Heart rate is one of the main indicators of human health and the quality of the cardiovascular system. This level is assessed on the same basis as blood pressure.
A change in the nature of functional activity indicates pathological abnormalities in cardiac structures or other parts of the body. There are many options for the development of heart problems.
Atrial extrasystole is a special case of arrhythmia, which is characterized as the occurrence of extra, single, paired or multiple heart beats that disrupt the adequate rhythm of the organ.
The pathology has a favorable, benign course in most cases. It is extremely rare that pathogenic factors in the development of the problem are possible.
It is impossible to distinguish one condition from another, as they say, by eye. At a minimum, an objective assessment is required, plus electrocardiography.
Diagnosis is carried out under the supervision of a medical specialist as part of a screening program or based on patient complaints.
In the absence of help, atrial extrasystole can transform into other, more dangerous forms, such as ventricular.
Mechanism of disease development
In order to clearly understand how this process occurs, you should refer to the anatomical reference.
The heart and cardiac structures are the only ones capable of spontaneous occurrence of excitation. That is, for adequate work they do not require either hormonal or electrical stimuli from the outside.
The task of signal generation is handled by a special anatomical structure, a cluster of cardiomyocyte cells called the sinus node. This is the main, natural pacemaker.
As part of the pathological process under consideration, it, as it should, creates electrical impulses, but a second area of atypical activity also appears. This is the atrium, one or both at once (the latter case is more severe and poses a greater danger to health and life despite the general benign nature of the course). A vicious circle arises.
To eliminate the source of excitation, it is necessary to reduce the load on it at least for a while.
This is impossible to do under normal, everyday conditions. Outside help is needed. As a rule, medications are powerless here; surgical or minimally invasive intervention is required.
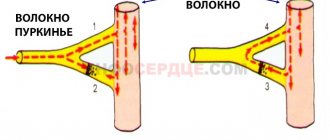
Closer to the heart
Conduction system of the heart
To better understand the causes and types of extrasystole, let’s move closer to the heart. Let's briefly touch on its anatomy and physiology. The human heart is a hollow organ that consists of four chambers. Two atria and two ventricles, together with large blood vessels, make up this organ. The heart has two sections - right and left. Normally, these sections do not communicate with each other, performing the function of the pulmonary and systemic circulation. “From head to toe,” this organ is permeated with conducting pathways along which the resulting impulse runs and causes the muscle layer of the atria and ventricles to contract.
The entire conduction system is represented by nodes or pacemakers and internodal tracts (pathways) connecting these nodes. The very first node is the most important, the most powerful, with the ability to generate an electrical impulse with a frequency of 60 to 80 in one minute. This is the sinus node. Next are the nodes that have the ability to generate an impulse in a descending order. Atrioventricular node (AV node), His bundle and Purkinje fibers.
This is what the heart looks like together with its conduction system. When an extraordinary impulse occurs in the atria, it can occur in the immediate vicinity of the sinus node, or a little further from it. Atrial excitation will proceed normally or in the opposite direction. The impulse will travel to the ventricles in the usual way. If the impulse originates in the ventricles, it will go backwards, going from the ventricles to the atria. These changes in the formation of the impulse and its conduction will be reflected in the electrocardiogram.
Classification
The distribution of pathological processes by type is possible in different ways. Clinically, such reasons are the most significant.
Depending on the origin of atypical abbreviations, they are distinguished:
- Heart variety. It is formed as a result of problems with cardiac structures. From a supervision point of view, it presents great difficulties.
- Endocrine, neurological, other types. They are more numerous, occur many times more often, but in terms of cure they are favorable.
Based on the frequency of the signals, they are called:
- Single. In this case, as the name suggests, against the background of normal functioning of the cardiovascular system, a few contractions occur outside the main rhythm. The frequency of extrasystoles varies from 20 to 30 per hour or about 700 per day. This is quite normal, this occurs, including in healthy patients without pathologies of cardiac structures or others. There is no great danger to life or health. Dynamic observation is indicated. If there are signs of deterioration, treatment is prescribed.
- Multiple or frequent atrial extrasystoles. Much more dangerous, since contractions appear in groups, cardiac arrest is likely. Whether this will happen or not is a moot point.
There are other classifications, but they do not have great clinical significance; they are used for a deeper understanding of pathological changes.
For example, bigeminy, trigeminy, and quadrigeminy are distinguished. This is every second, third or fourth pathological impulse. According to the place of origin, monotopic and polytopic, from the same ectopic focus, or from different ones.
Detailed ECG diagnostics
Functional extrasystoles that occur after stress and overload are difficult to detect during electrocardiography. Doctors prescribe additional examination methods:
- Daily Holter monitoring will allow you to see how the heart works over a 24-hour period.
- Bicycle ergometry is prescribed to assess heart rate during physical activity.
The results obtained may be characteristic of several pathological processes. For a more accurate diagnosis, it is recommended to undergo echocardiography (EchoCG) and donate blood for tests. Based on the final data, the doctor will make a diagnosis for the patient. It will be necessary to treat not the failure of the heartbeat, but the underlying disease causing it. If extrasystoles occur under the influence of irritating factors, then you should try to avoid them.
On the ECG, extrasystoles are displayed as premature ventricular or atrial complexes. From them, the doctor can understand where the focus of ectopic impulses is located and what the shape of the arrhythmia is. If cardiac symptoms are detected, the patient will only need to go to the clinic for an electrocardiogram. Additionally, other examination methods may be prescribed to accurately differentiate the pathological process that causes an abnormal heartbeat.
Source: MirKardio.ru
Causes of atrial extrasystole
The vast majority of people with atrial extrasystoles are not patients of the cardiologist, since they do not have specialized problems. The main role is played by subjective, self-correctable factors.
Among them:
- Use of antihypertensive drugs. The list of these is wide: from glycosides, ACE inhibitors to calcium channel blockers and others. With illiterate use and excessive amounts of medications, various types of arrhythmias are likely. Including a potentially lethal plan. There may also be an iatrogenic cause, when an insufficiently competent specialist is to blame.
- Caffeine abuse. Tea and other drinks have a tonic effect on the entire body, in particular on the heart and blood vessels. Tachycardia develops, usually of the sinus type. In more complex cases, generalized rhythm disturbances are likely, up to a complete stop of the organ’s functioning. Therefore, coffee and similar drinks are not recommended for patients prone to cardiac pathologies.
- Lack of sleep, prolonged fatigue. During the night's rest, the brain and the whole body “reboot”, metabolic phenomena normalize, and the body gets rid of toxic substances that are dangerous to health and life. If there is a lack of sleep, intoxication is possible. The heart begins to work harder due to the constant production of cortisol and stress hormones in large quantities. It’s hard to say what this entails. But such a thing does not bode well for a person.
- Alcohol abuse. Alcohol provokes vascular stenosis, increased blood pressure and resistance, and disruption of the rheological properties of blood. Here are the most common consequences of taking ethanol, even in minimal dosage. For some, alcohol is completely contraindicated, since the body is not adapted and cannot provide adequate resistance to neutralize the toxic substance. The maximum permissible dose of alcohol per day is 30-50 ml, no more. It is advisable to completely quit the bad habit.
- Stressful situation. Psychotraumatic periods are associated with increased synthesis of hormones from the adrenal cortex and pituitary gland. This ends with an increase in blood pressure and other consequences from the cardiac structures. It is impossible to avoid stress, but it is worth minimizing unfavorable moments. Relaxation techniques are shown. Their development does not require much labor.
- Tobacco smoking. It provokes the same phenomenon as alcohol consumption, but not right away. The effect is delayed, but much more lasting.
Temporary atrial extrasystole can also be provoked by the following problems:
- Myocardial infarction. The phenomenon is observed within 2-3 months from the moment of the incident. Normalization is carried out using medicinal methods.
- Arterial hypertension of any origin, regardless of type.
- Infectious and inflammatory diseases. Especially affecting the heart and its structures.
- Malformations of cardiac formations, both congenital and acquired.
- Violations of the exchange plan. Lack of potassium or magnesium.
Determining the root cause plays a big role in diagnosis. This is the only way to prescribe etiotropic treatment. In the absence of evidence for organic pathology, they speak of an idiopathic type of problem. Therapy is indicated to eliminate symptoms.
Treatment tactics
When treating single atrial extrasystole, it is necessary to limit coffee consumption
Therapy for single atrial extrasystole is as follows:
- In planning your daily routine
- Quitting smoking and drinking alcohol
- Limiting the consumption of coffee, as well as energy drinks and strong tea
- In the correction of pathologies of the heart, blood vessels, nervous system
Symptoms
Manifestations even in late stages, when several structures are involved, are minimal or completely absent. The problem can be detected only based on the results of objective studies: ECG, echocardiography, heart rate counting.
However, we can talk about the following signs:
- Feeling of pounding in the chest. In a normal state, a person does not feel the work of cardiac structures. This shouldn't happen.
- Tachycardia or reverse process. Acceleration of cardiac activity to 100 beats per minute or more, or 60 or less.
- Shortness of breath with little physical exertion. Against the background of intense mechanical activity, it can become more significant.
- Interruptions in the functioning of a muscle organ. They are felt especially strongly when extrasystoles occur. Patients describe them as missing beats and irregular rhythm.
In any case, the signs are non-specific, it is difficult to say anything specific.
Symptoms and signs
Patients with infrequent premature contractions often report no symptoms. Extrasystoles are detected in them during preparation for surgery. In other cases, manifestations appear against the background of a standard heart rhythm and are accompanied by a pause. It is visualized like “missed” beats or a feeling of stopping the heartbeat. When palpating the pulse in such patients, a loss of the pulse wave is recorded.
Patients also note that extrasystoles cause a feeling of cardiac arrest, falling from a height, or jumping from a springboard. Complaints are supplemented by sensations of irregular heartbeat. They are uncomfortable and cause significant anxiety. Symptoms that are aggravated by exercise are the most concerning and important. Other manifestations are also possible:
- fainting or dizziness;
- atypical chest pain;
- fatigue;
- fainting while coughing.
Diagnostics
Examination of patients with cardiac problems is carried out under the supervision of a cardiologist. As necessary, if there is a suspicion of a non-cardiac origin of the problem, third-party doctors are involved. Which ones exactly depend on the nature of the disease.
Approximate list of events:
- Interviewing the patient for complaints. The patient’s task is to provide as much information as possible so that the doctor has something to work with. What is important - he will determine for himself; it does not matter much to a person.
- Anamnesis collection. Bad habits or lack thereof, lifestyle, family history of pathologies. All these are important points that must be recorded in writing for further analysis.
- Measuring blood pressure numbers. It is carried out primarily to exclude hypertension, which can cause the process.
- Listening to heart sounds. He is usually normal, but is deaf. Rhythm disturbances are recorded already at this stage.
- Heart rate calculation. Using an automatic blood pressure monitor or the old “old-fashioned” way: a stethoscope and a watch. The second method is less accurate and informative.
- Daily monitoring using a Holter device. The preferred method for quickly assessing the state of the cardiovascular system in dynamics, against the background of normal living conditions of the patient.
- Electrocardiography. The main tool in the hands of a cardiologist. Allows you to catch even single extrasystoles that do not manifest themselves in any subjective way. Deciphering the results presents certain difficulties; you need decent experience in the field of cardiology. Less competent specialists often make mistakes and make incorrect diagnoses. Hence, inadequate therapy and, at a minimum, a complete lack of effect.
- Echocardiography. Ultrasound technique for assessing the condition of cardiac structures. Aimed at visualizing the heart. Gives a rather meager amount of information. Indispensable in the diagnosis of organ malformations.
- Load tests. To determine the system's response to physical activity. It is carried out with great caution; complications, including death, are possible. Doctors must be prepared to provide first aid.
- Angiography and Doppler scanning of blood vessels.
- MRI, CT as necessary.
All these studies are carried out in a complex. At the discretion of the cardiologist and other doctors, the list can be expanded or narrowed.
Prognosis and complications
Group extrasystole often turns into a more dangerous rhythm disorder (atrial flutter, fibrillation, paroxysmal tachycardia, atrial fibrillation, etc.). A complication may be chronic insufficiency of coronary, renal, and cerebral circulation.
In most cases, a single atrial extrasystole does not pose any danger to human life. In addition, scientific research has proven that 99% of people over the age of 50 have this pathology.
It is difficult to say what the prognosis of the disease will be for a particular person. This depends on what concomitant pathologies occur against the background of extrasystole. What is taken into account is not so much premature contractions, but the cause of their occurrence and the severity of the underlying disease.
Signs on cardiography
Among the characteristic features:
- Early appearance of the P wave. Its slight deformation.
- Normal heart rate.
- The compensatory pause is incomplete.
Atrial extrasystole is difficult to detect on an ECG, especially in the early stages. A full assessment is only possible by a specialist.
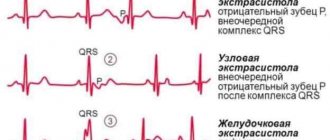
Signs of atrial extrasystole on an ECG and examples of films
There are several distinctive ECG signs of atrial extrasystole:
- premature appearance of a morphologically altered or negative P wave followed by a normal (sinus) QRST complex;
- a small compensatory pause after PE in the form of a straight line without teeth or complexes.
It may also be that the electrocardiogram displays the P wave, but the QRST complex that follows it does not. This is called blocked PE. Often repeated blocked PEs are confused with sinus bradycardia.
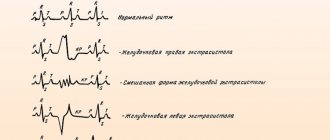
In my practice, I often see cardiograms in which atrial extrasystoles appear with a certain regularity (allorhythmia). There are the following types of allorhythmia:
- bigeminy – PE occurs after each normal QRST complex;
- trigeminy - PE after every second complex;
- quadrigeminy - PE after every third complex.
Very rarely, with PE, the QRS complex becomes wide and deformed, which makes it look like a ventricular extrasystole.
Sometimes the shape of the P is not the same in different leads. Then PE is called “polytopic atrial extrasystole”. I constantly observe this ECG picture in patients with a long history of smoking and suffering from COPD (chronic obstructive pulmonary disease).
To count the total number of extrasystoles and to diagnose other possible heart rhythm disturbances, I prescribe daily (Holter) monitoring.
Treatment
Therapeutic tactics are determined by the cardiologist in tandem with other doctors. Example treatment strategies include medications, surgery, and lifestyle changes.
Medicines. They are required in a small number of cases, since the pathological process has almost no organic origin, and if one is present, the tablets will be of little use.
List of drugs:
- Cardiac glycosides. Lily of the valley tincture, Digoxin and their analogues, it is important not to combine these medications with each other.
- Calcium channel blockers. It is better to use Diltiazem in medium dosage.
- Mineral complexes. Including Asparkam and some others. They are used at the discretion of the treating specialist; excess substances also do not carry a useful load.
Surgical intervention and minimally invasive tactics are required in a small number of clinical cases.
Among the techniques:
- Electrocardioversion. Restoring the functional activity of an organ using current. They resort as a last resort if tachycardia flows in parallel.
- Elimination of the pathological focus using classical atrial resection or endoscopic surgery.
Endovascular radiofrequency ablation is used somewhat less frequently. This is an innovative treatment method, but it is not always suitable.
Changing your lifestyle involves following a few tips.
Among them:
- Rejection of bad habits. Smoking, alcoholism and drug addiction are a direct path to pathologies not only of the cardiovascular system. In the next few years, or even sooner, lethal complications are possible.
- Normalization of sleep. At least 8 hours a day. In this case, at least a third of the time should be before 23.00.
- Drinking regime. 2 liters of water per day. There should be no dehydration. You should also not forcefully consume liquid.
- Physical activity. 1-3 hours of walking or exercise therapy. The main thing is that there is no physical inactivity.
- Proper nutrition. Anything is possible, but in moderation so that the diet does not turn out to be one-sided. There are no categorical contraindications in this case.
Risk factors
Doctors identify groups of patients who are most susceptible to developing atrial extrasystole. There is a high risk of deviation formation in:
- people belonging to the older age category;
- people with abnormal growth;
- patients with elevated cholesterol levels in the bloodstream.
Also, the risk of developing the disease is increased if you have bad habits. Smoking, drug use and alcohol-containing drinks increase the possibility of developing atrial extrasystole.
If there are risk factors for the formation of pathology, the patient should more carefully monitor his well-being. It is important to adhere to preventive measures.
Causes and symptoms
If we compare ventricular and atrial extrasystole, the second one will be less serious. There is a type of extrasystole that does not affect the heart with disease and is practically safe for the body - idiopathic.
Some of the main causes of the disease are:
- excess dose of caffeine;
- alcohol and tobacco abuse;
- constant emotional stress;
- fatigue;
- chronic lack of sleep;
- medications that have side effects such as increased heart rate;
- lack of magnesium and potassium in the body;
- Excessive use of the drug digoxin.
And also some heart diseases can provoke atrial extrasystole , so you should pay attention to them:
- general heart rhythm disturbances, which are severe and can lead to stroke;
- endocarditis is an inflammatory process of the inner lining of the heart;
- hypertension – high blood pressure;
- various defects of one of the valves of the heart muscle.
EXTRASYSTOLIA: stages of treatment
Extrasystole (ES) is the most common type of rhythm disturbance and is diagnosed in patients with a wide range of diseases, not only cardiac ones. At the same time, its clinical significance varies greatly among different patients, so the treatment of ES requires a differentiated approach. This message will outline the basic principles of treatment for various types of ES.
The first step necessary to select adequate treatment is an accurate diagnosis of ES with determination of its origin (ventricular or supraventricular). It is not difficult to suspect that a patient has ES when it is subjectively felt. Often the most unpleasant for the patient is “harmless” functional SE. With ventricular extrasystole (VES), the symptoms are more pronounced, apparently due to an increase in the duration of the pause (a feeling of “cardiac arrest” and a stronger first post-extrasystolic contraction of the heart). To make a diagnosis of ES, a standard ECG in combination with Holter monitoring (HM) is sufficient. Diagnosis of supraventricular extrasystole (SVES) can be difficult in the presence of a wide (E 0.12 s, due to aberrant conduction) QRS complex on the ECG, in most cases - as a right bundle branch block; “early” NVES (superposition of the P wave on the preceding T may cause an error in identifying the P wave); blocked NVES (premature P wave not conducted to the ventricles). To differentiate between VES and NVES with aberrant conduction, a comparison of the shape and coupling interval with previously recorded extrasystoles should be used.
The constancy of the coupling interval and the shape of the P wave (with NVES) or the QRS complex (with VES) is a sign of the monotopy of ES. The need for more accurate topical diagnosis of ES arises in the case of surgical treatment, which is preceded by an electrophysiological study (EPS). Induction of extrasystoles, completely identical to “natural” ones, using a localized stimulus, confirms the accuracy of the topical diagnosis.
CM is carried out to verify the diagnosis of PVCs (especially in the presence of rare extrasystoles that cannot be recorded on a standard ECG), to determine the mono- and polymorphism of PVCs and mainly to determine the number of PVCs during the day, their distribution by time of day and their relationship with various factors. . The presence of no more than 30 ES per hour is considered acceptable. Shorter monitoring may be used (for example, to assess the effectiveness of treatment). ES can also be first detected during various stress ECG tests. If there is a clear anamnestic connection between the occurrence of ES and exercise, these tests can be performed specifically to verify the diagnosis of ES (usually ventricular); in these cases, conditions must be created for possible resuscitation. The association of PVCs with exercise most likely indicates their ischemic etiology.
At the same time, idiopathic PVCs can be suppressed by physical activity.
The second stage - and one of the most important - on the path to selecting adequate therapy for ES is determining its etiology, knowledge of which, in addition to the possibility of carrying out etiotropic therapy for a number of diseases, allows you to determine the prognostic value of ES in a particular patient and select an antiarrhythmic drug. Therefore, all opportunities should be used to make an etiological diagnosis, which in therapeutic practice is of much greater importance than determining the electrophysiological mechanism of ES (reentry or trigger activity).
First of all, it is necessary to identify those causes of SE that can be eliminated (effective etiotropic therapy is possible), without which SE therapy will not be successful:
1. Abuse of tea, coffee, alcoholic beverages (including beer), heavy smoking, taking psychostimulants, drugs, methylxanthines, tricyclic antidepressants, thiazide and loop diuretics, Cavinton, nootropil, hormonal contraceptives, use of inhaled β-adrenergic agonists. The patient himself may note the connection between interruptions in heart function and one of these factors; in this case, along with underestimation, their role may also be exaggerated. In the case of a fairly acute development of ES, it is necessary to exclude hypokalemia, including that caused by taking diuretics. We should not forget about the possible arrhythmogenic effect of antiarrhythmic drugs IA, IC, III classes and cardiac glycosides (they can provoke not only PVCs, but also NPVS).
2. Hyperthyroidism (thyroid hormone screening is mandatory in patients with ES).
3. Myocarditis, including within the framework of infectious (including infective endocarditis) and autoimmune diseases. The connection between the first episode and “exacerbations” of extrasystole, which flows in waves (with periods of remission) with intercurrent infections, is the most characteristic sign of a history of myocarditis, which led to the formation of post-myocardial cardiosclerosis or remains active (cardiosclerosis is proposed to be considered only as one of the phases of latent myocarditis). In the absence of obvious clinical signs of myocarditis, this diagnosis may be supported by: nonspecific signs of inflammation; antibodies to the myocardium (especially the IgM class), Coxsackie viruses group B, ECHO, cytomegalovirus, Epstein-Barr virus, HIV (up to 10% of those infected suffer from myocarditis), streptococci; nonspecific changes in the T wave on the ECG and conduction disturbances, often at different levels; signs of pericarditis in combination with mosaic contractility disorders, subclinical valve regurgitation, moderate chamber dilatation (possibly only the atria), a moderate decrease in ejection fraction; increased troponin T levels (determined only during the first month of illness); decreased interferon levels and increased tumor necrosis factor (are additional markers of immune myocarditis). The most accurate method for diagnosing indolent myocarditis, the only manifestation of which may be ES, is a myocardial biopsy (not performed in most institutions).
In the absence of signs of myocarditis and the simultaneous presence of an inflammatory focus, which is difficult to “discount” when trying to identify the etiology of ES, it is appropriate to make an assumption about toxic-infectious myocardial dystrophy.
The diagnosis of “post-myocardial cardiosclerosis”, which implies the completion of the inflammation process and the impossibility of etiotropic treatment, is justified when identifying signs of inflammatory myocardial damage without immunological markers of current inflammation. It should be noted the possibility of the existence of a trigger mechanism for PVCs, sensitive to verapamil or β-blockers, in patients with post-myocardial cardiosclerosis.
4. Anemia. Its importance for the development of SE may be underestimated, but at the same time, against the background of an increase in hemoglobin levels, the course of SE significantly improves.
For other diseases accompanied by ES, the possibilities of etiotropic therapy are significantly limited (often it is impossible), however, making an accurate etiological diagnosis remains important. Similar causes of ES include the following factors:
- IBS. ES can serve as an early clinical manifestation of myocardial infarction, be of a reperfusion nature (and in this case it does not require treatment), reflect electrical instability in the area of the post-infarction aneurysm (reminiscent of infarction QRS) and be a manifestation of diffuse cardiosclerosis. When performing a treadmill test, the appearance of paired VVCs at a heart rate < 130/min in combination with ischemic ST changes is important. We can speak with confidence about the non-coronary nature of PVCs only after coronary angiography. NVES can also be a manifestation of coronary artery disease, but has a lesser effect on the prognosis in these patients.
- Dyshormonal myocardial dystrophy is usually diagnosed in women. In these cases, ES can occur with dysovarian disorders - in puberty, with premenstrual syndrome, against the background of ovarian dysfunction of various origins, with uterine fibroids (“myomatous heart”) and, of course, in the menopause. Often the stigma of trouble in this area is fibrocystic mastopathy. The presence of dyshormonal myocardial dystrophy can also be assumed in individuals with signs of dyspituitarism; in this case, of course, autonomic imbalance should also be taken into account - within the framework of hypothalamic-pituitary dysfunction. ES in such individuals can be either ventricular or supraventricular.
- Hypertrophic cardiomyopathy (HCM). PVC is one of the earliest symptoms and largely determines the prognosis; the development of NWES is uncharacteristic.
- Dilated cardiomyopathy. It is characterized by a combination of VES with NVES, which eventually turns into atrial fibrillation (AF). Often, PVC develops as part of alcoholic cardiomyopathy. For familial forms of the disease, a combination with AV blocks of varying degrees, Duchenne or Emery-Dreyfus myodystrophy is typical.
- Restrictive cardiomyopathy can also be accompanied by the development of VES and NSES in combination with blockades; the ECG shows a decrease in voltage. Amyloidosis can occur not only with restrictive changes, but also in the form of isolated atrial damage with the development of NVES and AF. In all cases of unclear heart disease, it is advisable to perform a biopsy of the mucous membrane of the gums and rectum for amyloid. Heart damage is most typical for primary and familial amyloidosis. Isolated cardiac damage does not exclude the presence of amyloidosis, but detection of weakness, fever, weight loss, purpura, macroglossia, lymphadenopathy, neuropathy, hepatosplenomegaly, enteropathy, and nephropathy makes the diagnosis more likely.
- Heart defects (congenital and rheumatic). PVC appears relatively early in aortic defects and may first develop during treatment of MA with cardiac glycosides. Mitral defects (especially mitral stenosis) are characterized by the early appearance of NVC due to overload of the right ventricle. Early development of PVCs with mitral valve disease may reflect active rheumatic carditis.
- Hypertonic disease. The severity of PVCs usually clearly correlates with the degree of left ventricular hypertrophy; a provoking factor may be the use of potassium-sparing diuretics. NVES is less typical and apparently reflects severe diastolic dysfunction with the development of mitral regurgitation.
- Chronic cor pulmonale. Characteristic is the appearance of NVES and right ventricular ES, which is combined with deviation of the heart axis to the right, signs of right ventricular hypertrophy, P-pulmonale, and conduction disturbances in the system of the right bundle branch.
- Sarcoidosis. Mostly young and middle-aged people are affected, more often women; isolated heart damage is uncharacteristic. In the presence of typical changes in the lungs, evidence of sarcoidosis of the heart can include: syncope, persistent cardialgia, a picture of dilated (less often, restrictive) cardiomyopathy, a combination of AV block, right bundle branch block and ventricular arrhythmias. The method for verifying the diagnosis is a biopsy (intrathoracic lymph nodes, liver, skin); An additional diagnostic test is to detect elevated levels of angiotensin-converting enzyme (synthesized by granuloma cells).
- Hemochromatosis. Mostly men aged 40–60 years are affected, but the heart is usually affected in those who become ill at a younger age. Heart damage (restrictive or dilated type) occurs in 15–20% of cases and can be combined with bronze coloration of the skin, arthropathy of the second and third metacarpophalangeal joints, hepatomegaly, and diabetes mellitus. NVES is more common than VES; AV block of varying degrees and supraventricular tachyarrhythmias are possible. The most specific are an increase in the level of serum iron, ferritin, a high - up to 55% or more - percentage of transferrin saturation, a decrease in the total iron-binding capacity of serum (TIBC), hemosiderin with fibrosis and cirrhosis in liver biopsy, as well as confirmation of a specific mutation in a genetic study.
- Mitral valve prolapse, especially in the presence of a prolonged QT interval (in 25%), mitral regurgitation and additional chordae (more often, but not necessarily in people with the stigmata of mesenchymal dysplastic syndrome). PVCs are more often observed in the presence of myxomatous valve degeneration and mitral regurgitation. NVES develops against the background of severe mitral regurgitation.
- Heart operations.
- Tumors of the heart (rarely) affecting the ventricles, pericardium, and atria.
- Heart injuries.
- "Heart of an Athlete" Characteristic is a combination of various rhythm disturbances (including ES) and conduction against the background of myocardial hypertrophy with inadequate blood supply.
A special etiological group consists of genetically determined diseases, in which arrhythmias (PVS, ventricular tachycardia (VT), less commonly, NVES, supraventricular tachyarrhythmias) are the main clinical manifestation. In terms of the degree of malignancy of ventricular arrhythmias, this group is close to ischemic heart disease. These diseases include primarily arrhythmogenic right ventricular dysplasia (ARVD), which must be excluded in all patients (especially young and middle-aged women without obvious heart pathology) who have mono- or polytopic right ventricular ES. When VT occurs, most patients experience syncope.
The criteria for the diagnosis of ARVD proposed by the European Association of Cardiology in 1998 are presented in the table.
Also characteristic are deviations of the EOS to the right, conduction disturbances in the system of the right bundle branch, the ratio of the QRS width in the opening. V2 and V4 more than 1.1. A normal ECG with an arrhythmic history of more than 5 years makes the diagnosis of ARVD unlikely. The diagnostic standard is cardiac MRI: lesions with a diameter of several mm are identified, and the content of adipose tissue is calculated. EchoCG reveals an increase in the end-diastolic diameter of the right ventricle and disturbances in its contractility. When ventriculography is specific, the combination of aneurysms of the wall of the right ventricle and increased trabecularity of the apex.
Other monogenic channelopathies (congenital syndromes of long and short QT interval, Brugada syndrome) are manifested almost exclusively by ventricular tachycardia - the development of VVCs (and especially NVES) is uncharacteristic for them. In WPW syndrome, PVCs and NPVS are not a common symptom; they are combined with other arrhythmias that are more specific to the syndrome (primarily supraventricular tachycardias and AF).
In the absence of all of the above reasons, ES is regarded as idiopathic. The so-called “functional” (as opposed to organic) extrasystole is characterized by the following features, which should be assessed together: the absence of visible organic damage to the heart; constitutional features (in particular, mesenchymal dysplasia syndrome); signs of vegetative dystonia; emotional lability; the occurrence of extrasystoles at rest; often young and middle-aged. It is often possible to identify a connection between NSES and the activation of the sympathetic (during exercise) or parasympathetic (during sleep, after eating, in the presence of a hiatal hernia, cholelithiasis, prostate adenoma) nervous system.
Idiopathic PVCs and tachycardia from the anterior wall of the left ventricular outflow tract occur against the background of vagotonia; ectopic activity predominates at night against the background of a slowdown in the basic rhythm, is suppressed by physical activity, PVCs have a large (not “R to T”) and constant coupling interval, arrhythmias are continuously recurrent in nature. PVCs and tachycardia from the outflow tract of the right ventricle have the morphology of left bundle branch block with moderate widening of the QRS complex and the “right” axis, are provoked by stress and physical activity, and are triggering.
At the third stage, a decision is made on the need for treatment of ES. Indications for the use of antiarrhythmic drugs (AAP) are:
a) poor subjective tolerability of ES (in some cases, psychotropic drugs can be used, AAP can be prescribed situationally); b) prognostically unfavorable ES: frequent (more than 1–1.5 thousand/day) NSES in patients with atrial dilatation, especially against the background of organic myocardial damage (heart defects, dilated cardiomyopathy) threatens the transition to AF; malignant (according to JT Bigger) VES (fainting or cardiac arrest in the anamnesis, there is a heart disease, the frequency of VES is 10–100/hour, stable paroxysms of VT are often detected) and potentially malignant (there is no history of fainting or cardiac arrest, VT is unstable) PVCs threaten the development of ventricular fibrillation; c) regardless of tolerability - frequent ES (more than 1.5–2 thousand/day), which itself can lead to arrhythmogenic cardiomyopathy with a decrease in myocardial contractility. Thus, it is possible to refrain from treatment only in cases of relatively rare ES, which is well tolerated and occurs in patients without serious organic myocardial damage, as well as without a history of episodes of AF and ventricular tachycardia. Moreover, this rule does not apply to acute cases of ES, when the cause of its occurrence is not entirely obvious, but nevertheless, one can think about the action of some arrhythmogenic factors that will persist over time and, in the absence of treatment, can lead to the consolidation of ES.
At the fourth stage (after deciding on the need for therapy), an AAP is selected taking into account the type of ES, its etiology, prognostic significance, initial ECG parameters (heart rate, PQ, QT intervals, duration of the QRS complex), previous treatment experience, concomitant diseases and allergic reactions.
It should be remembered that β-blockers and Ca antagonists (verapamil, diltiazem) are effective mainly for NVC and only for certain (trigger mechanism, usually idiopathic), rare variants of PVC, the features of which are described above. Of the class I drugs, allapinin, etacizine, disopyramide, propafenone and flecainide (not available in Russia) have a universal effect (on both NSES and VES). Quinidine should not be prescribed in the presence of ventricular ectopy; ethmozin and class IB drugs (lidocaine, mexiletine, diphenine) are effective only for PVCs. Representatives of class III AAPs d,L-sotalol and amiodarone are equally effective in cases of PVCs and NPVS; “pure” class III AAPs in isolated ES are usually not prescribed (due to their serious proarrhythmogenic effect, they are used only for paroxysmal tachycardias resistant to other drugs), although they are capable suppress both VES and NSES.
The etiology of ES only to some extent determines the choice of AAP. Thus, in case of thyrotoxicosis, ischemic heart disease, hypertension, HCM, the prescription of b-blockers (in case of HCM - and calcium antagonists) is pathogenetically justified, while in case of ES in combination with paroxysmal tachycardia against the background of WPW, verapamil is contraindicated; ajmaline can be used; for ARVD, d,L-sotalol is the most effective; for digitalis ES, diphenine is very effective (and safe); for PVCs, lidocaine is used predominantly in the acute period of myocardial infarction. Ethmozin is most effective for PVCs of ischemic origin. Taking into account the etiology, the prognosis of ES is also determined - serious organic damage to the myocardium in various diseases is associated not only with a high risk of transition of ES into life-threatening arrhythmias, but also with the risk of developing the proarrhythmic effect of AAP of classes IA, IC and III and requires caution when prescribing these drugs. In the early post-infarction period, only class IB drugs, amiodarone and, apparently, d, L-sotalol, are safe. For other organic pathologies, the approach must be individual. In order to reduce the risk of transition of PVCs to fibrillation, as well as the development of the proarrhythmic effect of AAPs (primarily tachycardia of the “pirouette” type), in addition to AAPs of classes I and III, beta-blockers should be prescribed whenever possible (especially in the presence of sinus tachycardia). If NVES is highly significant (for example, in patients with mitral stenosis), amiodarone can be immediately prescribed to suppress it. In case of VES, to improve the accuracy of the prognosis, a complex of predictors of sudden death is additionally used, each of which individually is not decisive: cardiac arrest or a history of sustained ventricular tachycardia; severe left ventricular hypertrophy; left ventricular ejection fraction less than 40%; presence of late ventricular potentials; increased dispersion of the QT interval over time or space; decreased heart rate variability.
It should also be remembered that most AAPs lead to an increase in the PQ interval (the exception is class IB) and a decrease in heart rate in sinus rhythm, with the most severe effects of propranolol, atenolol, betaxolol, high doses of verapamil and diltiazem (360–480 mg/day). day), d,L-sotalol (160–320 mg/day) and amiodarone (400–600 mg/day); Propafenone also has β-blocking activity. AAPs that increase the rhythm include allapinine (sympathomimetic), quinidine, disopyramide and novocainamide (anticholinergics); This effect is characteristic of etacizin and ethmosin to a much lesser extent. In patients with sick sinus syndrome and initial AV block, the reaction to taking “increasing” drugs may be the opposite. Slowing of intraventricular conduction (QRS widening) is caused by drugs IA, IC (ethacizine, flecainide) and, to a lesser extent, “pure” class III drugs. Amiodarone and d,L-sotalol can be prescribed for moderate (with caution for severe) QRS widening. Class I drugs and, to a lesser extent, class IA and IC drugs lead primarily to prolongation of the QT interval with the risk of developing tachycardia of the “pirouette” type - with a QT with more than 460–470 ms, these drugs should not be prescribed. QRS widening and QT interval prolongation are not a contraindication to the use of β-blockers and Ca antagonists. It should be noted that a moderate and non-progressive increase in the duration of the PQ interval (up to 0.22–0.24 s), as well as moderate sinus bradycardia (up to 50 beats/min) are not indications for discontinuation of drugs, subject to regular monitoring ECG.
Finally, if there is a history of ineffectiveness of one of the β-blockers or calcium antagonists in adequate doses, there is no point in prescribing another representative of the same class of AAP. At the same time, representatives of class I AAP, as well as amiodarone and d,L-sotalol, have significant differences and should be tested independently of each other (it does not make sense to replace the ineffective ethacizin with ethmosin or poorly tolerated ethmosin with ethmosin, since ethmosin is weaker metabolite of etacizine). If you want to prescribe etacizin, you should exclude an allergy to honey.
So, there is all the preliminary data in order to choose one or another AAP. In case of NVC, especially in patients with tachycardia, stress-induced ES, in the presence of other indications for the use of β-blockers (coronary heart disease, arterial hypertension, sympathoadrenal crises, etc.) or verapamil (bronchial asthma, variant angina, nitrate intolerance in patients with coronary artery disease) Treatment of NJES begins with these AAPs. β-blockers include propranolol 30–60 mg/day, atenolol or metoprolol 25–100 mg/day, bisoprolol 5–10 mg/day, betaxolol 10–20 mg/day, nebivolol 5–10 mg/day); verapamil or diltiazem are prescribed in doses of 120–480 mg/day. In case of simultaneous presence of NZHES and VES, a more rational drug is d,L-sotalol (80–160 mg/day). At the same time, patients with vagus-mediated NVES are prescribed belloid, 1 table. 4–5 times a day, small doses of teopec (50–100 mg 2–3 times a day and at night), nifedipine, taking into account their rhythm-increasing effect; in this case, the circadian rhythm of NVES is taken into account (if NVES occurs against the background of nocturnal bradycardia, drugs that increase the rhythm should be prescribed at night).
If there is a tendency to bradycardia, AAPs that increase the rhythm can be immediately prescribed (disopyramide 200–400 mg/day or quinidine-durules 400–600 mg/day, or allapinin 50–100 mg/day), which are not only safer, but also allow you to act on the pathogenesis of brady-dependent NSES. It makes sense to start treatment with drugs IA or IC class (propafenone is prescribed in a dose of 600–900 mg/day, etacizine - 100–200 mg/day, flecainide - 200-300 mg/day, ajmaline - 200-400 mg/day). patients with a high prognostic significance of NVES, when class II and IV AAPs are generally not so effective. Prescribing amiodarone (200–300 mg/day) for NSES, taking into account the numerous side effects, is advisable only if other therapy is ineffective; however, if it is necessary to quickly achieve maximum effect, amiodarone can be prescribed immediately (without testing other drugs), in a rapid saturation mode. When treating patients with an undulating course of NZHES, one should strive for complete withdrawal of the drug during periods of remission (excluding cases of severe organic damage to the myocardium).
For PVCs of a benign or potentially malignant nature, therapy begins, as a rule, with the prescription of class I AAP (in addition to the previously mentioned universal drugs - ethmozin 400-600 mg / day), and only if they are ineffective - amiodarone or d, L-sotalol. Mexiletine 400–600 mg/day and diphenine 0.117, 1 tablet each. 3 times a day (in the absence of glycoside intoxication) are usually inferior to other AAPs and are prescribed only if there are contraindications to more active treatment. Sometimes novocainamide can be used - 2–4 g/day, i.e. 1–2 tablets. 4–6 times a day, the effectiveness of which for PVCs is quite high, but the dosage regimen for oral administration is inconvenient. For malignant and potentially malignant (in the case of a previous heart attack) PVC, it is preferable to prescribe amiodarone (300–400 mg/day, effective in approximately 50% of cases) or d,L-sotalol (80–320 mg/day). However, d,L-sotalol should be used only in cases where amiodarone is contraindicated or ineffective. In patients with life-threatening ventricular arrhythmias, the development of thyroid dysfunction is not a reason to discontinue amiodarone. G. A. Melnichenko, N. Yu. Sviridenko et al. (2004) developed an algorithm for monitoring and normalizing thyroid function (both in hypothyroidism and thyrotoxicosis) during long-term therapy with amiodarone. It should be noted that in this category of patients therapy with class I antiarrhythmics is not excluded. Their effectiveness in general is significantly less than that of amiodarone, and the incidence of proarrhythmic effect is higher, however, in a particular patient, a class I drug may be the most effective and safe.
Frequent PVCs require parenteral therapy in cases of acute occurrence or increase in frequency in patients at high risk of sudden death. Lidocaine or amiodarone is administered intravenously as a bolus and subsequently as a drip. The frequency of PVCs may decrease during therapy with β-blockers (with myocardial infarction).
An ineffective drug is usually completely discontinued, and another AAP is prescribed as monotherapy - thus, all potentially effective AAPs for a given patient are consistently tested. If monotherapy is insufficiently effective, combinations of AAPs can be used; in particular, if high doses of d,L-sotalol and allapinine are poorly tolerated, their combination using lower doses is indicated (40 mg x 2 sotalol + 25 mg x 2 or 12.5 mg x 4 allapinine); combinations of allapinin with β-blockers, calcium antagonists are possible, which successfully combine the multidirectional effects of drugs on heart rate, but increase the inhibitory effect on AV conduction; combinations of quinidine (0.4–0.6 mg/day) with β-blockers, calcium antagonists. The prescription of amiodarone in combination with β-blockers for malignant PVCs, especially with persistent sinus tachycardia, is justified. Combinations of class I and III AAPs (especially those including amiodarone) have the most powerful effects; however, with isolated ES, such aggressive (and unsafe) therapy is usually not required.
Along with the appointment of AAP, the following options should be used:
- Prescription for 1–2 months of glucocorticoids (prednisolone 10–20 mg/day), aminoquinolones (delagil 250–500 mg/day, plaquenil 200–400 mg/day) or NSAIDs (butadione, ibuprofen, voltaren) if current myocarditis is suspected.
- Prescription of tincture of hawthorn, motherwort, as well as benzodiazepines that have an antiarrhythmic (phenazepam 0.5–1 mg) or vegetotropic (clonazepam 0.5–1 mg) effect and improve the subjective tolerability of NVES.
- Prevention of sudden death (with malignant PVC) using aspirin, ACE inhibitors (which apparently also have an antiarrhythmic effect), statins.
- In patients with moderate atrial dilatation, without heart defects, with ischemic and alcoholic origin of ES, with concomitant hyperlipidemia - the use of hemosorption or plasmapheresis with a clear connection between the “exacerbation” of ES with infection, an increase in ES over the last 6 months, with the development of resistance to previously effective antiarrhythmics (especially amiodarone), ineffectiveness of drug therapy or contraindications to it, if it is necessary to achieve an antiarrhythmic effect in the coming months (before surgery).
The fifth stage in selecting therapy for ES can be considered adequate monitoring of the effectiveness and safety of treatment. The effectiveness of AAP can be assessed empirically (observation of the patient while taking therapeutic doses), during an acute test (after a single dose of half the daily dose), using a standard ECG (the safety of treatment is assessed to a greater extent; the effect can only be assessed with frequent ES) and optimally - control HM. Firstly, the drug can be evaluated in an acute test (half of its daily dose is prescribed at once, chemotherapy is carried out within 2-3 hours before taking the AAP and for the same time after taking it), however, extrapolation of the data obtained in the acute test to the results of long-term use AAP is not always possible. Secondly, with the help of CM, the effect of planned therapy is assessed - daily CM is carried out before the appointment of an AAP and on the 2-3rd day of its administration, treatment is considered effective when tachycardia runs, steam, early ES disappear, ES decreases by 75-80% after days; An assessment is made of the proarrhythmic effect that occurs during the treatment of conduction disorders.
Finally, at the sixth stage , the insufficient effectiveness of drug therapy serves as the basis for the use of surgical (interventional) techniques. In all cases of frequent (up to 10 thousand/day or more) ES - including those with a known etiology - and resistance to 3-5 AAPs, the question of conducting EPI mapping and ablation of arrhythmogenic foci should be raised. To preliminarily identify such lesions, cardiac MRI is performed. The need to prescribe AAP after ablation often remains (it is lower in patients with idiopathic PVCs and post-myocardial cardiosclerosis), but their effectiveness can be significantly higher than before the procedure; less often it is possible to completely abandon AAP 3–12 months after ablation. Surgical treatment (ablation of arrhythmogenic foci) for ARVD should be quite early, since simultaneously with the relief of arrhythmias (in 75–80%; in 40–50% of patients - with subsequent administration of AAP), fatty replacement of the myocardium is stopped. In later stages of the disease, heart transplantation is necessary. A difficult option for surgeons may be left ventricular triggered PVC, in which the arrhythmogenic focus is located subepicardially near the ostia of the coronary arteries - the risk of developing coronary artery stenosis makes it necessary to refuse radical treatment, however, ablation of the zone adjacent to the arrhythmogenic focus can lead to a change in its electrical properties and the appearance of sensitivity to previously ineffective AAP. In patients with PVCs with post-infarction aneurysm, in principle, the more preferable intervention is aneurysmectomy, which allows simultaneously with the elimination of the arrhythmia substrate to improve hemodynamics, however, such a large-scale operation is not always feasible. In the absence of ventricular tachycardia, the indication for aneurysmectomy is congestive heart failure in combination with PVCs, including allorhythmia.
The need for another type of surgical treatment (implantation of a permanent pacemaker) may arise both in the early stages of selecting therapy and after the prescription of AAP: the impossibility of prescribing adequate doses of AAP due to the development of severe concomitant bradycardia, pauses of ≥ 3 s, and conduction disturbances is an independent indication to install a stimulator.
It is also important to correctly determine the duration of antiarrhythmic therapy. In patients with malignant PVC or NPV that threatens the development of MA, AAP therapy should be continued indefinitely. For less malignant types of ES, therapy should be quite long (up to several months), with the possibility of gradual (due to the danger of the rebound effect) its withdrawal. After discontinuation of continuous therapy, the patient should be advised to constantly carry a well-proven AAP with him and take it when cardiac dysfunction recurs. Usually this is enough.
A. V. Nedostup, Doctor of Medical Sciences, Professor O. V. Blagova , Candidate of Medical Sciences, Associate Professor of MMA named after. I. M. Sechenova
Types and stages of the disease
If we take into account the number of consecutive contractions that appear, we can determine single atrial untimely contractions of the heart, triplets. This occurs when undergoing non-periodic contractions in a row. This fact is called unsustainable tachycardia. If extrasystoles are arranged in a certain order, they are called allorhythmia, which in turn is divided into several types:
Structure of the heart
- bigeminy - every normal impulse is “pursued” by a pathological one, which creates a consequence;
- trigeminy - arrhythmic contractions are formed with periodic precision, every third;
- quadrigeminy - here the periodicity changes to 4 contractions.
Based on the source of pulse formation, they are divided into two types:
- Monotopic - the site of formation coincides, the same place of origin;
- Polytopic - the place of origin is different, the impulse arises in different areas.
The difference in degree occurs according to the relationship with the last complex of the ventricle:
- early degree - contractions that go beyond the norm within one hour are considered. The permissible norm is no more than 30;
- late degree - the permissible norm is more than 30.
They are further divided into polytopic extrasystoles and paired extrasystoles.