Unstable angina is a type of coronary syndrome in which the lumen of the artery of the same name, which supplies the muscle fibers, narrows. The result is a so-called heart attack, which can result in a heart attack.
According to the name, this type of pathological process is characterized by fast or slow, but steady progression over several years or even dozens. Who's lucky?
Prospects for cure vary. The unstable form of angina sooner or later ends in the death of muscle tissue, the actual heart attack and death.
Mechanism of symptom development
The essence of the development of a pathogenic phenomenon lies in the disruption of the supply of cardiac structures, in particular the myocardium, with blood, and therefore with oxygen and nutrients.
The duration of the development of the problem is from several months to a couple of years, then angina pectoris goes on a constantly progressive straight line with a delayed prospect of a heart attack. The possibility remains even during therapy.
One or two factors cause the onset of unstable angina:
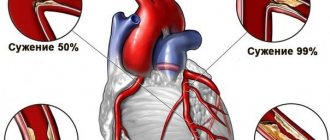
- The coronary artery narrows (stenoses).
- Less commonly, blockage of the lumen of the vessel occurs with a cholesterol plaque or thrombus.
In the first case, an increasing clinical picture is more likely, with a chronic or latent course. In the second there is an acute variety.
As soon as the blood supply structure is narrowed to 70%, typical symptoms occur. Among which are chest pains and others.
In the absence of urgent help, acute myocardial ischemia, heart attack and death from failure of the muscular organ are possible.
The prospect of recovery directly depends on the speed of first aid, its nature and literacy, and the adequacy of basic therapy in the hospital.
Diagnosis of an angina attack
Doctors can usually tell if you are having an angina attack by listening (auscultating) to your heart. The complaints presented to patients are also important.
The most commonly used diagnostic tests are:
- Blood tests.
- lipoprotein profile , which allows you to check your cholesterol levels.
- Fasting glucose test , necessary to determine blood glucose levels.
- A C-reactive protein (CRP) test may indicate inflammation (a risk factor for coronary heart disease).
- Tests for cardiac markers such as troponin, which is released during severe ischemia or injury.
- Regular testing for low hemoglobin (the part of the red blood cell that carries oxygen throughout the body) can help rule out other possible causes of chest pain.
- Electrocardiography (ECG) is a test that uses adhesive material to attach small electrodes to the arms, legs, and chest to measure the rate and regularity of the heartbeat and test the health of the heart muscle.
- Stress test with physical activity . The subject is asked to perform an exercise such as walking on a treadmill, and ECG and blood pressure readings are taken before, during and after the exercise. As a result, the magnitude of changes in heart rate and blood pressure is determined.
- Cardiac catheterization - a thin flexible tube (catheter) is passed through an artery in the groin or arm into the coronary arteries, due to which the vessels are examined from the inside and the quality of blood flow is monitored.
Variant angina is most often diagnosed using a Holter monitor. This test allows you to continuously measure the rate and rhythm of your heart for 24 hours (or longer) and record the data, which is then checked and analyzed by a doctor.
Video: Relieving an angina attack
Differences from stable form
Typical features of the classic, stable variety of the pathological process:
- Slow development. The duration of formation is several years.
- Relative predictability. As soon as the painful signs and the anatomical changes themselves reach a certain critical mass, the phenomenon stops, there is no more progression, which gives hope for a complete recovery with proper treatment.
- Good prognosis. The effectiveness of therapy varies between 80-90%, which makes supervision a necessary element in removing the patient from the pathological condition.
- Weakness of symptoms. Manifestations, compared to other forms, are characterized by mildness; heart attacks are rare; this is rather an exception. It occurs against the backdrop of a long process, with an advanced variety.
Unstable angina is the complete opposite: it progresses quickly, has a vivid clinical picture, objective signs are severe and reduce the quality of life significantly, the risk of a heart attack depends on the duration and nature of the process, in general it is within 60%, even treatment does not eliminate this probability.
Often the etiology of the pathogenic process is different:
- the stable variety is determined by cholesterolemia and plaque formation;
- unstable type - thromboembolism, cardiac organic problems, advanced atherosclerosis due to calcification of lipid deposits.
Treatment is differentiated and requires a thorough diagnosis of the cardiological plan. Typically surgical.
Classification of unstable angina
Typing is carried out on two grounds: the characteristic moment of detection, the course, and the degree of severity and anatomical deviations. In accordance with the main criterion, the following are distinguished:
- Primary or recently emerging form. It is characterized by newly developed symptoms of unstable angina, and the manifestations must begin less than 2 months ago. The symptom complex increases gradually or sharply, spasmodically, recovery is still possible, a potentially reversible phenomenon. Against the background of a heart attack, the prognosis worsens significantly.
- Post-infarction type. As the name suggests, it occurs as a result of necrosis of cardiomyocytes. The larger the area, the more serious the consequences. Angina attacks can occur up to several times a week, each more severe than the previous one. Without urgent medical care, a relapse is likely to develop, this time fatal.
- Angina at rest. Mainly associated with neurogenic or hormonal factors, less often with purely cardiac ones. The process is accompanied by stenosis of the coronary arteries. Attacks are frequent. Up to several times in the short term, each episode lasting about 10-20 minutes. It is difficult to identify such a phenomenon, since during remission there are no objective signs. The condition is dangerous for a heart attack. The risk is almost 80%, development prospects are 3-6 months, sometimes faster.
- Progressive variety. Matches any shape above. Characterizes the course of the pathological process. In this case, there is an increase in attacks, up to 6-10 times a week. Recovery is problematic because organic pathologies occur. A heart attack is almost inevitable, the treatment is radical, and its effectiveness is difficult to predict.
Main clinical manifestations
In addition to the listed symptoms, as the attack progresses, the following occur:
- disturbance of heart rhythm (only in 60% of all cases is tachycardia, and in 40% is the opposite situation with a slowdown in heart rate), against the background of changes in heart rate in severe cases, extrasystole, fibrillation, paroxysmal tachycardia may occur: interrupting the arrhythmia is vitally important, in otherwise, cardiac arrest and death may occur;
- acrocyanosis of the nasolabial triangle is a hallmark of angina, associated with insufficient oxygen supply to all tissues and organs, congestion in the pulmonary circulation;
- pale skin occurs due to vegetative-vascular disorders: imbalance of spasm and vasodilation occurs at a reflex level, such hemodynamics lead to marbling of the skin;
- sleep disturbance does not develop in everyone, only in patients with a history of coronary artery disease and signs of heart failure;
- shortness of breath is asthmatic in nature, causing fear of death, panic (if the process progresses, asphyxia may occur);
- panic attacks are observed in 95% of cases, occur in response to stress, and are accompanied by retardation of thinking against the background of psychomotor agitation;
- presyncope and fainting begin with dizziness and indicate cerebral hypoxia, the danger lies in the development of a stroke;
- disturbance of the monthly cycle, infertility are nonspecific signs of angina in women, but they do exist: for normal ovulation, sufficient nutrition of all pelvic tissues is required, which is impossible with angina, so even if menstruation persists, the likelihood of infertility is high;
- pastiness increases from the periphery, the ankles and legs swell, the hands and face are gradually involved in the process: the reason is either impaired blood supply to the kidneys or impaired liver function;
- acute circulatory disorders are mainly represented by symptoms of angina pectoris, which are extremely life-threatening (mortality rate is about 50%), the main cause is stroke, and the following symptoms require calling an ambulance: increasing pulsating cephalalgia; dizziness; vomit; loss of coordination; myalgia, muscle weakness; ataxia; sluggish speech; loss of sensitivity, paresis, paralysis.
- asthenia, mental disorders occur late, manifested by a feeling of drowsiness, loss of cognitive functions, and depression.
Stages of the pathological process
The second criterion is determined by the following stages of the pathogenic phenomenon:
- First or easy. There are no attacks, and accordingly, no symptoms either. Characterized by objective deviations, and even then not always. Since typical symptoms occur only during spasm of the coronary arteries. There are no organic disorders yet, the process is completely reversible. At this stage, unstable angina does not last long, the duration of the favorable period is about 1 year or a little more.
- Second. Moderate. It is defined by mild attacks, they last no more than 30 minutes, and there are no defects in the cardiac structures. Recovery is still possible, but help is often surgical. The origin of the process is cardiac, less often neurogenic or hormonal.
- Third. Expressed. Severe organic changes in the heart and coronary vessels, progressive failure, hemodynamic disorders and organ dysfunction. Recovery is unlikely, but there are chances to prolong the patient’s life and delay a heart attack as far as possible. At this point, a cure is only possible through a donor heart transplant.
- Fourth phase. Terminal. The risk of cardiomyocyte necrosis is maximum, and after the first episode, a second one is inevitable. Therapy, even radical therapy, makes little sense. The only chance of salvation is an urgent heart transplant.
Classifications are required to stage the clinical form of the pathological process, on the one hand, and, on the other, to determine the paths of supervision and the prospects for the effectiveness of treatment.
Causes
The factors, as is already clear, are hormonal, cardiac or neurogenic.
- Diabetes. Systemic, well-studied disease. Involves generalized organ dysfunction. Recovery is impossible; treatment is lifelong, supportive and emergency during attacks. Angina pectoris occurs as a late consequence; it is difficult to predict when this moment will make itself known.
- Hyperthyroidism. Excessive production of thyroid hormones. T3, T4, also TSH (pituitary substance). The essence of treatment is to normalize the background of specific compounds, which requires comprehensive assistance from an endocrinologist. A diet and the use of iodine preparations are necessary to normalize the condition. The change is not terminal in nature unless the phenomenon is triggered. Considering that the symptoms are quite developed, it is difficult not to notice them.
- Obesity. The main reason is a violation of lipid metabolism and metabolism in general. The result is the development of diabetes mellitus and the deposition of cholesterol plaques on the walls of blood vessels. Actually, increasing body weight is not a factor in development. Everything is much more complicated.
- Alcohol abuse. Oddly enough, people who constantly drink in large quantities are less susceptible to developing cardiac pathologies, as long as they maintain their body with alcohol. Withdrawal syndrome ends in angina pectoris in 100% of cases, if we are talking about a long-standing, severe form of alcoholism.
- Drug use. The classic substances that damage the heart in particular are cocaine and heroin. Not to mention street varieties of incomprehensible structure - desomorphine and others. Persons who consume such compounds do not live long. Angina pectoris provokes a heart attack almost immediately, recovery does not make sense, the organic abnormalities are too severe.
- Smoking. Has a delayed effect. At first, the patient is unlikely to feel anything. There will be no symptoms after the first year of tobacco use. All problems will appear later. By that time, getting back on your feet will be very difficult. A complex of problems arises. The classic combination is COPD + coronary insufficiency. Death occurs as a result of a heart attack, stroke or thromboembolism. A bonus is blockage of the arteries of the lower extremities or persistent stenosis of the structures. The result is gangrene and the need for amputation.
- Recent heart attack. A generalized hemodynamic disorder affects. When acute tissue death occurs, relapse is almost inevitable. If you're lucky, you can delay it for many years; sometimes death occurs from another factor altogether, the patient does not have time to live to see a second heart attack.
- Spasm of the coronary arteries. Occurs under the influence of angiotensin-II and aldosterone. Also as a result of disruption of inhibition processes in the nervous system. Treatment is urgent, with the use of medications to reduce blood pressure.
- Stage 2-3 hypertension, without specialized therapy or due to insufficient recovery measures.
- Atherosclerosis. The most likely pathological process on the part of the blood supplying structures of the body, leading to ischemic heart disease (coronary heart disease), which is the cause of attacks of unstable angina. It is characterized by stenosis of the coronary arteries or, more often, the deposition of cholesterol plaques in the vessels.
For an attack of unstable angina to begin, a trigger factor is required:
- Intense physical activity.
- Consuming a caffeinated drink.
- Smoking.
- Stress.
- Fatigue and lack of sleep.
- Long-term use of cardiac drugs.
Classification of the disease
There are several types of pathology such as angina pectoris. Symptoms and what medications the patient should take must be discussed with a doctor.
The classification below will allow you to understand what form of the disease you are dealing with:
- Stable angina. Occurs only against the background of overvoltage. The pathology is characterized by 4 development classes, which characterize the permissible level of load that can be tolerated by the heart.
- Unstable angina. It is also called progressive. The patient may suddenly feel a deterioration in health. In this case, there may not be any provoking reasons. Doctors say that this type of pathology develops against the background of a crack in the heart vessel, localized near an atherosclerotic plaque. A blood clot forms in the coronary arteries, interfering with normal blood flow.
- Vasospastic angina. The disease manifests itself as local spasms in the heart arteries. The reason for the development of this pathology is the failure of oxygen delivery to the myocardium. As a result, a spasm develops, which characterizes angina pectoris. A similar illness can occur at rest.
Symptoms
Manifestations occur when the lumen of the artery is blocked by 70% or more. Blood supply drops significantly, hemodynamics are disrupted. An attack is difficult to confuse with other processes.
Symptoms of unstable angina are determined from the nervous and cardiovascular systems:
- Intense pain in the chest on the left side. It radiates to the arm, shoulder blade, back or lower back. The duration corresponds to the length of the episode. Relief is carried out with analgesic drugs.
- Dyspnea. Against the background of physical activity. And if the pathological process has been going on for a long time, then even in a state of complete rest.
- Dyspeptic phenomena. Heartburn, nausea, vomiting, abdominal pain. They arise as a consequence.
Unstable angina in rare cases can be mistaken for an ulcer or other gastroenterological processes.
The duration of the episode is about 10-30 minutes or a little more. It goes away on its own if there is no heart attack.
Symptoms in men and women
The main symptom of an angina attack is sudden pain in the chest, and people describe this condition in different ways. Some complain of a burning sensation and aching pain radiating to the left arm .
Others feel bursting pain radiating under the shoulder blade or in the stomach, neck, and throat. The attack most often lasts no more than 15 minutes and goes away on its own or after taking nitroglycerin . If this condition does not go away, it may mean that an acute myocardial infarction has occurred.
Angina pectoris most often manifests itself when:
- fast walking;
- climbing stairs;
- excitement;
- going out into the cold;
The most severe exacerbation of angina occurs during physical activity immediately after a heavy meal.
Angina can also manifest itself at rest, for example, during night sleep. This occurs as a result of spasms of the coronary vessels passing along the surface of the heart. This form of angina is called “angina at rest,” which is considered a more severe manifestation of the disease.
Similar pain sensations can also occur with neuroses, chondrosis of the upper spine, heart defects, diseases of the lungs or gastrointestinal tract, and myocardial infarction.
During attacks, nonspecific symptoms of cardiac angina may appear: nausea, vomiting, muscle weakness, excessive sweating, dizziness, panic.
Severe sudden pain in the heart area can occur in young men in the early morning or at night . Spasm of the vessels supplying the heart muscle does not always occur as a result of atherosclerosis. This type of angina is called vasospastic or Prinzmetal's angina.
Women are less likely to experience shortness of breath or pain radiating to the arm during attacks . More often they experience sensations in the form of pulsation or tingling, nausea, and pain in the abdominal area. The most common complaints in men are sharp pains in the heart that radiate to the shoulder blade or arm.
First aid
Initial methods of prehospital care require mandatory adherence to a clear algorithm:
- Call a team of doctors.
- Measure blood pressure and heart rate (HR).
- Make the patient sit down. Place a cushion under your back. You can use a blanket or clothes. This position will ensure adequate blood circulation in the cardiac structures and prevent the development of a heart attack.
- Give prescribed medications. If the patient has visited a cardiologist before, there are probably recommendations for pre-medical care measures.
If you have angina for the first time, you cannot use medications on your own; the body’s reaction is unknown and can only make things worse. Death is the most likely outcome of self-medication during an attack.
- Open a window or vent to ensure fresh air flows into the room. Oxygen is necessary to relieve the most serious consequences of unstable angina: hypoxia and hemodynamic abnormalities.
- Measure your blood pressure again, calculate PP (lower systolic minute indicator), and estimate your heart rate.
If you lose consciousness, turn your head to the side, release your tongue, try to bring the patient to his senses using ammonia (ammonia solution).
You need to act quickly, but primary measures do not replace qualified recovery in a hospital.
Classification
There are several subgroups of unstable angina:
- New-onset angina - the first symptoms of the disease appeared a couple of months ago.
- Progressive angina - painful attacks increase in severity, the condition constantly worsens without proper treatment.
- Vasospastic angina is another name for spontaneous angina. The clinical picture in this case is not caused by any external stimuli and occurs in absolute silence and peace.
- Post-infarction angina - within two to three weeks after a myocardial infarction, pain and shortness of breath return, which indicates the progression of coronary heart disease (CHD). Danger of recurrent heart attack.
Diagnostics
Management of patients with coronary insufficiency (a particular type is unstable angina) is the task of a specialized doctor.
If there is suspicion, it makes sense to hospitalize the person for a short time; this is the most correct decision, because the patient’s life is at stake. The next episode could be the last.
Scheme of events:
- Oral interview with the patient. The complaints are typical, which allows us to draw conclusions almost immediately.
- Anamnesis collection. Data for organic pathologies is also on the surface. This is the path to identifying the origin of a process.
- Measurement of blood pressure, heart rate.
- Listening to heart sounds. The tones are dull and irregular. Violations worsen the prognosis.
- Daily monitoring using an automatic Holter device.
- Electrocardiography. Specific functional signs on the ECG include widening of the QRS complex, premature appearance of the P wave, doming of the ST segment, and many others. The interpretation is carried out by a cardiologist and diagnostic specialist. Errors may occur.
- Echocardiography. To determine organic changes and defects.
- MRI or CT.
- Angiography of the coronary arteries.
This is enough for the system. It is possible to involve third-party specialists as part of advanced diagnostics if there is no evidence of cardiac sources of the problem.
Treatment
The therapy is mixed, the prevailing technique depends on the stage and nature of the phenomenon.
Medication methods include the use of the following drugs:
- Antihypertensive. Calcium antagonists, beta blockers and ACE inhibitors. All of them are aimed at solving one problem - lowering blood pressure and dilating blood vessels.
- Statins. Against the background of early stages of atherosclerosis. Eliminates cholesterol deposits. There are numerous names, the selection is carried out by a doctor. There are a lot of side effects, self-administration is excluded.
- Antithrombic. Restores the rheological properties of blood. Mainly fluidity. Aspirin is preferred.
Drug treatment of unstable angina is effective at stages 1-2 of the pathological process. Later, this is maintenance therapy against the background of the main method of the surgical plan. Also, drugs can be used during the preparatory period to reduce risks.
Surgical assistance is required in most advanced cases. Coronary bypass surgery is performed (creating a bypass route for blood circulation), as well as vascular plastic surgery, if there is still a chance to restore the normal functioning of the artery.
The effectiveness of a particular method depends on the specific situation; there are no universal recipes. Therefore, the qualifications of the treating cardiac surgeon play a great role.
All the described methods are effective if there are no significant violations on the part of the heart itself. Organic transformations worsen the outcome.
It also makes sense to change your lifestyle. This is especially important in the early stages, there is a chance of completely eliminating the process using non-radical methods.
Among the measures:
- Quitting bad habits. Not a drop of alcohol is allowed, cigarettes are completely excluded.
- Diet correction. Treatment tables No. 3 and No. 10, further at your own discretion.
- Healthy sleep 8 hours per night.
- Physical activity at a minimum level (walking, swimming, cycling, exercise therapy).
Treatment measures are complex, and recovery requires effort on the part of doctors and the patient himself. The chances are not obvious even with an integrated approach.
Treatment methods for angina pectoris
We looked at first aid and symptoms of angina in women.
Medicines for the treatment of this disease are primarily intended to stop attacks, reduce their frequency and number, and also to prevent the development of myocardial infarction.
In addition to Nitroglycerin, drugs are prescribed to reduce thrombosis:
- "Aspirin".
- "Clopidogrel".
Medicines that reduce oxygen deprivation:
- "Bisaprolol."
- "Metoprolol."
- "Atenolol."
Statins are also used:
- Atorvastatin.
- "Simvastatin".
Not only drug treatment relieves the symptoms of angina pectoris in women. Treatment with folk remedies receives quite good reviews.
Prognosis and possible complications
Possible consequences are:
- Myocardial infarction. The most common option and the main cause of death in patients with coronary insufficiency.
- Heart failure.
- Cardiogenic shock. Fall in blood pressure and blood output.
- Stroke. Acute malnutrition of cerebral structures with the development of deficiency phenomena in parts of the brain. It poses a great danger to life, and on the other hand, even complete restoration of functions does not guarantee the absence of defects in higher nervous activity.
Prognostic assessments are determined by the severity of the process and its nature. Also neglect.
Favorable moments:
- Early start of treatment.
- Good response to therapy.
- Youth.
- No bad habits, no family history, no obesity.
- Minimum somatic pathologies.
The probability of heart attack and death over a period of 1-3 years without treatment is 60-80%, with supervision - 20%. Radical elimination of the process is associated with a better outcome, complete recovery is possible.
Causes of angina pectoris
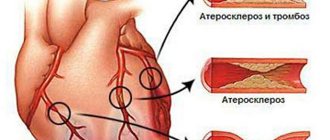
Perhaps the main cause of angina is the narrowing of the lumen of the coronary arteries (their spasm), which occurs against the background of pathological processes in these arteries. As a result of the spasm, a discrepancy appears between the myocardial need for oxygen and its delivery. The most common (92%) pathological process - the cause of arterial spasm - is atherosclerosis, sometimes it can be combined with thrombosis. Another cause of stenosis may be a dysfunction of the endothelium (inner lining) of blood vessels.
Rice. 1. Causes of narrowing of the coronary arteries.
In recent years, researchers have identified risk factors that can lead to coronary atherosclerosis. All of them are divided into 3 main groups.
Group 1 – lifestyle.
The risk factors of this group are modifiable, i.e. changeable:
- a diet high in cholesterol (egg yolks, caviar, cheeses, margarine, pork, etc.);
- smoking;
- excessive alcohol consumption;
- low physical activity (hypodynamia).
Group 2 – physiological characteristics , which are also modifiable characteristics:
- increased level of total cholesterol in the blood plasma (normally it should be 3.6-5.2 mmol/l);
- high blood pressure;
- low levels of “good” cholesterol (HDL cholesterol);
- increased level of triglycerides in the blood plasma (normal – less than 1.7 mmol/l);
- diabetes;
- obesity.
Group 3 – personal characteristics (non-modifiable factors):
- age (over 45 years for men and 55 years for women);
- male gender;
- family history of atherosclerosis.
The combination of several risk factors significantly increases the likelihood of developing atherosclerosis and, as a consequence, coronary artery disease and its form – angina pectoris. Today, IHD is the main cause of mortality in the population. According to the State Scientific Research Center (State Research Center) for Preventive Medicine in Russia, about 10 million of the working population suffer from coronary artery disease. It must be borne in mind that angina pectoris as the onset of coronary artery disease occurs in almost 50% of patients. Moreover, about 40-50% of these people are aware of the disease they have, while 50-60% of cases of the disease remain unrecognized and untreated. It is for these reasons that it is very important to recognize angina pectoris in time and seek help from a doctor.