© Author: Ilya Vitalievich Soldatenkov, general practitioner, especially for SosudInfo.ru (about the authors)
Ischemia of the lower extremities develops as a result of circulatory disorders in the body and poor blood supply to the parts of the body most distant from the heart - the legs. A deficiency of oxygen and nutrients delivered by arterial blood flow leads to serious consequences.
The main cause of ischemia is a local decrease in blood supply, caused by narrowing or obstruction of the lumen of blood vessels and leading to temporary dysfunction or permanent damage to tissues and organs. The distal parts of the legs—the feet and legs—are most susceptible to ischemia.
Insufficient blood flow to the lower extremities leads to rapid fatigue and muscle pain. In advanced cases, patients develop gangrene, in which drug therapy becomes ineffective. The extreme manifestation of ischemia is tissue necrosis. Only amputation of a limb can save the patient's life.
Classification of acute limb ischemia:
- Exertion ischemia is the appearance of signs of pathology during exercise.
- Ischemia degree I - preservation of sensitivity and movement in the affected limb, the appearance of numbness, coldness, paresthesia and pain.
- Ischemia of the second degree is a sensory disorder and limitation of active movements.
- III degree ischemia is the appearance of necrobiotic phenomena.
sequence of disease progression
Etiology
Causes of occlusion or narrowing of the vessels of the lower extremities, due to which ischemia occurs:
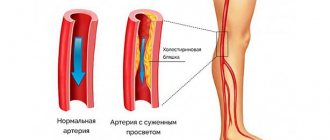
- In atherosclerosis, cholesterol plaques are located on the inner walls of the vessels of the legs and partially or completely block their lumen.
- With thrombosis, an artery is blocked by a formed blood clot; with embolism, the clot moves into the vessels of the lower extremities from other places.
- Endarteritis is characterized by inflammation of the arterial wall, leading to vessel spasm.
- In people with diabetes, the blood vessels in the legs are often damaged (diabetic foot syndrome).
- Injuries of large vessels.
Risk factors that provoke leg ischemia include: smoking, hypertension, hypercholesterolemia, atherosclerosis of other localizations, frostbite of the legs, excess weight.
The main links in the pathogenesis of limb ischemia:
- Stagnation of venous blood,
- Formation of tissue edema,
- Compression of weakly filled arteries,
- Deterioration of blood supply,
- Deficiency of oxygen and nutrients,
- The appearance of areas of necrosis,
- Formation of trophic ulcers,
- Inflammation of sensory nerves
- The occurrence of unbearable burning pain.
From the point of view of pathophysiology, acute ischemia is the result of a fixed narrowing of the lumen of blood vessels, impaired vascular tone, and atherosclerotic dysfunction of endothelial cells.
Staged course
- The initial stage is characterized by a minimum of symptoms: the unreasonable occurrence of fatigue in the legs with little physical activity (walking up to 1 km), the appearance of stabbing sensations and chilliness in the feet, the skin is cold and pale to the touch.
- At subsequent stages, more intense manifestations occur:
- pain in the legs with the inability to move at the usual speed (“intermittent claudication”), which occurs after covering a distance of 200 m;
- pallor of the skin of the legs, hair loss, decreased elasticity of the skin, and trophic lesions appear.
Chronic ischemia with severe vascular occlusion leads to:
- pain at rest or with minimal physical activity (inability to overcome 25 m);
- muscle transformations (atrophic phenomena and weakness);
- the appearance of cracks due to minor injuries, ulcers, in the nail plates of the toes - inflammatory processes (felons).
When the lumen is blocked in the upper parts of the abdominal aorta, there are necessarily signs of ischemia of the pelvic organs (disorder of stool, urination, dysfunction of the genital organs).
Symptoms
The main symptom of lower limb ischemia is intermittent claudication. Pain occurs when walking and is localized in the calf or gluteal muscles, lower back or hips. Most often, patients describe these sensations with the words “fetters”, “compresses”, “woodens”. To alleviate the condition, patients need to stop and stand still. The intensity of the pain will decrease, allowing you to continue your journey. Over time, the condition of patients worsens: the legs become cold and numb, the skin turns pale, the pulse in the legs disappears, the growth of nails slows down, and hair falls out. Against the background of chronic ischemia of the lower extremities, swelling of the lower legs and feet appears. Most men experience impaired potency and erectile dysfunction. In advanced cases, trophic changes appear on the skin - ulcers and areas of necrosis. Gangrene of the legs may develop, leading to amputation.
Degree of disease development:
- Weak vascular occlusion is manifested by a feeling of tingling and numbness in the legs, the appearance of pins and needles, pallor of the skin of the legs and increased sweating.
- The main symptom of arterial insufficiency is intermittent claudication, which limits movement over long distances and requires frequent rest for tired muscles.
- The appearance of pain at rest, especially at night.
- Formation of ulcers and necrotic changes on the feet.
Acute ischemia lasts approximately fourteen days and has two outcomes - gangrene or chronicity of the process.
The most severe form of acute ischemia is called decompensation of the blood supply. It goes through 3 stages of its development: reversible changes, irreversible changes, biological tissue death, in which amputation of the limb is indicated. With subcompensated ischemia, limb function is impaired. This form is identical in course and manifestations to critical leg ischemia. Signs of compensated ischemia: rapid relief of vasospasm, development of collateral blood flow, minimum clinical manifestations, complete restoration of organ function.
A special condition characterized by extremely low blood circulation in the legs and requiring emergency care is called critical ischemia. With this form of pathology, blood practically stops flowing to the feet. In patients, abrasions and abrasions on the feet do not heal well, which leads to the formation of painful ulcers. The skin of the legs becomes dry and cold, cracks and ulcers appear on it, leading to the development of necrosis and gangrene. Symptoms of the pathology constantly torment patients. Critical leg ischemia ends with the development of obliterating arterial diseases, which, if left untreated, leads to loss of limb.
In patients, trophic ulcers appear on the skin of the feet and toes, and pain occurs in the calf muscles at rest and at night. It lasts more than 2 weeks and requires pain relief. The patient's feet are cold and pale. The veins in the legs collapse in a horizontal position and become congested when the leg is lowered. The skin acquires a purplish-bluish tint.
Patients with critical lower extremity ischemia have a characteristic appearance: they sit with their leg down and intensively rub and massage it. At the same time, the patient’s face expresses suffering. In the absence of adequate treatment and with the progression of ischemia, gangrene of the limb develops.
Classification
The medical classification of lower extremity ischemia distinguishes two forms of the disease: acute and chronic. The occurrence of the acute form does not require the presence of concomitant diseases. It develops abruptly and spontaneously, while the patient himself may initially feel good.
Ischemia of the lower extremities of the chronic type is a long-term process. That is, the deterioration of the patient’s condition occurs gradually, while the majority of patients are men who belong to the class of smokers, as well as those who suffer from diabetes.
Diagnostics
A vascular surgeon deals with a similar problem. He begins diagnosing the disease by interviewing the patient to find out the main complaints and life history.
The following factors will help to suspect leg ischemia:
- A history of atherosclerosis, endarteritis or diabetes mellitus,
- Pain in the calf muscles when walking, forcing the patient to stop,
- Foot pain requiring strong pain relief
- The skin of the feet is cold and purple,
- Hanging a leg off the bed brings relief to the patient,
- The appearance of trophic ulcers, increasing pain.
Physical methods of examining the patient include: general examination of the limb, thermometry, assessment of joint movements, determination of sensitivity, study of peripheral pulsation and “capillary” pulse. To determine the affected area, the patient is asked to bend and straighten the affected leg several times. Compression is accompanied by pale skin.
Among the instrumental diagnostic methods, the most informative is Doppler ultrasound. It allows you to determine the level of damage to the vascular bed, makes it possible to see the walls of the vessel and the tissues that surround it, as well as obstacles that disrupt normal circulation. Additional instrumental methods: magnetic resonance angiography, duplex scanning, electrothermometry, capillarography, arterial oscillography, radiopaque aortoarteriography. Using these methods, you can accurately determine the nature of the disease and identify its stage.
HAN
Chronic arterial insufficiency (CAI) of the legs refers to pathological conditions that are accompanied by a decrease in blood flow to muscle fibers and other tissues and its ischemia during increased function or at rest.
Stages of HAN (according to Pokrovsky-Fontaine):
- I – the patient is able to easily overcome up to 1000 meters.
- II A – intermittent claudication when covering 200–500 meters.
- II B – pain when covering a distance of less than 200 meters.
- III – pain when covering a distance of 20–50 meters or at rest.
- IV – trophic ulcerative phenomena or gangrene of the fingers are formed.
The last two stages are defined as critical ischemia.
Treatment
Treatment of ischemia of the lower extremities is a pressing problem and an incompletely resolved issue in modern medicine. Treatment of the disease should be long-term, comprehensive, continuous and aimed at increasing blood flow, preventing thrombus formation and atherosclerotic deposits.
First of all, patients are advised to quit smoking, lead a healthy lifestyle and perform special physical exercises that improve blood circulation in the legs.
Conservative therapy for leg ischemia consists of using:
- Disaggregants – “Curantila”, “Tromboassa”;
- Antioxidants – “Dibikora”, “Coenzyme Q 10”;
- Fibrinolytics – “Fibrinolysin”, “Streptokinase”;
- Drugs that correct lipid metabolism - Lovastatin, Fenofibrate;
- Agents that improve microcirculation - “Pentoxifylline”, “Trental”, “Cavinton”;
- Antispasmodics – “Papaverine”, “Novocaine”;
- Physiotherapeutic treatment aimed at improving blood circulation and ensuring its flow to the lower extremities - diadynamic currents, magnetic therapy, regional barotherapy.
The initial stages of the pathology respond well to drug therapy. In later stages, irreversible changes occur in the body, requiring surgery.
Surgical intervention is aimed at removing blood clots and plaques from the arteries, expanding the lumens of blood vessels, and restoring blood flow in the arteries. To do this, the following types of operations are carried out:
- To expand the lumen of blood vessels - balloon angioplasty and stenting.
- To remove atherosclerotic plaques from the lumen of the arteries - endarterectomy.
- To restore arterial blood flow - bypass and prosthetics.
In the absence of competent and effective treatment, the prognosis of the disease is unfavorable. If blood flow cannot be restored, the patient faces amputation of the limb. Timely bypass surgery or angioplasty allows limb preservation in 90% of patients with critical ischemia.
Treatment of obliterating (occlusive) atherosclerosis of the lower extremities
Therapy for this pathology must be comprehensive and continuous.
1. Conservative therapy:
- to give up smoking;
- constant use of drugs that stabilize the level of cholesterol and lipid fractions - statins (Atorvastatin, Simvastatin, Crestor);
- constant use of antiplatelet agents (“Cardiomagnyl”, “Aspirin cardio”);
- courses of vasodilator therapy in a hospital at least 2 times a year using “Reopoliglyukin” 400 ml + “Trentalom” 5 ml - intravenous drip No. 10, “Xanthinol nicotinate” 2 ml - intramuscular No. 10, “Papaverine” 2%, 2 ml - 2 times a day No. 10, B vitamins.
2. Surgical treatment. Indicated at the 3rd stage of the disease, when pain appears at rest, and with the formation of trophic disorders. The essence of the operation is to form a bypass shunt, which is sewn above and below the site of artery blockage. A number of bypass operations are performed depending on the localization of the process: aortofemoral bypass, iliofemoral bypass, femoropopliteal bypass and other modifications.
3. Endovascular treatment. Recently, endoscopic treatment methods have become widely used, namely angioplasty and stenting in the presence of stenosis in the lumen of the arteries. A conductor is inserted through a small hole in the artery, and a stent is installed at the site of narrowing of the vessel, which widens the lumen and restores blood flow. But a prerequisite is to take blood thinning medications for 1–2 years to prevent thrombosis of the implanted stent.
Treatment is prescribed only after confirmation of the diagnosis by a medical specialist.
Essential drugs
There are contraindications. Specialist consultation is required.
- Clopidogrel (antiplatelet drug). Dosage regimen: orally, at a dose of 75 mg 1 time per day.
- Ramipril (hypotensive, vasodilating agent). Dosage regimen: orally, at a dose of 10 mg/day. in 2 doses.
- Cilostazol (antiplatelet drug). Dosage regimen: orally, before meals, at a dose of 100 mg 2 times a day.
- Naftidrofuril (angioprotective, vasodilating agent). Dosage regimen: orally, at a dose of 600 mg/day. in 3 doses. The course of treatment is long.
Prevention
Preventive measures for leg ischemia:
- Proper, balanced nutrition,
- Increased physical activity
- Optimization of work and rest,
- Fighting bad habits
- Regular monitoring of basic blood parameters,
- Correction of high blood pressure,
- Daily and proper foot care,
- Maintaining a healthy lifestyle.
Compliance with these rules will help avoid ischemia. After all, it is known that a disease is easier to prevent than to treat.
Etiological factors and pathogenetic mechanism
The main reasons are all pathological conditions and processes that lead to impaired vascular patency:
- atherosclerotic disease;
- diabetes;
- prolonged smoking;
- inflammatory process in the wall of the vessel;
- congenital vascular anomalies;
- thrombosis and thromboembolism of arterial vessels of the legs.
HAN can provoke four groups of pathologies:
- pathological processes manifested in metabolic disorders (atherosclerotic lesions, diabetes mellitus);
- prolonged inflammation in the arteries with the presence of an autoimmune component (nonspecific aortoarteritis, thromboangitis obliterans, vasculitis);
- pathologies with a disorder of the innervation of arterial vessels (Raynaud's disease and syndrome);
- exocompression of arterial vessels.
Arterial insufficiency of the legs is mostly caused by damage to the abdominal segment of the aorta or great vessels as a result of atherosclerosis (80%). Nonspecific aortoarteritis is recorded in about 10% of patients, mainly young women.
Diabetes mellitus provokes microangiopathies in 5% of patients. Thromboangiitis obliterans accounts for less than 2%, mainly affects males 20-40 years old, and is characterized by an undulating course with exacerbations and remissions.
The main risk factors for CA are: smoking, dyslipid metabolism, high blood pressure, diabetes mellitus, excess body weight, physical inactivity, alcohol abuse, psycho-emotional factors, genetic predisposition, infections, etc.
Diagnosis
To identify ischemic leg disease, the following procedures are used:
- Inspection. The primary diagnosis is carried out by a surgeon or phlebologist. During the examination, the condition of the skin and vascular pulsation are assessed.
- ECG. Used to identify cardiovascular pathologies that can cause circulatory problems.
- Dopplerography of the vessels of the lower extremities. The method helps to determine the patency of the arteries, measure the pressure in the legs, feet and fingers.
- Angiography. An X-ray examination using a contrast agent is aimed at determining the location of the affected area and the degree of blockage of the vessel.
- Capillaroscopy. Examination of small vessels helps to identify impaired blood supply to soft tissues. Laser Dopplerography is performed for the same purposes.
Important information: How to treat coronary heart disease (CHD) in acute (chronic) form and what are the symptoms of myocardial ischemia in women (men)