Pacemakers (pacers) are electronic devices that cause the heart to contract using electrical impulses, thereby restoring or maintaining a normal heartbeat. In our article we will talk about situations when pacemakers are necessary, their types and precautions for patients with an installed pacemaker.
The conduction system of the heart and the “natural pacemaker”
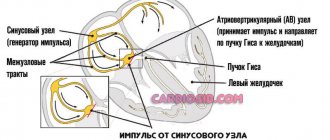
The heart has its own system of nerve fibers through which impulses are transmitted for myocardial contractions. It is called the conducting system. The electrical signals that travel along it set the heart rhythm and ensure coordinated contraction of the heart chambers for the most efficient pumping of blood.
Electrical signals, or impulses, are automatically created in a special collection of cells called the sinus node. This node is sometimes called a natural pacemaker. Each time an impulse is generated, it passes through the upper chambers of the heart (right and left atria). It causes the muscles of the atria to contract, pumping blood into the lower chambers - the right and left ventricles.
The electrical signal then travels to another special area located between the atria and ventricles, the atrioventricular node. Here the signal speed is momentarily reduced to allow the atria to contract fully.
From the AV node, the impulse goes to a system of fibers called the His bundle, and then passes along its right and left legs, going respectively to the right and left ventricles. The signal quickly spreads throughout all parts of the ventricles, causing their muscles to contract in a coordinated manner. As a result, blood from the right ventricle is pumped into the vessels of the lungs, and from the left - into the aorta and into the vessels of the whole body.
ECG during cardiac pacing (ECG during asynchronous cardiac pacing)
ECG with asynchronous cardiac pacing. The stimulating electrode is located in the right ventricle. The QRS complex is wide and shaped like a left bundle branch block. An artifact is visible before each QRS complex. The rhythm of ventricular contraction is correct.
Characteristic ECG signs during pacing with a fixed pulse frequency:
- constant pulse frequency;
- artifact before the ventricular QRS complex;
- widened and deformed ventricular QRS complex, reminiscent of the shape of the ventricular complex with complete blockade of one of the bundle branches;
- ST segment and T wave, located discordant to the main wave of the ventricular complex;
- The location of the electrical axis of the heart depends on the location of the stimulating electrode.
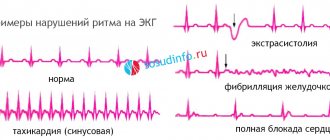
Heart rhythm disturbances
The conduction system must function normally for the heart to beat at the right rhythm and effectively pump blood. Disturbances in the passage of electrical impulses are called arrhythmias. This is a general term meaning that there are problems in the conduction system and the heart rhythm is changing.
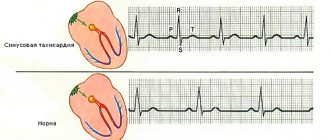
Bradyarrhythmias are rhythm disorders with an abnormally slow heartbeat. Most bradyarrhythmias are associated with one of two problems: sinus bradycardia or conduction block.
Sinus bradycardia occurs when the heartbeat is too slow because the “natural pacemaker” (sinus node) is working too slowly. This condition is the norm for well-physically trained people. In other cases, a pulse below 50 while awake requires examination by a doctor.
Heart block is a general term, not entirely correct from a medical point of view, which means that there are changes in the conduction system of the heart. They cause the electrical signal to travel too slowly or stop completely. Installation of a pacemaker may be necessary for the following types of this disorder:
- Atrioventricular (AV) block of the third degree, or complete, when impulses from the sinus node reach the AV node and are blocked there. At the same time, its own source of ri is formed in the ventricles, which produces impulses for heart contractions with a frequency of about 40 per minute.
- Sinoatrial (SA) block of the third degree, when the impulse does not exit the sinus node itself. At the same time, “spare” pacemakers also begin to function, but they cannot ensure the normal rate of heart contractions.
Bradysystolic form of atrial fibrillation (atrial fibrillation), when the atria contract chaotically, and only a small part of the electrical signals from them enters the ventricles.
The heart beats irregularly and slowly. This condition does not apply to blocks, but can sometimes be complicated by complete AV block (Frederick's syndrome develops), and in this case it is very dangerous.
Symptoms and reasons for installing an pacemaker
The manifestations of arrhythmia depend on its type and other factors, especially if a person has an underlying serious heart disease. Sometimes there are no symptoms, but often people who need a pacemaker have the following complaints:
- fainting, often with pallor, short-lived;
- dizziness and lightheadedness;
- feeling of irregular heartbeat;
- extreme fatigue, confusion;
- constant shortness of breath.
The decision whether to treat an arrhythmia with pacing depends largely on the presence and severity of these symptoms.
The most common diseases that may require pacemaker installation are:
- cardiac ischemia;
- previous myocardial infarction (post-infarction cardiosclerosis);
- some congenital heart defects;
- hereditary and genetic abnormalities that can lead to arrhythmia (for example, long QT syndrome);
- sick sinus syndrome;
- dilated and hypertrophic cardiomyopathy;
- natural aging of the heart muscle.
Indications for pacemaker installation
Direct indications for pacemaker implantation:
- sick sinus syndrome, accompanied by a rare heartbeat (less than 50 per minute) and accompanied by symptoms (fainting, dizziness, and others);
- sinus bradycardia caused by medications necessary for the patient, for example, with atrial fibrillation or coronary artery disease;
- AV block of the second or third degree without symptoms, but accompanied by pauses of more than 3 seconds or a decrease in heart rate below 40 per minute;
- complete AV block without symptoms due to atrial fibrillation with pauses of 3–5 seconds;
- Second or third degree AV block in combination with neuromuscular diseases such as myotonic dystrophy, Kearns-Sayer syndrome, Erb's dystrophy (muscular dystrophy of the limbs) and peroneal muscular atrophy;
- Second or third degree AV block during exercise in the absence of myocardial ischemia;
- recurrent fainting caused by stimulation of the carotid sinus in the neck, occurring spontaneously and accompanied by pauses of more than 3 seconds.
If symptoms are present, the criteria for pacemaker installation are “softened.” The main diagnostic study to identify indications for cardiac stimulation is daily ECG monitoring (Holter).
How do pacemakers work?
An artificial pacemaker is an electronic device that delivers impulses that cause the heart to beat at a normal rhythm. Most often, pacemakers are used for bradyarrhythmias, which are described above. The decision to use such a device and the choice of its type depend on many factors:
- main cause and type of arrhythmia;
- temporary or permanent nature of rhythm disturbances;
- the presence or absence of the symptoms described above;
- required stimulation frequency;
- concomitant or underlying heart diseases.
Therefore, before installing the pacemaker, the patient is carefully examined. It is mandatory to conduct an ECG, 24-hour ECG monitoring, echocardiography, and in many cases transesophageal electrophysiological studies, as well as consultation with a cardiac surgeon. Such operations are usually performed in medical institutions of regional, regional or federal significance.
The pacemaker consists of the following main elements:
- a thin metal case that contains a power source, as well as a miniature processor in which the operating characteristics of the device are specified;
- flexible wires running from the body into the chambers of the heart (usually the right atrium and right ventricle, but there may be variations).
Each pacemaker has “feedback”, that is, it not only generates impulses, but also reads the natural contractions of the heart, adjusting its work to them.
Pacemaker on an ECG, or description of an ECG with a pacemaker.
So, dear friends. The following information is intended for medical workers: cardiologists, functional diagnostics specialists. And we will talk about the features of assessing and describing the ECG of a person with a pacemaker. The information is posted for educational purposes, because very often specialized centers receive calls and questions from doctors from hospitals and clinics who have difficulty interpreting the ECG of a person with a pacemaker.
What to evaluate when analyzing the ECG of a person with a pacemaker.
- Everything is the same as in a person without a pacemaker (when it is possible to evaluate this): sinus rhythm or not, whether there are ischemic changes or not, heart rate, the presence of extrasystoles (atrial or ventricular), the presence of tachycardia and its type.
- Are there artifacts (stimuli) from the pacemaker. If so, is there any capture (that is, is there a QRS complex or P wave after the stimuli). Based on this information, we can conclude whether the pacemaker is single-chamber or double-chamber. If the pacemaker is single-chamber, then the electrode can be located in the atrium or ventricle. It is also possible to determine disturbances in the functioning of the pacemaker, such as hypersensing, hyposensing, lack of capture (which may be a result of an increase in the stimulation threshold, or dislocation of the electrode).
Now let's go through all the stages of ECG assessment for a pacemaker in order.
What is the rhythm: sinus or not?
Let's understand what the options are and when is it important? Firstly, if there is a pacemaker, this does not mean that it is constantly and continuously working. So, during the intervals when the pacemaker is not working, we can evaluate sinus rhythm or not. For example, the illustration below shows normal sinus rhythm when P waves are present. Another option is atrial fibrillation or atrial flutter - when instead of P waves we see either fibrillation waves or atrial flutter waves. In addition, there may be a pacemaker rhythm with atrial pacing, ventricular pacing, or both atrial and ventricular pacing. In these cases, we will see pacemaker spikes before the P waves or before the QRS complexes, respectively. The illustration below shows an ECG with an example of dual-chamber cardiac stimulation.
Types of pacemaker
To maintain normal heart contractions, different types of pacemakers and their modes of operation have been developed. All modern pacemakers monitor the internal activity of the heart and stimulate it only when the heart rate decreases below the programmed rate. This programmed rate is called the base pacing rate.
Most modern pacemakers have the ability to respond to the degree of human physical activity. At the same time, they speed up work, for example, during walking or exercise. This achieves a physiological increase in heart rate, necessary for the normal supply of blood to tissues. This type of stimulation is called frequency-adapted.
Also, pacemakers are one-, two-, or three-chamber:
- single-chamber stimulators have a single wire attached to the right atrium or ventricle;
- two-chamber have two wires attached to both of these chambers of the heart; this makes it possible to generate contractions of both the atria and ventricles, simulating the normal functioning of the conduction system of the heart;
- in three-chamber ones, one wire goes to the right atrium, one to the right ventricle and one more to the left ventricle; They are usually installed in patients with severe heart failure, synchronize the work of the ventricles and increase its efficiency.
In addition to permanent ECS, there are also temporary ones. They are intended for short-term use in life-threatening conditions or before the installation of a permanent pacemaker, as well as in cases where the rhythm disturbance may quickly disappear (for example, with a drug overdose). The temporary pacemaker pulse generator is not sewn under the skin, but is located outside the patient’s body. This procedure is carried out only in a hospital, and the patient’s condition is constantly monitored by doctors.
Permanent pacing is recommended for chronic or recurrent arrhythmias, most often for bradyarrhythmias accompanied by clinical manifestations. Some types of pacemakers (cardioverter-defibrillators), on the contrary, are used to prevent ventricular tachycardia and ventricular fibrillation.
About pacemakers
30.03.2011 11574
Types of cardiac stimulation. Coding of pacemaker type in hospital extracts. Checking the operation of the pacemaker at the prehospital stage. Principles of therapy for patients with ECS. Pacemaker syndrome.
Types of cardiac stimulation. Coding of pacemaker type in hospital extracts. Checking the operation of the pacemaker at the prehospital stage. Principles of therapy for patients with ECS. Pacemaker syndrome.
Electrocardiostimulation modes. The international three-letter code nomenclature developed by the Intersociety Commission on Heart Disease (ICHD) is used to designate the pacemaker mode and pacemaker types. The first letter indicates the chamber of the heart that is being paced (A-atrium, V-ventricle, D-dual); the second letter indicates the chamber of the heart from which the control signal is perceived (A-atrium, V-ventricle, D-dual, O-not perceived); the third letter indicates the way the pacemaker reacts to the perceived signal (I-inhibited, prohibited; T-triggered, repeating; D-dual, O-lack of ability to perceive signals and respond to them) (Table 1). Suppression of stimulation when sensing the electrical activity of the heart (Inhibited) corresponds to stimulation on demand (demand). Table 1. ICHD pacing mode code. Paced chamber Detected chamber Response method Characteristic V, A, DOO Fixed rate asynchronous pacing AAI Atrial pacing inhibited by P wave detection VVI Ventricular pacing inhibited by wave detection RVVT R-repetitive ventricular pacing VAT Ventricular pacing synchronized to the wave PVDD Ventricular pacing synchronized with the P wave and inhibited by the RDVI wave Sequential stimulation of the atria and ventricles, prohibited by the RDDI wave Sequential stimulation of the atria, prohibited by the P and R waves, and ventricles, prohibited by the RDDD waves The same + synchronization of ventricular stimulation with the P waves Single-chamber pacemakers use one electrode, placed or right atrium, or right ventricle. A dual-chamber pacemaker senses electrical activity or stimulates both the atria and ventricles. Most dual-chamber pacemakers require two leads, with one placed in the right atrium and the other in the right ventricle. Frequency-adaptive pacemakers can be either single-chamber or dual-chamber. A special feature of these devices is the presence of a special sensor (or several sensors) to determine the required heart rate. Thus, such an pacemaker can increase or decrease the frequency of its operation depending on changes in the physiological needs of the body.
With the development of more sophisticated pacing systems, the ICHD code was expanded to a five-letter code in 1979. Subsequently, the creation of new models of pacemakers led to the transformation of the five-letter ICHD code into a five-letter code for implantable systems of electrical influence on the heart rhythm - pacemakers, cardioverters and defibrillators in accordance with the recommendations of the British Pacing and Electrophysiology Group (BREG) and the North American Society of Pacing and Electrophysiology (NASPE) (Table 2). The code was called NASPE/BREG (NBG).
In Russia, a combined coding is traditionally used: for stimulation modes that do not have frequency adaptation, the three-letter code ICHD is used, and for modes with frequency adaptation, ? first 4 letters of the NASPE/BREG (NBG) code. Table 2. NASPE/BREG (NBG) pacing mode code. Designation location in the three- to five-digit code I Paced chamber(s) of the heart II Detected chamber(s) of the heart III Response option to the detection signal IV Programmability V Antiarrhythmic function(s) O — none O — none O - none O - none O - none A - atrium A - atrium T - triggered P - simple programmable P - pacing (antitachyarrhythmia) V - ventricle V - ventricle I - inhibited M - multiprogrammable S - shock D - dual (A + V ) D — dual (A+V) D — dual (T+I) C — communicating D — dual (P+S) S — single (A or V) S — single (A or V) R — rate modulation Designations :
A - Atrium / atrium C - Communicating / two-way communication D - Dual / double (I,II - A+V; III - I+T; V - P+S) I - Inhibited / suppressed M - Multiprogrammable / multiprogrammable O - None / no P - (IV) Simple Programmable / programmable (simple programming) P - (V) Pacing (antitachyarrhythmia) / antitachyarrhythmic stimulation R - Rate modulation / frequency regulation S - (I,II) Single / single S - (V) Shock / defibrillation (cardioversion) T - Triggered / switched V - Ventricle / ventricle
Note: Headings I - III are used exclusively to indicate antibradycardic functions. The need for one or another type of stimulation is determined by specialists from arrhythmia and pacing surgery centers. Many questions related to the functioning of the pacemaker can be answered immediately by a sufficiently long ECG recording. The stability of rhythm imposition and biocontrol (the perception of spontaneous biopotentials by the pacemaker), and the stimulation mode are assessed. It is mandatory to conduct a magnetic test (application of a magnet over the area of the implanted pacemaker). Magnetic test. If pacing is persistently suppressed by spontaneous cardiac activity, pacemaker function can be assessed using a magnetic test. When a magnet is placed on the skin over the pacemaker, the stimulator's ability to sense incoming signals is temporarily disabled. This leads to the device being switched to asynchronous stimulation mode. The stimulation frequency during a magnetic test is usually higher than the base one (in domestic pacemakers, the nominal stimulation frequency during a magnetic test is 100 imp/min).
Pacing impulses generated outside the refractory period after spontaneous QRS complexes cause new ventricular depolarization. Correct placement of the magnet can sometimes be difficult in obese patients or in cases of deep pacemaker implantation. The magnet must be powerful enough. The location of the magnet is refined during long-term ECG recording until stable asynchronous stimulation with a fixed frequency is established. The nominal stimulation frequency depends on the stimulator model. A decrease in stimulation frequency to the value specified in the pacemaker passport serves as an indicator of pacemaker replacement. For frequency-adaptive stimulators, the device's transition from the adaptive stimulation mode to the on-demand mode also serves as a low battery indicator.
A sudden deterioration in the patient's condition requires checking the serviceability of the cardiac pacing system (both pacemaker and electrodes). To assess the adequacy of the ES system during programming, a 12-lead ECG recording will be required, which raises doubts about the correct operation of the ES.
. . In some patients (with transient AV block, sick sinus syndrome), there may be no signs of cardiac ES on the ECG at rest. In all these patients, their own heart rhythm should be recorded at a frequency higher than the basic ES frequency.
The pacemaker should be replaced when the frequency decreases to the value specified in the device passport. But even if the heart rate has dropped to a certain level indicating that the battery is low, the pacemaker will continue to work for several months. Features of therapy for patients with implanted pacemakers. Therapy for patients with implantable pacemakers does not differ from the generally accepted one: indications for the choice of medications, as well as criteria for their effectiveness, remain common. It should be taken into account that the use of certain medications may contribute to a temporary increase in the threshold of ES and, accordingly, in some patients, a violation of the effectiveness of ES (exit-block). Potassium, β-blockers, calcium channel blockers, quinidine, ajmaline, isuprel, isadrin have this effect. A decrease in the ES threshold (also temporary) was noted with the administration of prednisolone, norepinephrine, and ephedrine.
It should be taken into account that ES has both antiarrhythmic (with brady-dependent extrasystoles, tachycardias) and proarrhythmogenic effects. The more physiological the system, the less its proarrhythmogenic effect. Isolated ventricular ES (VVI) has the maximum proarrhythmogenic effect. In patients with isolated atrial ES (AAI), AAPs are prescribed according to general principles, and in case of dual-chamber and ventricular ES, they can be prescribed regardless of their effect on AV conduction.
It should be noted that with the deterioration of myocardial contractility, the band of permissible heart rate at rest narrows (60-120), and with severe circulatory failure, any deviation from the optimal heart rate (approximately the corresponding rhythm frequency in patients with an intact cardiac conduction system in similar clinical situation).
Heart rate can serve as an indicator of pacemaker performance. An arrhythmologist may recommend checking your pulse rate at varying intervals. In this case, it will indicate the boundaries of possible changes in heart rate in different situations during normal operation of the pacemaker. The adequacy of the selected stimulation parameters is evidenced by a decrease in signs of circulatory failure, a decrease in the frequency and severity of angina attacks, a decrease in daily intake of nitroglycerin, restoration of adequate diuresis, a decrease in central venous pressure, normalization of blood pressure and cardiac index. If the pulse rate is less or more than the specified values, and also if you doubt the correct operation of the pacemaker, you should consult an arrhythmologist. EX syndrome. Pacemaker syndrome consists of a range of clinical features, not all of which are necessarily present in every individual patient. Signs of mild KS include pulsation of the neck veins, fatigue, weakness, malaise, tiredness, palpitations, dizziness, cough, feeling of fear, heaviness in the chest. With moderate severity of the syndrome, jaw pain, chest pain, dizziness, hypotension, shortness of breath during exercise, changes in thinking, and headache appear. In severe cases, with presyncope and syncope, patients with KS may feel even worse during VVI stimulation than before pacemaker implantation.
The development of pacemaker syndrome is associated with a number of mechanisms, the leading of which is the preservation of ventriculoatrial conduction with retrograde excitation of the atria during electrical stimulation, and in some cases, with the appearance of echo complexes. In some patients with intact VA conduction without clinically significant MC at rest, during exercise against the background of stimulation in the VVIR mode, hemodynamics may not improve, since the beneficial effect of increased heart rate is offset by the adverse hemodynamic effects of constant retrograde conduction. Implantation of a VVIR type pacemaker does not guarantee the patient against the development of KS at rest and/or during physical activity. MC may occur during exercise in patients with VVIR pacing in the following situations: (1) continuous pacing while maintaining VA conduction during exercise; (2) patients with chronotropic insufficiency may remain in normal sinus rhythm at rest, and during exercise, an inappropriate increase in the frequency of sinus rhythm leads to the inclusion of ventricular pacing (at a frequency exceeding sinus rhythm) with retrograde conduction; (3) VA conduction is dynamic, and in some patients with blocked VA conduction at rest, it may improve and recover with exercise under the influence of catecholamines or other factors. Conversely, MC observed at rest may disappear during exercise if increased ventricular pacing blocks VA conduction.
MC with atrial or dual-chamber pacing is observed in the following situations: long programmed AV delay (AR or PR interval > 200 ms), pacemaker-mediated (infinite circular) tachycardia, pacing in DDI or DDIR modes (variable PV intervals), sinus bradycardia less than baseline frequency during stimulation in VDD mode, switching stimulation mode (from DDDR to VVIR), rhythm smoothing function for dual-chamber stimulation.
Installation process
The pacemaker is implanted into the soft tissue under the skin in the area under the collarbone. Its wires are inserted into a large vein and advanced to the heart, where they are secured with prongs, hooks or small screws. Less commonly, the generator is placed under the skin of the abdomen.
The procedure is performed under local anesthesia, sedatives are used, and the patient is conscious. After the pacemaker is installed, its position is monitored using radiography. The duration of the procedure depends on the type of device and does not exceed 1 hour. The wound is sutured with absorbable sutures, so no stitches need to be removed. An immobilizing device is applied to the arm for 24 hours.
There are leadless pacemakers (without wires) that are inserted through the femoral vein and attached directly to the heart.
After implantation, the pacemaker is programmed - the base frequency, the maximum frequency at which the pacemaker can operate, and changes in the pacing rate during physical activity are determined. All this data is reflected in the device passport.
Recovery period and possible complications
The recovery period is short, and the procedure itself can be performed even on an outpatient basis. Anesthesia is usually not required. Before discharge, a control x-ray is taken to ensure that there are no complications and that the stimulator is positioned correctly. Antibiotics are often prescribed for the first 10 days to prevent infection. To avoid displacement of the body, it is recommended to limit active movements of the arms in the first month.
Complications after surgery are very rare. It could be:
- pneumothorax or hemothorax (accidental injury to the pleura, as a result of which air/blood enters the pleural cavity and compresses the lung);
- damage to the subclavian artery;
- perforation of the pericardium and heart, which can cause tamponade (bleeding with compression of the myocardium);
- bleeding from a postoperative wound, hematoma (accumulation of blood under the skin) or inflammation of a vein - thrombophlebitis;
- soft tissue infection;
- air embolism – entry of air into the venous system;
- temporary disturbance of heart rhythm;
- allergic reaction to medications.
All these complications can be quickly eliminated with timely diagnosis. The risk of early postoperative complications is higher in people over 75 years of age.
Follow-up
Patients with an implanted pacemaker require regular monitoring. The condition of the pacemaker is checked during a personal visit to a cardiac surgeon. In modern conditions, it is possible to transmit data about its operation remotely, using a telephone or a special web system. However, this method has a significant drawback - it does not allow you to immediately reprogram the device if it is not operating efficiently.
Frequency of observation:
- with a single-chamber stimulator: twice during the first six months, then annually or when signs of pacemaker malfunction appear;
- with a two-chamber stimulator: twice during the first six months, then once every 6 months or if the device malfunctions.
The pulse generator is usually powered by lithium batteries, which last 5 to 8 years before needing to be replaced. When the battery power begins to deplete, it happens slowly and predictably, allowing you to notice this process in time. Replacing the generator is a simple procedure. A skin incision is made over the old one, the previous housing is removed, and a new one is installed in its place, the wires are connected to the new generator.
The pacemaker can operate indefinitely, unless there are problems with its output wires. For example, they may lose contact with the heart muscle or break off. In such cases, a new wire is installed, but the old one is not removed, since it is quite difficult to remove it. Complete removal of the system is necessary if infection develops. Risk factors for developing infectious complications (endocarditis):
- operation to replace the pulse generator;
- implantation of a 2-3 chamber device;
- age over 60 years;
- renal failure;
- taking anticoagulants.
In these cases, preventive antibiotic therapy is intensified.
Problems during ECS
The stimulation amplitude may be too low. Increase the current. The leads may not make contact with the myocardium, the leads may short-circuit, the pacemaker leads or contacts may be faulty, or the pacemaker battery may be depleted. Swap the electrodes. Replace the pacemaker cord and pacemaker itself.
Create a skin electrode (see Inactive Skin Electrode) and attempt to establish a rhythm using it as the passive electrode and each epicardial electrode in turn as the active electrode. The amplitude of the ECG waveform on the monitor may not be sufficient to register spikes. Select a different monitoring lead or zoom in.
The electrodes can contact the myocardial area with a high excitation threshold. In addition, the contact of the electrodes with the myocardium may be disrupted. In AF, atrial pacing will be ineffective. Increase stimulation amplitude to maximum, try changing electrodes, or create a passive skin electrode. Try a different stimulation mode.
In patients requiring epicardial pacing for more than 24 hours, it is important to regularly check the pacing threshold. This is done by gradually reducing the amplitude of the stimuli until the stimulation capture disappears. The minimum amplitude before the capture disappears is called the stimulation threshold. The threshold increases due to edema and trauma of the myocardium, hematoma at the site of contact of the electrode with the heart. In pacemaker-dependent patients, consider temporary transvenous pacemaker or permanent pacemaker placement.
If the pacemaker senses the f waves and f waves of AF and atrial flutter or T waves, this will suppress demand pacing when operating in VVI mode. Increase the sensitivity threshold or change the stimulation mode.
Electrical stimulation can lead to a catastrophic decrease in cardiac output if it competes with and disrupts the patient's own rhythm. Switch from asynchronous mode to on-demand pacing mode, or turn off the pacemaker completely.
What the patient needs to know
A person with an implanted pacemaker must specify the date of the next visit during each visit to the doctor and adhere to it. He is recommended to carry a copy of the ECS passport with him, and also to know which device is installed. To do this, you need to remember three letters indicating the operating mode of the EX:
- AAI – atrial stimulation;
- VVI – ventricular stimulation;
- DDD – stimulation of both atria and ventricles.
If this designation is also followed by the letter R, this means that the pacemaker works with frequency adaptation, that is, the frequency of the pulses changes depending on the patient’s physical activity. During an ECG or 24-hour monitoring, medical personnel should first of all be informed of these letters.
Modern pacemakers are little sensitive to external electromagnetic influences. Patients are advised to know the following:
- household appliances, mobile phones, computers, Wi-Fi do not affect the operation of the pacemaker;
- electromagnetic anti-theft systems or security systems can theoretically affect the operation of the ECS, so it is better not to be near them for a long time; You can walk through the “frame” in stores;
- metal detectors at airports are unlikely to affect the operation of the stimulator, but they will react to it; therefore, such patients usually undergo a manual search (it is important to have the device passport or a copy of it with you);
- in workplaces where there is welding equipment or powerful electric generators, disturbances in the operation of the ECS may occur; The patient is advised to stay at least a meter away from such devices and immediately leave the facility if dizziness or other unpleasant symptoms occur.
Medical procedures that are not recommended for people with an installed pacemaker:
- magnetic resonance imaging, except in cases where a modern “MRI-safe” stimulator is installed; although even with the usual type of ECS, MRI can be performed, but only in those institutions where the patient can be provided with the necessary assistance and the device can be reprogrammed again;
- a method of treating pain is transcutaneous electrical stimulation of a nerve or muscle;
- physiotherapy – diathermy;
- shock wave lithotripsy to remove gallstones or kidney stones;
- radiation for a malignant tumor;
- any operation where electrocoagulation is used to stop bleeding, including dental treatment.
35% of people with installed ECS develop anxiety disorders, neuroses and even depression. Therefore, they need the support of relatives, doctors, and medical psychologists. These patients do not have any restrictions in diet or daily activity. When the pacemaker is functioning normally, they lead a normal life.
Take the TEST: Do you have bradycardia?
Share results via
Facebook Twitter Google+ Pinterest LinkedIn VK
Similar articles:
Types of pacemakers - Electrocardiogram with artificial pacemaker
AND STIMULATION MODES
https://www.youtube.com/watch?v=ytcopyrightru
EX VVI is a pacemaker inhibited by the R wave (Fig. 21). Otherwise, this type of ECS is called “demand” and “standby”, which means “working on demand” and “spare”. Just like the V00 pacemaker, its operation requires implantation of one electrode into the ventricle, but in addition to stimulating, it also plays a detector role.
Rice. 20. Options for rhythm competition.
a — monitor recording, lead Vj. Frequent ventricular extra asystole with asynchronous stimulation. The extrasystolic complex is located between two imposed - b - competition of rhythms associated with the restoration of sinus rhythm and the presence of ventricular extrasystoles.
Rice. 21. Functioning of the pacemaker in VVI mode (diagram). An asterisk in a circle indicates perception of the control signal and stimulation.
EX type WI has two operating modes: native and fixed.
In the absence of its own heart contractions, the pacemaker generates impulses at the frequency set for it. When spontaneous ventricular depolarization occurs outside the refractory period of the stimulator, the device perceives it and the generation of a stimulating impulse is blocked (Fig. 22). The next impulse can occur only after a set interval, which determines the frequency of stimulation.
In other words, if within a certain time the spontaneous wave R is not perceived by the stimulator, then a stimulating impulse will be generated; if this situation persists for a long time, the pacemaker will begin to work constantly at its inherent base frequency. This operating mode is called native (Fig. 23). Explaining the principle of operation of the pacemaker, we do not specifically say that “the stimulator begins to generate impulses when the natural heart rate is lower than the stimulation frequency,” although such an explanation is often found in the literature.
Rice. 23. Functioning of the pacemaker in its own operating mode. Alternation of spontaneous complexes (atrial flutter with different conduction coefficients) with imposed ones. Stimulation frequency 73 pulses/min (stimulation interval 848 ms). The interval between spontaneous contractions is less than 848 ms.
This is not entirely correct, since the frequency of natural contractions may be lower, but individual contractions falling within the above-mentioned interval will be perceived by the ECS and block the application of the stimulating impulse (Fig. 24).
In type VVI pacemakers, the following intervals are distinguished: automatic, pop-up and asynchronous stimulation interval.
Automatic interval, or stimulation interval: the interval between two consecutive imposed complexes.
Pop-up pacing interval: the interval between a spontaneous (sinus or extrasystolic) beat and the subsequent imposed beat.
In most VVI pacemakers, the pop-up pacing interval corresponds to the automatic interval.
However, in practice, when analyzing an ECG, the stimulation interval that pops up may turn out to be slightly larger than the automatic one (Fig. 25). This is due to the fact that it is very difficult to determine from the configuration of the QRS complex the moment when the amplitude of the R wave will be sufficient for the sensory mechanism to perceive the pacemaker [E1-Sherif N. et al., 1980]. Since the counting is made from the beginning or top of the QRS complex, there may be a discrepancy in determining the true value of the automatic interval.
The upper curve is an ECG in standard lead II; the lower curve is transesophageal recording of atrial potentials (t/p). Stimulation frequency 70 imp/min (stimulation interval 850 ms), sinus rhythm frequency 60 per 1 min (P-P interval 1000 ms).
Automatic interval 920 ms. The jump interval, measured from the beginning of the QRS complex after the first and third extrasystoles, is 960 ms, after the second extrasystoles - 920 ms.
Rice. 26. Changing the value of the pop-up interval when introducing a hysteresis value.
a—original ECG (hysteresis value not entered). Automatic and pop-up intervals are equal. b - a hysteresis value of 375 ms is entered. The pop-up interval increased to 1255 ms (880-t375).
In recent years, programmable ECS have been produced here and abroad, in particular based on the hysteresis value. Hysteresis, when applied to stimulation, means the difference between frequency. at which the pacemaker begins to generate impulses, and the frequency with which this stimulation occurs. As we mentioned above, in most cases the automatic and pop-up pacing intervals are equal.
If hysteresis is introduced into the ECS, then it will make the difference between the pop-up and automatic intervals. In other words, in the case of positive hysteresis, the pop-up stimulation interval will be greater than the automatic one (Fig. 26, a, b). The significance of hysteresis is that it allows maximally maintaining a more favorable hemodynamically sinus rhythm (Fig. 27).
Recognizing hysteresis is very important to avoid misdiagnosis of a problem in the stimulation system. In the USSR, EKS-500 devices are produced, which have a hysteresis value. To simplify the analysis of the ECG in table. Figure 3 shows the correspondence between the frequency of the start of stimulation and the frequency with which this stimulation is carried out, at different values of hysteresis.
Asynchronous pacing interval: This is an automatic interval that is recorded when the pacemaker enters a fixed mode under the influence of magnetic fields. The device is switched to a fixed operating mode when an external magnet is brought to the site of pacemaker implantation.
Table 3. Change in stimulation frequency when introducing hysteresis
True stimulation frequency at different hysteresis values
In this case, the asynchronous stimulation interval may become shorter than the automatic one, which leads to an increase in the stimulation frequency. This change in stimulation frequency when a magnet is applied is called a magnetic test. The frequency of stimulation during a magnetic test depends on the pacemaker model. For example, with EX-222, the stimulation frequency does not change much, and this difference can only be detected using special monitoring equipment.
Rice. 28. Transfer of EKS-500 to fixed mode. When a magnet is applied (arrow), the device operates in a fixed stimulation mode with a frequency of 100 pulses/min.
a — the initial sinus rhythm; b — the initial imposed rhythm.
The stimulation frequency of the magnetic test depends on the state of the power supply, and therefore this test is used to determine the energy state of the power supply. During the operation of the pacemaker, the frequency of stimulation when performing a magnetic test decreases (Fig. 31). A decrease in the frequency of generated impulses below the critical value specified in the passport indicates an threatening depletion of the power source and, even with effective stimulation, requires replacement of the pacemaker.
Rice. 29. Transferring Spectrax-5985 pacemaker to fixed mode.
a — initial sinus rhythm. When a magnet is applied, the first artificially evoked complex appears 600 ms after the spontaneous one. The first three imposed complexes follow at a frequency of 100 imp/min. Subsequent pacemaker pulses are recorded with a frequency of the basic stimulation rhythm of 69 imp/min, falling into the refractory period of the ventricles, they do not cause their depolarization.
The asynchronous stimulation interval of 600 ms is recorded only twice, since the countdown starts from the sinus complex; b - the initial rhythm is imposed by the pacemaker. The base stimulation frequency is 70 pulses/min. When a magnet is applied, the first artificially evoked complex appears after 600 ms. The next three complexes follow with a frequency of 100 impulses/min, after which stimulation is again carried out with a frequency of 70 impulses/min.
In some types of pacemaker operating in VVI mode, when a magnet is applied to the pacemaker area or removed, the automatic interval increases due to the pacemaker inhibition (Fig. 32). This fact is explained by a change in the difference in electromechanical potentials between the intracardiac electrode and the ground plate.
The arrows indicate the moment of application and removal of the magnet. An increase in rhythm up to 100 imp/min is recorded only in two complexes (and not in three, as one would expect). Starting from the sixth complex, the pacemaker functions in the R-inhibited mode, as evidenced by the absence of a stimulus when a ventricular extrasystole occurs.
Rice. 31. Magnetic test when the power source is depleted (Siemens-Elema-668 ECS).
https://www.youtube.com/watch?v=ytdevru
Arrows indicate the moment of applying and removing the magnet. When applying a magnet, the stimulation frequency increases only to 89 pulses/min (the initial frequency during the magnetic test is 100 pulses/min). This result indicates depletion of the power source, but not the need to replace the pacemaker, since reimplantation is indicated when the stimulation frequency is reduced to 85 pulses/min.
This picture occurs only in those pacemakers whose magnetically controlled contact circuit is connected to a sensor circuit; in models where these circuits are isolated, the application or removal of a magnet does not lead to pauses.
Each type VVI pacemaker has a refractory period, i.e., a time during which it does not perceive any signals. The pacemaker remains refractory to intracardiac potentials not only after each imposed, but also after each “caught” spontaneous complex.
Stimulation increases to 90 pulses/min after a pause, the value of which can vary.
a - pause duration 108 ms; b - pause duration 156 ms.
As a rule, the refractory period in various ECS models ranges from 200 to 500 ms. A spontaneous ventricular complex that occurs in the interval corresponding to the refractory period will not be detected by the device, and the next imposed complex will appear after a specified automatic interval. The device perceives only those complexes in which the amplitude of the intracardiac potential is at least 2-2.5 mV.