Causes of right atrial hypertrophy
The disease occurs against the background of pathological processes due to which the filling of the right atrium (RA) with blood becomes excessive. To ensure normal blood flow and to protect the chamber from rupture, the myocardium builds up layers, as a result of which the frequency and strength of its contractions increase. GPP can develop with a strong emotional outburst, due to deformed ribs, obesity or addiction to alcohol. The reasons for thickening of the PP are:
- pulmonary pathologies (obstructive pulmonary disease, bronchitis);
- heart defects (congenital);
- bicuspid valve stenosis;
- pulmonary artery embolism;
- tricuspid valve insufficiency;
- enlargement of the right ventricle.
Hypertrophy is classified by type. They are distinguished depending on the factors that affect the functioning of the heart:
- Working HPP develops against the background of constant overexertion or intense loads of a healthy person.
- Replacement is the result of the heart’s adaptation to normal conditions in various pathological conditions of the main organ.
- Regenerative HLP develops after myocardial infarction, when a scar is formed, and the functions of the lost zone are taken over by cardiomyocytes (muscle cells of the heart) that have grown around.
Clinical symptoms
The main signs of RA overload are pain in the chest area and respiratory problems. Symptoms are often preceded by pneumonia, pulmonary artery embolism, bronchial asthma and other pathologies. After treatment of the underlying disease, signs of hypertrophy may completely disappear. The following clinical symptoms will help to recognize GPP:
- swelling;
- shortness of breath, worsening breathing, cough;
- pale skin, cyanosis;
- heart rhythm pathology;
- tingling discomfort in the heart area;
- severe fatigue with moderate exertion.
Signs of hypertrophy on the ECG
The rhythm of the heart muscle creates an electric field that has a positive and negative pole. The difference in these potentials is recorded on the ECG in the allocated electrodes, which are pre-attached to the patient’s chest and limbs. The electrocardiograph records altered signals received over a certain period of time, and then displays them on paper in the form of a graph.
The atrial complex of the electrocardiogram with RA hypertrophy is called P pulmonale on the ECG. As a rule, it is observed in patients with chronic lung pathologies, tricuspid stenosis, and repeated thromboembolism. The main signs of right atrium overload on the ECG:
- pulmonary (pulmonary) P wave;
- increase in the right atrial part of P;
- pointed and high P in leads 2 and 3, aVF.
Electrical axis shift to the right
In the normal position of the axis, the angle between the vector of electrodynamic activity and the horizontal coordinate is 30-70°. For thin people and asthenics, the norm is an angle of 90°. For dense and short people, the normal value is from 0 to 30°. By studying the data of right atrium hypertrophy on the ECG, the diagnostician can see a sharp deviation of the axis to the right up to 120°. This patient's condition is not a pathology, but may indicate that the right ventricle and/or right atrium is abnormally enlarged, which signals diseases such as:
- ischemia;
- pulmonary stenosis;
- mitral valve stenosis;
- atrial fibrillation;
- atrial septal defect and others.
"Pulmonary heart"
Detected hypertrophy of the right atrium on the ECG is a sign of a pathology such as cor pulmonale. This is the name given in cardiology to a set of symptoms that occur with high pressure in the pulmonary circulation. The reasons for the development of cor pulmonale are various lesions of the respiratory system. About 80% of diseases of the lungs and bronchi provoke this disease. Signs of cor pulmonale on the ECG:
- vertical location of the electrical axis or deviation to the right;
- presence of P pulmonale (signs of overload of the right heart);
- pronounced S wave or a decrease in its amplitude;
- RV6/SV62 ratio;
- registration of the S wave in all chest leads from V1 to V6;
- decreased ST segment and negative T wave in leads V1, V2;
- presence of QRV1 (with the exception of focal myocardial damage).
Is the condition dangerous if a load on the right atrium is detected on the ECG?
If the right atrium (RA) is overfilled with blood or pressure overload, myocardial hypertrophy subsequently occurs. Signs of this condition are shortness of breath, dizziness, fainting, and irregular contractions. Treatment requires an impact on the disease that caused overstrain of the heart muscle (lung disease, valvular heart disease).
Causes of increased load on the right atrium of the myocardium
In order for the load on the cardiac muscle of the RA to increase when blood is ejected into the ventricle, the pressure in it must increase due to an obstruction (tricuspid valve stenosis) or the blood volume must increase.
This situation occurs with reverse reflux (valvular insufficiency), high pressure in the right ventricle (heart defects).
Diseases leading to overload, and subsequently hypertrophy of the PP, may differ in adulthood and childhood.
In adults
The most common pathologies accompanied by a large load on the right atrium:
- chronic bronchitis (obstructive);
- bronchial asthma;bronchial asthma
- emphysema of pulmonary tissue;
- hardening of the lungs (pneumosclerosis);
- multiple cysts;
- bronchiectasis;
- tuberculosis infection;
- sarcoidosis;
- pneumonia;
- occupational lung diseases;
- chest injuries and deformities, operations;
- obesity;
- pulmonary hypertension (primary and secondary forms);
- autoimmune diseases;
- thrombosis, embolism and atherosclerosis of pulmonary vessels;
- tumors in the chest.
All these processes disrupt the ejection of blood from the right ventricle into the lungs, which leads to its overstrain and subsequent hypertrophy, and the RA is affected for the second time.
Also causes of pathological changes include rheumatism, endocarditis involving the tricuspid valve.
Excessive load on the RA occurs with tricuspid stenosis, insufficiency and combined acquired defect of this valve.
We recommend reading the article on myocardial hypertrophy. From it you will learn about the mechanism of development and types of myocardial hypertrophy, as well as about the diagnosis and treatment of the disease.
And here is more information about left atrial hypertrophy.
The child has
The first place among the factors of PP overload is taken by heart defects, in which circulatory disorders occur in the pulmonary circulation:
Right atrium overload
The addition of hypertrophy of the right parts of the heart occurs with decompensation of circulatory failure of the left ventricular type. This is due to the increase in congestion in the lungs, which over time complicates the work of the right atrium.
Signs and symptoms of stress
If overstrain of the PP occurs against the background of acute inflammatory processes or exacerbation of bronchial asthma, bronchitis, then there are no characteristic symptoms, or the overload is manifested by an excessive increase in shortness of breath during physical activity. If the underlying diseases are heart defects, then the signs are:
- increasing weakness and fatigue;
- cardiopalmus;
- pain and heaviness in the liver area;
- indigestion;
- cyanotic or icteric skin tone;
- swelling in the legs;
- accumulation of fluid in the abdominal cavity;
- pulsation of neck veins.
Is it dangerous
Increased load on the right atrium does not have negative consequences if it is possible to eliminate its cause - through medical or surgical treatment of the underlying disease. With unoperated heart defects, heart failure and congestive processes in the internal organs develop quite early, many of which have irreversible consequences.
In the later stages, fluid accumulates in the abdominal cavity (ascites), chest (hydrothorax), pericardial sac (hydropericardium), liver cirrhosis and severe rhythm disturbances occur.
ECG readings of load on the right atrium
Short-term manifestations of PP overload can be detected by recording an ECG at the time of an asthma attack, thromboembolism, or extensive pneumonia:
- pulmonary (pulmonary) P wave;
- increase in the first (right atrial part) P;
- high and pointed P in leads 2 and 3, aVF.
These symptoms disappear after the patient’s condition normalizes, or their severity decreases significantly. With hypertrophy, the P waves are high-amplitude, pointed, and have a normal duration.
ECG changes with increasing pulmonary hypertension and chronic overstrain of the RA are usually combined with symptoms of right ventricular hypertrophy . If an overload is detected, chest X-ray, cardiac ultrasound with Doppler ultrasound, CT and MRI are indicated to find the cause of the abnormalities.
How to reduce indicators
To correct circulatory disorders due to heart defects, surgical treatment with plastic surgery or valve replacement is required.
For lung diseases, anti-inflammatory therapy is needed, the use of drugs that dilate the bronchi and improve the function of external respiration (Teopek, Eufillin).
For the treatment of pulmonary hypertension, vasodilators (Corinfar retard, Diacordin), diuretics (Lasix, Veroshpiron), and oxygen inhalations are prescribed.
A decrease in the manifestations of heart failure occurs with the use of ACE inhibitors (Diroton, Enap), beta blockers (Corvitol, Concor), angiotensin antagonists (Lorista, Diovan).
We recommend reading the article about heart dilatation. From it you will learn about the types of heart dilatation, symptoms, as well as methods for diagnosing and treating the disease.
And here is more information about right ventricular hypertrophy.
High load on the right atrium occurs in diseases of the lungs and heart. It can be temporary or permanent, leading to myocardial hypertrophy. Often appears secondary to overstrain of the right ventricle.
Clinical symptoms (shortness of breath, cyanosis, edema, liver enlargement) occur when heart failure occurs. To identify it, it is enough to conduct an ECG, but to find the cause, additional examination is required. Treatment depends on the underlying pathological condition.
Watch the video about atrial hypertrophy on the ECG:
Source: https://CardioBook.ru/nagruzka-na-pravoe-predserdie-na-ekg/
Treatment
The goal of all therapeutic methods is to normalize the functioning of the heart muscle. After right atrial hypertrophy is detected on the ECG, the patient is individually prescribed drug therapy, physical activity is limited to moderate, and an anti-cholesterol diet is recommended. The basis of treatment is the following groups of drugs:
- Antianginal agents. Reduce preload on the myocardium, improve blood supply in the subendocardial parts of the heart muscle (Nitroglycerin, Mildronate).
- Antihypoxants. Medicines that improve the utilization of oxygen circulating in the body, increasing resistance to oxygen deficiency (hypoxia). Prescribed for GPP to prevent myocardial remodeling (Actovegin, Preducal).
- Cardioprotective drugs. They help strengthen the heart muscle, reduce the concentration of toxins in the body, accelerate cell regeneration, and prevent the formation of blood clots. Cardioprotectors are divided into several groups: statins (Acorta, Crestor), beta blockers (Atenolol, Anaprilin, Metoprolol, Bisoprolol), antiplatelet agents (aspirin C, Curantil).
- Antihypertensive drugs. They reduce the rate of myocardial hypertrophy and also help delay the development of heart failure in the chronic stage. Antihypertensive drugs are divided into several subgroups: ACE inhibitors (Enalapril, Quadropril, Perindopril), angiotensin 2 receptor antagonists (Angiakand, Lozap).
Signs of LVH on ECG
LVH or left ventricular hypertrophy is an increase in the volume of the structural unit of the heart (left ventricle) due to increased functional loads that are incompatible with capabilities. Hypertrophy on the ECG is not the cause of the disease, but its symptom. If the ventricle extends beyond its anatomical size, then the problem of myocardial overload already exists.
Severe signs of LVH on the ECG are determined by a cardiologist; in real life, the patient experiences symptoms of heart disease, which determine dilatation (pathological enlargement of the heart chamber). The main ones include:
- instability of heart rhythm (arrhythmia);
- symptom of short-term cardiac arrest (extrasystole);
- persistently elevated blood pressure;
- extracellular hyperhydration of the extremities (edema due to fluid retention);
- lack of oxygen, impaired frequency and depth of breathing (shortness of breath);
- pain in the heart area, chest area;
- short-term loss of consciousness (fainting).
If symptoms appear on a regular basis, this condition requires consultation with a doctor and an electrocardiographic examination. A hypertrophied ventricle loses its ability to contract fully. Impaired functionality is displayed in detail on the cardiogram.
Causes
The causes of left ventricular hypertrophy (LVH) have a fairly wide range and depend on the following factors:
- patient's age;
- heredity;
- Lifestyle;
- presence of bad habits;
- state of the vascular system.
At a young age, the main cause of left ventricular myocardial hypertrophy is regular physical activity (sports, hard work), while for older people the main cause is atherosclerotic damage to the vascular system. In all cases, there is an increase in the thickness of the myocardium (heart muscle) designed to compensate for the increased need for oxygen (during sports) or with difficult hemodynamics (with atherosclerosis of the arteries).
Unlike the left, right ventricular hypertrophy (RVH) develops due to disruption of the valve system:
- congenital heart disease (usually found in children);
- mitral valve stenosis;
- lung diseases.
Important! In most cases, at an early stage, diagnosing RVH is difficult, since the size of the right ventricle is 3 times smaller than the left. Therefore, the diagnosis of RVH is made at stages when the size of the right ventricle exceeds the size of the left.
In the figure: on the left is a healthy heart, on the right is hypertrophy of the left ventricular myocardium (an increase in the thickness of the myocardium and a decrease in the ventricular cavity can be seen)
Basic ECG concepts for the left ventricle
The rhythmic work of the heart muscle creates an electric field with electrical potentials having a negative or positive pole. The difference between these potentials is recorded in leads - electrodes attached to the patient’s limbs and chest (indicated “V” on the graph). The electrocardiograph records changes in signals that arrive over a certain time range and displays them as a graph on paper.
A fixed time period is reflected on the horizontal line of the graph. Vertical angles (teeth) indicate the depth and frequency of impulse changes. Teeth with a positive value are displayed upward from the time line, with a negative value - downward. Each tooth and lead are responsible for recording the functionality of a particular cardiac section.
Indicators of the left ventricle are: waves T, S, R, segment S-T, leads – I (first), II (second), III (third), AVL, V5, V6.
- The T-wave is an indicator of the recovery stage of the muscle tissue of the ventricles of the heart between contractions of the middle muscular layer of the heart (myocardium);
- Q, R, S - these teeth show agitation of the cardiac ventricles (excited state);
- ST,QRST, TP are segments indicating the horizontal distance between adjacent teeth. Segment + tooth = interval;
- Leads I and II (standard) – display the anterior and posterior walls of the heart;
- III standard lead – fixes I and II according to a set of indicators;
- V5 – lateral wall of the left ventricle in front;
- AVL – lateral cardiac wall anterior to the left;
- V6 – left ventricle.
The electrocardiogram evaluates the frequency, height, degree of jaggedness and location of the teeth relative to the horizontal in the leads. The indicators are compared with the norms of cardiac activity, changes and deviations are analyzed.
Electrocardiographic signs of hypertrophy (overload) of the left atrium (P-mitrale)
Enlargement of the left atrium is a consequence of mitral regurgitation with congenital, acquired (due to rheumatic carditis or infective endocarditis), relative mitral regurgitation or mitral stenosis. Characterized by:
- an increase in the total duration (width) of the P wave by more than 0.10 s;
- widened double-humped P wave in leads I, aVL, V5-V6;
- the presence of a pronounced negative phase of the P wave in lead V1 (more than 0.04 s in duration and more than 1 mm in depth).
Electrocardiographic signs of hypertrophy (overload) of the right atrium (R-pulmonale).
It develops in pulmonary pathology, as well as in chronic pulmonary heart disease and congenital heart defects. Characterized by:
- a high-amplitude P wave with a pointed apex in leads II, III, aVF, this sign is required in lead V1 or V2;
- with a P wave duration not exceeding 0.10 s.
ECG signs of left ventricular hypertrophy:
Causes: aortic stenosis, aortic insufficiency, coarctation of the aorta, hypertension, coronary artery disease, cardiomyopathies. LV hypertrophy is typical for athletes.
Since the ECG normally reflects the activity of only the left ventricle, electrocardiographic signs of left ventricular overload emphasize (exaggerate) the norm. Where the R wave is normally high (in lead V4, the position of which coincides with the left border of the heart), it becomes even higher; where the S wave is normally deep (in lead V2), it becomes even deeper.
ECG signs of LVH are considered in leads: I, II, aVL, V5,6.
· Sokolov-Lyon index: the sum of the amplitudes of the R wave in lead V5 or V6 (where it is larger) and S in lead V1 or V2 (where it is larger) is more than 35 mm, more than 45 mm in young people.
· Cornell voltage index, sex-specific: Ravl + Sv3 > 28 mm for men, > 20 mm for women
· R in V6 is greater than R in V5, greater than R in V4 and greater than 25 mm.
· Shift of the electrical axis to the left.
· RI› 15 mm, RavL≥11 mm.
The transition zone shifts to the right precordial leads
ECG signs of right ventricular hypertrophy:
Causes: in children with congenital heart disease, in adults with mitral valve stenosis, in lung diseases (chronic cor pulmonale). In some cases (PE or acute decompensation in a patient with bronchopulmonary disease), acute dilatation of the right ventricle can occur without wall hypertrophy, which is an extremely rare phenomenon in the left ventricle.
Electrocardiographic signs of overload (hypertrophy) of the right ventricle appear when its mass increases by 2-3 times.
General ECG signs of right ventricular hypertrophy are considered in leads III, II, aVF V1,2.
· high R wave in VI-V2 (R`>7mm), when RV1>=SV1. A deep S wave appears in leads V5, V6.
· with pronounced hypertrophy of the right ventricle, the ECG in V1, V2 has the form qR, with pronounced hypertrophy - rSR`, or rSR`, or rR`, with moderate - RS, Rs.
Deviation of the electrical axis of the heart to the right
· decrease in the RS-T segment and inversion of the T wave is observed in III, II, aVF, V1-V2.
The transition zone shifts to the left chest leads
There may be an S-type ECG in the precordial leads, in which a pronounced S wave is observed from V1 to V6. The ECG looks like S, RS, or Rs. The S-type is combined with the electrical axis of the spine SI-SII-SIII; it occurs more often in patients with pulmonary emphysema, cor pulmonale, mitral stenosis, and pulmonary hypertension.
ECG diagnostics of intraventricular blockades
Intraventricular blockade: this is a slowdown or complete cessation of the conduction of excitation along one, two or three branches of the His bundle.
ECG signs of right bundle branch block:
1 – widening of the QRS complex >0.12 sec.
2.QRS V1-V2 and III -avf type – rSR' or rsR'.
3. In the same leads, ST is shifted downward with a convexity upward, Z.T is negative.
4. In the left chest leads (V5-V6); I and avl – wide, jagged z.S, ST – slightly raised and z.T +.
With incomplete blockade of PNPG, conduction along the right leg is preserved, but somewhat slowed down. ECG signs –QRS -0.09 sec.-0.11 sec. QRS V1 type rSr'-rSR', and in I hole. and in V6 – widened Z.S
ECG signs of blockade of the left leg of the bundle of His: (2 branches of the left leg);
1. widening of the QRS complex >0.12 sec.
2. deviation of the electrical axis of the heart to the left (non-permanent sign).
3. in leads I, avl, V5-V6 – a high, widened, M-shaped wave R, z.q, V5-V6 – absent. In the same leads, ST is shifted downward with a convexity upward, Z.T is negative
4. in leads III, avf, V1, V2 – a widened and deepened complex of type QS or rS.
ECG diagnosis of rhythm and conduction disorders.
The term “heart rhythm disturbances” refers to arrhythmias and heart blocks. Arrhythmias are disturbances in the frequency, regularity and consistency of heartbeats. Disturbances in the conduction of excitation cause the development of heart blocks.
All arrhythmias are the result of changes in the basic functions of the heart: automaticity, excitability and conductivity.
They develop when the formation of the cell action potential is disrupted and the speed of its conduction changes as a result of changes in potassium, sodium and calcium channels.
Impaired activity of potassium, sodium and calcium channels depends on sympathetic activity, the level of acetylcholine, muscarinic-like M2 receptors, and ATP.
Didn't find what you were looking for? Use the search:
Source: https://studopedia.ru/20_4575_elektrokardiograficheskie-priznaki-gipertrofii-peregruzki-levogo-predserdiya-r-mitrale.html
Left ventricular hypertrophy on the cardiogram
When compared with the norms, the signs of left ventricular hypertrophy on the ECG will have the following differences.
| Prong/segment | Standard indicators | Deviations in hypertrophy |
| R (standard leads) | acute-angled, high in leads II and AVF | high in I and AVL, serrated |
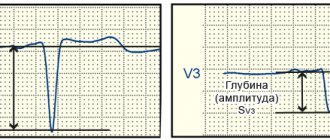
| R(chest leads) | in V3, V4 – high | in V5, V6 – high |
| T left (I, AVL, V5, V6) | always positive | negative, consists of two parts |
| S-wave | in leads II and V3 equal in height to R | lowest in I, AVL, V5, V6, and deepest in III, AVF, V1, V2 |
| ST (segment) in the left leads | always in line with the horizontal line | sloping lower in relation to the horizontal line in V5, V6, located opposite to the left in V1, V2 |
Right atrium enlargement
Clinical conditions
- heart defects with hyperfunction of the right side (tricuspid valve defects, atrial septal defect, Fallot group defects)
- restrictive cardiomyopathy
- right atrium tumor
- congestive heart failure
- diseases of the bronchopulmonary system
Video 1. Echocardiography. Enlarged atria in atrial fibrillation
ECG diagnosis of right atrium enlargement
Limb leads
- deviation of the P wave vector down, forward and to the right
- deviation of the electrical axis of the P wave to the right: PIII>PII>PI
- P wave duration is within normal limits (see Fig. 5)
ECG criteria for right atrium enlargement
- in leads II, III, aVF rapid rise and increase in the amplitude of the P wave ≥2.5 mm (at least in one of the leads)
- II, III, aVF, V1-V2 - the pointed P wave can be biphasic, with a predominance of the first phase
- in lead V1, an increase in the amplitude of the positive phase of the P wave ≥1.5 mm
- in lead I, the P wave is often negative or smoothed
- aVR P wave deep, negative, pointed
Enlargement of the right atrium is often combined with right ventricular hypertrophy, so analysis of the QRS waves on the electrocardiogram is necessary.
Rice. 5. ECG diagnosis of right atrium enlargement
Pseudo P-pulmonale
With an increase in the left atrium, the P wave vector deviates posteriorly and downward more than to the left.
A negative P wave is recorded in leads V1-V2.
There is a high P wave in leads II, aVF.
Reasons for increasing P wave amplitude
- severe hypokalemia
- hypersympathicotonia
- low position of the diaphragm with an asthenic constitution
If in standard leads the P wave becomes high and elongated, then this is right atrial hypertrophy or P-pulmonale. If the P wave has become widened and humped, most often these changes are noticeable in standard leads I and II, this indicates hypertrophy of the left atrium or P-mitrale.
Rice. 6. ECG picture of enlargement of both atria
Learn more about changing tine values
Left ventricular hypertrophy is visually determined by the height and width of the R wave in leads V5 V6 (increased wave parameters), compared to leads V1, V2. Transformation of the T-wave in leads V5, V6 indicates left-sided pathology in the case of:
- negative tooth value;
- doublings (two parts of one tooth);
- the first half “looks” down, and the second half looks up.
A slight displacement of the S-T segment up or down relative to the horizontal line is a sign of thickening of the walls of the left ventricle. Significant displacement is an indicator of myocardial infarction or ischemic heart disease (coronary heart disease).
The S-wave in the presence of a hypertraffiated ventricle changes as follows:
- in leads: III, AVF, V1, V2 – increased depth of the tooth;
- in leads: AVL, V5, V6, I – weakly expressed;
- jaggedness is observed.
Deviations from the norm of the parameters of the Q, R, S waves are called the voltage of the cardiogram. If the teeth are located below normal by more than 0.5 mV, a low-voltage potential will be recorded on the cardiogram. Voltage changes always indicate the presence of cardiac pathology.
Deviation of the electrical axis of the heart to the left as a sign of left ventricular hypertrophy
If the left ventricle is enlarged, that is, has hypertrophy, then it can change the location of the heart in the chest. Its borders move to the left, giving the heart a more horizontal position. When determining the electrical axis of the heart, they find out exactly how impulses propagate throughout the heart. The electrical axis of the heart coincides with the anatomical axis. With left ventricular hypertrophy, the following appears:
- high R wave in lead 1 and lead AVL;
- deep S wave in lead 3 and lead AVF;
- displacement of the transition zone from chest leads V3 to V4 or V2;
- R waves are widened.
Causes of hypertrophy
Left ventricular hypertrophy detected during an ECG means the presence of excessive load on the heart and myocardial diseases:
- narrowing of the aortic lumen in the valve area (aortic stenosis). Due to the transformation of the valve leaflets, blood flow is disrupted, and the heart is forced to work in emergency mode;
- change in the volume of the left ventricular wall towards thickening (hypertrophic cardiomyopathy). The thickness of the walls impedes blood circulation, which increases the load on the myocardium;
- persistently high blood pressure (hypertension).
Deformation can occur due to reasons that depend directly on the patient himself. First of all, these are the following factors: eating habits leading to obesity, irrational physical activity. LVH is common to many athletes, since excessive load on the heart during training provokes an increase in the volume and mass of the organ, systematic psycho-emotional overload (state of stress), and an unhealthy lifestyle (smoking, alcohol, lack of fresh air, unhealthy foods).
Large R wave in precordial leads V5, V6
When examining an electrocardiogram, the doctor will immediately notice if the R waves are significantly higher and much wider in precordial leads V5, V6 than in other leads. This clearly indicates left ventricular hypertrophy.
Negative, biphasic or double-humped T waves
Typically, the T wave changes in precordial leads V5, V6, which also indicates the presence of left ventricular hypertrophy:
- directed downwards (negative);
- may consist of two halves pointing upward (double-humped);
- one half can be facing up and the other down, that is, a two-phase tooth;
- the tooth faces upward especially in the chest leads V1, V2
Dangerous consequences
The left ventricle is responsible for oxygen saturation and movement of arterial blood into the aorta and further through all small vessels to nourish the organs. As the volume increases, the blood presses on the walls, the connective tissue displaces the muscle tissue, and the ventricle ceases to cope with its functional duties.
What such changes threaten is determined by the following diagnoses:
- coronary heart disease - a violation of the blood supply to the heart due to thickening of the walls of the gastric chamber;
- myocardial infarction – death (necrosis) of part of the heart muscle;
- ventricular extrasystole (arrhythmia) – failure of the heart rhythm;
- atrioventricular or ventricular block - cessation of the passage of electrical impulses between the atria and ventricles, leading to hemodynamics;
- heart failure is a low contractility of the heart muscle, often leading to death.
Timely detection of LVH will help prevent serious complications. The most informative in terms of diagnosing pathology is the electrocardiographic examination method.
Development mechanism
Enlargement of the right atrium is the result of an increase in pressure in the pulmonary artery, other vessels of the small circle, as well as overload of the chamber with blood as a result of the influence of one or another factor.
Detection plays a diagnostic role, because hypertrophy has several types.
An increase in pressure in the pulmonary and other arteries develops as a result of hemodynamic disturbances, vascular defects, and hypertension.
The normal outflow of blood from the right atrium weakens, the remains of liquid connective tissue press on the walls, provoking adaptive mechanisms.
The load on the atrium increases, the organ grows. Builds muscle mass to improve contractility and prevent tissue tearing.
Another mechanism is associated with dysfunction of the tricuspid valve. It covers the passage between the right atrium and the ventricle.
Malfunction leads to incomplete ejection of blood, increased pressure in the chambers and their hypertrophy for the same reasons.
Based on the origin of the process, the mechanism of formation, three forms are distinguished:
- Cardiosclerotic variety. It occurs as a result of inflammation, heart attack and other phenomena of the same kind (coronary insufficiency, coronary artery disease). The affected area becomes scarred, cells are roughly arranged around the area, and tissue grows artificially. Hence the increase in volume, disruption of normal activity.
- Compensatory type. It develops as a result of the influence of a negative factor: an increase in pressure in the pulmonary artery, pulmonary vessels, and other processes.
- Working variety. It develops in patients who are professionally involved in sports. Less likely to engage in similar physical activity as part of work (loaders, others).
Determining the mechanism plays an important role in diagnosis. This is the basis for prescribing competent therapy.
Prevention of LVH
The main preventive measures include:
- elimination of bad habits (alcohol and nicotine addiction);
- a healthy diet (eliminating foods containing low-density lipoproteins, the so-called bad cholesterol, while increasing the intake of high-density lipoproteins, the “good cholesterol”);
- body weight control (obesity always negatively affects heart function);
- balanced physical activity appropriate for age;
- regular exposure to fresh air (active oxygen stimulates proper cardiac activity).
These recommendations will help not only avoid heart disease, but also improve your overall quality of life.
Diagnosis and treatment of right atrial hypertrophy
Enlargement of any of the chambers of the heart with thickening of the heart muscle leads to heart failure. Right atrium hypertrophy occurs when blood flow through the pulmonary artery is disrupted and is manifested by dilation of the cavities of the right side of the heart. Symptoms indicate an underlying disease, and cardiac changes are detected by electrocardiography or sonography. With the right approach to treating the disease that caused hypertrophic changes, heart function will improve and the size of the atrium will return to normal.
Causal factors for enlargement of the right chambers of the heart
Changes in wall thickness and dilatation of the internal cavity of the right atrium appear with increasing load: venous blood collects in the right parts of the heart, which enters the pulmonary circulation through the pulmonary artery and is saturated with oxygen in the lungs.
The main causes of myocardial hypertrophy on the right arise when there is difficulty in the flow of blood into the right ventricle and pulmonary arterial trunk in the following cases:
- partial blockage of a vessel (pulmonary embolism);
- pulmonary heart;
- chronic diseases of the bronchopulmonary system;
- congenital heart anomalies (atrial septal defect, transposition of great vessels);
- acquired defects with significant narrowing of the opening between the atrium and the ventricle (valvular insufficiency or stenosis);
- right ventricular myocardial hypertrophy;
- myocardial infarction.
Factors contributing to pulmonary hypertension and the formation of hypertrophied cardiac chambers include:
- obesity;
- alcohol abuse;
- smoking;
- hard physical labor;
- chest injuries;
- congenital deformities of the bone skeleton (kyphosis, scoliosis).
The main causative factor is a pronounced load on the main artery of the pulmonary circulation with the formation of pulmonary hypertension syndrome. The right side of the heart tries to push venous blood toward the lungs, resulting in one of 3 types of hypertrophic thickening of the heart muscle:
- compensatory (myofibrillar), which occurs during severe physical activity;
- replacement (with pronounced tension of the heart muscle against the background of lung diseases and cardiovascular pathology);
- regenerative, which is a consequence of recovery processes in the heart against the background of myocardial infarction.
Having found out the probable cause of heart disease, it is necessary to evaluate the symptoms and conduct all the necessary diagnostic tests.
Causes
Right atrium pressure overload is characteristic of tricuspid valve stenosis. This is an acquired heart defect, in which the area of the opening between the atrium and the ventricle decreases. Tricuspid valve stenosis may be due to endocarditis.
With another acquired heart defect, tricuspid valve insufficiency, the right atrium experiences volume overload. In this condition, blood from the right ventricle, when it contracts, flows not only into the pulmonary artery, but also back into the right atrium, causing it to work under overload.
The right atrium is enlarged in some congenital heart defects. For example, with a significant atrial septal defect, blood from the left atrium enters not only the left ventricle, but also through the defect into the right atrium, causing its overload. Congenital heart defects accompanied by the development of HPP in children - Ebstein's anomaly, tetralogy of Fallot, transposition of the great vessels and others. Right atrium overload can occur quickly and manifest primarily on the electrocardiogram. This condition can occur during an attack of bronchial asthma, pneumonia, myocardial infarction, or pulmonary embolism. Subsequently, with recovery, the signs of HPP gradually disappear.
Sometimes electrocardiographic signs of HPP appear when the heart rate increases, for example, against the background of hyperthyroidism. In thin people, electrocardiographic signs of HPP may be normal.
Symptoms of the disease
Typical signs of right atrial hypertrophy are absent. All manifestations are caused by the underlying disease and symptoms of developing heart failure. It is important to promptly pay attention to the following symptoms:
- discomfort and pain in the left side of the chest;
- a periodic feeling of interruptions in heart rhythm;
- shortness of breath when moving and at rest;
- night cough;
- breathing problems, especially in a horizontal position;
- change in vascular tone towards hypertension;
- swelling of the limbs;
- pronounced pallor;
- fast fatiguability.
As heart failure progresses with impaired blood flow in the pulmonary circle, typical manifestations of cor pulmonale occur.
It is advisable to identify cardiac pathology earlier than signs of serious complications appear.
Clinic for right atrium overload
ECG for right atrial hypertrophy
As a rule, patients’ complaints appear in the later stages, when pronounced hypertrophy or expansion of the atrium occurs, or during an acute attack of stress on the right side of the heart. For a long time, a person may not even know that one of the chambers of his heart is experiencing overload. In the initial stages it is asymptomatic and diagnosed only by ECG.
With severe exertion, complaints may include shortness of breath during physical activity or at rest, dry cough, hemoptysis, and general weakness. If the diagnosis is not carried out on time, the patient does not receive treatment, not only the right, but also the left parts of the heart suffer, and circulatory failure develops in a large circle.
Signs of which include heaviness and pain in the right hypochondrium, ascites, nausea, vomiting, swelling of the feet, ankles, and legs. Heart failure develops. You should be aware that overload can occur acutely and suddenly. And also suddenly pass without a trace. This condition can develop during an asthmatic attack, pneumonia, when, after relief of symptoms or cure, the clinical manifestations go away, the cardiogram returns to normal, and the patient’s condition returns to normal.
Diagnostic principles
Based on the patient’s complaints, the doctor will make a presumptive diagnosis, which can be confirmed by the following studies:
- ECG;
- duplex ultrasound scanning;
- Dopplerometry of blood vessels;
- tomography.
Hypertrophy of the right atrium on the ECG is manifested by the following signs:
- increase in height and sharpening of the P wave;
- change in P wave width;
- increase in S wave amplitude.
Echocardiographic signs are sufficiently reliable and informative to prove the presence of hypertrophy. An ultrasound scan will help assess the size of the heart, the amount of dilatation and the degree of thickening of the wall of the right atrium, which normally should not exceed 12 mm. Doppler measurements will reveal hemodynamic disorders, and with tomography, the doctor will be able to examine in detail a three-dimensional image of the atria and ventricles.
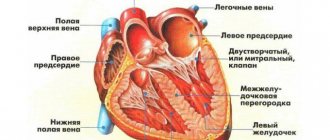
Structure and functions of the heart
Every person knows what the heart is. However, in order to get a complete understanding of how cardiac activity is reflected in the electrocardiogram, it is important to have information about its anatomical structure and functions.
The main structural elements of the heart are 4 chambers (cavities):
- atria (left and right);
- ventricles (left and right).
Since the systemic circulation begins in the left ventricle and, accordingly, ends in the right atrium, the muscular wall of the ventricle has a significant thickness necessary to provide sufficient pressure to push out the entire volume of blood located in the cavity. Unlike the left, the right ventricle has a significantly smaller wall thickness, since the resistance to blood flow in the small circle is several times less and, accordingly, there is no need to provide the same high pressure as in the large circle.
Due to the fact that blood flow must occur in one direction, regulation is carried out using 4 valves that allow or prevent the movement of blood flow:
- mitral - bicuspid valve separating the left atrium and ventricle;
- tricuspid - separates the right atrium and ventricle;
- aortic;
- pulmonary.
The structure of the human heart
Therapy tactics
To obtain the desired positive effect from complex treatment, you must follow the following doctor’s recommendations:
- complete cessation of smoking and alcohol;
- gradual loss of body weight;
- regular performance of a complex of physical therapy;
- normalization of the diet under the supervision of a nutritionist.
Effective treatment tactics require mandatory treatment of the underlying disease. If there are indications (congenital or acquired defects, thromboembolism), surgical intervention is performed. In other cases, drug treatment aimed at normalizing blood flow through the pulmonary artery, correcting diseases of the lungs and bronchi, normalizing blood pressure and preventing myocardial infarction will be optimal (you can read more about this disease in our article at the link).
Hypertrophy of the right heart is almost always a secondary change, so with timely treatment of the primary pathology, there will be no serious problems in the atrium and ventricle.
Right ventricular hypertrophy
During a cardiogram in a healthy state, the signal from the left ventricle predominates, which is considered stronger. This is due to the fact that normally the weight of the right ventricle is one third of the weight of the left, the signals from which usually predominate in electrocardiographic indicators. But the picture looks completely different when there is right ventricular hypertrophy on the ECG.
In cardiological practice, there are 3 types of RPG:
- Sharply expressed - the muscle mass of the pancreas significantly exceeds this indicator in the ventricle, from which the systemic circulation begins.
- Classic hypertrophy - the right ventricle is enlarged, but its severity is inferior to that of the left ventricle, and the process of excitation in it is longer.
- Moderate RV - there is a visual enlargement of the RV, but its mass remains less than that of the LV.
When the left side of the heart is overloaded, this can negatively affect the functioning of the entire organ, but acute overload on the right side is an even more serious symptom. The physiological capabilities of the right heart are determined by its work only with the pulmonary (pulmonary) circulation, and the loads in it are relatively small.
If a narrowing of the pulmonary artery occurs in its various sections or an additional volume of blood is discharged from an adjacent section, then the pressure of the pulmonary circulation increases significantly and the right ventricle of the heart is significantly loaded. He is not adapted to increased loads, so he has to increase his size and increase his mass. This may be the starting point for the appearance of prostate cancer.
S-type ECG in standard chest leads clearly indicates RVH
Possible complications
Dilation of the right atrium cavity with thickening of the myocardial wall in the absence of adequate therapy can cause the following dangerous complications:
- chronic heart failure;
- progressive cor pulmonale;
- cardiac arrhythmia and conduction disturbances such as blockade;
- complete pulmonary embolism;
- myocardial infarction;
- sudden cardiac death.
Combination therapy and long-term medical observation are the best option for treatment tactics: with the right approach to treatment, you can prevent deadly complications , reduce the size of the heart and significantly improve the quality of life of a sick person.