Processing of statistical data of myocardial infarction in Orenburg
It is known that MI is one of the most common causes of death.
Experts estimate that approximately 4.3 million people die from it every year. If we convert this data into a percentage, we get 48% of all causes of death. Today, mortality tends to decrease, because many modern medications have appeared, balloon coronary angioplasty is being performed, but still, the problem does not become less urgent, because the standard of living is falling, leading to an increase in the number of heart diseases, and surgical intervention Not shown to everyone.
The most common attack occurs in men; their number is 50 times higher than in women, if we take into account the age category of 35-50 years (working age).
Representatives of the fair half of humanity are at greatest risk upon reaching the age of 50, because in this case hormonal disorders play a role, which are considered good soil for the development of MI.
It is also worth considering the fact that attacks in women more often end in death than in men. In the first case, death is observed in 53% of attacks, in the latter - only 43%.
Ponomareva E. A., Ametova E. I. Processing of statistical data of myocardial infarction in Orenburg // Young scientist. - 2020. - No. 4. — P. 292-295.
In this work the myocardial infarction is considered statistically these diseases. Cardiovascular diseases are the main cause of death around the world for any other reason so many people don't die.
Keywords: cardiovascular diseases myocardial infarction, organizational aspects of medical care, on an outpatient basis, crews of SMP, high mortality, rehabilitation, complications.
This disease occupies one of the leading places not only in our country, but throughout the world, especially in developed countries. More than one million Russians die annually from cardiovascular diseases, of which 634 thousand were diagnosed with acute myocardial infarction.
According to the Russian Scientific Cardiology Center, mortality from cardiovascular diseases has increased by 82% among people aged 20 to 24 years over the past 14 years, by 63% among 30-35 year olds over the same period. Cardiovascular diseases are the leading cause of death worldwide: for no other reason do more people die each year than from cardiovascular diseases [1].
Considering the high prevalence of myocardial infarction, it is necessary to provide medical care to such patients at all stages of medical care (starting from the pre-hospital stage in providing care to patients and ending with preventive measures). The work of nursing staff is also important here.
The purpose of our study is to study the disease myocardial infarction and determine the organizational aspects of providing care to these patients.
Acute myocardial infarction (MI) is an acute disease caused by the development of necrosis in the heart muscle as a result of a violation of its blood circulation, which occurs as a result of thrombosis of the coronary artery or its sharp narrowing by an atherosclerotic plaque. In very rare cases, disruption of coronary blood flow occurs as a result of spasm of an unaffected coronary artery [2].
The work uses statistical data from the annual report of the State Autonomous Institution “GKB im. N.I. Pirogov" Orenburg for 2012, 2013, 2014.
Research methods.
- Working with archival and reporting materials.
- Statistical processing of material.
Having analyzed the morbidity patterns of patients who suffered myocardial infarction
The number of patients admitted to the cardiology department of the State Autonomous Institution of Clinical Hospital named after. N.I. Pirogova.
Table 1
| Year | 2012 | 2013 | 2014 |
| Number of applicants | 1732 | ||
| 1817 | 1539 |
According to the journal, we found that in 2014 at the State Autonomous Institution of the City Clinical Hospital named after. N.I. Pirogov, 1539 patients were admitted to the cardiology department, which is 378 people less than in 2013 (1917 patients) and 193 people less than in 2012 - 1732 patients, this is for similar periods of time. We believe that this is explained by reasons that show that for some patients, highly specialized care was provided on an outpatient basis and at home by EMS cardiology teams.
table 2
| Diseases/year | 2012 | 2013 | 2014 | |||
| Total | % | Total | % | Total | % | |
| Acute myocardial infarction | 117 | 6,81 | 158 | 8,69 | 201 | 3,06 |
| IHD | 634 | 36,6 | 565 | 31,09 | 602 | 39,13 |
| hypertonic disease | 447 | 25,8 | 457 | 25,18 | 311 | 20,2 |
| Rheumatic heart defects | 19 | 1,09 | 54 | 2,97 | 65 | 4,22 |
| Unstable angina | 324 | 18,7 | 329 | 18,10 | 203 | 13,19 |
| Other heart diseases | 190 | 10,96 | 254 | 13,97 | 157 | 10,20 |
| Total: | 1732 | 100 % | 1817 | 100 % | 1539 | 100 % |
From the data in Table 2 it is clear that the incidence of myocardial infarction is increasing every year. This is also due to the fact that since 2014, the cardiology department of the GAUZ City Clinical Hospital named after. N.I. Pirogov became known as the cardiovascular department. The number of patients with this disease has increased.
The incidence of myocardial infarction and, accordingly, the levels of socio-economic losses increase with increasing age of the population, since myocardial infarction in elderly patients develops against the background of already existing organic and functional changes in the heart and blood vessels of an age-related nature [3].
This can be clearly seen in Table No. 3
Distribution of myocardial infarction by age group for 2012–2014.
Table 3
| Age | 30–40 | 40–50 | 50–60 | 60–70 | 70–80 | Total |
| Quantity | 7 | 25 | 51 | 184 | 209 | 476 |
| Total % | 1,4 | 5,2 | 10,7 | 38,6 | 21,6 | 100 % |
Table 4
Distribution of myocardial infarction by gender for 2012–2014.
| Age | 30–40 | 40–50 | 50–60 | 60–70 | 70–80 | Total |
| men | 2 | 19 | 62 | 95 | 102 | 280 |
| women | — | 8 | 40 | 56 | 92 | 196 |
From table No. 4 we see that men are more likely to encounter this disease than women, since women are protected by female hormones until a certain time (before menopause).
Having studied the structure of the incidence of myocardial infarction, we can conclude that the incidence is typical not only for people over 60 years of age, but also occurs in adulthood. The incidence is more common in men than in women; this can also be explained by the fact that men have more bad habits, which are predisposing factors for the disease. Women suffer less often, because until a certain age (before menopause), they are protected by female hormones [4].
Recommendations:
- Providing medical care to patients with myocardial infarction at the pre-hospital stage should be carried out according to clear algorithms of action for medical staff.
- Increasing the professional level of training of medical personnel.
- support and encourage the patient’s desire for recovery in the current clinical situation;
be patient and correct when performing intimate procedures;
- take into account the level of personal maturity of the patient;
- speak a language he understands;
observe the principle of informed consent: explain the significance of the treatment procedure, aim for positive results;
- help the patient become an active participant in the treatment process [5].
Literature:
- Mortality from acute myocardial infarction (epidemiological study based on programs, Gafarov V.V., Blaginina M.Yu. //WHO Register of Acute Myocardial Infarction", MONICA). Cardiology.-2012.-T.5.-P.49–50.
- Baranovsky V.A., Bannikov E.A. Nurse's Directory. - 2012.-p. 207
- Regulatory documents//Chief nurse. - No. 12, - 2010, - P. 117.
- Karpov Yu. A., Sorokin E. V. Stable coronary heart disease: strategy and tactics of treatment. - M.: Reafarm, 2011. - 244 p. 19.
- New opportunities in the treatment of stable angina: recommendations of the European Society of Cardiology, Karpov Yu. A. //Siberian Medical Journal (Irkutsk).-2013.-T.122.-S.UDC: 616.1
Key terms (automatically generated): myocardial infarction, myocardial infarction, myocardial infarction data, prevalence of myocardial infarction, myocardial infarction with each, myocardial infarction diseases, acute myocardial infarction, incidence of myocardial infarction, distribution of myocardial infarction, incidence of myocardial infarction, acute th myocardial infarction, myocardial infarction in the elderly, patients with myocardial infarction, cardiovascular diseases, patient care, coronary artery, cardiovascular diseases, patient care, coronary artery thrombosis, unaffected coronary artery.
extra_toc
Myocardial infarction: statistics, pathogenesis, definition Diagnosis of myocardial infarction Differential diagnosis of myocardial infarction Laboratory tests for myocardial infarction Instrumental studies for myocardial infarction Risk assessment Emergency care for heart attack Thrombolysis Coronary angioplasty and coronary artery bypass grafting Anticoagulants Beta-blockers Inhibitors ACE Calcium antagonists Magnesium sulfate Correction of hyperglycemia Antiarrhythmics means Intra-aortic balloon counterpulsation Inotropic agents Cocaine myocardial infarction Unresolved issues
According to statistics, the incidence of acute myocardial infarction among the male population over the age of 40 varies in different regions of the world from 2 to 6 per 1000 population. Myocardial infarction is the leading cause of death in North America and Europe. In the United States, more than 500,000 people die from ischemic heart disease every year.
More than 1 million heart attacks occur in the United States each year. Approximately 200,000 - 300,000 patients die from myocardial infarction in the prehospital stage. In the United States, every 29 seconds someone has a myocardial infarction, and every minute one patient dies from it. The overall mortality rate from myocardial infarction, including prehospital mortality, is 45%.
However, over the past 30 years, with the advent of intensive care units, thrombolysis, and balloon coronary angioplasty, morbidity and mortality have decreased. Thrombolysis has reduced mortality in myocardial infarction, but it is not indicated for many. Most patients cannot be quickly transported to a clinic where emergency coronary angioplasty is performed.
Forecast
Myocardial infarction can be complicated by diseases of varying severity; therefore, MI most often gives a conditionally unfavorable prognosis. The worst consequences are expected in the case of extensive heart attacks, when large areas of the heart muscle are affected. So-called microinfarctions can be carried on the legs, but this does not mean that such patients are not in danger. Most likely, arrhythmias may appear over time. Therefore, it is extremely important to carry out timely treatment of MI, especially in the form of thrombolytic therapy, after which the prognosis of the disease significantly improves.
Video: What are the chances of survival after a major myocardial infarction?
Heart attack | Medical encyclopedia | Medicine in Novosibirsk
Myocardial infarction is the most severe manifestation of coronary heart disease. A heart attack is a cardiovascular accident that leads to the death of any part of the heart muscle. The death (necrosis) of part of the myocardium occurs as a result of an acute cessation of blood supply and, accordingly, oxygen starvation of the heart tissue.
Myocardial necrosis
Myocardial necrosis is an irreversible process; a scar subsequently forms at the site of damage. This leads to the fact that the heart will never be able to perform its function at the same level.
Main symptoms of a heart attack
The clinical manifestations of a heart attack are severe pressing pain behind the sternum, which can radiate to the left arm, shoulder, or jaw. Pain is usually accompanied
- feeling of lack of air.
A characteristic sign is that the pain does not go away when taking nitroglycerin. Factors that can provoke a disaster include heavy physical activity, emotional stress, and stress.
Myocardial infarction - statistics
Myocardial infarction is a life-threatening condition. According to world statistics, the prehospital mortality rate is at least 50%, that is, the disease progresses so quickly that every second patient dies before the doctors arrive. Complications, both early and late, are also very dangerous - they account for another 30% of deaths.
The basis of heart disease
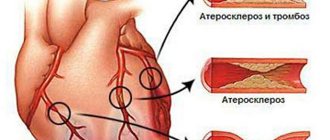
It is well known that the basis of coronary disease is the process of atherosclerosis, that is, the deposition of cholesterol on the walls of blood vessels. Cardiologists have reliably identified risk factors for the aggressive course of atherosclerosis, and, accordingly, such a serious complication as myocardial infarction. All these factors are divided into two fundamental groups: those that can be changed and those that cannot be changed.
The second group includes male gender (the likelihood of developing IHD in men is approximately 2 times higher than in women), age (over 55 years for men and over 60 years for women), family history (presence of strokes in close relatives in the direct line, heart attacks, hypertension in middle age). These factors are beyond our control and cannot be changed. We can and should influence other risk factors.
Atherosclerosis
In diabetes mellitus, atherosclerosis progresses rapidly, and cardiovascular diseases develop at a younger age. Myocardial infarction in diabetics can be painless, and changes are found only on the ECG (this is a painless form of heart attack). With normal blood glucose levels (less than 5.
Prevention of heart disease
Considering the high prevalence of coronary artery disease, its severe complications and high mortality, the prevention of cardiovascular diseases is a priority. Myocardial infarction is easily suspected by severe pain in the chest. The first research method to confirm a heart attack is electrocardiography.
Already in the first minutes, changes characteristic of myocardial damage appear on the ECG. They indirectly indicate the depth of the lesion and the area of the affected area. Sometimes these changes appear only after a few hours. Echocardiography allows you to clarify the structural changes that have occurred and assess the contractility of the heart.
Treatment
There are two approaches to the treatment of this disease - conservative, that is, treatment with drugs (the predominant method in Russia for a number of reasons) and surgical (which has become widespread in developed countries). In the first case, the patient is given special medications that can dissolve the blood clot that has blocked the vessel (this is only possible in the first hours from the onset of the disease).
Surgical methods for treating coronary artery disease can completely restore blood flow in the vessel. If the operation is performed in the first hours, there is a chance that myocardial necrosis will not have time to develop and the chances of cure are maximum. Among the operations used are balloon angioplasty and coronary artery bypass grafting. In severe heart attacks and the presence of early complications, contraindications to surgical treatment are often identified.
Consequences of necrosis
You can notice the consequences almost immediately. They significantly influence the worsening development of pathology, having a negative impact on the general condition of the patient’s body.
Complications of myocardial infarction 1st period
The first 72 hours are characterized by the development of arrhythmias: ventricular fibrillation is the most dangerous consequence of a heart attack, which can lead to death. Heart rhythm disturbances in the late period are typical for 40%. Moreover, in the early stage this happens in one hundred percent of cases.
- Left ventricular heart failure is characterized by wheezing, asthma of cardiac origin, and the likelihood of developing pulmonary edema. The most significant consequence is cardiogenic shock, causing the death of the patient. In this case, the pressure drops to 80 mmHg and below. The patient is prone to loss of consciousness, cyanosis and tachycardia occur. The development of acute heart failure is typical for 50% of cases in the early period.
- Blood can flow into the pericardial area - this is caused by rupture of muscle fibers in the area of infarction necrosis. This pathology is called cardiac tamponade.
- A small (two to three) percentage of patients suffer from pulmonary thrombosis. This is an extremely dangerous complication leading to unexpected death.
- Eight percent of heart attacks result in mental disorders.
- Heart attacks are characterized by the formation of intestinal and stomach ulcers. This is possible in 5% of situations.
- Acute cardiac aneurysm. Upon transition to the chronic stage, heart failure is likely to develop in 12% of cases.
Complications of myocardial infarction, period 2
Is it possible to change statistics
Statistics are simply numbers that reflect the situation at a given moment. They can be changed if people begin to take their health more responsibly.
The first step is to determine how high the risk of developing MI is in a particular person. In order to assess the situation objectively, you need to take into account the following factors:
- gender and age of the person;
- hereditary characteristics;
- presence of heart disease;
- excess weight;
- blood cholesterol levels;
- smoking or alcohol abuse;
- poor nutrition;
- a sedentary lifestyle or vice versa – systematic exposure of the body to excessive physical activity;
- features of the emotional background, frequency of stressful situations.
The presence of all these indicators makes it possible to assume the development of MI in 90% of cases in men. As for women, for them this figure will be 94%.
At the same time, the likelihood of developing a myocardial infarction, as statistics show, largely depends on the gender, age of the patient, as well as on his heredity.
These are the main indicators by which the degree of risk can be determined. Smoking comes next. Its share is 35% of the total number of reasons. Next are stressful situations, they take 32%.
If all of these factors are present together, the risk of developing a heart attack increases three times, if not more.
Speaking of death, the likelihood of its occurrence is also assessed taking into account several conditions:
- the presence of all or most risk factors;
- type of attack and timeliness of first aid;
- compliance with the rules of the rehabilitation period.
The last period is very important for a person with heart disease. Statistics of the disease of myocardial infarction show that in the first year after the first attack, just during this period of rehabilitation, relapses most often occur. They account for 40% of the total number of cases.
The success of recovery and the risk of recurrent MI depend only on the correct selection of rehabilitation procedures and on the patient’s compliance with the doctor’s recommendations.
General data for European countries, collected by professional doctors, is provided. As for the statistics of heart attacks in Russia, they are not particularly different here. Mortality accounts for 40% of the total number of recorded cases. The indicator can be reduced if you seek medical help in a timely manner.
Important to knowImportant to know! Studies have shown that in most cases an ambulance is called within 50 minutes or more. Sometimes professional help is sought after 10 hours.
This is due to little awareness of this attack and the inability to immediately and accurately determine it. And in order for the statistics of myocardial infarction in Russia to become more comforting, everyone should know about the peculiarities of their manifestation.
What is the prognosis of a patient with a heart attack and how to influence it
The general prognosis in the post-infarction period is calculated separately for each patient, since additional data from the comorbid background and individual characteristics are taken into account.
Modern methods of diagnosis and emergency care increase survival after a heart attack to 90% during the first year.
To improve the prognosis on their own, patients are recommended to:
- monitoring the course of the disease with regular examinations and additional studies;
- Seeing a doctor if new symptoms appear;
- lifestyle changes;
- systemic medication (for the treatment of hypertension, arrhythmia, prevention of lipid disorders and thrombus formation).
After an MI, lifelong treatment and rehabilitation are required to prevent complications and the development of pathologies in other organs and systems.
Correction of risk factors
The death of a patient in the early or late post-infarction period is largely determined by risk factors for the development of complications or recurrent MI.
In order to prevent and increase life expectancy, it is recommended:
- lifestyle modification: adequate physical activity, giving up bad habits and balanced nutrition;
- weight normalization using non-drug methods. If ineffective, pharmacological agents are prescribed;
- control of blood pressure indicators;
- avoidance of stressful situations;
- systemic intake of prescribed drugs.
Treatment of concomitant pathologies
Injuries, infectious and endocrine diseases aggravate the course of coronary heart disease, so control and adequate treatment of concomitant pathologies affects the prognosis for the patient. Mandatory correction is required:
- diabetes mellitus - glucose level monitoring is carried out in a cardiology hospital to take into account the risk of complications and prescribe treatment;
- myocarditis – inflammation of the muscle mass of the heart worsens the course of the post-infarction period with the development of rhythm disturbances and decreased contractile function;
- kidney disease - impaired excretion of fluid from the body, disorders of hormone synthesis lead to damage to the vascular wall, increased blood pressure;
- pathologies of the thyroid gland (Hashimoto's goiter, diffuse toxic goiter and others).
Traumatic brain injuries with damage to the medulla oblongata (this is where the center for regulating vascular tone and cardiac activity is located) worsens the prognosis for rehabilitation after a heart attack.
Signs of MI and first aid
The first signs that should cause concern and become a reason for providing first aid will be:
- pain behind the sternum, the nature of which is quite difficult for a person to determine. They quickly change in intensity and manifestation, they can be sharp, cutting, squeezing;
- shortness of breath - it is manifested by a lack of air even in the absence of physical activity, accompanied by blanching of the skin and mucous membranes;
- dizziness – often leads to fainting, accompanied by tachycardia or loss of pulse.
If these symptoms occur, an ambulance should be called immediately.
Then start providing first aid. First, you will need to give the patient a nitroglycerin tablet, which will help relieve pain. Then you need to put the person to bed and unbutton the collar. Open the vents, windows, turn on the air conditioner.
If the pain persists, repeat taking nitroglycerin, but do not take more than 3 tablets. If all else fails, inject analgin. Give aspirin. The future prognosis depends on these measures.