Description of the pathology
When the sinus node is weakened or stops working, and this happens either on an ongoing basis or from time to time, ectopic rhythms arise (or they are also called replacement rhythms).
Their frequency is less than that of sinus rhythm. Ectopic atrial rhythm can be considered non-sinus. The further away its source is, the less frequent its pulses will be. What is the reason for changes in heart function?
Treatment
Treatment measures will not be required if the adult or child does not experience any discomfort when the anomaly develops, and they do not have heart or other diseases. The occurrence of atrial rhythm in this situation is not dangerous to health.
Otherwise, the therapeutic effect is carried out in the following directions:
- Accelerated pathological atrial rhythm is treated with beta blockers (Propranalol, Anaprilin) and other drugs that reduce heart rate.
- For bradycardia, medications are prescribed that can accelerate the slow rhythm: drugs based on atropine, sodium caffeine benzoate, and plant extracts (Eleutherococcus, ginseng).
- Vegetative-vascular disorders that cause ectopic rhythm require the use of sedatives “Novopassit”, “Valocordin”, motherwort tincture, valerian.
- To prevent heart attack, it is proposed to use Panangin.
- In addition to antiarrhythmic drugs (“Novocainamide”, “Verapamil”), in case of irregular rhythm, specific treatment is prescribed after establishing the specific cause of the disorders that have developed.
- In severe cases that are not amenable to standard drug treatment, cardioversion and installation of an artificial pacemaker are used.
What are the signs of ectopic atrial rhythm?
As already mentioned, the underlying disease leads to non-sinus rhythms. It is not characterized by any specific symptoms. The main ailments and causes of the rhythm determine the symptoms.
Below are symptoms that you should pay close attention to and then consult a doctor immediately:
- an attack of paroxysmal tachycardia begins suddenly and ends just as suddenly;
- there are no warning signs of an attack;
- there is no shortness of breath or heart pain at the beginning of the attack;
- the emergence of feelings of severe anxiety and fear;
- the appearance of motor restlessness, such that a person seeks a body position that will help stop the attack;
- a person’s hands begin to tremble, his vision darkens, his head begins to spin;
- the appearance of increased sweating;
- presence of nausea and bloating;
Other symptoms
There are certain signs of non-sinus rhythm. Depending on what the possible ectopic atrial rhythm is accompanied by, they can be different:
- So, for example, with extrasystoles the heart may work intermittently, a person feels as if his heart is stopping, feels heat in the throat and heart. But these symptoms may not exist. Excess body weight and hypersthenic constitution often lead to vagotopic extrasystoles.
— In a child, an attack of paroxysmal tachycardia leads to fainting, darkening of the eyes, dizziness, feelings of tension and anxiety, pallor, cyanosis, shortness of breath, and abdominal pain. This is what distinguishes ectopic atrial rhythm in children.
Reasons for rhythm changes
Non-sinus rhythms can occur due to changes occurring in the area of the sinus node, as well as in other conducting sections. These modifications can be:
- sclerotic;
- ischemic;
- inflammatory.
Ectopic disorders are classified in different ways. There are several forms:
- Supraventricular rhythm of ectopic nature. Its causes are an overdose of cardiac glycosides, as well as vegetative dystonia. It rarely happens that this form is caused by increased automatism of the ectopic focus. In this case, the heart rate will be higher than with an accelerated or replacement rhythm of an ectopic nature.
- Ventricular rhythm. Typically, this form indicates that significant changes have occurred in the myocardium. If the ventricular rate is very low, ischemia may occur, affecting important organs.
- Atrial rhythm. It often occurs in the presence of rheumatism, heart disease, hypertension, diabetes mellitus, ischemia, neurocirculatory dystonia, also even in healthy people. As a rule, it is present temporarily, but sometimes it lasts for a long period. It happens that atrial rhythm is congenital.
Changes occurring in the myocardium due to neuroendocrine influences can also occur in children. This means that in the child’s heart there are additional foci of excitation that function independently of each other. Such violations are divided into several forms:
- active: paroxysmal tachycardia and extrasystole;
- accelerated: atrial fibrillation.
The disease can occur even in a child.
Ventricular extrasystoles in childhood begin to develop in cases of cardiac organic pathology. It is very rare, but there are cases when this type can be diagnosed in a healthy child, even a newborn.
Against the background of a viral infection, attacks of paroxysmal tachycardia occur at an early age, which can occur in a very severe form, called supraventricular. This is possible with congenital heart defects, atropine overdose and carditis. Attacks of this form often occur when the patient awakens and changes body position.
to the point ↑
Methods for diagnosing ectopic rhythm
If a person exhibits the above symptoms, he needs to urgently consult a physician or cardiologist. The specialist will prescribe an ECG, which will show certain changes in the heart or ectopic atrial rhythm.
The R wave changes its configuration during atrial rhythm. It does not have clear diagnostic signs. The PQ interval does not change with left atrial rhythm. Due to normal excitation along the ventricles, the QRST complex does not change. There will be a positive PaVR and a negative P in the third and second leads aVF when the pacemaker is located in the left and right atria, namely in their lower sections. The exact location of the ectopic rhythm is not determined in cases of inferior atrial rhythm.
In a right heart rhythm, the source of automaticity (P-cells) will be located in the right atrium. This is how ectopic atrial rhythm manifests itself in adolescents.
Children also require a thorough diagnosis. With atrial extrasystoles, the P wave changes. The PQ interval is shortened, an incomplete compensatory pause and a narrow ventricular complex are observed.
What is ventricular ectopic activity?
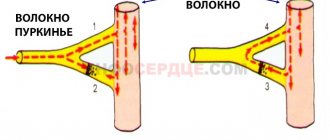
Ventricular ectopic impulse
is carried out through the ventricles not through the His-Purkinje system, but through the relatively slowly conducting myocardium. A change in the sequence and slower activation of the ventricles leads to the fact that the developing ventricular complexes become deformed and widened.
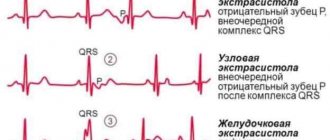
The complexes are premature, wide (0.12 s) Changed in shape (deformed) It is not preceded by a premature P wave Several terms are used to describe the location of the source, the time of occurrence and the number of ventricular extrasystoles.
Ventricular extrasystole
.
Scheme
. a Left ventricular extrasystole with a compensatory pause (picture of PNPG block). b Right ventricular extrasystole with a compensatory pause (picture of LBP block).
Characteristics of the source (focus) of ventricular extrasystole
Ectopic complexes of the same shape, following with the same coupling intervals, arise in the same focus. They are called “monofocal”, “monomorphic”, “monotopic”. Ventricular complexes that differ in shape and coupling intervals suggest the presence of more than one focus. Such extrasystoles are called “ multifocal”
", "
polytopic
", "
polymorphic
".
The moment of occurrence of ventricular extrasystoles
Ventricular ectopic complexes
, which occur very early in the cardiac cycle, can superimpose the T wave of the previous contraction and are referred to as “R on T” extrasystoles. Most episodes of ventricular fibrillation (VF) and many episodes of ventricular tachycardia (VT) are initiated by R to T beats, although this does not mean that R to T beats always cause these forms of arrhythmia.
Ventricular extrasystoles
, occurring only slightly prematurely in the cardiac cycle, may by chance occur immediately after the P wave caused by the normal activity of the sinus node: the P wave, therefore, unlike an atrial extrasystole, will not be premature. Such ventricular extrasystoles are called end-diastolic.
Usually after ventricular extrasystole
there is a pause. When such a pause is absent and the extrasystole thus appears “sandwiched” between two normal complexes, the extrasystole is called interpolated.
Ventricular extrasystoles frequency
When extrasystoles
follow after each sinus complex, the term “bigeminy” is used. If extrasystoles follow a pair of normal complexes, this is “trigeminy”. When two ectopic complexes follow in a row, they are designated by the term “paired extrasystole”, or “couplet”. “Gulp” refers to more than two consecutive ectopic complexes.
Atrial activity of ventricular extrasystoles
Manifestation of atrial activity after ventricular extrasystole
depends on whether the ventricular impulse is conducted in a retrograde direction, i.e. through the AV connection to the atria. If this occurs, an inverted P wave is formed, which often overlaps the ventricular ectopic complex itself and can be hidden by it.
In cases where the AV connection
does not conduct ventricular impulses to the atria, atrial activity continues regardless of ventricular activity; only in these cases, after a ventricular extrasystole, can a complete compensatory pause be seen (when the interval between the pre- and post-extrasystolic sinus complexes is equal to twice the duration of the sinus cycle).
Occasionally, the ventricular impulse may "spill" into the AV junction
only partially. In this situation, the next sinus impulse may reach the AV junction while it is still partially refractory, resulting in slower conduction and prolongation of the PR interval. This phenomenon of “hidden retrograde conduction” often occurs after interpolated ventricular extrasystoles.
Causes of ventricular extrasystole and its significance
Ventricular extrasystole
is a very common phenomenon, and its incidence in the general adult population increases with age. Causes of ventricular extrasystole include acute infarction or myocardial ischemia, arterial hypertension; myocardial damage caused by previous MI, myocarditis or cardiomyopathy; mitral valve prolapse, valvular heart defects, digitalis intoxication. However, often no signs of heart disease are found.
In patients with symptomatic and/or frequent ventricular premature beats
its cause should be sought using non-invasive testing methods, including a careful analysis of the 12-lead ECG, echocardiography and, if necessary, exercise testing.
Single ventricular extrasystoles
recorded on a regular ECG, and even complex forms of extrasystole (i.e., frequent, multifocal, “R on T” or salvo) extrasystoles recorded during ambulatory ECG monitoring can be incidentally detected in individuals with a healthy heart and are not necessarily pathological or have any prognostic significance.
On the other hand, some observational studies in adults
(mainly men) who underwent a test with dosed physical activity, it was shown that the appearance of frequent ventricular extrasystole during exercise and especially immediately after its cessation is associated with an increase in mortality (about 3 times) over the next 5-15 years.
In patients with irreversible structural myocardial damage
Due to coronary heart disease (CHD), there is a correlation between the severity of damage and the frequency of ventricular extrasystoles. According to recent data, ventricular premature beats should be considered as an additional and independent risk factor, but there is no evidence that its suppression with antiarrhythmic therapy improves the prognosis.
Indeed, it has been shown that some antiarrhythmic drugs
increase mortality in patients with ventricular premature beats after MI.
Usually extrasystoles
are asymptomatic. However, some patients still experience discomfort. They may be concerned about a feeling of irregular heartbeat due to premature contraction or subsequent compensatory pause, as well as a feeling of “heavy beats” caused by an increase in the strength of the post-extrasystolic contraction.
Patients may be anxious at the thought that irregular heartbeat
is a warning sign of a heart attack or other serious heart problems.
In some cases, patients with a structurally healthy heart
For those experiencing discomfort due to ventricular extrasystole, it is difficult to explain the situation and reassure them. In such situations, therapy may be required to reduce symptoms. Beta blockers may be effective, especially in the treatment of patients whose symptoms are related to exercise.
For patients with a structurally normal heart and no signs of CAD
Administration of flecainide may be helpful. Avoiding caffeine is generally recommended, but this is rarely effective.
The significance of ventricular extrasystole in acute myocardial infarction (MI) is discussed in a separate article on the website (we recommend using the search form on the main page of the website).
a — Ventricular extrasystole of the “R to T” type, which in this case initiates ventricular fibrillation (VF). b - the 3rd complex is an end-diastolic ventricular extrasystole. It is preceded by a well-timed P wave.
a — ECG recorded simultaneously in leads V1 and V2. Two end-diastolic ventricular extrasystoles can be seen. The second of them imitates the picture characteristic of Wolff-Parkinson-White (WPW) syndrome. b — Interpolated ventricular extrasystole. In the post-extrasystolic sinus complex, an increase in the PR interval can be seen due to hidden retrograde conduction.
a — Ventricular bigeminy. b — Ventricular trigeminy.
a - After the 1st sinus complex there follows a pair of ventricular extrasystoles. b - the 3rd complex is a ventricular extrasystole, the excitation from which is carried out to the atria, which led to the appearance of a negative P wave (lead aVF). After the extrasystole, you can see the complex slipping out of the AV junction.
In case of intoxication with cardiac glycosides
When intoxicated with digitalis, polytopic extrasystoles occur, which lead to ventricular fibrillation. Immediate discontinuation of the drug and treatment with Inderal, Potassium, and Lidocaine are required. Unithiol and diuretics will help remove intoxication. What else should be done when diagnosed with ectopic atrial heart rhythm?
Sometimes the carotid sinus is massaged for 20 seconds on the left and right sides if there is a supraventricular form. Pressing on the stomach and eye area helps. Lack of relief requires the use of beta blockers. They are administered at a slow speed, and monitoring of pulse and blood pressure is necessary. Mixing Propanol and Verapamil intravenously is not recommended.
Forecast of ventricular extrasystole
With ventricular extrasystole of types 1 and 2, the prognosis is favorable. The disease has virtually no effect on the patient’s quality of life and does not cause severe consequences.
With ventricular extrasystole of type 3 and higher, the prognosis is relatively favorable. With timely detection of the disease and initiation of therapy, you can completely get rid of symptoms and prevent complications.
The course of ventricular extrasystole depends on its form, the presence of organic heart pathology and hemodynamic disorders. Functional ventricular extrasystoles do not pose a threat to life.
Meanwhile, ventricular extrasystole, developing against the background of organic heart damage, significantly increases the risk of sudden cardiac death due to the development of ventricular tachycardia and ventricular fibrillation.
What to do if the attack does not stop?
If the attack does not stop and continues for some time, the patient’s condition worsens, electropulse therapy is used. Intoxication with cardiac glycosides is a contraindication to such therapy. For frequent and severe attacks, cardiac pacing is used continuously.
Complications may include exacerbation of heart problems. Timely consultation with a doctor will ensure the absence of ectopic rhythm, since the underlying diseases will be cured or at least controlled. Therefore, it is important not to panic if an atrial ectopic rhythm is detected on the ECG. We've looked at what it is.
Symptoms of a slow or fast heartbeat
The manifestations of ectopic heart rhythms depend entirely on how far the new pacemaker is located from the sinus node. If its localization is in the cells of the atria, then there are often no symptoms, and the pathology is diagnosed only on an ECG.
Atrioventricular rhythm can be with a pulse rate close to normal - from 60 to 80 contractions per minute. In this case, it is not felt by the patient. At lower values, paroxysmal dizziness, fainting, and general weakness are observed.
Extrasystole gives the feeling of a freezing heartbeat, followed by a sharp shock in the area of the apex or sternum, after which everything returns to normal. The intensity and frequency of these symptoms depends on the frequency of extraordinary contractions.
Atrial bradycardia goes unnoticed if the number of beats per minute is about 60; a rarer pulse is accompanied by increased fatigue and drowsiness due to oxygen starvation of the brain.
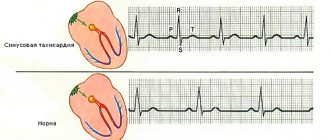
Paroxysmal tachycardia is manifested by a sudden acceleration of the heart rate, reaching 150 beats/minute, and the pulse can be rhythmic and not exceed 100. This is due to the fact that not all contractions lead to effective cardiac output. Complaints are associated with a lack of myocardial nutrition - pain or burning behind the chest, lack of air.
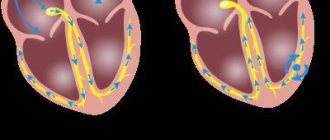
Atrial fibrillation is a disordered contraction of different groups of muscle fibers. Its rhythm ranges from 150 to 50 beats. The tachysystolic form (above 100) provokes attacks or constant rapid heartbeats, and the bradysystolic form (up to 50 contractions) provokes fainting and weakness.
Atrial fibrillation due to cardiac arrhythmia
Ventricular rhythm occurs when the heart muscle is severely damaged. Its speed does not exceed 30 - 40 beats, so it occurs with attacks of loss of consciousness. If there is a pause of more than 1 - 2 minutes between successive contractions, cardiac arrest is possible.
Watch the video about the causes of heart rhythm disturbances: