Superficial
They originate from the branching of venous networks, the location of which is in the forearm and hands, more precisely, in the subcutaneous tissue.
There are 2 main ones - the royal one and the head one. Characteristics:
- royal - formation begins in the elbow or hand from the venous network. In the area of the hand and forearm, it anastomoses with other venous branches. Then it flows into the axillary fossa into the canal of the same name. Its largest anastomosis crosses the cubital fossa in an oblique direction, where it is located under the skin. This vessel is the connector of all superficial vessels. In addition, with its help, an anastomosis is established between the superficial and deep channels. It should be noted that the diameter of the ulnar fossa in relation to the position of the canals does not have a constant value;
- head - beginning - radial side of the hand. It is located in front of the forearm and in the ulnar fossa. It then flows along the deltoid pectoral groove, from where it is directed under the collarbone.
Superficial veins into which IV injection can be made.
Ticket number 1.
Histological structure of tissues. Topography of fabrics.
Histology - the science of tissues
Tissue is a historically established collection of cells and intercellular substance, united by a unity of origin, structure and function.
There are four types of fabrics:
- Epithelial
- Connective
- Muscular
- Nervous
Epithelial tissues:
They consist of a large number of well-defined cells and a small amount of intercellular substance. The shape of cells in epithelial tissues can be different.
Connective tissues:
They consist of cells and intercellular substance, and both cells and substance are very well developed.
Highlight
- Connective tissue itself (loose fibrous and dense fibrous).
- Tissue with special properties (pigment and adipose tissue).
- hard skeletal tissue (bone, cartilage).
- Liquid connective tissue (blood, lymph).
Muscle tissue:
Capable of shrinking. Myocyte cells are spindle-shaped. In the center are myofibrils, due to which cells are able to contract.
The following types of muscle tissue are distinguished:
- Smooth muscle tissue.
- Cross-striped muscle tissue.
Smooth muscle tissue is a mononuclear cell consisting of myocytes connected to each other by connective tissue. They contract slowly and practically do not get tired. They are innervated by the autonomic nervous system, that is, they are not subject to consciousness. They are part of blood vessels and hollow internal organs.
Nervous tissue:
Consists of cells and intercellular substance.
Cells are neurons. Consist of a body and appendages. Short processes are dendrites. Long ones are axons.
They carry nerve impulses from organs and tissues to the brain. Their bodies are outside the central nervous system.
1.Intercalary neurons are located in the central nervous system and transmit information from the sensory neuron to the motor neuron.
2.Efferent - motor. They carry information from the central nervous system to the working organ. The bodies are located in the central nervous system.
2. Venous drainage from the upper limb.
Through the veins, blood flows in the systemic circulation through the superior and inferior vena cava and the coronary sinus. The coronary sinus is located in the coronary sulcus; the veins of the heart, small and large, flow into it.
Venous drainage from the neck
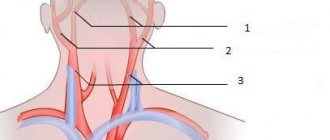
There are superficial and deep veins of the neck.
The superficial veins are the external and anterior jugular veins. The external jugular vein lies in the neck over the sternocleidomastoid muscle and collects blood from the soft tissues of the neck and occipital region. This vein flows into the internal jugular, subclavian veins or into the venous angle.
The anterior jugular vein is formed from small veins of the mental region, descends along the sides of the midline of the neck behind the sternum, where the left and right anterior jugular veins are connected by a transverse anastomosis - the jugular venous arch, which flows into the external jugular vein of the corresponding side.
In the neck, the following deep veins flow into the internal jugular vein, accompanying the arteries of the same name: pharyngeal, lingual, and superior thyroid veins.
The veins of the upper limb are divided into superficial and deep.
Superficial veins are located under the skin, where they form venous networks. The largest superficial veins of the arm are the lateral and medial saphenous veins of the arm. The lateral saphenous vein of the arm, cephalica, begins on the back of the hand, from where it follows to the radial side of the forearm, then passes to the shoulder, where it lies in the lateral groove outward from the biceps muscle, rises to the clavicle and flows into the axillary vein. The medial saphenous vein of the arm, basilica, begins on the back of the hand, rises along the ulnar side of the forearm to the shoulder, where it flows into one of the brachial veins. In the area of the cubital fossa between the lateral and medial saphenous veins of the arm there is a well-defined anastomosis - the intermediate vein of the elbow.
The deep veins of the upper limb lie next to the arteries and have the same names. In this case, each artery is usually accompanied by two companion veins. From the deep veins of the hand, blood flows into the veins of the forearm. The ulnar and radial veins merge into the two brachial veins. The brachial veins merge to form the axillary vein. The axillary vein azygos is the main collector of venous blood flowing from the upper limb. In addition to the veins of the arm, it receives the veins of the muscles of the shoulder girdle and partly the muscles of the chest. At the level of the outer edge of the first rib, the axillary vein continues into the subclavian vein.
The subclavian vein passes in front of the subclavian artery, being separated from it by the anterior scalene muscle. Merging behind the sternoclavicular joint with the internal jugular vein, they together form the brachiocephalic vein.
Superficial veins into which IV injection can be made.
The ideal place for injection is the venous vessels, the contour of which can be palpated, in the elbow. The reason for this also lies in the thin layer of skin covering them. The injection can be given into any palpable veins on the body.
4. The concept of disease (health, disease, nosology, etiology). Causes and conditions for the development of diseases. Forms and stages of development of diseases. Outcomes of the disease .
Disease is a special condition that occurs as a result of a violation of the correspondence between the body and the environment.
Signs of the disease - SYMPTOMS. Each disease has its own specific symptoms, i.e. every disease has its own face. Symptoms are: - Subjective - Objective Subjective are those sensations that the sick person himself speaks about - nausea, pain, weakness, loss of appetite, feeling hot. Objective - these are the signs of the disease that are revealed during examination - change in skin color, appearance of a rash, presence of a tumor
Clinically, the following periods are distinguished during the course of the disease: - latent (latent, incubation period) - prodromal period - period of pronounced manifestations. - recovery period (outcome) Latent period - from the beginning of exposure to pathogenic agents to the first manifestations. At this time, the body tries to self-regulate on its own to suppress trouble. The duration of this period can be long or short in cases of poisoning. The prodromal period (from prodrom - harbinger) from the appearance of the first symptoms of the disease, which are often vague, uncharacteristic of any one disease - headache, weakness, loss of appetite, body aches, etc. Period of pronounced clinical manifestations: during this period, the most characteristic symptoms of the disease appear. Sometimes an abortive form of the disease occurs, when the disease begins acutely, violently and suddenly ends in a short time and recovery occurs. According to the duration of the disease, they are divided into: - acute (lasting up to 4 days), - acute (5-14 days) - chronic when the disease continues for years, decades. Acute diseases have a certain duration and a certain clinical picture. The subacute course of the disease and can occur in a chronic course, when there is an unclear picture of the disease, it can last for months, and chronic diseases drag on for years. Sometimes diseases can have undesirable complications when another, more severe one develops against the background of a given disease. With influenza, damage to the kidneys, lungs, and brain can develop. Outcome of the disease: - recovery - relapse (resumption) - protracted course and transition to a chronic form. -death Distinguish between: -full recovery, when no disorders caused by the disease remain in the body. - incomplete recovery, when residual phenomena remain in the body in the form of a violation of structure and function, i.e. a pathological condition develops.
Etiology is the study of the causes and conditions for the development of a disease.
Health is a state of complete physical, spiritual, social well-being, and not just the absence of disease or physical effects.
Nosology is the study of diseases, which allows solving the main problem of particular pathology and clinical medicine: knowledge of the structural-functional relationships in pathology, the biological and medical basis of diseases. Nosology answers the following questions: what is disease, and how does it differ from health, what are the causes and mechanisms of disease development, recovery or death.
Ticket number 2.
Possible diseases
Vein disease of the upper limb is a rare phenomenon. It usually appears gradually and progresses slowly.
Possible diseases:
- post-injection thrombophlebitis - occurs after injection of certain medications under the skin. Once administered, they cause tissue damage or irritation. Such drugs may be: calcium chloride, radiocontrast agents, furagin or ristomycin. Very rarely occurs as a result of an insect bite, after local trauma;
- acute thrombosis of the subclavian vein - localization - subclavian bed, with spread to the shoulder and axillary beds. When an illness occurs in the upper extremities, blood flow is disrupted. Its second name is Pagett-Schroeter syndrome;
- superior vena cava syndrome is a serious disorder of the circulatory system. This condition is considered severe;
- venous insufficiency - a condition characterized by lower pressure in the blood vessels of the arms than in the lower extremities. Quite a rare disease. Its result is a disruption of the valves, which do not allow blood to fully move in the opposite direction of blood outflow;
- varicose veins - the disease has 2 causes. It can occur during intrauterine development of the fetus, the second reason is heredity. It can be detected quite easily if you palpate the vein along its entire length. In this case, small balls and strong pulsation should be felt in the canal;
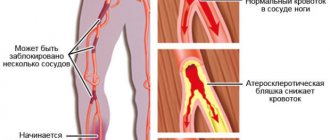
- Peripheral vascular disease or artery disease is a disorder that blocks or noticeably reduces a vessel in the upper extremities, resulting in decreased blood flow to them.
Intravenous injection: preparation for the procedure
Before the injection, preparation is carried out:
- patient
- medical worker
- workspace
Patient preparation
The nurse must introduce herself to the patient, explain to him that the doctor has prescribed a procedure, and obtain consent to perform it. The patient should be asked about a history of allergic reactions and experience with such manipulations. You should also find out how long ago the patient ate food.
Most drugs cannot be administered intravenously on an empty stomach. In some situations, on the contrary, you should not eat food before the injection. The patient must consent to the medical intervention “intravenous injection”.
Nurse training
The nurse checks that all equipment necessary for the intravenous injection is present. Instruments, medicines, consumables, disinfection solutions - everything should be checked for availability and expiration dates.
The health worker washes his hands hygienically and dries them with a disposable towel. Then, with clean hands, put on a mask, goggles, and an oilcloth or plastic apron. The skin of the hands is treated with a skin antiseptic. You should wait until your hands are dry, then put on non-sterile gloves.
Preparing your workspace
To carry out the procedure you will need:
- Hand washing soap
- Skin hand sanitizer
- Manipulation table
- Couch
- Chair for intravenous manipulation. If it is not available, use a pillow to place under the elbow or other injection site.
- Sterile tray for syringe with medicine
- Non-sterile waste tray
- Scissors or tweezers (non-sterile) for opening bottles
- File for opening the ampoule
- Syringes of appropriate volumes
- Alcohol wipes or sterile cotton balls + antiseptic for treating ampoules, vials and the patient’s skin (70% alcohol or other)
- Non-sterile gloves
- Sterile gloves
- Container for collecting sharps waste class B
- Containers for collecting waste of classes A and B
Read also: Putting ointment in the eyes, nose, ear: equipment, preparation, algorithm
In which veins are intravenous injections given?
Veins for injection procedures must meet the following parameters:
- be clearly visualized;
- clearly appear above the skin;
- be slightly displaceable;
- have a strong shell.
For intravenous injections, you can choose any vein, but the one located in the bend of the elbow is more accessible and convenient. It is perfectly visible and palpable, so it is easy to penetrate it with a needle.
Due to the risk of developing thrombotic processes, the blood channels of the legs are chosen only when other veins are inaccessible.
Occasionally, subcutaneous blood vessels located in the forearm area or the back of the hand are selected for intravenous manipulation.
For infants, venipuncture is performed into the subcutaneous vessels of the scalp.
In emergency situations, injections are also given in the sublingual area, where a rich venous network is localized and there is better access to the bloodstream. The vascular channels in this area are dilated even in the event of death and are located next to the vessels of the brain, head, and heart.