Takotsubo cardiomyopathy (or stress-induced cardiomyopathy) is a type of non-ischemic cardiomyopathy in which there is a sudden, transient decrease in the contractility of the heart muscle. In many ways, the manifestations of this disease - pain in the heart and difficulty breathing - are similar to the signs of myocardial infarction. Their appearance is provoked by severe psycho-emotional or physical stress (for example, the sudden death of a relative, news of cancer, an asthmatic attack).
That is why the disease received such names as “broken heart syndrome” and “takotsubo cardiomyopathy.” In the first version, the name reflects the cause of the development of the pathology: severe stress or anxiety. In the second case, the name appeared due to the fact that, translated from Japanese, the word “tako-tsubo” is the name of a device for catching octopuses, and with this type of cardiomyopathy, the shape of the left ventricle takes the shape of this object, which is a ceramic pot with a spherical base and a narrow top .
Takotsubo cardiomyopathy belongs to the category of rare forms of cardiomyopathies, but in recent years experts have noted a trend towards an increase in the number of patients with this disease. In this article we will provide you with information about the causes, prevalence, characteristics of the course, methods of identifying and treating broken heart syndrome.
A little history
Alcohol addiction and smoking are factors that increase the risk of developing takotsubo cardiomyopathy.
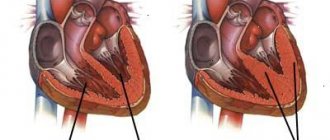
This heart disease was first described in 1991 by a group of Japanese scientists - Dr. H. Sato and his co-authors. It was they who gave it the name “takotsubo cardiomyopathy”, since the shape of the pathologically altered left ventricle in this disease resembled the device used by Japanese fishermen for catching octopuses - tako-tsubo. It was this symptom that made it possible to distinguish the syndrome in question from myocardial infarction. With this form of cardiomyopathy, the left ventricle becomes similar to tako-tsubo and during systole its apex does not contract, and its basal sections simultaneously contract excessively.
Takotsubo cardiomyopathy became widely known in 2006 thanks to a discussion of this topic at the European Congress of Cardiology held in Barcelona. Since then, scientists have begun to pay more attention to studying the mechanisms of its development. So far, specialists have not been able to fully study these aspects of the disease.
Rarely causes death
Despite its rather serious symptoms, broken heart syndrome rarely leads to death or serious complications, although it requires medical supervision. Typically, maintenance therapy is used as treatment - the patient is prescribed acetylsalicylic acid, ACE inhibitors to lower blood pressure, and other drugs. Already in the first few days, the contractility of the heart muscle begins to return to normal, and it takes an average of 2 months to completely restore the functions of the left ventricle.
Causes
So far, scientists suggest that broken heart syndrome develops under the influence of the following factors:
- severe stress and intense psycho-emotional experiences: news of a serious illness, death of a relative, accidents, etc.;
- physical activity exceeding the body's capabilities: sudden serious illness, asthmatic attack, etc.
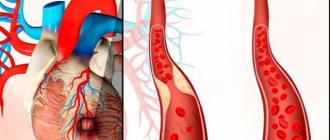
The mechanisms of development of such cardiomyopathy are still unclear. There are several theories of pathogenesis: transient vagospasm, microvascular dysfunction, twisted left anterior descending artery. However, none of them have yet been fully proven. Observations of large groups of people with Takotsubo cardiomyopathy showed that in many of them the disease developed precisely against the background of intense stress (emotional or physical). However, in approximately a third of patients such factors were absent.
Observations by European specialists have shown that takotsubo cardiomyopathy develops somewhat more often in winter. This fact can be explained by two probable reasons:
- in the cold season, spasm of small branches of the coronary vessels occurs more often;
- During the autumn and winter months, people are more likely to suffer from viral diseases.
It is believed that bulging of the left ventricular apex occurs due to increased levels of catecholamines in the blood. The mechanism of development of this disease has not yet been fully elucidated. Scientists believe that the most likely role is played by the release of adrenaline that appears at the moment of stress, which provokes vasospasm and sharply worsens the quality of microcirculation in the vessels of the heart. As a result, the patient experiences transient dysfunction of the left ventricle, manifested by changes in the ECG and blood tests characteristic of myocardial infarction.
Expert observations show that in addition to psycho-emotional and physical stress, the following predisposing factors can contribute to the development of broken heart syndrome:
- a constant source of traumatic situations in the family or at work;
- intense pain syndrome;
- addiction to alcohol or nicotine addiction;
- hyperlipidemia;
- a sharp decrease in blood pressure;
- performing procedures or surgery (eg, cardiac stress test).
Takotsubo cardiomyopathy, or stress-induced cardiomyopathy
Takotsubo cardiomyopathy was first described in Japan in 1990 by H. Satoh as a transient disorder of myocardial contractility. The classic variant of the disease is accompanied by akinesis or dyskinesis of the apex of the heart with hyperkinesis of the basal segments. At the same time, the heart acquires a unique configuration: the left ventricle in the acute phase is shaped like an hourglass or a Japanese octopus trap takotsubo - a jug with a narrow neck and a wide bottom. Takotsubo cardiomyopathy is a reversible dysfunction of the left ventricle in response to physical or mental stress, clinically and electrocardiographically resembling acute coronary syndrome, mainly in postmenopausal women without significant stenosis of the coronary arteries, characterized by a relatively favorable outcome.
The pathogenesis of Takotsubo syndrome is not completely known. Several hypotheses have been proposed to explain the possible mechanisms of development of CIPT: coronary artery vasospasm, left ventricular outflow tract (LVOT) obstruction, catecholamine overload, neurohumoral disorders and coronary microvasculature dysfunction. The main theory for the development of cardiomyopathy at the moment is the toxic effect of elevated levels of catecholamines on the myocardium and excessive sympathetic stimulation. The impact of endogenous (emotional) or exogenous (trauma, surgery or excessive physical activity) stress is noted in the vast majority of cases of cardiomyopathy. This relationship has led to the suggestion that the mechanism of development of cardiomyopathy may be associated with the influence of the sympathetic nervous system under stress.
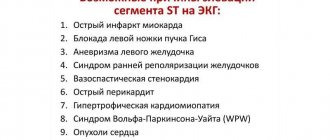
Clinical picture. As described by Russian and foreign researchers, the symptoms that develop with cardiomyopathy largely coincide with the clinical picture observed with acute myocardial infarction. Thus, the most typical clinical signs of cardiomyopathy are an acute onset, an attack of chest pain or shortness of breath, while on the electrocardiogram the ST segment elevations are most often observed, and in the blood an increase in the level of creatine phosphokinase, the MB fraction of creatine phosphokinase and troponin, as well as hypercatecholaminemia is determined. In cases where an endomyocardial biopsy is performed, foci of myocytolysis, infiltration of mononuclear cells, as well as necrosis of cardiomyocytes in the form of overcontraction bands in the absence of signs of myocarditis are determined histologically. When performing echocardiography in such patients, severe disturbances in contractility of the left ventricular myocardium are determined. At the same time, coronary angiography in patients with cardiomyopathy does not show significant stenosis of the coronary arteries. It should be noted that the main criterion for diagnosing CIPT is the complete reversibility of impaired myocardial contractility. ECG changes in the acute phase of CIPT develop in approximately 80–85% of cases. According to diagnostic guidelines for CIPT, the main ECG changes characteristic of CIPT are ST segment elevations, inverted T waves, QT prolongation, and rare or absent reciprocal changes. The most common ECG changes in patients with CIPT are ST segment elevations in the precordial leads (in leads V1–V4). Also, over time, the appearance of negative T waves and pathological Q waves is possible. Thus, the features of the course of Takotsubo CMP are: the absence of significant obstruction of the coronary arteries; the area of akinesia does not correspond to the zone that can be supplied by one coronary artery; a huge difference between the volume of myocardium involved and the degree of enzyme increase; rapid complete normalization of myocardial contractility.
Basic diagnostic criteria for Takotsubo cardiomyopathy (“modified Mayo Clinic criteria”):
1. Transient hypokinesis, dyskinesis and akinesis of the middle segments of the left ventricle with or without involvement of the apex, balloon-like expansion of the left ventricular cavity that does not correspond to the blood supply zone of any one coronary artery, a physical or mental traumatic factor preceding the development of this condition is desirable.
2. Absence of coronary artery obstruction or angiographic evidence of acute plaque rupture.
3. The appearance of ECG changes – ST segment elevation, possible T wave inversion.
4. Moderate increase in troponin
5. No previous head trauma, intracranial hemorrhage, hypertrophic cardiomyopathy, pheochromocytoma or myocarditis.
Complications:
— Arrhythmias: AV blockade, sinus bradycardia, atrial fibrillation, ventricular tachycardia and fibrillation
— Acute left ventricular failure
- Pulmonary edema
— Cardiogenic shock
— Myocardial rupture
- Formation of thrombus in the apex of the LV and embolism
— Pericarditis
Treatment: Currently, specific treatment methods have not been developed. There are no clear criteria for the duration of therapy. It is necessary to continue therapy until cardiac function is completely restored. In most cases, patients with cardiomyopathy are admitted to the hospital with clinical and laboratory signs of acute myocardial infarction, and before a diagnosis of cardiomyopathy is made, their treatment tactics are determined by the recommendations for the treatment of acute ST-segment elevation myocardial infarction. After diagnosing Takotsubo cardiomyopathy, it is possible to transfer patients to maintenance drug therapy. Due to the fact that Takotsubo syndrome is accompanied by the development of transient left ventricular dysfunction, patients are prescribed treatment with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers. In hemodynamically unstable patients, it is necessary to exclude possible obstruction of the left ventricular outflow tract (LVOT), which requires the administration of beta-blockers. Due to the lack of studies on the negative effects of vasopressors in severe cardiomyopathy, such patients are also indicated for support with ionotropic drugs. Some researchers believe that long-term treatment with beta-blockers is indicated to prevent relapses of cardiomyopathy. However, this disease is benign, in most cases ending in complete restoration of left ventricular function 2-4 weeks after the onset of symptoms.
Prognosis: 95% of patients have a favorable prognosis, within a few weeks there is a complete reversal of ECG and ECHO-CG changes , repeated cases are extremely rare 2.7%
Conclusion: Thus, Takotsubo cardiomyopathy is a rare syndrome. However, it can be assumed that this syndrome occurs much more often than described, which is due to the complexity of its diagnosis. Takotsubo syndrome occupies an important place among cardiovascular diseases. This is due primarily to the fact that in the acute period, according to the clinical characteristics, the disease resembles acute myocardial infarction. Most often, the disease develops after emotional stress and is accompanied by an attack of chest pain, ST segment elevations on the ECG, as well as disturbances in myocardial contractility according to EchoCG. It has been shown that of the number of patients admitted to the emergency cardiology department with a preliminary diagnosis of ACS, 3% are subsequently diagnosed with Takotsubo cardiomyopathy.
Prevalence
Takotsubo cardiomyopathy is found much more often in the fair sex. According to specialists, the average age of patients with this disease is 61-76 years. In women who are already 55 years old, the risk of developing this pathology is 4.8 times higher than in those who have not reached this age limit. It is assumed that this fact indicates that more often broken heart syndrome develops in older women, whose estrogen levels decrease and vascular and heart tissues become more sensitive to the effects of stress hormones. Statistics also confirm this assumption: in more than 90% of cases, broken heart syndrome occurs in postmenopausal women.
Takotsubo cardiomyopathy can be detected even in children. This fact is explained by the fact that differentiation of the adrenal glands lasts up to 14-16 years, and during this period of hormonal instability the body may react incorrectly to stress.
History of discovery and features of Takotsubo cardiomyopathy
Japanese cardiologists in 1990 described a case of a special enlargement of the heart, which resembled the shape of a takotsubo pot made of clay, intended for catching octopuses. It has a spherical base and a narrow neck. This is what the heart looks like due to spasm of the base of the left ventricle and expansion of its apical zone. Some doctors compare the shape of the left ventricle to an amphora or ampoule.
One of the main features of takotsubo cardiomyopathy is the connection of its occurrence with strong negative emotions (death of loved ones, news of a serious illness), which made it possible to give this disease the name broken heart syndrome. It is most often found in older women who are postmenopausal (65 - 75 years old), which does not exclude the significance of the loss of the protective effect of estrogen in stressful situations.
Such myocardial damage accounts for approximately two percent of all patients with acute coronary pathology. After being investigated by Japanese doctors, the disease was reported at the European Congress in 2006. Due to its relative novelty and rare occurrence, specialists are not yet keen on it, so in real practice there may be more such cases.
We recommend reading the article about ischemic cardiomyopathy. From it you will learn about the causes of the development of pathology, symptoms, methods of diagnosis and treatment. Read more about dilated cardiomyopathy here.
Symptoms
Takotsubo cardiomyopathy is clinically similar to myocardial infarction.
Coronary angiography will help to distinguish these pathologies from each other. The manifestations of broken heart syndrome are in many ways similar to the symptoms of acute myocardial infarction. The most common signs of this disease are chest pain, observed in 59% of patients, and shortness of breath, observed in 30% of patients. In addition, this form of cardiomyopathy may be accompanied by attacks of tachycardia and periodic fainting.
When conducting an examination in patients with Takotsubo cardiomyopathy, the following symptoms are revealed:
- pain in the heart after any overload (psycho-emotional or physical);
- ischemic changes on the ECG;
- no signs of patency of the coronary vessels or minor disturbances in the functioning of the arteries of the heart;
- increased levels of creatine kinase-MB and/or troponin.
Forecast
Despite the dire initial clinical presentation in some patients, most patients survive the initial attack with very low rates of in-hospital mortality or complications. After undergoing the acute stage of the disease, patients can expect a favorable outcome with a good long-term prognosis.[4][15][17] Even with severe systolic dysfunction at the onset of the disease, myocardial contractility begins to recover within the first few days and normalizes within several months.[15][9][10][11] In 5% of cases[23] there is a relapse of the disease, probably provoked by an associated trigger.[14][15]
Features of the flow
The problem with timely diagnosis of this form of cardiomyopathy is that the results of blood tests and ECG are almost identical to the manifestations of myocardial infarction. Broken heart syndrome can be distinguished from this common disease only by the results of coronary angiography, which shows that the arteries of the heart remain healthy and there is no hemodynamically significant narrowing of these vessels.
Published in the European Heart Journal, the most significant studies of this form of cardiomyopathy showed that approximately 1.7-2.2% of myocardial infarctions are actually Takotsubo cardiomyopathy. In more than half of patients with this disease, the attack is preceded by intense stress and in 74% of patients the level of catecholamines increases. It is noted that compared with normal values in Takotsubo cardiomyopathy, the level of these hormones can increase tens of times.
Cases of broken heart syndrome may have increased during the pandemic
During the pandemic, American scientists tried to establish a direct relationship between the spread of Takotsubo cardiomyopathy and socio-economic and political factors. They studied the medical records of 1,914 patients from two Cleveland hospitals.
The incidence of broken heart syndrome among patients with heart disease was found to have increased to 7.8%, compared to 1.7% of patients diagnosed with stress cardiomyopathy before the pandemic. In addition, patients with Takotsubo cardiomyopathy spent longer in the hospital during the pandemic than before.
It is not difficult to explain the increase in cases of broken heart syndrome: during the pandemic, people around the world have been subjected to enormous stress due to fear for themselves and the health of loved ones, being isolated and deteriorating the socio-political situation.
However, as the study notes, its results require further confirmation. Since only patients from one city were studied, it is too early to apply the findings to patients in other countries. Some patients with cardiovascular diseases could avoid visiting hospitals during the pandemic, which also affected the final result.
Read on topic: 7 heart attack symptoms that occur in women
Complications
Takotsubo cardiomyopathy can be complicated by the following conditions:
- heart failure;
- bradyarrhythmia;
- tachyarrhythmia;
- cardiogenic shock;
- severe mitral regurgitation;
- stroke;
- apical thrombus formation.
The development of acute heart failure in broken heart syndrome increases in the presence of the following factors:
- decrease in left ventricular ejection fraction less than 40%;
- presence of a physical stressor;
- age over 70 years.
Prevalence and causes
Strong emotional experiences
Since the disease was discovered relatively recently, it is not yet possible to speak with certainty about the prevalence, causes and pathological links of broken heart syndrome. Based on observations, it has been established that this syndrome occurs predominantly among postmenopausal women aged 40 to 55 years. Exacerbations of the syndrome are observed in winter. Much less frequently, but still, this syndrome can occur in young women, in early pregnancy, in the postpartum period, in adolescents and children.
There are many hypotheses regarding the nature of the disease: a number of authors speak of Takotsubo cardiomyopathy as an interrupted variant of acute myocardial infarction. Japanese cardiologists, in turn, propose to consider broken heart syndrome as an unknown (idiopathic) disease accompanied by transient dysfunction of the left ventricle. Possible causes of the disease include emotional and physical stress, which leads to the release of a significant amount of catecholamines into the blood. Specific provoking factors may be the following:
- treadmill (treadmill),
- hypothermia,
- alcohol abuse,
- sexual intercourse,
- a sharp drop in blood pressure,
- surgery,
- strong emotional feelings,
- financial crisis,
- health problems,
- natural disasters.
Diagnostics
To detect Takotsubo cardiomyopathy, the following tests are prescribed:
- ECG – changes typical for acute heart failure are detected, manifested in disturbances in the rhythm, rhythm and speed of contraction of the walls of the ventricles of the heart (recovery of ECG indicators in broken heart syndrome occurs after 2-3 weeks of the disease);
- Echo-CG - dyskinesia or akinesis of the middle part and apex of the left ventricle is detected against the background of apical and basal hyperkinesis, a characteristic change in the outline of the left ventricle is always determined, sometimes there is obstruction of the outflow tract of the left ventricle;
- coronary angiography – unlike acute coronary insufficiency, there are no hemodynamically significant stenoses of the coronary arteries;
- MRI - administration of gadolinium shows that the contrast does not accumulate transmurally or subendocardially, as in myocarditis and myocardial infarction;
- analysis of cardiac serum markers - increased levels of creatine kinase-MB and/or troponin are found in the majority (approximately 89%) of patients.
Patient's symptoms
The largest number of diagnostic errors in Takotsubo cardiomyopathy are associated with the fact that the clinical signs of the disease are almost completely identical to the acute period of myocardial infarction. Patients complain of:
- feeling of fear, anxiety;
- pain in the left side of the chest;
- sweating;
- a rush of heat to the head and neck;
- severe lack of air;
- increased heart rate;
- interruptions in the rhythm of contractions.
Typical forms include severe cardiac pain, which is later followed by shortness of breath, fainting and tachycardia. These criteria are the basis for identifying broken heart syndrome based on research from the Mayo Clinic. Due to severe compression of the base of the heart, the ejection of blood into the aorta is disrupted.
Therefore, in some patients the disease begins with signs of cerebral circulatory disorders:
- nausea, vomiting;
- dizziness with loss of consciousness;
- convulsive seizure.
Low cardiac output leads to cardiogenic shock. If it is difficult for blood to pass into the aorta, it can open the mitral valve leaflets and pass into the left atrium.
Often, in severe cases, rhythm disturbances occur - tachycardia, bradycardia, atrial fibrillation, ventricular fibrillation, followed by cardiac arrest. Complications also include the formation of a blood clot in the cavity of the left ventricle, stroke, and acute heart failure.
Watch the video about the causes and treatment of cardiomyopathy:
Treatment
Broken heart syndrome is an indication for emergency hospitalization.
If signs of Takotsubo cardiomyopathy are detected, the patient should be urgently hospitalized in a hospital. There are no clear recommendations for the treatment of this form of cardiomyopathy. If the development of the disease was preceded by a strong stress factor, then the patient in the acute stage is advised to take tranquilizers. In the presence of severe pain and other provoking factors that contributed to the development of the disease, their elimination is indicated.
Also, patients with takotsubo cardiomyopathy are prescribed the following drugs that reduce the load on the myocardium:
- beta blockers;
- ACE inhibitors;
- diuretics;
- calcium antagonists;
- organic nitrates;
- antiplatelet agents;
- anticoagulants.
When dynamic obstruction of the left ventricular outflow tract is detected, positive inotropic agents are included in the drug treatment plan.
For Takotsubo cardiomyopathy, intra-aortic balloon counterpulsation may be indicated.
The duration of medication is determined by the rate of recovery of left ventricular function. The first signs of improvement in heart function appear within a few days, and with supportive drug therapy, the heart usually recovers completely within the first 2 months.
First aid and treatment
Patients with suspected stress-induced cardiomyopathy are advised to undergo urgent hospitalization. This is due to the possibility of rapid development of complications and the difficulty of making a correct diagnosis without special instrumental and laboratory examination.
In the first stages, patients need the administration of sedatives (Diazepam) and painkillers (Morphine, Droperidol).
The main problem is the development of cardiogenic shock against the background of low cardiac output.
Usually used in this case, Dobutamine and Norepinephrine can significantly worsen the condition of patients, as they experience a thirty-fold increase in stress hormones in the blood. Therefore, they most often use:
- beta blockers (Carvedilol);
- ACE inhibitors (Capoten);
- stimulants of cardiac contractility (Simdax).
In cases of severe hypotension, intra-aortic balloon counterpulsation is used. If signs of thrombosis are detected, Warfarin is indicated; as blood circulation indicators normalize, its duration of use is reduced.
Which doctor should I contact?
If you experience chest pain, shortness of breath, episodes of tachycardia and occasional fainting, you should consult a cardiologist. After an ECG, Echo-CG and coronary angiography, the doctor will be able to differentiate Takotsubo cardiomyopathy from other manifestations of acute coronary insufficiency and prescribe the necessary treatment.
Takotsubo cardiomyopathy is a rare form of cardiomyopathy and often develops against the background of severe emotional or physical stress. In recent years, this pathology has been detected more and more often. Its manifestations are almost identical to those of acute myocardial infarction, and these two diseases can only be distinguished after coronary angiography. The treatment tactics for these two heart diseases are also largely similar and involve the use of tranquilizers to eliminate stress factors and drugs to reduce the load on the heart muscle.
About broken heart syndrome in the program “Live Healthy!” with Elena Malysheva:
Diagnosis of the disease
In order to accurately diagnose stress-related cardiac pathology, the cardiologist prescribes a number of such hardware tests:
- Angiography. Makes it possible to differentiate stress pathology from acute coronary insufficiency.
- Coronography. Allows you to track the possible development of important arterial stenoses, which can subsequently lead to more serious complications in the functioning of the left ventricle.
- Electrocardiogram or echocardiogram (ECG or EchoCG). Here the transcript will indicate an increase in the pathological ST segment. The doctor may also note sinus bradycardia or ventricular tachycardia.
- MRI of the heart. Allows a more detailed assessment of the heart condition of a patient admitted to the hospital.
- Ultrasound of the heart (ultrasound examination). Performed due to the lack of an MRI machine.
Forms of the disease
When “broken heart syndrome” occurs, the upper part of the ventricle stops contracting, but its basal part contracts intensely. At the moment, there are two forms of this pathology:
- The apical partial or moderate form is most often characteristic of middle-aged people (30-45 years).
- The reverse form is characteristic of young women who have hyperdynamicity of the upper ventricle and complete akinesia of its basal segments. This is a rarer form of the disease that is more difficult to identify.