathological changes occur in the structure of red blood cells. Once the walls of blood cells lose their natural strength, they also lose their ability to hold hemoglobin. With anemia, a change in the shape of blood cells is also recorded, which does not allow them to penetrate small blood vessels. When trying to fulfill its purpose, the red blood cell is destroyed.
The pathology is associated with DNA damage as a result of exposure to negative factors during the child’s intrauterine development, but in most cases the cause is hereditary spherocytosis. The following can provoke a mutation in fetal genes:
- Exposure of a pregnant woman to radioactive and x-rays.
- A severe viral disease suffered by a woman while pregnant.
- Intoxication of the body of a pregnant woman with nicotine, narcotic substances or salts of heavy metals.
Inheritance of the disease occurs according to an autosomal dominant trait.
Features of hemolytic anemia
The concept of “hemolytic anemia” includes a wide group of diseases. All of them are characterized by a common pathogenesis. Increased destruction of red blood cells leads to an increase in their breakdown products and to an increase in erythropoiesis. The cycle of red cell formation is disrupted. The processes of their destruction gradually begin to prevail over the mechanisms of appearance and ripening.
All hemolytic anemias are conventionally divided into two groups: hereditary and acquired. In this article we will focus on the first option in more detail. To be more precise, let's look at what hereditary Minkowski-Choffard anemia is.
In medical reference books you can find several names describing the pathological process. These include microspherocytic anemia, hereditary spherocytosis, and Minkowski-Choffard disease. The latter name is most often used after the names of the pioneering scientists.
This disease is considered very common (1 case for every 5 thousand population). It is diagnosed mainly in residents of Northern Europe. The first signs become noticeable in children at an early age. If you do not start treating the disease in a timely manner, its course will negatively affect the functioning of the entire body.
How is hemolytic anemia treated in a child?
Treatment will depend on your child's symptoms, age and general health, and how advanced the illness is. The cause of the disease also matters.
A child with hemolytic anemia is often treated by a hematologist. He is an expert on blood problems. Some children do not need treatment.
Treatment includes:
| Blood transfusions |
| Medicines—corticosteroids or steroids |
| Intravenous immunoglobulin (IVIG) |
| Rituximab - a medicine to control the immune system |
| Antibiotics to treat infection if this is the underlying cause |
| Other medications depending on the type of hemolytic anemia |
Some children may also be prescribed:
- Splenectomy. This is an operation to remove the spleen.
- Immunosuppressive therapy. This is the use of other medications to control the immune system.
- Plasmapheresis. This is the removal of antibodies from the blood that destroy red blood cells.
- Stem cell transplantation. In severe cases, abnormal bone marrow cells are replaced with donated bone marrow.
Causes and mechanism of disease development
Minkowski-Choffar anemia is accompanied by a disruption of the structure and function of the erythrocyte cell membrane. As a result of the processes taking place, they change their shape to round and become fragile. The first signs of hemolysis appear - the destruction of red blood cells with the simultaneous release of hemoglobin.
In a healthy person, red blood cells are shaped like a biconcave disc, due to which they move freely through the vessels. With anemia in the membrane of these elements, protein synthesis is disrupted. This leads to the penetration of fluid into the cells. For this reason they change their shape. Passing through the vessels, red blood cells are greatly deformed, and after a while they begin to collapse. Against the background of the ongoing processes, the level of red blood elements drops sharply, and hemolytic anemia develops.
If one of the parents has already been diagnosed with this disease, it will certainly be inherited by the child. It is extremely rare that sick children are born to completely healthy mothers and fathers. In this case, anemia develops against the background of changes in DNA. The primary gene mutation occurs during fetal development. A prerequisite for the development of the disease is the impact on the mother’s body of the following factors:
- radiation, x-rays;
- intoxication with salts of heavy metals, narcotic substances, nicotine;
- virus attack.
Under the influence of these factors, not only Minkowski-Choffard anemia can occur, but also more serious pathologies. Therefore, during pregnancy, a woman should try to protect her body.
Possible complications and consequences
Timely diagnosis and treatment are the key to success
The prognosis for hereditary spherocytosis is most often favorable - with timely detection and proper treatment, the pathological process of destruction of red blood cells can be stopped. However, sometimes if medical care is untimely or incorrectly provided during a hemolytic crisis, there is a risk of death.
Considering that the pathology is inherited, there is a high risk of having a sick child. If one of the parents has a diagnosis, the newborn baby is immediately registered at the dispensary.
If a child develops hereditary spherocytosis in the absence of proper treatment, there is a risk of bone deformation, mental retardation, and disruption of the cardiovascular system.
First symptoms
The clinical picture is largely determined by the severity of the pathological process and the number of altered red blood cells. Its first symptoms can be observed in children of preschool and early school age. The course of this type of anemia is usually wavy. Attacks of a hemolytic crisis, when a large number of red blood cells are simultaneously destroyed, are followed by periods of calm. However, the symptoms may differ slightly.
For example, the interictal period of the disease is manifested by signs of anemia. Among them are the pallor of the skin, mucous membranes and sclera of the eyes. During a hemolytic crisis, the clinical picture changes and is accompanied by the following symptoms:
- Fever up to 38 degrees, headache, general malaise.
- Development of jaundice.
- Abdominal pain of a spasmodic nature.
- Discomfort in the liver area due to its enlargement.
- Inflammation of the spleen.
Hereditary hemolytic anemia of Minkowski-Choffard also occurs in adults. The most common reason for visiting a doctor in this case is jaundice of the skin. However, in most cases, this disease is asymptomatic. Patients learn about its existence by chance and usually during a routine examination.
Signs and symptoms of spherocytosis
During the period of exacerbation, attacks of cholecystitis may bother you
The disease is expressed depending on the level of healthy red blood cells: the more there are in the blood, the weaker the symptoms. The first signs of spherocytosis in a child are noticed in early childhood - usually in the preschool period or early school age. Spherocytosis has a wave-like course - with periods of remission and exacerbations; at an early stage it is characterized by an asymptomatic course.
During the interictal period, the patient’s condition is satisfactory, only signs of anemia are noted:
- jaundice,
- pale skin color,
- dizziness.
With the onset of a hemolytic crisis, an increase in symptoms appears:
- changes in the parameters of the liver and spleen - the organs protrude beyond the border of the ribs by 2 - 3 cm;
- decreased hemoglobin level;
- signs of cholecystitis with a rise in low-grade temperature, the appearance of stones in the gall bladder, pain in the right hypochondrium, white feces and darkened urine;
- general weakness, chronic fatigue, inability to move;
- migraine;
- spasmodic pain in the epigastric region;
- attacks of nausea, vomiting;
- The dark brown color of the stool is due to the content of a large amount of the pigment stercobilin.
Medical examination
Diagnosis of Minkowski-Choffard anemia is quite simple. If you suspect a disease and its initial signs appear, you should seek help from a doctor. Pathologies of the hematopoietic system are the responsibility of a hematologist. After studying the patient’s complaints and family history, the specialist must examine the skin and sclera and palpate the abdomen. An ultrasound scan of the liver and spleen is mandatory, since one of the symptoms of the disease is an increase in the size of these organs.
At the same time, the hematologist gives a referral for a number of laboratory tests. Minkowski-Choffard hemolytic anemia is confirmed if the following changes are present:
- Urine: hemoglobinuria, increased protein and urobilin levels.
- Blood biochemistry: decreased cholesterol, increased lactate dehydrogenase, increased indirect bilirubin.
- Examination of erythrocytes: pronounced reticulocytosis, reduction in cell size, decrease in their osmotic stability.
- Complete blood count: acceleration of ESR, slight decrease in platelets and leukocytes, reduction in color index.
Electrophoresis of erythrocyte membrane proteins in combination with their quantitative determination helps to definitively confirm the preliminary conclusion.
Diagnostics
Individuals suffering from hereditary spherocytosis usually have an enlarged spleen.
The diagnosis of Minkowski-Choffard disease is based on the presence of typical clinical signs in the patient in combination with morphological changes in red blood cells.
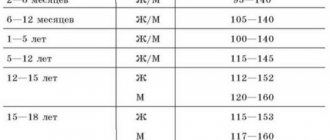
The severity of anemic syndrome with this pathology may vary. The hemoglobin level outside of a crisis often remains at the level of 100-110 g/l, and during a severe hemolytic crisis it drops to 40 g/l.
The severity of hemolysis depends on the total number of altered red blood cells (microspherocytes) in the population. Some people have large amounts of them. Therefore, during a crisis, the level of indirect bilirubin and reticulocytes in their blood increases sharply.
Characteristic features of red blood cells in hereditary spherocytosis are:
- microcytosis with normal average volume, decreased diameter and increased cell thickness;
- lack of central clearing in altered erythrocytes;
- decrease in osmotic resistance.
When studying the cellular composition of the bone marrow, its hyperplasia is revealed with an increase in the activity of the erythroid lineage of hematopoiesis.
It should be noted that individually, each of the manifestations of hereditary spherocytosis is not specific and can also occur in other diseases; only their combination allows us to assume the correct diagnosis. Therefore, such patients should be fully examined to exclude:
- chronic hepatitis;
- liver cirrhosis;
- other hemolytic anemias;
- dyserythropoietic anemia.
Differential diagnosis
Minkowski-Choffard hemolytic anemia in children sometimes causes difficulties during diagnosis. This disease has symptoms similar to other autoimmune pathologies. Therefore, doctors should know some distinctive and characteristic signs of this type of anemia.
First of all, we are talking about hereditary predisposition. Only in exceptional cases are both parents completely healthy. On the other hand, a sick child exhibits obvious changes in the bones of the skull. In doubtful cases, the Coombs test is additionally prescribed. If the test is negative, the patient is confirmed to have Minkowski-Choffard anemia. The diagnosis is considered complete at this point.
Symptoms of hemolytic anemia in a child
The most common symptoms of hemolytic anemia in children are:
- pale skin;
- jaundice, or yellowing of the skin and eyes;
- dark colored urine;
- fever;
- weakness;
- dizziness;
- confusion;
- intolerance to physical activity;
- enlarged spleen and liver;
- fast heartbeat;
- heart murmur.
Symptoms of hemolytic anemia may look like other health problems. Always consult a doctor when diagnosing your child's health condition.
Conservative treatment methods
Therapy for anemia is selected taking into account its severity. During the lull period, as a rule, no intervention is required. During the next attack, the patient is immediately hospitalized.
Conservative treatment of Minkowski-Choffard anemia includes the following measures:
- Red blood cell replacement therapy if the hemoglobin level in the blood drops to 70 g/l.
- Albumin treatment is prescribed for high bilirubin levels.
- Infusion therapy is used to detoxify the body.
- In the absence of a pronounced hemolytic crisis, the use of choleretic drugs is indicated.
The duration of such therapy, specific drugs and their dosage - all these issues are decided by the doctor on an individual basis.
Treatment of Minkowski-Choffard anemia
Depending on the severity of the disease, the methods of its medicinal correction will differ. During the period of remission of anemia, therapy is not carried out. During an exacerbation of the pathology, the patient must be hospitalized.
Treatment boils down to the following activities:
- When the hemoglobin level decreases to 70 g/l, the patient is transfused with red blood cells.
- If the level of bilirubin in the blood is high, the patient is given albumin.
- To remove intoxication from the body, the patient is given infusion therapy.
- Choleretic drugs can improve the patient’s well-being during a hemolytic crisis.
Severe Minkowski-Choffard anemia requires surgical intervention. To do this, the patient's spleen is removed. This will not make it possible to completely get rid of anemia, but the person’s condition improves, since the life cycle of red blood cells can be extended.
After removal of the spleen, the patient will no longer be at risk of hemolytic crises. However, this procedure is contraindicated under the age of 5 years, since splenectomy can be fatal in children. In addition, the absence of a spleen in the body contributes to a decrease in immunity. A person becomes susceptible to various infections.
Another surgical method for treating anemia is endovascular occlusion. This procedure is an alternative to splenectomy. During the procedure, the patient is given a drug that causes a splenic infarction. A certain part of it does not die, but continues to function, so the patient’s condition improves, but immunity does not decrease.
If the disease is mild and the patient receives high-quality and timely treatment, then the prognosis for life is favorable. Removing the spleen avoids crises. Without surgery, the average duration of remission between hemolytic crises is 2 years.
Surgery
If microspherocytic hemolytic anemia of Minkowski-Choffard occurs in a severe form, conservative treatment does not cope with the stated objectives, the patient is recommended to have surgery to remove the spleen. This approach does not completely cure the disease. On the other hand, after the intervention, the number of destroyed red blood cells is noticeably reduced, and their life cycle is extended.
Hemolytic crises do not recur after surgery, but it has a number of contraindications. For example, spleen removal is not recommended for children under 5 years of age due to the high postoperative mortality rate. The negative side of the procedure is considered to be a decrease in the body's resistance to viral and fungal infections.
An alternative option for removing the spleen is endovascular occlusion. This is another treatment method that is often used for the diagnosis of microspherocytic anemia of Minkowski-Choffard. During the procedure, the doctor injects a medicine into the organ, which provokes a spasm and leads to a splenic infarction. Some of it then retains a full blood supply and does not lose its ability to resist infections.
Pathogenesis
In the structure of the circulatory system, the main ones are leukocytes (protective cells) and erythrocytes (saturate organs with oxygen). In hereditary microspherocytosis, the membrane membrane of the erythrocyte does not contain the protein spectrin. Red cells affected by Minkowski-Choffard anemia do not mature; red blood cells die in the bone marrow or take on the shape of a sphere, becoming spherocytes. The body does not receive the necessary oxygen as the level of red cells decreases. Due to this, sick patients have weakened muscles and pale skin.
With a more severe form of anemia, the structure and structure of red blood cells changes, they become microspherocytes and die.
Spherocytes are absorbed by macrophages of the spleen, which certainly leads to its enlargement. The spleen is the main place where hemolysis occurs. According to studies, the red blood cells of a healthy person live 90-120 days, while in patients with Minkowski-Choffard anemia it is from 8 to 15. Increased destruction of red blood cells leads to an increase in bilirubin, which enters the bile in large quantities and leads to the appearance of stones. Alcohol consumption, poor diet, infections, and parasites complicate the course of the disease and lead to a hemolytic crisis.
Deficiency of spectrins in the erythrocyte membrane manifests itself in all patients without exception with hereditary spherocytosis, this leads to its excessive permeability to sodium ions, water accumulates in it, this creates an additional load and it acquires a spherical shape.
Red blood cell deficiencies are caused by genes, but due to provoking factors, these defects are aggravated and a hemolytic crisis occurs, which manifests itself:
- hypoglycemic and acidotic changes;
- hemodynamic disorders;
- hyperbilirubinemia;
- cerebral edema;
- hypoxia and anemia.
Possible complications
Minkowski-Choffard hemolytic anemia in preschool children often leads to retardation in mental and physical development. Especially if parents did not seek medical help for a long time or ignored the doctor’s recommendations.
In adult patients, the most common complication is cholelithiasis due to impaired bilirubin metabolism. The thing is that a hemolytic crisis is often perceived as the beginning of the development of obstructive jaundice, so proper treatment is delayed. In the presence of gallstones, cholecystectomy along with splenectomy is recommended.
Diagnosis of spherocytosis
Laboratory tests are an important part of diagnosis
Spherocytosis cannot always be recognized at an early stage, because the disease is often asymptomatic. Sometimes the only sign of the disease is pale skin and general weakness of the body. If these and other symptoms of spherocytosis begin to bother you, it is recommended to immediately consult a specialist. The doctor will collect anamnesis, examine the patient, and inquire about the presence of hereditary pathologies.
To make an accurate diagnosis, you cannot do without laboratory diagnostics:
- general blood test with detection of erythrocyte sedimentation rate, hemoglobin level, erythrocyte form;
- biochemistry with the exception of iron deficiency anemia and hyperbilirubinemia;
- method for determining the osmotic resistance of erythrocytes;
- bone marrow biopsy (in rare cases when it is difficult for a doctor to make a diagnosis or when there is insufficient information about the disease).
As a supplement, the doctor often prescribes an ultrasound of the internal organs and evaluates the parameters of the liver, spleen, and excludes the presence of stones in the gall bladder.
The most important indicator for spherocytosis is a decrease in the osmotic resistance of red blood cells. When a hemolytic crisis occurs, the number of reticulocytes (cells that precede red blood cells) increases, and normal red blood cells are visualized in the peripheral blood, although leukocytes and platelets are normal.
Note! In the presence of hereditary anemia, a blood smear reveals polychromasia and poikilocytosis, but there are few or no nucleated red blood cells.
Prevention methods
Minkowski-Choffar anemia is hereditary. Therefore, it is not possible to prevent the occurrence of the disease. In order to prevent severe forms of the disease, patients with an identified form of anemia are recommended to periodically undergo a complete examination by a hematologist.
When planning a pregnancy, you should understand that the probability of developing the disease in the unborn child is 50%. Therefore, the newborn is also indicated for constant monitoring by a doctor to identify pathology at an early stage.
Treatment
Treatment of hereditary spherocytosis is carried out depending on the clinical picture, the age of the patient and the frequency of crises. For mild forms of the disease, treatment consists of proper nutrition. The following products must be included in the diet:
- legumes;
- cottage cheese;
- liver;
- buckwheat;
- nuts;
- tomatoes;
- cabbage;
- corn;
- carrot;
- citrus;
- watermelons;
- asparagus.
More severe forms of Minkowski-Choffard anemia are treated in a hospital. Treatment is designed to reduce the risk of cerebral edema, eliminate hyperbilirubinemia, hypoxia and includes:
- transfusion of red blood cells;
- administration of prednisolone, carboxylase, vitamin C, B12 and glucose;
- after recovery from the crisis, a course of treatment with choleretic drugs is carried out.
If after treatment there is no reticulocyte reaction, the issue of surgical intervention and removal of the spleen (splenectomy) is decided. The operation is a last resort, but sometimes it is necessary to do it if there is a threat of serious changes in the pancreas and liver. A child can undergo this operation no earlier than 4-6 years of age. Children with Minkowski-Choffard anemia from infancy may have delays in mental, physical and sexual development.
Pregnant women (if necessary) undergo surgical intervention, since the progression of spherocytosis threatens complications with more serious consequences (cirrhosis, hepatitis, cholelithiasis). Immunoglobulin is used to treat pregnant women. In old age, a hemolytic crisis and, as a result, the death of the patient is possible.