According to the World Health Organization, the number of people with diabetes is increasing every year. One of the frequent complications of the disease is diabetic angiopathy of the lower extremities. This pathological condition often causes a violation of the quality of life, as well as disability. The danger is that the disease occurs not only in older people, but also in young people. What are the triggering mechanisms, reasons for progression, first symptoms and treatment methods for diabetic angiopathy?
What is diabetic angiopathy of the lower extremities
The main danger of increased glucose levels is the impregnation of blood proteins and body tissues with the products of its metabolism. The latter then lose their normal structure. The vascular wall, as well as the nervous tissue, are most sensitive to hyperglycemia (increased blood sugar levels).
It is against the background of pathological changes in blood vessels that all complications of diabetes mellitus arise. This abnormal transformation is called angiopathy.
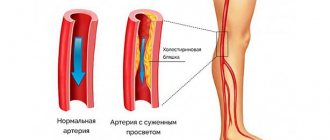
Vessel narrowing leads to circulatory disorders in the lower extremities.
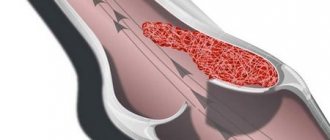
Diabetic angiopathy of the lower extremities is changes in the structure of the vessels of the legs in patients with diabetes mellitus in the form of a decrease in the elasticity of the vascular wall and its thickening, leading to a narrowing of the lumen or complete obliteration (blockage) of the arteries.
Such changes cause a decrease in blood flow to the lower extremities. The foot suffers the most, as it is the most distant segment of the leg. The resulting ischemia (insufficient blood supply and oxygen starvation) causes loss of functional abilities of the lower extremities, trophic changes in the skin, necrosis (necrosis, gangrene) of the fingers, foot or even the entire limb.
Prevention
To prevent diabetic angiopathy, it is necessary to regularly carry out prevention, which includes:
- taking a blood test and monitoring blood glucose levels;
- healthy lifestyle;
- timely contact a dermatologist if any skin rashes, wounds or ulcers appear.
In a preventive complex, it is necessary to monitor the health and condition of the skin of the feet. The slightest wound or scratch on the leg can cause an ulcer to form. Therefore, it is recommended to carry out hygienic treatment and inspection of the feet daily. Nourish and moisturize the skin with cosmetic care products, and trim your nails strictly at a right angle. If there are abrasions and scratches, you must carefully treat them with an antiseptic, but do not use callus plasters or products with a high content of alcohol or other tannins. Wear comfortable shoes that do not rub or squeeze the foot. Avoid overheating and hypothermia of your feet.
Diabetes mellitus is an insidious disease that affects blood vessels. To reduce the risk of developing diabetic leg angiopathy to a minimum, it is necessary to identify all threatening factors, treat the underlying disease and prevent possible complications.
Classification
Depending on which vessels are affected, the disease is divided into the following types:
- Macroangiopathy is damage to vascular structures and arteries of large caliber (diameter) in any segment of the lower extremities. Depending on the specific location of the vessel, macroangiopathy can be located in:
- aorta;
- iliac vessels;
- popliteal artery;
- femoral segment;
- arteries of the leg.
- Microangiopathy is a diabetic lesion of the microvasculature. Changes affect only small vessels of the legs:
- capillaries;
- arterioles;
- venules.
- Combined angiopathy is a combination of diabetic damage to large arteries and small vessels of the legs.
Important to remember! Diabetic microangiopathy of the lower extremities in isolated form is rare. It is combined with damage to the microvasculature of other localizations, including the kidneys (nephropathy) and the retina (retinopathy)!
Causes and mechanisms of the disease
The diagnosis of diabetic angiopathy of the lower extremities itself implies the occurrence of pathology exclusively in patients with diabetes mellitus of both the first and second types. Only a persistent and prolonged increase in the level of glucose (sugar) in the blood can act as the sole cause of such a specific complication.
The likelihood of leg angiopathy and the rate of its progression is influenced by many external and internal factors.
Risk factors for the development of diabetic angiopathy - table
| Risk factors | Influence on the occurrence and course of angiopathy |
| Duration of diabetes | The longer a person has diabetes, the higher the likelihood of vascular damage to the lower extremities. |
| Degree of increase in blood sugar | The higher the glycemia (blood glucose level), the faster and more severe the angiopathy occurs. |
| Age of patients | The effect of age is insignificant and ambiguous:
|
| Concomitant vascular diseases | The presence of any pathology of arterial or venous vessels in diabetic patients (obliterating atherosclerosis, chronic venous insufficiency, endarteritis, etc.) accelerates the onset of angiopathy and aggravates its course. |
| Obesity | Promotes the progression of pathological changes in blood vessels (mostly large arteries) against the background of diabetes. |
| Hypertension | Negatively affects the microvasculature. |
| Smoking | It causes the deposition of atherosclerotic plaques in large arteries, spasms (narrows) capillaries. |
| Leg load | Excessive and insufficient load on the lower extremities leads to worsening angiopathy. |
| Increased blood clotting | Accelerates the onset of diabetic changes in small and large arterial vessels. |
Diagnostic measures
Methods for studying diabetic angiopathy are based on the mechanisms of its development. To make a diagnosis, a specialist uses not only examination data, but also additional diagnostic procedures.
- Determination of lipid fraction indicators - total cholesterol, low and high density lipoproteins.
- Study of the level of glycosylated hemoglobin - the longer the glucose-lowering therapy is ineffective, the higher its percentage.
- Dopplerography of the vessels of the lower extremities - helps to assess the speed of blood flow, the condition of the vein valves and their patency. The method is used without fail in patients with trophic ulcers.
- Ultrasound of the arteries of the legs - makes it possible to determine the thickness of the layers of the artery wall and their capabilities, identifies blood clots and the localization of inflammatory processes on the endothelium, the presence of atherosclerotic plaques, as well as the speed of arterial blood flow and the degree of blood supply to soft tissues.
Arteriography allows you to assess the degree of vascular patency
- Arteriography - the essence of the method is to introduce a contrast agent into the femoral artery and visualize its distribution through small vessels using X-rays or computed tomography. The study helps determine the extent of pathological changes in the vessel, the degree of narrowing and the location of formation of plaques of atherosclerotic origin.
The formation of trophic ulcers is typical for damage to blood vessels of various origins, which must be distinguished.
Differential diagnosis of trophic ulcers - table
| Type of trophic ulcers | Cause | Localization | Pain | Forms |
| Arterial | Severe arterial damage, Buerger's disease | Fingers, foot, ankle joint | Expressed | Various shapes, pale base, dry |
| Venous | Chronic venous insufficiency | Ankle area, especially medial | Moderate | Uneven, with a pink base and detachable |
| Mixed arteriovenous | Chronic venous insufficiency and severe arterial damage | Usually in the ankle area | Moderate | Uneven, with a pink base |
| Skin infarction | Systemic disease, embolism | Lower third of the limb, ankle area | Expressed | Small in size, often multiple |
| Neuropathic | Diabetic neuropathy, neuropathy associated with vitamin deficiency | Plantar surface of the foot (load bearing) | Absent | Calloused edges, often deep, infected |
| Neuroischemic | Diabetic neuropathy + ischemia | Localization as in ischemic, neuropathic or arterial ulcers | Due to neuropathy - reduced | Various shapes, pale base, dry |
Symptoms and clinical manifestations
The presence of diabetes mellitus (even with its most favorable course) for 5 years threatens the development of angiopathy of the lower extremities. Patients have the following complaints about their legs:
- Pain on exertion and at rest.
- Fatigue and fatigue.
- “Intermittent claudication” is a condition when a person is forced to stop while walking short distances due to pain in the legs.
- Swelling.
- Feeling cold.
- Changes in skin color of the legs and feet (pallor, redness, darkening of the fingers).
- The presence of trophic ulcers and poor healing of wounds on the legs
Interesting to know! Diabetic angiopathy can manifest itself to varying degrees in one or both lower extremities. It is often combined with neuropathy (damage to nerve roots and trunks), which significantly aggravates the course. To a greater extent, this feature is characteristic of microangiopathy. The problem remains unrecognized for a long time due to the absence of pain or other warning symptoms, appearing only with the development of irreversible changes in the toes.
Signs of diabetic angiopathy of the lower extremities - table
| Signs of the disease | Characteristic |
| Pale and cold skin | Usually recorded only on the foot and lower leg and indicates the presence of reversible circulatory disorders. |
| Cyanosis | Critical disturbances of blood supply (critical ischemia), threatening transition to gangrene (cold skin). |
| Redness of the skin of the foot | Often indicates diabetic foot phlegmon or erysipelas (the skin is warm). |
| Darkening of the fingers or toes | Evidence of irreversible or severe circulatory impairment:
|
| Presence of non-healing wounds | |
| Edema | If it occurs periodically or briefly on both limbs, it does not pose any danger. Persistent dense edema localized on one leg indicates severe angiopathy, especially if combined with other signs of ischemia. |
| Hypotrophy (volume reduction) | Signs of long-term macroangiopathy affecting high vascular segments. |
| Hair growth disorder on legs | |
| Absence of arterial pulsation or its weakening | A direct and reliable symptom of obliteration (narrowing or blocking) of large vessels. In this case, the pulsation of the arteries below the site of narrowing is most often not detected at all. |
| Muscle weakness of the legs | It appears when walking, accompanied by pain in the calf and other muscles of the leg, intermittent claudication. Patients are not able to perform the usual, and in case of severe angiopathy, minor loads. |
Manifestations of angiopathy of the lower extremities - gallery
Angiopathy degrees
Classification of diabetic angiopathy by severity is very important for an expert assessment of the patient’s condition and determination of the disability group. Any types of damage to arterial vessels due to diabetes mellitus are divided into the following stages:
- Preclinical. Initial pathological changes appear in the vessels, but they do not manifest any symptoms. They can only be detected during a special examination.
- Functional disorders. Diabetic transformation of blood vessels is so pronounced that specific clinical signs arise due to impaired blood supply to the legs. They are reversible.
- Organic changes. Vascular transformation and circulatory failure in the lower extremities are so pronounced that trophic disorders occur. They are either partially reversible or irreversible. Ulcers spontaneously appear on the feet, and gangrene (death) of the fingers or the entire foot occurs.
For purely diabetic macroangiopathy, the following classification has been developed:
- 1st degree - initial manifestations in the form of cold feet, pain in the lower leg when walking a distance of about 1 km;
- 2nd degree - the presence of “intermittent claudication” (pain in the legs when walking, forcing you to stop) at a distance from 50–200 to 400–500 m;
- 3rd degree - inability to walk 50 m without pain, as well as the presence of pain at rest;
- 4th degree - severe pain, trophic ulcers, gangrene of the fingers or the entire foot.
Decoding of ultrasound examination. Ultrasound signs of major pathologies
Vascular macroangiopathy most often develops against the background of other pathologies that have a negative impact on the circulatory system. Conditions such as:
- Hypertension, which bothers the patient for a long period of time.
- Diabetes.
- Hereditary predisposition.
- Changes in blood vessels due to old age.
In most cases, macroangiopathy is a consequence of advanced pathology affecting the condition of the blood vessels. Therefore, vascular damage can be prevented only by timely treatment of these diseases.
Ignoring high blood pressure can lead to the development of macroangiopathy
The ultrasound decoding includes the following indicators that experts pay attention to:
- Systole size (maximum speed of blood movement through the vessels)
- Diastolic blood flow velocity (minimum)
- The ratio of systole and diastolic speed
- Resistance index (ratio divided by diastolic velocity)
The specialist compares the indicators with existing standards and, in accordance with the comparisons obtained, makes a diagnosis. The specialist may also recommend further studies, such as MRI, CT, EchoEG.
There are several of the most common diagnoses that are made based on ultrasound results, these are:
- Atherosclerotic lesion of the vessels of the neck
- Arterial thrombosis
- Arterial deformation
- Nonspecific aortoartery disease (Takayasu disease)
- Metabolic angiopathy
- Arterial dissection
- Cerebral venous circulation
In case of atherosclerotic damage to blood vessels, the specialist first checks the appearance of the vessel: is there any tortuosity or kinks in the vessel.
The condition of the inner layer of the arteries is also assessed, namely its thickness (the norm for the common artery is no more than 0.87 mm, and in the internal carotid artery no more than 0.9 mm).
It is this indicator that is key in diagnosing atherosclerotic lesions of the vessels of the neck.
Arterial thrombosis leads to blockage of the lumen of the vessel, therefore the main object of the ultrasound doctor will be to assess the patency of the vessel and measure the diameter of the lumen of the vessel.
The following indicators are the norm for the diameter of the vessel:
- Vertebral artery 3.5 mm (±0.5mm)
- Internal carotid artery 4.6 mm (±0.5mm)
- Common carotid artery 5.5 mm (±0.5mm)
- External carotid artery 3.7 mm (±0.5mm)
The degree of narrowing of the lumen of the vessel has 3 degrees:
- I degree: reduction of lumen by 40%
- II degree: reduction of lumen by 41 – 65%
- III degree: reduction of lumen by 65 – 95%
Complete blockage (100%) is called occlusion.
Arterial deformation is kinks, tortuosity of the internal and common carotid arteries, which have names:
- Artery lengthening
- Kinking (kinking of an artery)
- Coiling (loop formation)
When an artery is deformed, ultrasound examination is aimed at studying the speed of blood flow and the appearance of the arteries. Also, the best option when examining an artery for deformation is to use color mapping and a sound diagram to determine the intensity of pulsation.
It is the use of color mapping that makes it possible to assess in detail the condition of the vessel and the degree of its deformation.
Such an uncommon disease as nonspecific aortoartery disease (Takayasu's disease) is characterized by inflammation of the inner surface of the vessels, which leads to a gradual thickening of the walls of the vessels and its complete blockage.
Nonspecific aortoartery also has its own types:
- Type I – inflammation of the aorta, branches of the aorta are affected
- Type II – damage to the thoracic and abdominal aorta
- Type III – a combination of lesions of the aorta, abdominal and thoracic zones of the aorta
- Type IV – inflammation affecting the pulmonary artery
Doppler ultrasound examines the condition of the coronary vessels and the speed of blood flow. Normally, the blood flow velocity should be 5.9 ± 0.93 mm; ultrasound sound indicators are also used to determine the presence of murmurs in the aorta.
Metabolic angiopathy cannot be called an independent disease. This disease is similar to a syndrome in which blood vessels are hypersensitive.
This vascular disease is divided into:
- Microangiopathy, in which small vessels and capillaries are affected.
- Macroangiopathies: damage to large vessels.
For this disease, ultrasound examination checks the blood flow velocity (normally ≥0.9), peak velocity in diastole (≥0.5), percentage of stenosis (normally it should not be present), the presence of formations inside the lumen (normally it should not be present) , thickness of the artery wall (normally 0.9-1.1).
Arterial dissection refers to a tear in the intima through which blood enters. Spreading between the layers, it promotes delamination of the walls. Accumulating under the intima, blood contributes to the formation of stenosis.
Doppler ultrasound is considered an additional diagnostic method for this type of pathology. The main method is MRI. During dissection, thickening of the vessel walls is observed. This fact gives rise to further more detailed examination.
Cerebral venous discirculation is quite common. Most often, this pathology is called a cerebral circulatory disorder.
Today, there are three stages of development of this disease:
- Latent. This is the stage of latent development of the disease. There are practically no symptoms of the disease.
- Cerebral venous discirculation. Mild symptoms of the disease that the patient does not pay attention to.
- Venous encephalopathy. The active development of the disease, in which the symptoms appear clearly and clearly. At this stage, medical assistance is necessary, as the consequence may be a threat to human life.
During the examination, disturbances in blood flow in the arteries, dilation of veins, increased intracranial pressure, and disturbances in relationships with surrounding tissues are revealed.
Doppler ultrasound is indicated not only for older people, but also for teenagers and schoolchildren.
This is explained by the fact that today schoolchildren and students have problems with posture, which can lead to any type of pathology of the blood vessels of the neck and brain.
Timely detection of the disease can reduce the risk of developing undesirable consequences.
In addition, the study is completely painless, does not involve harmful radiation and has no contraindications or undesirable consequences.
Based on the patient’s complaints, an experienced doctor thoroughly examines the arteries, veins and aortas for possible pathologies. The doctor also takes into account the individual characteristics of the patient: age, weight, existing chronic diseases.
Ultrasound results can be obtained within 10-15 minutes after completion of the procedure. A simple method that is also considered affordable.
The study is not contraindicated for children either; it can be used to detect pathologies in newborns, which greatly simplifies treatment in the future.
In this case, the procedure is called neurosonography and is carried out through a fontanel on the child’s head that has not yet healed.
Diseases of the brachycephalic arteries are considered the most common among vascular pathologies. In Russia, 450 thousand people suffer from the consequences of a stroke.
Timely diagnosis of blood vessels will help prevent not only the occurrence of diseases, but also capture those that already exist, even in the early stages of development.
In most cases, the following factors lead to the development of angiopathy of one form or another:
- – damage due to injury;
- – violation of the nervous regulation of the tone of the vascular walls;
- – various blood diseases;
- - arterial hypertension;
- – intoxication and hazards at work;
- - elderly age;
- – smoking;
- – systemic vasculitis, which is autoimmune in nature;
- - diabetes;
- – bad habits, in particular smoking;
- – congenital features of the structure of vascular walls.
First of all, certain symptoms of angiopathy depend on where the pathological process is localized. Thus, with different types of angiopathy, the following symptoms may be observed:
- – complete loss of vision or a significant decrease in its acuity;
- – feeling of itching and burning in the legs;
- – pain in the lower extremities with the development of intermittent claudication, when pain occurs when walking and gradually disappears during a period of rest;
- – frequent and intense nosebleeds;
- – bleeding in the gastrointestinal tract;
- – appearance of blood in the urine – hematuria;
- – the appearance of petechiae and telangiectasia on the surface of the skin;
- – hemoptysis;
- - trophic disorders of various types - from dryness and flaking of the skin on the arms and legs to the occurrence of gangrene of the foot.
What is vascular angiopathy of the lower extremities? These are complications in the form of disruptions in the functioning of the walls of elastic tubular formations in the human body and their structure, caused by various diseases. The advanced form provokes irreversible processes due to improper blood circulation over a long period of time.
Vascular angiopathy of the lower extremities in diabetes mellitus is caused by excess glucose in the blood. It destroys small and large human tubular organs, which in some cases thicken and in others become thinner, which leads to their deformation. Fatty deposits can form in the tissue walls, while mucopolysaccharides are deposited on the inner surface. As a result, blood does not fully circulate in the body, and oxygen starvation occurs.
https://www.youtube.com/watch?v=E1eiw-5pwwI
If the legs are affected, the fingers atrophy first, then the foot, lower leg and thighs. These tissues can no longer be restored, so they can only be amputated. Angiopathy of the lower extremities develops between 30 and 40 years. It does not depend on the patient’s age, but on the severity and duration of diabetes, changes in blood sugar and control over it.
Angiopathy of the lower extremities, in addition to diabetes mellitus, has the following causes:
- disruption of the nervous system, which is responsible for the tone in the walls of blood vessels;
- hypothermia of the lower extremities;
- damage resulting from injury;
- bad habits;
- blood diseases;
- arterial hypotension and hypertension;
- work associated with hazardous work;
- systemic vasculitis, autoimmune origin;
- lesions of the brain and spinal cord;
- congenital pathology of the structure of the walls of blood vessels;
- damage to peripheral nerves when blood vessels lose their regulatory ability;
- long-term vegetative-vascular dystonia, which is not treated correctly.
Diagnostics
The following methods allow you to detect diabetic angiopathy of the lower extremities:
- rheovasography - graphic recording of the pulse wave of the arteries of the legs. It is rarely used due to the current availability of more informative methods;
- ultrasound diagnostics: Doppler examination - detects macroangiopathy at any level, determines the degree of its severity;
- color duplex scanning of vessels - displays the affected vascular areas on the screen.
An angiogram reveals a decrease in blood circulation in the vessels of the legs due to narrowing of their lumen
How is diabetic macroangiopathy diagnosed?
Diagnosis is carried out to determine how severely the coronary, cerebral and peripheral vessels are affected.
To determine the necessary examination method, the patient must consult a doctor.
The examination is carried out by an endocrinologist, diabetologist, cardiologist, vascular surgeon, cardiac surgeon, and neurologist.
For type 1 and type 2 diabetes, the following types of diagnostics are prescribed to identify pathogenesis:
- A biochemical blood test is performed to determine the level of glucose, triglycerides, cholesterol, platelets, and lipoproteins. A blood clotting test is also performed.
- The cardiovascular system must be examined using an electrocardiogram, 24-hour blood pressure monitoring, stress tests, echocardiogram, Doppler ultrasound of the aorta, myocardial perfusion scintigraphy, coronary angiography, and computed tomographic angiography.
- The patient’s neurological condition is clarified using Doppler ultrasound of cerebral vessels, duplex scanning and angiography of cerebral vessels are also performed.
- To assess the condition of peripheral blood vessels, the limbs are examined using duplex scanning, Doppler ultrasound, peripheral arteriography, rheovasography, capillaroscopy, and arterial oscillography.
Treatment
The set of conservative treatment measures for diabetic angiopathy of the lower extremities may differ depending on the severity of the disease, the age of the patient and the individual characteristics of the body.
Conservative treatment - table
| Direction of treatment | Description and detail |
| Reduced blood sugar levels |
|
| Lower cholesterol levels | statin drugs (Lovastatin, Atorvastatin, Simvastatin) |
| Blood thinning |
|
| Improving blood circulation and microcirculation |
|
| Stabilization of metabolic processes in affected tissues |
|
| Elimination of pain syndrome | painkillers and anti-inflammatory drugs (Ketorolac, Dexalgin, Diclofenac, Ibuprofen) |
| Fighting infection | Antibacterial therapy is indicated in the presence of any skin lesions and wounds on the lower extremities against the background of diabetic angiopathy, obvious signs of suppurative processes. Broad-spectrum antibiotics are prescribed (Ceftriaxone, Tsiprinol, Levofloxacin). |
| Treatment of concomitant neuropathy | Berlition or Tiogama in combination with a B complex of vitamins (Neuromax, Milgama, Vitaxon) |
| Hygienic foot care | The most important element influencing the frequency of purulent-gangrenous complications of diabetic angiopathy of the lower extremities. Patients should take care of their shoes (they should be comfortable), the appearance and treatment of abrasions, calluses, wounds, avoid prolonged standing on their feet, trim nails and corns (dry calluses) correctly and in a timely manner. |
The need and types of surgical intervention
Surgery for diabetic angiopathy of the legs is resorted to in the presence of:
- Lesions of large vessels (ilio-femoral-popliteal segment) in the form of single limited areas of narrowing. Such patients undergo:
- bypass operations (replacement of narrowed areas of the vascular bed with artificial or prosthetic ones from one’s own veins);
- thrombectomy and endarterectomy - removal of pathological tissues blocking the lumen of the artery;
- endovascular interventions - expansion of narrowed areas using a pneumatic balloon or a special vascular stent.
During vascular operations, the patency of the affected arterial vessels is restored - Widespread lesions of the artery in all segments or obliteration (narrowing) of the main branches on the lower leg. In such cases, the question of the advisability of an operation is considered - sympathectomy (removal of the nerve nodes responsible for arterial spasm.
- Purulent wounds, phlegmon, osteomyelitis, necrosis (death) of fingers. It is recommended to perform sanitizing operations, the essence of which is the opening and wide drainage of all purulent cavities, removal of non-viable tissues, and amputation of fingers. For cleaned large wounds, they are covered plastically with skin.
- Gangrene of the lower limb. Amputation is performed:
- forefoot - with gangrene of all toes;
- at the level of the lower leg - with wounds affecting the heel area against the background of preserved main blood flow to the level of the popliteal artery;
- at the level of the thigh - with gangrene of the foot and lower leg.
Important to remember! Sanitation operations for diabetic angiopathy of the lower extremities do not relieve a person of the problem, but only prevent intoxication and the spread of the purulent process.
Possibilities of traditional medicine and homeopathy
Treatment of angiopathy of the lower extremities should be comprehensive, so in no case should you rely entirely on folk remedies and homeopathy. Before using any recipes, you should consult a specialist.
Effective traditional medicine recipes:
- Lime tea. Pour a tablespoon of chopped dried linden blossom into a glass of boiling water. Keep on low heat for 10–12 minutes. Do not bring to a boil. Take a glass of the prepared drink after meals 3 times a day.
- Blueberry tea. Grind dry or fresh blueberry leaves, place in a metal bowl and pour two cups of boiling water. Put on the fire for 5-7 minutes, without bringing to a strong boil. Take 3-4 times a day 15-20 minutes before meals.
- Infusion from bean leaves. 5 tbsp. l. chopped bean wings, 2 tbsp. l. rose hips, St. John's wort and horsetail, 1/2 tbsp. l. Place flaxseeds in a thermos, add a glass of boiling water. Leave for at least 2–3 hours. Distribute into 3 doses. Drink 30 minutes before meals.
- Foot bath based on wheatgrass roots. Take 50 g of crushed dried wheatgrass roots, place in a metal bowl and add 1 liter of hot water. Bring to a boil and keep on low heat for 10–15 minutes. Add the prepared broth to a bowl or bath with 5 liters of water (no more than 35–36˚C). The duration of the procedure is 15–20 minutes.
Folk remedies against complications of diabetes mellitus - gallery
Possible consequences and complications
Diabetic angiopathy of the lower extremities sooner or later leads to complications. Possible outcomes of the disease:
- Stable course with minimal symptoms and slow progression. This option is most likely in mild forms of type 2 diabetes.
- Progression of angiopathy with the formation of diabetic foot syndrome: persistent pain, swelling, foot deformity, purulent complications (phlegmon, osteomyelitis), trophic ulcers.
- Necrosis (gangrene, necrosis) of fingers, feet, legs.
The presence of gangrene and purulent-necrotic complications poses an immediate threat to the patient’s life, as it causes severe intoxication of the body with the decay products of its own tissues.
Interesting to know! Patients with diabetes mellitus complicated by damage to the blood vessels of the legs are treated simultaneously by doctors of several specialties: an endocrinologist or a vascular surgeon. Today, there are specialized specialists working in “diabetic foot rooms.” They are called podiatrists!
Etiology and pathogenesis
Macroangiopathy in diabetes mellitus is a common occurrence; an increased content of glucose flows through the blood vessels, which has destructive power. It leads to denaturation, in one place the wall becomes thinner and brittle, while in another it thickens. Due to poor blood clotting, clogging and thrombosis occurs. Tissues and organs suffer from a lack of oxygen (hypoxia), which leads to dysfunction of many body systems.
Such changes occur in the body during the development of the disease:
- the walls of blood vessels become heterogeneous, damage appears;
- blood viscosity increases;
- the speed of blood transport through the vessels slows down.
The entire body suffers from the consequences, especially the lower limbs, where most of the load falls.
The main reasons for the development of the disease:
- heredity;
- injuries of varying degrees (in diabetes, healing is slow and problematic);
- blood and plasma diseases;
- intoxication of the body with drugs;
- hypertension;
- decreased body reactivity.
Return to contents
Preventive measures
Preventive measures are aimed at:
- preventing the onset and progression of diabetes. Relevant only for the second type of disease. Involves normalizing nutrition, combating obesity, quitting smoking, alcohol abuse and other bad habits;
- reducing the rate of progression of angiopathy. Timely correction of blood sugar levels, systematic drug and surgical treatment aimed at restoring blood circulation in the vessels of the legs;
- prevention of purulent gangrenous complications. Involves compliance with all measures for the care of the lower extremities.
Causes
There are many causes of angiopathy. Below are the most common factors in the development of this disease.
- diabetes;
- pathologies of the endocrine and vascular system;
- sepsis;
- various intoxications;
- rheumatism;
- hypovitaminosis;
- physical inactivity;
- harmful working conditions;
- obesity;
- bad habits;
- excessive salt consumption;
- age 55+.
To prescribe effective treatment, it is first necessary to find the root cause of the disease.
After all, fighting solely against the consequences is fraught with the progression of the disease and its periodic relapses.