Features of the phenomenon
Nature has programmed that the heart rate is set by the sinus node. The pulses travel through a conductive system that branches along the walls of the chambers. The atrioventricular node is located in the system that conducts impulses below the sinus node in the atrium.
The task of the atrioventricular node is to reduce the speed of the impulse when transmitting it to the ventricles. This occurs so that ventricular systole does not coincide in time with the contraction of the atria, but follows immediately after their diastole. If disturbances occur in the creation of heart rhythms for various reasons, then the atrioventricular node is able, in a sense, to take on the mission of setting the heart rhythm. This phenomenon is called atrioventricular nodal rhythm.
In this case, the heart, under the guidance of impulses from the atrioventricular system, contracts 40 ÷ 60 times per minute. Passive impulses last for a long period. Atrioventricular nodal rhythm of the heart is detected when six or more beats are observed, defined as the next replacement contractions of the heart. How the impulse emanating from the atrioventricular node is triggered: it passes with a retrograde movement upward to the atria and a natural movement downward, affecting the ventricles.
The rhythm according to ICD-10 is classified depending on the problems that caused the atrioventricular rhythm: 149.8.
Observations show that circulatory disorders during atrioventricular rhythm occur if the heart beats per minute are less than forty or more than one hundred and forty beats. The negative manifestation is reflected in insufficient blood supply to the heart, kidneys, and brain.
Symptoms of ectopic rhythm
The clinical picture of replacement heart rhythms can be clearly expressed or not manifested at all. Usually, the symptoms of the underlying disease come first in the clinical picture, for example, shortness of breath on exertion, attacks of burning pain in the chest, swelling of the lower extremities, etc. Depending on the nature of the ectopic rhythm, the symptoms may be different:
- With ectopic atrial rhythm , when the source of impulse generation is located entirely in one of the atria, in most cases there are no symptoms, and disturbances are detected by the cardiogram.
- With a rhythm from the AV junction, a heart rate close to normal is observed - 60-80 beats per minute, or below normal. In the first case, no symptoms are observed, but in the second, attacks of dizziness, a feeling of lightheadedness and muscle weakness are noted.
- With extrasystole, the patient notes a feeling of fading, cardiac arrest, followed by a sharp jolt in the chest and a further absence of sensations in the chest. The more often or less often the extrasystoles, the more varied the symptoms in duration and intensity.
- With atrial bradycardia , as a rule, the heart rate is not much lower than normal, within 50-55 per minute, as a result of which the patient may not notice any complaints. Sometimes he is bothered by attacks of weakness and sudden fatigue, which is caused by a reduced flow of blood to the skeletal muscles and brain cells.
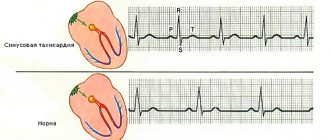
- Paroxysmal tachycardia manifests itself much more clearly. During paroxysm, the patient notes a sharp and sudden sensation of accelerated heartbeat. According to many patients, the heart flutters in the chest like a “hare’s tail.” The heart rate can reach 150 beats per minute. The pulse is rhythmic, and may remain around 100 per minute, due to the fact that not all heartbeats reach the peripheral arteries at the wrist. In addition, there is a feeling of lack of air and chest pain caused by insufficient oxygen supply to the heart muscle.
- Atrial fibrillation and flutter can be paroxysmal or permanent. The basis of atrial fibrillation is a chaotic, non-rhythmic contraction of different parts of the atrium tissue, and the heart rate in the paroxysmal form is more than 150 per minute. However, there are normo- and bradysystolic variants, in which the heart rate is within the normal range or less than 55 per minute. The symptoms of the paroxysmal form resemble an attack of tachycardia, only with an irregular pulse, as well as a feeling of irregular heartbeat and interruptions in heart function. The bradysystolic form may be accompanied by dizziness and lightheadedness. With a permanent form of arrhythmia, the symptoms of the underlying disease that led to it come to the fore.
- Idioventricular rhythm is almost always a sign of serious cardiac pathology, such as severe acute myocardial infarction. In most cases, symptoms are noted, since the myocardium in the ventricles is capable of generating electricity at a frequency of no more than 30-40 per minute. In this regard, the patient may experience Morgagni-Edams-Stokes (MES) episodes - attacks of loss of consciousness lasting several seconds, but no more than one or two minutes, since during this time the heart “turns on” compensatory mechanisms and begins to contract again. In such cases, they say that the patient is “massing.” Such conditions are very dangerous due to the possibility of complete cardiac arrest. Patients with idioventricular rhythm are at risk of developing sudden cardiac death.
Shapes and types
Atrioventricular rhythm occurs:
- Accelerated AV nodal rhythm - contractions per minute within 70 ÷ 130 beats. The disorder occurs as a result of: myocarditis,
- glycoside intoxication,
- rheumatic attack,
- myocardial infarction,
- heart operations.
- negative reaction to taking medications,
AV rhythm occurs in the following manifestations:
- when atrial excitation occurs first,
- the ventricles and atria receive impulses at the same time, and their contraction also occurs at the same time.
Read below about the reasons for the appearance of ectopic and other types of AV nodal rhythm.
Diagnosis of ectopic rhythm
The leading diagnostic method is the electrocardiogram. If an ectopic rhythm is detected on the ECG, the doctor should prescribe a further examination plan, which includes cardiac ultrasound (ECHO-CS) and daily ECG monitoring. In addition, patients with myocardial ischemia are prescribed coronary angiography (CAG), and patients with other arrhythmias are prescribed transesophageal electrophysiological examination (TEPE).
ECG signs for different types of ectopic rhythm differ:
- With an atrial rhythm, negative, high, or biphasic P waves appear, with a right atrial rhythm - in additional leads V1-V4, with a left atrial rhythm - in V5-V6, which may precede or overlap the QRST complexes.
accelerated ectopic atrial rhythm
- The rhythm from the AV junction is characterized by the presence of a negative P wave, superimposed on the QRST complexes, or present after them.
AV nodal rhythm
- Idioventricular rhythm is characterized by a low heart rate (30-40 per minute) and the presence of altered, deformed and widened QRST complexes. There is no P wave.
idioventricular (ventricular) ectopic rhythm
- With atrial extrasystole, premature, extraordinary, unchanged PQRST complexes appear, and with ventricular extrasystole, altered QRST complexes appear followed by a compensatory pause.
atrial and ventricular ectopia (extrasystoles) on the ECG
- Paroxysmal tachycardia is characterized by a regular rhythm with a high frequency of contractions (100-150 per minute), P waves are often quite difficult to determine.
- Atrial fibrillation and flutter on the ECG are characterized by an irregular rhythm, the P wave is absent, and fibrillation f waves or flutter waves F are characteristic.
Causes of atrioventricular nodal rhythm
The atrioventricular node is involved in creating rhythm under the following circumstances:
- If sinus rhythm does not enter the atrioventricular node. This may occur due to: sinoauricular block,
- the sinus node does not cope with its function,
- atrioventricular block;
- arrhythmia with slow sinus rhythm - bradycardia,
- if impulses from ectopic foci located in the atrium do not have the opportunity to enter the atrioventricular node.
- myocarditis,
- morphine
Elena Malysheva’s video will tell you about the reasons for the appearance of AV rhythm in a child:
Concept
This disease is considered a rare form of rhythm disorder. In such a situation, the generation of electrical signals occurs not in the sinus node, but in the atrioventricular node. This area is capable of generating fewer impulses than in the normal state. This causes the heart to beat about forty times per minute.
The generation of impulses occurs in different parts of the node, on which the work of the heart and its contractions depend. If this occurs in the upper parts of the node, then the heart beats about eighty times per minute. If the place where the electrical signals occur is lower, the heart slows down.
After production, the signal enters the atria and ventricles. If they appear at the bottom of the node, they first penetrate the ventricular myocardium and cause their contraction. This is not a normal condition, since the excitation must first reach the atria. If the upper part of the atrioventricular node is responsible for generating the impulse, then the atria contract first. The nodal rhythm is characterized by the penetration of impulses along the retrograde path.
If the problem arose in a child whose vagal tone has increased, then the generation of excitation does not always occur in the area of the atrioventricular node. It can enter the sinus node, and from it back into the AV.
Symptoms
The manifestation of atrioventricular rhythm coincides with the symptoms of the arrhythmia that initiated the occurrence of this problem. The severity of the condition depends on how severe the manifestations of the underlying disease are.
There are three main signs:
- the first heart sound has an amplified tone,
- There is a noticeable pulsation in the neck veins,
- bradycardia, which has the correct rhythm (number of contractions per minute: 40 ÷ 60 beats).
With prolonged atrioventricular rhythm, heart disease may result in:
- heart failure,
- acute conditions associated with Morgagni-Edams-Stokes syndrome,
- fainting,
- angina pectoris.
Atrioventricular rhythm: causes and diagnosis, treatment, prognosis and prevention
Atrioventricular rhythm is a condition characterized by disruption of heart contractions due to the fact that the AV node begins to act as a pacemaker. This pathology occurs in very rare cases. It is provoked by lesions of the heart muscle of various origins.
Concept
This disease is considered a rare form of rhythm disorder. In such a situation, the generation of electrical signals occurs not in the sinus node, but in the atrioventricular node. This area is capable of generating fewer impulses than in the normal state. This causes the heart to beat about forty times per minute.
The generation of impulses occurs in different parts of the node, on which the work of the heart and its contractions depend. If this occurs in the upper parts of the node, then the heart beats about eighty times per minute. If the place where the electrical signals occur is lower, the heart slows down.
After production, the signal enters the atria and ventricles. If they appear at the bottom of the node, they first penetrate the ventricular myocardium and cause their contraction.
This is not a normal condition, since the excitation must first reach the atria. If the upper part of the atrioventricular node is responsible for generating the impulse, then the atria contract first.
The nodal rhythm is characterized by the penetration of impulses along the retrograde path.
If the problem arose in a child whose vagal tone has increased, then the generation of excitation does not always occur in the area of the atrioventricular node. It can enter the sinus node, and from it back into the AV.
Symptoms
It is quite difficult to distinguish the problem from others, since specific manifestations are not observed. The patients do not experience any deterioration in their health. In this state:
- heart rate is slow;
- the pulse is very full;
- amplification of the first tone is heard.
Some cases are accompanied by characteristic manifestations:
- The neck veins pulsate simultaneously with the beats of the heart and pulsation in the area of the radial artery.
- How the pulsation will manifest itself depends on whether the contraction of the ventricles and atria occurs simultaneously or not.
- In some cases, the vena cava moves blood into the liver, causing it to pulsate.
Causes and diagnostic methods
Atrioventricular rhythm can be accurately confirmed on an ECG. This technique allows you to assess the state of the rhythm of contractions and identify failures in this process.
If impulses spread from the upper parts of the node, then excitation first begins in the atria. When the pacemaker is positioned low, the PQ interval is shortened.
During clinical and experimental observations, it is possible to discover that the rhythm began to develop in the wrong place under the influence of pathological processes in the area of the sinus nodes.
Extracardiac nerves have a certain influence on the development of the pathological condition. If the left sympathetic nerve is subjected to irritation, then automaticity develops in the atrioventricular node.
The development of such types of arrhythmias occurs:
- if a person suffers from rheumatism;
- after a heart attack with death of areas near the sinus node;
- after consuming quinidine or digitalis preparations.
Also read: Diagnosis and treatment of threadlike pulse
The pacemaker can migrate. This usually occurs if the source begins to move from the sinus node to the AV node and back.
This type of arrhythmia is characterized by suppression of the automatic functioning of the sinus node.
The impulse is generated in the centers of the second and third order, and until their automaticity stops, the sinus node will not be able to perform its functions normally.
Pacemakers can migrate if the sinus node is damaged, the tone of the vagus nerve has increased, and an infectious process develops in the heart muscle.
The heart can contract not only under the influence of excitation distributed from the sinus node, but also from different parts of the atrioventricular node.
To determine the cause of disorders, in addition to the cardiogram, other methods are prescribed. The patient undergoes ultrasound examination, angiography, and daily monitoring. Using the latter method, it is possible to determine at what time of day the disruption in rhythm occurs. Based on the results of these procedures, the diagnosis is confirmed and the appropriate treatment option is selected.
Treatment
Atrioventricular rhythm is a disease that requires special therapy. Treatment options depend on the underlying cause of this type of arrhythmia.
If the duration of the junctional rhythm is short and sinus bradycardia is observed, then there is no need for therapy.
If the development of junctional rhythm occurs against the background of complete atrioventricular block, is accompanied by significant disturbances in the movement of blood through the vessels and deterioration of the patient’s condition, then they try to achieve relief with medications. If they are ineffective, a device is installed that will generate electrical impulses. This device is called a pacemaker.
Among medications, in the presence of atrioventricular rhythm, they resort to Atropine, Isoprenaline and Orciprenaline. Treatment is carried out in dosages that are used for sinus bradycardia.
When the development of nodal rhythm occurs under the influence of drugs such as digitalis, quinidine and others, then they need to be abandoned.
Patients are categorically not recommended to use Quinidine, Procainamide, Aymalin and beta blockers.
If the patient has increased potassium levels or gastric acidity, then use sodium bicarbonate in an amount of up to three ampoules. This drug is infused into a vein by drip. For half an hour.
After this, 1000 ml of ten percent glucose is administered. It is also infused into a vein by drip over eight hours.
Prognosis and prevention
It is possible to predict what consequences the disease will lead to if you determine the severity of the arrhythmia and diseases that provoked the junctional rhythm, the condition of the heart and blood vessels, and the frequency of ventricular contraction.
If a person is completely healthy, has sinus bradycardia and atrioventricular rhythm appears periodically and not for a long time, then one can count on a favorable outcome.
A more severe situation is observed if the development of junctional rhythm occurred due to complete atrioventricular block, heart disease and organ failure.
If atrial fibrillation occurs and poisoning with digitalis preparations occurs, the consequences will be very serious. If the rhythm frequency is low, then Morgagni-Edams-Stokes syndrome and heart failure develop, which cannot be corrected with medications.
You can reduce the likelihood of developing this disease if you treat infectious diseases in a timely manner, do not use antiarrhythmic drugs without medical supervision, and identify the causes of high vagal tone. At the first signs you need to visit a cardiologist.
Source: https://KardioPuls.ru/bolezni/ritm/atrioventrikulyarnyy/
Treatment
If sinus bradycardia is observed and the junctional rhythm manifests itself for a short time, then this phenomenon is not treated.
In the case when the rhythm disturbance manifests itself clearly and leads to deterioration of blood circulation, then therapeutic procedures are provided.
Therapeutic
Treatment of rhythm disturbances consists of measures that will convert the atrioventricular rhythm to sinus. They treat major diseases and affect the autonomic system.
Healthy habits always help with heart health:
- walks in the open air,
- loads should be moderate,
- quitting cigarettes,
- positive thinking.
Medication
The specialist may prescribe medications:
- isoprenaline - used intravenously, combining the drug with a glucose solution or
- atropine – used intravenously.
Medicines may cause unwanted effects:
- angina pectoris
- decrease in pressure,
- ventricular arrhythmias.
If these medications are not suitable for the patient, then the doctor may use aminophylline intravenously or in tablet form instead.
If, before treating atrioventricular rhythm, drugs that could cause rhythm disturbances were used, they should be discontinued. This:
- digitalis preparations,
- guanethidim,
- quinidine,
- antiarrhythmics
- and others.
Operation
In case of rhythm disturbances caused by serious heart disease, measures are required to restore and maintain the correct heart rhythm. To do this, a simple operation is performed to introduce a pacemaker into the patient’s body.
Folk remedies
You can drink infusions and decoctions of herbs. Prescriptions should definitely be discussed with the doctor who is observing the patient.
Recipe No. 1
In a glass of boiling water, infuse herbs and seeds, taken in equal quantities (20 g):
- goldenrod grass,
- flaxseed (ground),
- motherwort grass,
- valerian root,
- viburnum shoots.
The infusion is drunk in small sips for a month.
Recipe No. 2
Prepare an infusion with components taken in equal quantities (40 g), mixing them with a glass of boiling water:
- lemon balm,
- motherwort grass,
- buckwheat flowers,
- goldenrod grass.
The decoction is drunk in small sips for fourteen days. After a week's break, repeat taking the herbal infusion the same way as the first time.
Treatment of ectopic rhythm
Treatment is not carried out in cases where the patient has an ectopic atrial rhythm that does not cause unpleasant symptoms, and pathologies of the heart, hormonal and nervous systems have not been identified.
In the case of moderate extrasystole, the prescription of sedatives and restorative drugs (adaptogens) is indicated.
Therapy for bradycardia, for example, with an atrial rhythm with a low contraction frequency, with the bradyform of atrial fibrillation, consists of prescribing atropine, ginseng preparations, Eleutherococcus, Schisandra and other adaptogens. In severe cases, with a heart rate less than 40-50 per minute, with attacks of MES, implantation of an artificial pacemaker (pacemaker) is justified.
Accelerated ectopic rhythm, for example, paroxysms of tachycardia and atrial fibrillation-flutter require emergency assistance, for example, the administration of a 4% solution of potassium chloride (panangin) intravenously, or a 10% solution of novocainamide intravenously. Subsequently, the patient is prescribed beta blockers or antiarrhythmic drugs - Concor, Coronal, verapamil, propanorm, digoxin, etc.
In both cases - both slow and accelerated rhythms, treatment of the underlying disease , if any, is indicated.
Disease prevention
In order not to create preconditions for rhythm disturbances with replacement of the influence of the main pacemaker on atrioventricular impulses, you should adhere to the following rules:
- Use medications with caution:
- reserpine,
- digoxin,
- morphine,
- strophanthin,
- antiarrhythmics.
- Promptly treat heart diseases that can cause these disorders,
- Carry out therapeutic and preventive measures to prevent:
- Acidosis - a change in the acid-base balance towards an acidic reaction can cause disturbances in the functioning of the heart. It is necessary to treat diseases that initiate an increase in the acidic environment, select the right diet, using consultations with specialists.
- Hyperkalemia – occurs when there is an increased level of potassium cations in the blood. Potassium is a mineral essential for kidney, heart and overall health. If its content significantly exceeds the required norm, it can cause the risk of heart rhythm disturbances and other problems. This occurs if the body does not cope well with eliminating the substance, or the use of potassium in supplements and medications occurs in doses that exceed the need for this substance.
- Hypoxia is a condition when tissues suffer from a lack of oxygen. The cause of the phenomenon should be investigated and the recommendations of a specialist should be followed.
AV dissociation
The third variant of the ectopic rhythm - the P wave is positive, can occur in two cases: with AV - dissociation and AV - dissociation with interference.
AB - dissociation
AV dissociation is characterized by the following: PP intervals are identical to each other, RR intervals are identical to each other, independence of the QRS complex from the P wave, PP frequency is less than the RR frequency.
AV dissociation can be confused with complete transverse block. But with complete transverse block, the P waves are more frequent than the QRS complex, and with AV dissociation, the PP frequency is less than the RR frequency.
AB - dissociation can be in active and passive modes. When the mode is active, the downstream source operates more often than expected, and the upstream source operates in normal mode or weaker. In the passive version, the higher source operates weakly, and the underlying one operates at a normal frequency.
Rice. 3. AV dissociation with interference.
AB - dissociation with interference
Signs:
- PP teeth are equal to each other
- RR teeth are equal to each other
- As the ECG is recorded, the P waves and R waves will move relative to each other
- as soon as the refractoriness goes away, the impulse from the sinus node will pass to the ventricles and a short-term connection of the P wave with the QRS complex will be obtained. And there will be a normal PQ interval - ventricular capture, and then they will begin to shift further. And if there are ventricular seizures, this is called dissociation with interference.
Tags: AV dissociation, ECG waves, idioventricular rhythm, pacemaker migration, rhythm, Friederick's syndrome, ECG, electrocardiogram
Forecast
If the atrioventricular rhythm operates for a short period during sinus bradycardia or rhythm migration, then we can talk about a good prognosis. It’s another matter if the nodal rhythm is caused by dangerous disorders, for example:
- serious heart disease,
- atrioventricular block,
- during intoxication.
A low nodal rhythm tends to lead to serious manifestations. For example, if a situation of rhythm disturbance leads to heart failure, then this phenomenon is irreversible.
Since atrioventricular rhythm appears as a result of a whole complex of diseases and disorders, the prognosis depends precisely on those primary causes that caused cardiac arrhythmias.
The video below will tell you more about AV block as a cause of junctional rhythm disturbances:
How to identify impaired heart automaticity on an ECG?
Sinus arrhythmia
Due to deviations in the automaticity of the heart, so-called sinus arrhythmia occurs. The production of impulses by the sinus node is most important for the functioning of the heart, which is why it is called the 1st order pacemaker. The sinus node produces signals at a frequency of 60-80 times per minute.
The following types of sinus arrhythmia are distinguished:
- Tachycardia. Occurs when the sympathetic nervous system predominates. In case of arrhythmias, an ECG can be observed to indicate a rapid contraction, more than 80 beats per minute. Occurs after meals, exercise, or in stressful situations. These are physiological reasons. Tachycardia can develop due to exposure to medications, alcohol, or due to heart failure (HF).
- Bradycardia. The decrease in excitability of the sinus node is due to the predominance of parasympathetic processes. Physiological bradycardia can appear even in the absence of physical activity or stressful situations. If it is caused by sclerotic changes in the myocardium, then they speak of pathological bradycardia. Regardless of the reason, the ECG shows a heart rate less than 59, which can be traced to a change in the interval of the RR teeth.
In this case, sinus arrhythmia may occur at irregular intervals. Irrhythmic contractions are caused due to uneven interruptions of automaticity. If the ECG diagnosis of sinus arrhythmia showed a difference of more than 10% between the largest and smallest RR intervals, then a diagnosis of sinus arrhythmia is made.
There is a distinction between respiratory and non-respiratory arrhythmia.
Ectopic rhythms
A violation of automaticity may be associated with the occurrence of an electrical impulse in groups of cells outside the sinus node. Then an ectopic rhythm occurs. There are:
- Right atrial. They occur when the automatism of cells of the right atrium predominates.
- Left atrial. Cells of the left atrium predominate in the formation of impulses.
- Coronary sinus rhythm. It occurs with the active participation of cells in the formation of impulses that are located in the coronary sinus vein. Arrhythmia on the ECG is recognized by a smoothed P wave in lead aVL and lead I and a negative wave in lead aVF, lead II, and lead III.
AV Junction Junctional Rhythms
There are only 3 options in relation to atrial excitation:
- Precedes it. The ECG shows a negative P wave before the QRS complex in leads I, II, aVF and in V1-V. The PQ segment does not exceed 0.12 seconds, and the heart rate is 50-60.
- Simultaneously. The P wave is not observed because the QRS complex overlaps it. Heart rate – 40-50.
- Precedes ventricular excitation. It is caused by a slow passage of contraction signals, due to which excitation occurs after the ventricles. The P wave is negative, following the QRS. The distance between the Q and P teeth does not exceed 0.2 sec. Heart rate is in the range of 30-40.
Pacemaker Migration
This means that the source of impulses from the SA junction passes through the atria. On the electrocardiogram this can be seen by the alternating P wave, long PQ and RR intervals. Deformations of the QRS complex are possible.
Extrasystole
Extraordinary impulses to contract may be caused by a violation of automaticity. In such situations, the contraction impulse is compared to a guiding blow. Extrasystoles also occur in the presence of an ectopic source. The study picture may be different depending on the location of the ectopic source.
The following types of extrasystoles differ by location:
- Sinus. On the electrocardiogram before the extrasystole there will be a reduced RR interval, and after it it will be normal.
- AV connections.
- Ventricular. The QRST complex is highly distorted and the QRS complex is widened, exceeding 0.11 seconds. Moreover, the form may vary depending on the ectopic focus. There should definitely be no P wave, and the ST segment should be shortened or completely absent.
- Coronary sinus.
- Atrial. Typically, the PQ interval is shortened and P wave changes appear.
The following extrasystoles are distinguished by time:
- Super early.
- Early.
- Late.
Attention! If an extrasystole appears after each contraction, this is called bigeminy, after two - trigeminy.
Features in children
Idioventricular rhythm is diagnosed in children during the first 10 days after birth. The pathology is transient in nature. In 9% of children, the pathology develops into a stable pathological process.
At older ages, after 8 years, the following forms of pathology are diagnosed:
- 4% of patients have sinus bradycardia;
- 10% of children were diagnosed with ectopic atrioventricular rhythm;
- in 12% of all cases, pacemaker migration or atrial extrasystoles are detected.
Idioventricular rhythm in children occurs due to organic damage to the heart - congenital malformations, degenerative processes, inflammatory processes in the myocardium, tumors of various etiologies in the heart. Pathology occurs during metabolic changes when hypo or hyperthermia is present.
Rhythms of the atrioventricular junction
Previous | Contents | next Heart rhythms emanating from the atrioventricular (AV) junction (AVJ) in the form of single extrasystoles, parasystoles, slow escape rhythm and non-paroxysmal tachycardia are the most well studied rhythms of the AV junction. Other less studied arrhythmias include conduction disturbances (false AV block) and reciprocal atrial or ventricular premature beats resulting from overt or latent automatic activity or conduction delay within the AV junction. In addition, the strange phenomena observed in patients with two conduction pathways within the AV node, as well as variants of pseudotachycardia caused by the interpolation of atrioventricular excitations into sinus contractions, make the AV junction the most colorful and variable region of the heart in terms of rhythm disturbances. The pronounced variability of the AVS itself is due, firstly, to its central localization, location at the crossroads of the conduction system of the heart, which ensures its influence on various electrical impulses approaching or passing through the atrioventricular connection in both anterograde and retrograde directions, and, in -secondly, its ability to develop tachycardia or slow rhythm through increased automaticity and through re-entry. The sensitivity of the AV node to autonomic influences results in even greater diversity and complexity of AV rhythms.
Deductive analysis of each complex arrhythmia requires consideration of all possible interactions of the underlying cardiac rhythm with one or more of the AV phenomena listed above. In this chapter we will try to show the diverse manifestations of AV rhythms and their surprising interaction with the prevailing cardiac mechanisms.
Difficulties in defining the term atrioventricular connection
The term atrioventricular connection cannot be defined without taking into account both anatomical and electrophysiological characteristics to the extent that they are currently studied. According to most authors, the concept of ABC includes the AV node with its three electrophysiologically distinct regions (AN, N and NH) and the His bundle. From the point of view of surface electrocardiography, the common denominator for all AV rhythms is the caudacranial direction of atrial activation, leading to the appearance of negative P-waves in leads II, III and aVF, as well as the P-P interval,
the duration of which is less than with the main sinus rhythm on the same curve. Similar signs, however, can be observed when recording excitations emanating from the coronary sinus or the lower part of both atria. In view of this, it seems necessary to include all these areas of the heart in the definition of ABC, as was done by Scherf and proposed by Belief. This approach seems completely justified, since electrocardiographic differentiation of rhythms emanating from the upper regions of the AV node and rhythms arising in the region of the bases of the right and left atria, as well as in the coronary sinus, is probably impossible. In the only undisputed cases of early left atrial activation observed during stimulation of the distal coronary sinus, and retrograde left atrial activation during tachycardia with excitation along the posterior left accessory pathways, the P-wave vector is directed from left to right, resulting in negative P-waves appearing in leads I and V 6 and often (but not necessarily) - in leads II, III and aVF. How far the electrode catheter must be advanced into the coronary sinus to obtain purely negative P waves in leads I and Ve is unknown; Moreover, electrical stimulation of the left atrium in humans causes the appearance of many P waves of various shapes. Further complicating the problem of determining the source of atrial activation based on the polarity of the P waves is Moore et al. and Waldo et al. who observed positive polarity of P waves in leads II, III and aVF due to electrical stimulation in the area of the AV node. These differences in P wave polarity probably reflect the presence of several options for retrograde propagation of impulses within the atria and the possible use of the interatrial septum to conduct them in a cranial direction with subsequent activation of both atria in a caudal direction. Similarly, rapid conduction of the left atrial impulse along the Bachmann bundle can cause advanced activation of the right atrium, as a result of which the P wave will be clearly of the right atrial type. The polarity of the P wave in lead I was studied by Scamroth, who argued that the axis of the P wave in an ideonodal rhythm (i.e., the rhythm of the AV node; translator's note) usually has an inclination from -60° to -90°, which leads to a flattened or slightly positive P wave in lead I, whereas with reciprocal rhythms involving the AV node, the axis of the P wave has an inclination from -90° to -110°, which corresponds to the negative polarity of the P wave in this lead. However, the author does not discuss the reasons for the different orientation of the P wave axis.
Rice. 9.1.
Anatomical diagram of the atria (A), ventricles (V), AV node (U) and His bundle (G) with various options for localizing the source of atrial activation (marked with a cross).
Each fragment below schematically represents the corresponding ECG in standard lead II. The horizontal line between the ECG and anatomical diagrams shows the place of origin of P-waves (a cross) and the direction of propagation of excitation (arrows). The zigzag part of the cardiac axis is the region of slow conduction through the AV node. Fragment 1: excitation originates in the sinus node and must travel the entire distance through the atria to reach the AV node; therefore, here is the longest P-R interval and a positive P wave. Fragment 2: excitation arises in the lower part of the atria and activates them retrogradely; the wave of atrial depolarization reaches the AV node faster than in the previous case (1); the result is a negative P wave and a shorter P-R interval. Fragment 3: the impulse originates within the AV node and depolarizes the atria and ventricles almost simultaneously. In the case of a slight delay in conduction in one direction or another, a negative P wave and a very short or zero P-R interval are noted. Fragment 4, 5 and 6: the source of the impulse moves more and more distally, localizing in the common trunk of the His bundle (4), in the bundle branches (5) or Purkinje fibers in the ventricles (6). P-waves are negative and appear on the ECG necessarily after the QRS complex (in all these cases). The further the source of the P wave is from the atria, the later the retrograde P wave appears after the QRS complex.
Impulses originating in the ABC or inferior atrium do not travel all the way along the wall of the right atrium before reaching the His bundle; therefore the interval P - R
necessarily shorter than with sinus rhythm in the same patient (0.1-0.14 s) (Fig. 9.1).
It should be noted, however, that very early AV junction premature beats may penetrate the AV node or His bundle before these structures have fully restored their conduction, resulting in a P- R
may significantly exceed the range of 0.1-0.14 s .
In any case, in a given patient, the P- R
of the impulse emanating from the ABC or the inferior part of the atria (provided it is not too premature) is shorter than the
P-R
in sinus rhythm (see Fig. 9.1).
Rice. 9.2.
ECG in leads V 1 and V2, recorded simultaneously the next day after acute myocardial infarction of the inferior wall, complicated by suppression of sinus rhythm.
There is a slow ABC rhythm with a frequency of 43 beats/min. P waves in lead Vi are negative and presumably retrograde, originating from the same ABC focus that activates the ventricles. When interpreting an ECG, it is best to proceed from the assumption that the source of the rhythm is localized in the distal part of the AV node, from where impulses pass unhindered into the ventricles, but with increasing deceleration they are conducted into the atria. Consequently, inverted P waves appear later and later after the QRS complex. When the delay in atrial activation increases so much that the P wave overlaps the T wave, there may be a reflection of the impulse into the ventricle (an echo phenomenon), causing a contraction with ventricular capture (capture beat). Passing along the AV path, the reflected P wave depolarizes the pacemaker focus and restarts it, thus delaying the next discharge at the full duration of the main cycle of the AV rhythm (1.36 s). In this case, an ever-increasing delay in the retrograde propagation of the P wave into the atrium should take place within the AV node. Therefore, the pacemaker should be localized in the lower part of the AV node. It cannot be in the lower atrial region, since none of the P waves are located in front of the QRS complex; but it cannot be localized in the His bundle either, since the known Purkinje conduction time is not sufficient for the QRS complex to appear after the P wave. In the ECG presented here and in all subsequent clinical recordings, intervals are expressed in fractions of a second, not in milliseconds, since at a recording speed of 25 mm/s, millisecond accuracy is hardly possible. P - atria; F - ventricles; ABC - atrioventricular connection.
Division of rhythms into upper nodal, midnodal or lower nodal based on the appearance of the P
before the
QRS
simultaneously with it or after it is currently rejected due to the fact that the temporal relationship between the
P
QRS
complex depends more on the speed of anterograde and retrograde conduction than on the exact anatomical location of the source of the rhythm.
In Fig. Figure 9.2 shows an AV rhythm in which retrograde P
occur before or after the
QRS complex, depending
on the timing of the impulse into the atria.
Using electrophysiological methods used in routine practice, it is almost impossible to accurately determine the location of the impulse originating from the ABC or inferior atrial regions, which probably justifies the use of the expression atrioventricular or inferior atrial when interpreting electrocardiograms with abnormal P
and short intervals
Р—R.
Assessing the reaction of this rhythm during vagal and sympathetic testing can make a certain contribution to elucidating the nature of the rhythm (see below).
The listed problems are further complicated by the fact that the possibility of the existence of centrally located peri-nodal pathways that can quickly conduct impulses from the atria to the ventricles (and vice versa), bypassing the AV node, which is characterized by slow conduction, cannot be ruled out with certainty. The resulting short P-R
may suggest the presence of an ABC rhythm.
Based on the provisions discussed above and the literature data, it can be concluded that the clinical consideration of AV junction rhythms should be based on the following logical assumptions:
1) QRS
will be similar to those observed in sinus rhythm in the absence of aberrant conduction caused by premature excitation;
2) areas with the greatest automaticity are the areas adjacent to the AV node (coronary sinus, lower part of the atria) and the main trunk of the His bundle;
3) impulses arising in the lower atrial region most likely activate first the atria and then the ventricles;
4) excitation emanating from the His bundle is much more likely to activate the ventricles before the atria;
5) impulses arising inside the AV node activate the atria and ventricles almost simultaneously or in rapid succession, unless their propagation in one direction or another is impaired;-
6) shape and polarity of P
may be the same regardless of which part of the ABC or lower atrial region the ectopic impulses occur.
These provisions are based on the following observations:
1) electrical stimulation of the ostium of the coronary sinus and the lower part of the right atrium, as a rule, causes the appearance of retrograde P waves,
appearing before
QRS complexes;
2) stimulation of the His bundle always leads to the appearance of QRS
to the P waves;
3) escape impulses of the AV junction, occurring after pauses in the case of Wenckebach periodics and most likely emanating from the subnodal areas (main trunk of the His bundle), are characterized by QRS complexes,
P
waves 4) in the case of the phenomenon of atrioventricular echo occurring after an increased P-R interval,
when a U-shaped turn of the impulse occurs in the lower part of the AV node, the retrograde
P
is always located after the
QRS
(Fig. 9.3-9.5);
5) in the case of nodal circulatory tachycardia, when the anterograde impulse changes the direction of movement to the opposite in the lower part of the AV node, activation of the ventricles almost always precedes activation of the atria;
6) with a slow ABC escape rhythm due to sinus bradycardia or silent sinus node and likely originating from the inferior AV node or superior His bundle, QRS
precedes the retrograde
P wave;
similar rhythms that arise in areas sensitive to autonomic influences respond to the strengthening or weakening of vagal influence by slowing down or speeding up, respectively (Fig. 9.6);
7) rhythmic activity, characterized by retrograde P
preceding the
QRS complexes,
according to the author’s observations, is, as a rule, insensitive to autonomic influences.
Rice. 9.3.
Simultaneous recording of I, II and V 1 ECG leads, revealing AV block with Wenckebach periodicity in a patient with acute myocardial infarction of the inferior wall.
Wenckebach periods end when echoes of P waves (negative P waves almost merging with QRS complexes 2 and 9) occur after the longest P-R interval (0.48 s). This phenomenon is not uncommon and should be suspected in cases where the P sine wave expected in the middle of the pause is absent. Reflected P waves may overlap the QRS complexes, so they are not always easy to identify. Their presence is indicated by the absence of the expected sinus P wave during pauses. The combination of a prolonged P-R interval and an echo phenomenon is a necessary substrate for the occurrence of AV nodal circulatory tachycardia (shown in the lower trace). Similar tachycardia caused by AV block with Wenckebach periodicity was observed in several other cases.
Rice.
9.4. The upper fragment is an ECG in lead II with atypical blockade with Wenckebach periodicity and echo-R waves (indicated by P), occurring at the moment when the P-R interval exceeds 0.5 s. The lower fragment is the EG of the His bundle (His), on which two H-potentials (H1 and H2) are clearly visible, reflecting the activation of the proximal and distal parts of the bundle; the blockage occurs between these two areas. The middle fragment is the lead from the upper right atrium (SRA), where the reflected P-wave occurs at the moment when the H1-H2 interval reaches 485 ms. Apparently, the echo occurs closer to the distal part of the His bundle, probably just before its bifurcation. The presented curves do not allow us to determine with certainty whether the His bundle itself or the adjacent James bundle is used to conduct the echo P wave.
These data are consistent with the proposal that this activity is localized in the lower part of the atria or the coronary sinus region (Fig. 9.7). These observations allow us to hope that when analyzing ABC rhythms, determining the relative position of the P
and the
QRS
will help establish the localization of ectopic activity.
A single beat or sustained rhythm characterized by a retrograde P
before the
QRS
most likely originates from the inferior atrial region or coronary sinus, whereas the presence of a
P
after the ventricular complex indicates the location of an ectopic pacemaker in the distal AV node or His bundle.
Between these two extremes there are many variations, with the P
and the
QRS
appearing almost simultaneously or quickly following each other (Fig. 9.8).
These rhythms probably originate within the AV node. However, an additional path or rapid conduction of the lower atrial impulse through the AV node will also cause a close relationship between the P
and the
QRS complex.
Finally, in some cases with AV rhythms, the morphology of the
P
is very variable, despite the almost constant duration of the cycle of this activity.
Rice. 9.5.
AV echo against the background of Wenckebach periodicity in two patients. Late appearance of retrograde echo P waves is characteristic, suggesting the use of a slow pathway within the AV node for reflected atrial activation. In contrast to the early appearance of retrograde P waves shown in Fig. 9.3 and 9.4 is obvious.
Rice. 9.6.
An AV junction rhythm in which P waves consistently appear after the QRS complexes.
It is most logical to assume that the pacemaker is localized in the distal part of the AV node or the proximal part of the His bundle. In the first case (upper fragment), the AV rhythm frequency decreases with carotid sinus stimulation (CSS) and increases after atropine administration, which is consistent with the known vagal reactivity of the AV node—the proximal part of the His bundle. In the second case (lower fragment), spontaneous changes in frequency are noted, associated with natural fluctuations in the tone of the autonomic nervous system.
Rice.
9.7. Some ECG leads (I, III, aVR, aVF, V 1, V3, V 4 and V 6) in five cases of ectopic rhythm ABC - the lower part of the atrium, where P waves precede the QRS complexes with a P-R interval varying from 0.02 to 0.11 s.
The rhythm frequency in all 5 patients (a-e) did not change with stimulation of the carotid sinus and administration of atropine, which suggests autonomous insensitivity of the ectopic focus, probably when localized in the region of the coronary sinus - the lower part of the atrium. The direction of the P-wave axis in these patients is different, which reflects either a different location of the AV rhythm driver or differences in the nature of the propagation of impulses. In all cases, P waves are negative in the inferior leads and positive in lead aV R, indicating retrograde atrial activation; however, the chest leads are different in all 5 patients.
Rice.
9.8. ECG in several simultaneously recorded leads demonstrating the rhythm of the AV junction, in which the P wave is superimposed on the QRS complex (in two patients).
In both cases, a return to normal sinus rhythm is also shown (below the ABC rhythm recording); similar leads are presented here. In these examples, the ABC rhythm is unlikely to originate from the inferior atrial region or coronary sinus because P waves do not precede the QRS complex. Localization of the ectopic focus in the main trunk of the His bundle is also unlikely, because the QRS does not appear before the P wave. Therefore, the most likely place of occurrence of the ectopic rhythm is the AV node; the exact location, however, cannot be determined.
It is very difficult (if possible) to determine what exactly reflects the lability of the P wave shape - migration of the atrial pacemaker or a change in the activation sequence in a series of contractions with constant localization of the ectopic focus. The latter explanation seems more acceptable.
In cases where the P
completely blocked by the
QRS complex,
it is very difficult or even impossible to determine the direction of propagation of the atrial wave unless at least two intra-atrial electrograms are obtained simultaneously.
In a certain number of cases, P
are attached to the beginning or end of the
QRS complex,
thereby creating the erroneous impression of expansion of the latter (Fig. 9.9).
In such recordings, determining the polarity of the P
may be difficult or even impossible, since the wave is not recorded at the level of the horizontal isoline.
It can be difficult to determine the polarity of the P
, regardless of its nature and in the case when it is superimposed on the inclined
ST
or on the
T
(Fig. 9.10).
Rice. 9.9.
An AV rhythm in which the P wave is coupled to the end of the QRS complex, suggesting intraventricular conduction delay with a QRS complex duration of 0.14 s (top of the figure). In normal sinus rhythm (bottom of the figure), the P wave and QRS complexes no longer merge with the P waves and their duration is only 0.09 s.
Rice. 9.10.
ECG in leads I, II and V 1 (recorded simultaneously) and EG of the upper right atrium (URA) and the His bundle (His). In each fragment (A-D), sinus contraction is accompanied by ventricular extrasystole. The coupling intervals of these extrasystoles vary somewhat in different fragments. As a result, sinus P waves following the extrasystoles are superimposed on various parts of the ST segments of the extrasystolic contraction. Therefore, some of the post-extrasystolic P waves in lead II appear negative (A, B and D), while others appear positive (C and D).
Classification and types
Modern cardiological communities have recognized the division of atrioventricular nodal reciprocal tachycardia into the following 3 types:
- slow-fast - a typical option in which the electrical impulse from the atria through the Aschoff-Tavara node passes along the “slow” path, and back along the “fast” path;
- fast-slow - an atypical form, which is the opposite of the first option;
- slow-slow - a rare type: the current passes through two “slow” beams.
The course of the disease can be paroxysmal (attacking) and chronic. The latter option is rarely observed. Over time, it leads to expansion of the cavities of the heart and the formation of tachycardiomyopathy. Paroxysms, in turn, are characterized by an acute spontaneous onset and the absence of long-term complications.
Wolff-Parkinson-White syndrome (WPU, WPW)
WPW syndrome is caused by the presence of an abnormal bundle of Kent, a connection between the atrium and one of the ventricles. With this pathology, the formation of atrioventricular reciprocal tachycardia through the re-entry mechanism is also possible. There are two types:
- orthodromic - forward along a specialized conduction system, back from the ventricles along an additional atrioventricular connection;
- antidromic - from the atria through the anomalous bundle of Kent and back through the AV node.
Causes
The emergence of IR is due to the following factors:
- myocarditis - an inflammatory process that spreads to the heart muscle;
- large-scale blood loss caused by heavy bleeding;
- an ischemic process that provokes oxygen deficiency in healthy myocardial fibers;
- cardiosclerosis;
- cardiac tamponade – accumulation of fluid in the pericardium, which causes compression of the organ cavities;
- myocardial infarction;
- thyroid pathology;
- hormonal imbalance.
IR can be the only pathology and does not lead to other cardiac dysfunctions or is complemented by other anomalies.
A similar phenomenon sometimes occurs in people with severe heart damage.
What is idioventricular rhythm?
A healthy person has only one pathway for transmitting nerve impulses to successive contractions. The path begins in the right atrial appendage, where the sinus node is located, and continues to the AV node. Passing through the His bundle and Purkinje fibers, the nerve impulse reaches the fibers of the ventricles.
For some reason, the sinus node loses the ability to generate excitations for contraction. In such cases, the excitatory process in the heart changes. To maintain the activity of the heart, compensatory ectopic rhythms develop. Translated, the word ectopia means that something arose in the wrong place where it should have.
Important! The source of ectopic rhythms may be located in the atria, the AV junction, or the ventricles.
Methods of therapy, treatment and recommendations of doctors
Methods of therapy for treating patients diagnosed with idioventricular rhythm - prescribing medications, performing ablation.
Drug therapy
The drugs that are most often prescribed to patients for heart rhythm disturbances are presented in the table:
| A drug | Purpose |
| Amiodarone | The drug is administered intravenously - into a central vein or as a bolus. Dosage: 150-300 mg over 20 minutes in case of emergency. For long-term therapy, 200 mg of the drug is prescribed daily. The treatment period is 14 days. |
| Digoxin | The drug is administered intravenously. For emergency treatment, 0.25 mg every 2 hours is indicated for the first 2-3 days. As maintenance treatment, no more than 0.375 mg per day is prescribed. |
| Metoprolol | The drug is indicated for emergency treatment at a dosage of 5 mg intravenously every 5-10 minutes. The total dosage is not more than 15 mg. As maintenance therapy, 100-200 mg is prescribed during the day. |
Antiarrhythmic drugs exhibit proarrhythmic effects. Their effect is aimed at restoring supraventricular or ventricular rhythm. Treatment with these drugs is prescribed to patients with severe coronary disease, organic disorder, and hypokalemia.
Invasive techniques (surgical procedures)
Effective invasive methods include:
- Percutaneous ablation. A catheter is inserted into the heart muscle. With its help, the doctor isolates the pulmonary veins, which lead to an increase in the frequency of impulses.
- Implantation of a cardioveterar defibrillator. This is an automatic device that helps restore normal heart rhythm. It can be programmed for each patient so that the defibrillator will perform antiarrhythmic stimulation of the heart.
After the invasive procedure, patients are hospitalized for inpatient recovery.
Emergency care and resuscitation
Emergency care is provided to patients who have a frequent idioventricular rhythm, which is combined with atrial dysfunction, tachycardia. Doctors advise calling an ambulance if you experience pressing or acute pain in the heart area.
Before their arrival, you need to take a horizontal position. To provide first emergency care, a solution of potassium chloride at a concentration of 4% or novocainamide (10%) is administered to the patient. Improvement in well-being is observed after 15 minutes. After hospitalization on the first day, patients are shown the drug Adenosine. It is administered at a dosage of 6 mg every 2 hours. The medicine is not intended for long-term therapy.
Idioventricular rhythm requires treatment, because during a pathological process in the heart, a disruption of the normal rhythm of myocardial contractions occurs. Lack of therapy leads to a worsening of the situation, the appearance of symptoms of tachycardia and shortness of breath.
To prevent the occurrence of idioventricular rhythm, you need to stop smoking, abuse alcoholic beverages, and eat well and properly. You should visit a cardiologist at least once a year. Diagnostics allows timely detection of idioventricular rhythm deviations on the ECG.