General information
Myocardial hypertrophy is understood as a clear increase in myocardial mass, which develops against the background of hypertension , pathology of the heart valve apparatus and other diseases that are accompanied by prolonged overload of a certain part of the heart.
Myocardial hypertrophy is more typical for the left ventricle, but hypertrophy of the right ventricle and atria may occur. As hypertrophy develops, the myocardium of a certain part of the heart thickens, which leads to a change in its shape, volume and size. Today, hypertrophy is considered not so much as a specific damage to the heart in arterial hypertension, but as a risk factor for the development of heart failure and sudden death.
An increase in myocardial mass is recorded in 16% of men and 19% of women under the age of 70 years. In the age group over 70 years old, these figures correspond to 33 and 49%.
What diseases does it develop in?
LV hypertrophy may not be an independent disease, but a symptom of a number of disorders, which include:
Arterial hypertension .
The left ventricle can hypertrophy with both moderate and regular increases in blood pressure, since in this case, in order to pump blood, the heart has to pump blood at an increased rate, which is why the myocardium begins to thicken.According to statistics, approximately 90% of pathologies develop precisely for this reason.
- Heart valve defects . The list of such diseases includes aortic stenosis or insufficiency, mitral insufficiency, ventricular septal defect, and quite often LV hypertrophy is the first and only sign of disease. In addition, it occurs in diseases that are accompanied by difficulty in the flow of blood from the left ventricle into the aorta;
- Hypertrophic cardiomyopathy . A serious disease (congenital or acquired), which is characterized by thickening of the heart walls, as a result of which the exit from the left ventricle is blocked and the heart begins to work under heavy load;
- Cardiac ischemia . In IHD, LV hypertrophy is accompanied by diastolic dysfunction, that is, impaired relaxation of the heart muscle;
- Atherosclerosis of the heart valves . Most often, this disease manifests itself in old age - its main feature is a narrowing of the exit hole from the left ventricle into the aorta;
- Heavy physical activity . LV hypertrophy can occur in young people who frequently and intensively engage in sports, since due to heavy loads the mass and volume of the heart muscle increase significantly.
Pathogenesis
A healthy, not organically changed heart is characterized by normal thickness of the walls of various cavities:
- left ventricle – 9-11 mm;
- right ventricle – 4-6 mm;
- left and right atrium – 2-3 mm.
Most often, hypertrophy is observed in the left ventricle, the thickness of which can reach up to 3 cm, and the mass of the entire heart can reach several kilograms. Such changes negatively affect the functioning of the entire cardiovascular system and lead to the development of heart failure .
The load on the heart can increase for various reasons, but all of them lead to thickening of the myocardium as a compensatory response to the increasing load. At the first stages, the patient does not notice any changes, but as trophism and nutrition of cardiomyocytes weaken, the vascular bed loses the ability to cover the needs of the increased myocardial area. Due to the lack of oxygen and nutrients, the contractility of the myocardium is weakened.
Just like blood vessels, the conduction system of the heart cannot expand indefinitely following the myocardium, so arrhythmias due to disturbances in impulse conduction. The thickened myocardium gradually begins to be replaced by connective tissue, losing its pumping function. Long-term hypertrophy can lead to diffuse cardiosclerosis .
Thickening of the wall of one chamber of the heart inevitably leads to expansion of other cavities if left untreated. Elimination of the causes and properly selected therapy leads to regression of LVH.
Types of Cardiomyopathy
Pathological processes in myocardial cells are based on hereditary predisposition (idiopathic cardiopathy) or dystrophy and sclerosis. The latter are caused by myocarditis, allergies and toxic damage to heart cells, endocrine pathologies (excess catecholamines and somatotropic hormone), and immune disorders.
Normally, the thickness of the ventricular walls is 9–14 mm in different zones; with the development of cardiomyopathy, these dimensions can increase significantly. Thickening of the walls is usually not strictly symmetrical; it can be localized in various parts: in the area where blood exits into the aorta, in the septum between the ventricles, at the transition from the atrium to the left ventricle.
Left ventricular hypertrophy is divided into two types:
- Concentric. It is characterized by thickening of the walls of the left ventricle and, as a result, an increase in myocardial mass without changes in the volume of the cavity - this is due to hyperplasia of the organelles of myocardiocytes;
- Eccentric. An increase in the size of the cavity of the left ventricle, which occurs against the background of proportional compaction of its muscles, is associated with the growth of cardiomyocytes.
This pathology is caused by volume overload, which provokes an increase in the cavity, and blood pressure overload, leading to increased muscle contraction of the ventricle and thickening of the walls.
Classification
According to the location of the thickening:
- right ventricular hypertrophy;
- left ventricular hypertrophy;
- right atrial hypertrophy;
- left atrial hypertrophy.
Variants of left ventricular hypertrophy
The widespread use of echocardiography makes it possible to classify the architectonics of the left ventricle in hypertensive patients into 4 geometric models taking into account myocardial mass:
- Concentric hypertrophy of the LV myocardium - an increase in the relative wall thickness of more than 0.45 and an increase in myocardial mass. Symmetrical hypertrophy is formed as a result of thickening of the muscle itself, but without increasing the cavity. In certain cases, a decrease in the cavity of the left ventricle is observed. This type is most often found in arterial hypertension.
- Eccentric hypertrophy. The asymmetric form is characterized by simultaneous enlargement and thickening of the myocardium of the left ventricle and its cavity. This option occurs in cardiomyopathies , heart defects and ischemia .
- Concentric remodeling . Characterized by thickening of the wall, while maintaining normal myocardial mass.
- Normal LV geometry. The mass and wall thickness remain within normal values.
There are different degrees:
- Moderate left ventricular hypertrophy is a slight thickening of the heart cavity, which is a consequence of hypertension or other pathology of the cardiovascular system. Moderate hypertrophy signals an overload of the heart and an increased risk of myocardial infarction . The pathology is often asymptomatic and is a finding during electrocardiography.
- Severe left ventricular hypertrophy . Dystrophic changes are observed, and the mitral valve located close to the septum interferes with blood flow, which causes excessive muscle strain and significantly loads the left ventricle.
ECG signs of myocardial hypertrophy of the left ventricle of the heart
Left ventricular hypertrophy is a thickening of the heart muscle and an increase in its size due to hypertrophy of cardiomyocytes.
The normal thickness of the walls of the left ventricle ranges from 9 to 14 mm. Cardiomyopathy is characterized by a significantly greater thickness of the walls of the LV, and different parts of it can be unevenly enlarged. Thus, the most common places subject to morphological changes are: the place of transition of the left ventricle into the aorta, the interventricular septum, the place of transition of the left atrium into the ventricle.
Causes
The main causes of left ventricular hypertrophy:
- Hypertonic disease. With high blood pressure, a persistent and prolonged spasm of peripheral vessels is formed. This is why the left ventricle has to make more effort to push blood through than at normal blood pressure . This mechanism is associated with an increase in total peripheral vascular resistance, which leads to overload of the chambers of the heart. Gradually, the walls of the left ventricle thicken, which leads to rapid wear of the myocardium and the formation of heart failure.
- Cardiac ischemia. During ischemia, the heart muscle lacks oxygen. Cardiomyocytes cannot work efficiently without additional energy substrates, which leads to overload. As a compensatory mechanism, muscle tissue gradually thickens and LV myocardial hypertrophy develops. The cause of age-related cardiac hypertrophy is ischemic changes that develop over time.
- Myocardial dystrophy, cardiosclerosis . Connective tissue grows in the myocardium after inflammatory processes (post-myocardial cardiosclerosis) or after heart attacks (post-infarction cardiosclerosis). Myocardial dystrophy develops with anorexia , anemia, intoxication, infections, etching. After suffering a pathology, some cardiomyocytes lose their contractility, and the remaining cells take on the entire load. In this case, hypertrophy is also a compensatory mechanism.
- Dilated cardiomyopathy. With this pathology, an increase in the size of the heart cavities is observed due to overdistension. The left ventricle must do extra work to push blood out, which leads to the formation of hypertrophy.
- Heart defects. Disruption of the normal anatomy of the heart causes overload of the left ventricle due to increased intracavitary pressure in aortic stenosis , or due to volume overload, which is observed in aortic insufficiency. With other valve defects, hypertrophic cardiomyopathy of the left ventricle also develops over time.
- Congenital LV hypertrophy. Changes begin to form during intrauterine development and appear in the first months after the birth of the child. The reason lies in a genetic predisposition, which leads to disruption of the functioning of myocardial cells.
- Sports heart. In a person who has been involved in sports for a long time and professionally, thickening of the walls of the left ventricle is considered normal. Hypertrophy is due to the fact that the left ventricle takes on the main job of expelling a sufficient volume of blood for the whole body during training. Skeletal muscles require more blood flow during regular exercise, and as muscles grow, the amount of increase in blood flow in muscle tissue becomes constant. That is why the myocardium increases its mass, and the walls of the ventricle become stronger and thicker. For athletes, it is extremely important not to miss the moment when physiological hypertrophy can turn into pathological. This requires regular monitoring by sports medicine doctors.
- Idiopathic LV hypertrophy. If, as a result of a complete examination, it was not possible to identify the cause for the development of hypertrophy, then they speak of idiopathic hypertrophy, which most often implies a genetic predisposition.
Left atrial hypertrophy
From the left atrium, blood enters the ventricle through the mitral valve. With pathology of the valve apparatus, or more precisely with mitral valve stenosis, the atrium has to make more efforts to expel blood. If the valve does not close completely, then part of the blood returns to the atrium with reverse flow, which leads to an increase in the volume of atrial ejection. Similar changes occur in atherosclerosis and rheumatism . If the left ventricle is hypertrophied, then the muscle layer gradually increases in the left atrium.
Right atrial hypertrophy
Main reasons:
- sclerosis of lung tissue;
- obstructive bronchitis;
- bronchial asthma;
- ventricular septal defect;
- changes in the structure of the tricuspid valve;
- right ventricular hypertrophy;
- pulmonary emphysema;
- pathology of the pulmonary valve.
In diseases of the pulmonary system, connective tissue grows, microcirculation is disrupted and pressure in the pulmonary vessels increases. All this leads to forced hypertrophy of the right half of the heart.
Right ventricular hypertrophy, what is it?
The pathology develops after suffering diseases of the pulmonary system of an obstructive nature. Thickening of the muscle layer occurs due to increased pressure in the pulmonary circulation, which makes it difficult for the normal release of blood. Venous congestion caused by progressive heart failure can lead to right ventricular hypertrophy. Thickening of the muscle layer is also observed with congenital heart defects, with narrowing of the pulmonary valve.
Hypertrophy of the interventricular septum
Thickening of the IVS is one of the characteristic signs of hypertrophic cardiomyopathy . In pathology, thickening of the walls of both ventricles is observed with the involvement of the septum between them. This condition is only a derivative of other diseases and is characterized by a specific thickening of the myocardial walls. IVS hypertrophy is considered a fairly common pathology, observed in more than 70% of people, but most often it is completely asymptomatic.
When the interventricular septum thickens, the useful volume of the chambers of both ventricles decreases. All this leads to a decrease in the volume of blood that is released into the vascular bed when the heart contracts. The heart has to work more often to provide organs and tissues with sufficient oxygen and nutrients. Tachycardia wears out the heart muscle and leads to diseases of the cardiovascular system.
SECTION No. 7 ECG FOR HYPERTROPHY
Atrial and ventricular hypertrophy
Hypertrophy of the atria and ventricles is usually reflected on the ECG. However, in the early stages of hypertrophy of the heart, the ECG changes little, and in some cases even pronounced hypertrophy is not accompanied by noticeable electrocardiographic changes. In this regard, the value of electrocardiography in the diagnosis of atrial and ventricular hypertrophy is relative.
ECG changes during hypertrophy are associated with an increase in the mass of muscle fibers of a certain part of the heart. This is accompanied by an increase in the vector of this section, which is manifested on the ECG by an increase in the amplitude of the P waves with atrial hypertrophy and the QRS complex with ventricular hypertrophy. This increase is detected in leads whose axes are parallel to the total vector. Due to the enlargement of the teeth, the electrical axis deviates towards the hypertrophied section.
An increase in the time required to excite the hypertrophied part of the heart leads to the expansion of the corresponding waves on the ECG. An increase in the amplitude and width of the waves causes a change in the shape of the P waves and QRS complexes, characteristic of hypertrophy. At later stages of ventricular hypertrophy, a displacement of the ST segment appears discordant to the main wave of the QRS complex, as well as smoothness and then inversion of the T wave. Changes in the terminal part of the ventricular complex indicate the development of myocardial dystrophy and dilatation of the cavity of the hypertrophied ventricle.
Left atrial hypertrophy
With hypertrophy of the left atrium, the total atrial vector deviates to the left and backward. For hypertrophy of the left atrium, the most typical expansion of the P wave is more than 0.11 s, its splitting and increase in amplitude in leads I, II, aVR, aVL. In these leads, the P wave has a double-humped shape.
The height of the PII wave becomes equal to the height of the Ra wave and may even exceed it. In some cases, there is a vertical position of the atrial vector. In this case, the amplitude of the P wave in leads III and aVF exceeds that in leads I and aVL.
In the right chest leads with hypertrophy of the left atrium, a wide and deep negative phase of the P wave is noted. In leads V3-V6, an extended and double-humped P wave is detected. The described shape of the P wave in standard and chest leads is known as P - mitrale, since it is more common with mitral heart defects.
As mentioned above, the expansion and splitting of the P wave during left atrial hypertrophy is caused by a slowdown in impulse transmission along the atrial pathways.
A typical example of P-mitrale is presented on the ECG of a 48-year-old patient with a diagnosis of rheumatic heart disease, mitral valve insufficiency.
Right atrial hypertrophy
With right atrial hypertrophy, the total atrial vector deviates downward and slightly to the right. The main sign of right atrial hypertrophy is an increase in the amplitude of the P wave in leads II, III and aVF. The height of the P wave in these leads significantly exceeds the height of the PI wave. A negative P wave is often detected in lead aVL.
The P waves in leads II, III and aVF have a pointed shape, their width usually does not exceed normal. In lead aVR, the P wave is usually negative, deep, and pointed.
In the right chest leads, pointed positive P waves of increased amplitude are recorded. In some cases, with pronounced hypertrophy of the right atrium, the P waves in leads V1 and V2 may be negative.
Changes in the P wave, characteristic of hypertrophy of the right atrium, are called P-pulmonale; they are more common in diseases associated with increased pressure in the pulmonary artery system. Hypertrophy of both atria
With hypertrophy of the two atria, the ECG reveals signs characteristic of both P-pulmonale and P-mitrale. There is a significant increase in the amplitude of the P wave, its expansion and splitting in the limb leads. Both the positive and negative phases of the P wave in lead V1 are increased.
In the remaining chest leads, the amplitude and width of the P wave are also increased. This form of the P wave is known as the P cardiale. Signs of enlargement of one atrium in standard leads may be combined with signs of enlargement of the other atrium in chest leads.
The figure shows an ECG of a 35-year-old patient diagnosed with lung cancer, rheumatic mitral heart disease with predominant stenosis. The ECG shows an increase in the amplitude of the P wave in leads I and II, a negative P wave in lead III, the width of this wave exceeds 0.11 s. There is a pronounced negative phase of the P wave in lead V1, high-amplitude P waves in leads V5 and V6.
All of these signs indicate hypertrophy of the left atrium. Along with this, there are undoubted signs of right atrium hypertrophy, in particular a pronounced positive phase of the P wave in lead V1, high-amplitude, pointed P waves in leads V2 and V3, deep P waves in lead aVR. In addition, this ECG shows signs of right ventricular hypertrophy: deviation of the electrical axis of the heart to the right, shift of the transition zone to the left, ventricular complex of the qR type in lead V1. Left ventricular hypertrophy
With left ventricular hypertrophy, the total QRS vector deviates back and to the left relative to its original position. This deviation may be insignificant and often does not affect the position of the electrical axis in the frontal plane. Only when studying the ECG in dynamics can it be noted that the axis of the heart has become more horizontal (or less vertical) than before. In the initial horizontal position, the electrical axis can deviate up to -30°, and in some cases even more.
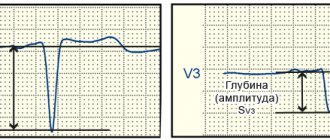
The most important diagnostic sign of left ventricular hypertrophy should be considered an increase in the amplitude of the R wave in leads V4-V6. An increase in the R wave in these leads of more than 25 mm is considered reliable. The R wave in leads V5 and V6 is often higher than in lead V4, which is also important for diagnosing this pathology.
In addition to the increase in the R wave in the left chest leads, there is an increase in the S wave in leads V1-V3, the amplitude of which can exceed 25 mm. However, an increase in the R wave in the left and the S wave in the right precordial leads is not always combined.
Often only one of these signs is detected. With left ventricular hypertrophy, the sum of the amplitudes of the R waves in lead V5 or V6 and the S waves in lead V1 exceeds 35 mm. The transition zone sometimes shifts to the right (closer to lead V1).
Severe left ventricular hypertrophy is characterized by an increase in the time of internal deviation in leads V5 and V6 by more than 0.05 s, i.e., a picture of incomplete blockade of the left leg appears.
In some cases, with left ventricular hypertrophy, there is a rather deep q wave in the leads where high R waves are recorded (usually in leads I, aVL, V5 and V6), which may be due to hypertrophy of the interventricular septum.
In this case, the width of the q wave usually does not exceed 0.03 s, and the depth is 0.25% of the amplitude of the R wave. Occasionally, in patients with left ventricular hypertrophy, a QS-type ventricular complex is observed in the right precordial leads.
With dystrophy of the left ventricular myocardium, the final part of the ventricular complex changes on the ECG. In leads where a high R wave is recorded, ST segment depression and T wave inversion are noted. These changes are usually most pronounced in the left precordial leads. In the right precordial leads, on the contrary, there is ST segment elevation above the isoelectric line along with a deep S wave. These changes progress over time.
Left ventricular hypertrophy (changes in the terminal part of the ventricular complex)
Changes in the terminal portion of the ventricular complex sometimes mimic signs of acute ischemia and myocardial damage. Correct diagnosis is helped by clinical manifestations, the absence of rapid ECG dynamics characteristic of acute coronary insufficiency, as well as other electrocardiographic signs of left ventricular hypertrophy.
Typical signs of severe left ventricular hypertrophy with dystrophic changes in the myocardium can be seen on the ECG of a 63-year-old patient diagnosed with rheumatic heart disease, aortic stenosis. There is a deviation of the electrical axis of the heart to the left up to -15°, an increase in the amplitude of the R wave in lead V5 by more than 30 mm and the amplitude of the S wave in V1 by more than 25 mm. The R wave in lead V5 is higher than in lead V4. The internal deviation time in the left precordial leads exceeds 0.05 s. There is ST segment depression and T wave inversion in leads I, aVL, V5 and V6, as well as ST segment elevation in leads V1 and V2. Signs of left atrial hypertrophy are also detected.
In rare cases, a significant enlargement of the left ventricle leads to a pronounced rotation of the heart around the longitudinal axis with the right ventricle forward and to the left. The left ventricle is located behind. With this rotation, ventricular complexes of the QS type are recorded in the right chest leads, and with a predominant S wave in the left chest leads. The appearance of such an electrocardiographic picture is also facilitated by blockade of the left anterior branch.
The figure shows an ECG of an 82-year-old patient with a diagnosis of stage III hypertension, coronary heart disease, exertional and resting angina, atherosclerotic cardiosclerosis. The ECG shows signs of atrial hypertrophy, mainly the left one, as indicated by the expansion and splitting of the P wave in leads II, III, V3–V6 and the pronounced negative phase of this wave in lead V1.
First degree atrioventricular block is noted, probably of the proximal type. In addition, there are obvious signs of left ventricular hypertrophy, in particular a significant increase in the amplitude of the S wave in leads II, III, aVF, V3 and V4 with discordant ST segment elevation, signs of slower conduction along the left branches, mainly the anterior one. The axis of the heart is sharply deviated to the left to -75°. Noteworthy is the predominance of the S wave in leads V4-V6, which is apparently associated with a significant backward rotation of the heart by the left ventricle and blockade of the left anterior branch.
Right ventricular hypertrophy (type 1)
Minor hypertrophy of the right ventricle, as a rule, is not detected on the ECG due to the physiological predominance of the potentials of the more massive left ventricle. Severe hypertrophy of the right ventricle leads to deviation of the electrical axis of the heart to the right and rotation of the heart around the longitudinal axis clockwise. Sometimes, due to pulmonary emphysema, the heart deviates with its apex posteriorly.
Deviation of the electrical axis of the heart to the right is one of the most common signs of right ventricular hypertrophy. More often you see a slight axis deviation from +95° to +110°. A deviation to the right of more than 110° more reliably indicates right ventricular enlargement.
The QRS complex in leads I and aVL is usually rS, and in leads III and aVF it is qR. When the heart turns its apex posteriorly, a deep, sometimes dominant, S wave is revealed in leads I, II and III (the so-called 5-type, or “three S syndrome”).
An important and common sign of right ventricular hypertrophy is an increase in the amplitude of the R wave in lead aVR by more than 5 mm (0.5 mV).
The most common sign of right ventricular hypertrophy in the precordial leads is a shift of the transition zone to the left. In this case, a pronounced S wave is recorded up to lead V6, and sometimes even further to the left.
An important diagnostic sign of right ventricular hypertrophy is an increase in the time of internal deviation in lead V1, which is associated with a slowdown in the activation of the hypertrophied section.
The QRS complex in lead V1 can have different shapes. Depending on this, 3 types of ECG can be distinguished for right ventricular hypertrophy. The first type is characterized by a high R wave in lead V1. This wave reflects the potentials of an enlarged right ventricle, therefore an increase in the amplitude of the R wave in lead V1 by more than 7 mm very reliably indicates hypertrophy of this section.
The ventricular complex can have the form R, RS or qR. This type of ECG is observed with severe hypertrophy of the right ventricle and occurs infrequently, mainly in patients with congenital heart defects. Some authors believe that the q wave in lead V1 indicates pronounced hypertrophy and dilatation of the right ventricle and classify this option as a separate type of ECG [Bober S. et al., 1974].
The figure shows an ECG of a 28-year-old patient diagnosed with congenital heart disease, pulmonary artery stenosis. The ECG shows signs of right ventricular hypertrophy of the first type: an increase in the R wave in lead V1 to 20 cm, a displacement of the transition zone to the left of V6, a deviation of the electrical axis of the heart to the right (A QRSII = +120°).
Right ventricular hypertrophy (type 2)
The second type of ECG is manifested by splitting of the ventricular complex in lead V1 in the form of rSRI, i.e., a picture of incomplete blockade of the right bundle branch, which is considered one of the signs of right ventricular hypertrophy. This form of the ventricular complex may be associated not only with right bundle branch block, but also with other factors. This type of ECG occurs more often than the first, mainly in patients with mitral stenosis, as well as with chronic pulmonary diseases.
Over time, incomplete blockade of the right leg in such patients can transform into complete blockade; some authors consider it as a special type of ECG for right ventricular hypertrophy. With this option, the amplitude of the R wave in lead V1 is increased.
The third type of ECG is characterized by a low-amplitude r wave and a pronounced S wave (ventricular complex type rS) in lead V1 and in subsequent precordial leads. Sometimes this reveals a pronounced S wave in leads I, II and III (S-type ECG). Sometimes with this type of ECG, the QRS complex in leads I and aVL or III and aVF has the form rSrI. This type of ECG is more common in patients with pulmonary emphysema with the development of chronic pulmonary heart disease.
The figure shows an ECG of an 83-year-old patient with a diagnosis of chronic obstructive bronchitis, pulmonary emphysema, and pneumosclerosis. There is an increase in the amplitude of the P wave with a typical change in its shape in leads II, III and aVF, inversion of the P wave in lead aVL, which indicates hypertrophy of the right atrium. Low-amplitude QRS complexes, split in leads II, III and aVF, a predominant S wave in leads V1-V5 and a sharp shift of the transition zone to the left indicate right ventricular hypertrophy.
In some patients with cor pulmonale, the ECG reveals a QS-type ventricular complex in the right precordial leads, along with clear signs of right ventricular hypertrophy in the limb leads and left precordial leads. The QS wave in leads V1-V3 requires differential diagnosis with myocardial infarction.
With hypertrophy of the right ventricle with dystrophic processes in the myocardium, changes in the final part of the ventricular complex are observed in the form of depression of the ST segment and inversion of the T wave in the leads where a high R wave is recorded (III, aVF, V1). In leads where a deep S wave is detected, there is ST segment elevation.
Right ventricular hypertrophy is indirectly indicated by signs of enlargement of the right atrium.
Hypertrophy of both ventricles
Electrocardiographic manifestations of combined hypertrophy occur only in a small part of patients with this pathology, since signs of enlargement of the right and left ventricles often cancel each other out. With a significant predominance of the potentials of one of the ventricles on the ECG, only signs of its hypertrophy are possible, and with a uniform increase in both ventricles, the ECG may not differ from normal.
However, sometimes the ECG shows signs of hypertrophy of the right and left ventricles simultaneously. Thus, signs of left ventricular hypertrophy in the precordial leads can be combined with deviation of the heart axis to the right, a high R wave in lead aVR and other manifestations of right ventricular hypertrophy in the limb leads.
Sometimes you can see the opposite combination: an indication of right ventricular hypertrophy in the precordial leads (high R wave in lead V1, shift of the transition zone to the left, etc.) and signs of left ventricular hypertrophy in the limb leads (deviation of the heart axis to the left). In the chest leads there are simultaneously signs of hypertrophy of both ventricles, for example, the rSR1 type ventricular complex in lead V1 and a high R wave in the left chest leads.
Signs of right ventricular hypertrophy in the standard and precordial leads may be combined with an increase in the amplitude of the S wave in leads V1-V3, which is an indicator of concomitant enlargement of the left ventricle.
An example of hypertrophy of both ventricles is the ECG shown in the figure of a 28-year-old patient with a diagnosis of rheumatic combined heart disease, recurrent rheumatic carditis, atrial fibrillation, and stage II circulatory failure. The ECG shows signs of right ventricular hypertrophy, in particular deviation of the electrical axis of the heart to the right, with a clockwise rotation around the longitudinal axis (QIIISI syndrome), an increase in the amplitude and width of the R wave in leads V1 and V2.
In addition, there are indications of left ventricular hypertrophy: an increase in the amplitude of the R wave in lead V5 is more than 25 mm, the R wave in leads V5 and V6 is higher than in V4. There are signs of diffuse changes in the myocardium.
Symptoms
Myocardial dysfunction in the form of hypertrophy manifests itself with characteristic symptoms. There is some difference between lesions of the right and left sides of the heart.
Left ventricular hypertrophy is characterized by:
- discomfort in the heart area;
- rhythm disturbances;
- poor tolerance to physical activity;
- shortness of breath when walking;
- fatigue, general weakness.
Right ventricular hypertrophy is characterized by:
- blueness and paleness of the skin;
- swelling;
- heavy breathing accompanied by shortness of breath, unproductive cough;
- the appearance of arrhythmia such as extrasystole , atrial flutter or atrial fibrillation.
In some cases, autonomic symptoms, poor sleep, tinnitus, and headache .
Right ventricular hypertrophy
During a cardiogram in a healthy state, the signal from the left ventricle predominates, which is considered stronger. This is due to the fact that normally the weight of the right ventricle is one third of the weight of the left, the signals from which usually predominate in electrocardiographic indicators. But the picture looks completely different when there is right ventricular hypertrophy on the ECG.
In cardiological practice, there are 3 types of RPG:
- Sharply expressed - the muscle mass of the pancreas significantly exceeds this indicator in the ventricle, from which the systemic circulation begins.
- Classic hypertrophy - the right ventricle is enlarged, but its severity is inferior to that of the left ventricle, and the process of excitation in it is longer.
- Moderate RV - there is a visual enlargement of the RV, but its mass remains less than that of the LV.
When the left side of the heart is overloaded, this can negatively affect the functioning of the entire organ, but acute overload on the right side is an even more serious symptom. The physiological capabilities of the right heart are determined by its work only with the pulmonary (pulmonary) circulation, and the loads in it are relatively small.
If a narrowing of the pulmonary artery occurs in its various sections or an additional volume of blood is discharged from an adjacent section, then the pressure of the pulmonary circulation increases significantly and the right ventricle of the heart is significantly loaded. He is not adapted to increased loads, so he has to increase his size and increase his mass. This may be the starting point for the appearance of prostate cancer.
Tests and diagnostics
At the initial visit to the doctor, complaints are collected and anamnesis is described. An objective examination includes listening to heart sounds, percussion and palpation. These methods allow you to determine the boundaries of the heart and identify its expansion. When listening to tones, the rhythm and their intensity (intensification/muffling) are assessed. Instrumental diagnostic methods are required. Indirect signs can be seen from the results of electrocardiography.
ECG. Signs of left ventricular hypertrophy on the ECG, signs of damage to other parts of the heart:
- the electrical axis is deflected to the left or located horizontally; in the V and VI chest leads, the R wave is enlarged;
- the P wave on the ECG is deformed due to changes in the atria; the “P-pulmonale” shape corresponds to the right atrium, and the “P-mitrale” shape corresponds to the left atrium;
- right ventricular hypertrophy is characterized by deviation of the electrical axis to the right, in leads V1 and V2 there is an increase in the R wave; changes in the electrical conductivity of the heart are recorded.
EchoCG. Allows you to determine the size of the heart cavities, thickening of the myocardium, calculate the pressure gradient, and calculate the mass of the myocardium during hypertrophy. Based on the results of echocardiography, it is possible to assess the pumping function of the heart and the condition of the valve apparatus.
R-graphy of the chest organs. The shape of the heart shadow is assessed; most often, the film clearly shows a hypertrophied, stretched left ventricle in the form of a characteristic protrusion at the apex.
Additionally, if indicated, coronary angiography and MSCT of the heart .
Changes in repolarization processes
Pathophysiological mechanism
There is an increase in the action potential of the hypertrophied section. As a result, a delay in repolarization processes occurs.
ECG manifestations of hypertrophy
- discordant (relative to the QRS complex) ST segment displacement. The appearance of an asymmetrical or biphasic T wave.
- prolongation of electrical ventricular systole (QT interval)
The position of the heart in the chest changes due to rotation of the heart around its longitudinal axis. This can be done in two ways:
- rotation of the left ventricle anteriorly (counterclockwise)
- rotation of the right ventricle anteriorly (clockwise)
Pathophysiological mechanisms of hypertrophy also include conduction disturbances. Which is characterized by the development of intraatrial and intraventricular blockades.
Procedures and operations
Surgical treatment is aimed at eliminating the causes that provoke the progression of LV hypertrophy. To combat ischemia, coronary angiography is performed, followed by stenting of the coronary arteries or bypass surgery (open heart surgery).
Correction of coronary blood flow allows you to normalize adequate nutrition of the heart muscle and prevent the progression of hypertrophy. In case of heart defects, prosthetics or plastic surgery of the damaged valve is performed, which also has a positive effect on the structure and function of the heart in the future. For an aneurysm of the apex of the left ventricle, excision of the muscular protrusion is performed. The operation is extremely difficult and dangerous.
Hypertrophy of the left ventricle of the heart on an ECG: what does it mean, how to diagnose the disease
Left ventricular hypertrophy is a deviation in the functioning of the heart, which can be congenital or acquired. The disease is accompanied by an increase in the volume of the heart muscle and its compaction. Left ventricular hypertrophy on the ECG is displayed by pronounced signs, but be that as it may, in order to recognize it, you need to have certain knowledge. Hypertrophy of the left ventricle of the heart on the ECG: what does this mean, let’s look at it in more detail.
A clear example of what a healthy heart looks like and a damaged one
To begin with, it is worth noting that the normal thickness of the walls of the ventricle ranges from 9-14 mm; in the case of hypertrophic lesions, this figure increases significantly. In addition, this disease is often accompanied by a violation of the uniformity of the walls; the interventricular septum is especially susceptible to changes.
Treatment with folk remedies
Traditional medicine will not help in the later stages of the disease, however, with moderate hypertrophy and minor changes, herbal therapy can alleviate the condition and reduce the risk of developing serious consequences. With treatment, it is possible to reduce shortness of breath and chest pain.
Lily of the valley in the form of gruel or tincture. To prepare the solution, pour lily of the valley with alcohol or vodka and leave in a dark place for two weeks. The tincture should be taken three times a day, 10 drops each, for two months. You can prepare a paste: pour boiling water over lily of the valley flowers and leave for 10 minutes, then drain the water and chop the softened plant. You need to take 1 tablespoon twice a day.
Herbal infusions. Horsetail, cornflower flowers, blueberries, hawthorn and motherwort improve heart function and strengthen blood vessels.
Adonis. Pour 1 teaspoon of Adonis herb into a glass of hot water and boil for 3 minutes over low heat. Leave for 20 minutes, tightly closing the lid. The resulting solution should be filtered and taken three times a day, 1 tablespoon.
Prevention
The development of myocardial hypertrophy can be prevented by changing lifestyle and treating the underlying disease that loads the myocardium. Key important recommendations:
- Refusal to drink alcoholic beverages.
- To give up smoking.
- Fighting extra pounds. With a weight loss of even 3-5 kg, it is possible to lower blood pressure and reduce the load on the left ventricle.
- Avoid salt and smoked foods, which slow down metabolism and promote fluid retention.
- Exercise regularly. Loads should be measured, daily. Try to walk more, Nordic walking is encouraged. Yoga and fitness classes have a positive effect on the functioning of the cardiovascular system.
Myocardial hypertrophy in children
In pediatric practice, congenital and acquired hypertrophy of the left ventricular myocardium is considered. Acquired forms are associated with pulmonary hypertension, various carditis and heart defects. The clinical picture can be completely contradictory. Some newborn babies are too lethargic, while others, on the contrary, are too restless and noisy. Most often, during feeding and crying, the child notices blueness of the nasolabial triangle.
Older children can talk about their complaints and describe their symptoms in detail. The most common symptoms are chest pain of various types, shortness of breath even with light exertion, pallor of the skin, fatigue and lethargy. The treatment tactics for myocardial hypertrophy in children are determined by a pediatric cardiologist together with a cardiac surgeon in the presence of organic pathology.
Causes
This deviation is more often recorded in children. Right ventricular hypertrophy found in a child is physiological in nature. During the first days outside the womb, babies experience an increase in the load on the right region of the organ. Sometimes the disease is caused by a congenital heart defect. Mitral stenosis of the organ is also a provocateur.
Typically, the disease in question in cardiology is recorded in the following categories of patients:
IT IS IMPORTANT TO KNOW! No more shortness of breath, headaches, pressure surges and other symptoms of HYPERTENSION! Find out the method our readers use to treat blood pressure. Learn the method.
- children. A pathological condition occurs in the presence of congenital defects of the organ;
- adults. In the presence of valve defects, lung damage, which are complicated by impaired functioning of the cardiovascular system.
There are different configurations of the disease in question. They depend on the severity of the pathology and the specifics of development. Cardiologists consider the following to be the leading provoking factors for right ventricular hypertrophy:
- Pulmonary hypertension. This disease provokes an increase in pressure inside the pulmonary artery. Manifested by dizziness, shortness of breath, and frequent fainting.
- Tetralogy of Fallot. This pathology is recorded in infants at birth. This disease is classified as a congenital defect of the organ. It can cause blue baby syndrome. When it occurs, the outflow of blood from the pancreas is impaired.
- Ventricular septal defect. This disease becomes a provocateur of the mixing of blood from 2 sections. There is a lack of oxygen. It is accompanied by increased work of each part of the heart muscle, including the pancreas.
- Left valve stenosis. With this lesion, the flow of blood from the pancreas to the artery is disrupted.
We mentioned above that right ventricular hypertrophy can be caused by lung lesions. These cardiologists include the following:
- chronic bronchitis;
- asthma;
- pneumonia;
- fibrosis;
- pneumosclerosis;
- emphysema.
Diet for myocardial hypertrophy
Diet for hypertension
- Efficacy: therapeutic effect after 21 days
- Timing: constantly
- Cost of products: 1600-1700 rubles. in Week
For hypertrophic thickening of the heart walls, split meals and daily intake of sufficient fluids are recommended. Avoid salt and animal fats, limit your consumption of sweets and starchy foods. Eating foods rich in omega-3 and microelements is encouraged. Weight correction through nutrition will reduce the load on the left ventricle.
Description of left ventricular hypertrophy
LVH is a disease that is accompanied by damage to the heart.
This disease is especially common in people with diagnosed hypertension. It is worth noting that the main cause of LVH is significant thickening of the wall of the left ventricle. The nature of the course of this disease depends on the type of wall thickening, since it occurs uniformly or in certain areas.
Interesting! Although cardiovascular disease is more common in older people, LVH can be called a young disease. This is due to the fact that it is very often diagnosed in young people.
In addition to hypertension, the cause of this pathology is heart disease, as well as excessive and frequent physical activity. Since this disease belongs to the category of cardiovascular diseases, it is diagnosed using an electrocardiogram.
List of sources
- Shaposhnik I.I., Bogdanov D.V., “Differential diagnosis of hypertrophic cardiomyopathy and myocardial hypertrophies of secondary origin,” Breast Cancer, issue No. 12, 2014
- Chazova I. E., Ratova L. G., Boytsov S. A., Nebieridze D. V. “Diagnostics and treatment of arterial hypertension,” Systemic hypertension No. 3, 2010
- Dmitriev V. L. “Remodeling of the left ventricular myocardium in patients with stable angina according to comparison of ventriculography and echocardiography,” “From arterial hypertension to heart failure,” Proceedings of the Russian Conference of Cardiologists, Moscow, 2001