Reasons for artificial ventricular implantation
IHFs are used for people with end-stage congestive heart failure that cannot be cured with medications. In the heart, the left ventricle does most of the work. IVC can be used to pump blood from the left, right or both ventricles. Implantation of an IVC is the best way to restore normal cardiac activity without a heart transplant.
IHS is most often used while waiting for a heart transplant. However, modern devices are quite reliable, can work for decades, and perhaps soon a heart transplant will not be a vital necessity. Depending on overall health, patients may return to normal activities after a recovery period.
Heart failure occurs when the heart is too weak to pump all the blood. Blood begins to stagnate, first in the lungs (if the left ventricle of the heart is not working properly) and then in the lower part of the body, causing swelling in the ankles.
Prevention
Left ventricular hypertrophy is only a consequence of certain pathological processes, so it is important to follow the rules of prevention in order to prevent their development:
- give up alcohol and drugs;
- quit smoking;
- Minimize the consumption of caffeine and energy drinks;
- undergo a full examination annually;
- get enough sleep (7-8 hours a day);
- fully treat emerging diseases;
- adjust your diet;
- exercise;
- try not to overload yourself physically and mentally;
- avoid stress.
The growth of the wall of the left ventricle also occurs due to other factors, among which the first place is occupied by diseases of the cardiovascular system. The development of the pathological process is accelerated by dysfunction of internal organs, bad habits, excess body weight and stress. Treatment includes medications and other means aimed at eliminating the cause and reducing the load on the heart. Advanced cases require surgical intervention.
Possible complications of implantation of an artificial heart ventricle
If you are planning to implant an artificial heart ventricle, you need to be aware of possible complications, which may include:
- Bleeding;
- Blood clots;
- Infection;
- Device failure;
- Adverse reactions to anesthesia;
- Damage to the kidneys, lungs, heart.
Factors that may increase the risk of complications:
- Severe infectious diseases;
- Diseases of vital organs other than the heart;
- Blood clotting disorders.
In addition, if you are short, implantation of an IVC is not possible, since the device is quite bulky. But the next generation of devices is being developed, which are much smaller in size.
You should discuss these risks with your doctor before surgery.
Reasons for the development of the anomaly
Enlargement of the left ventricle can occur if some unfavorable factor causes the heart to work harder than usual. This means that the heart muscle will need to make several times more contractions in order to pump blood around the body.
Model of the heart with left ventricular hypertrophy
Reasons that can provoke a significant deterioration in heart function:
Read more: Common heart diseases
- High blood pressure (hypertension) is considered the most common cause of thickening of the ventricular wall. More than one third of all patients learn about hypertrophy at the time of diagnosis of arterial hypertension.
- Aortic valve stenosis is a disease that is a narrowing of the flap of muscle tissue that separates the left ventricle from the aorta. Narrowing of the aortic valve causes the heart to contract several times more often in order to pump blood into the aorta.
- Hypertrophic cardiomyopathy is a genetic disease that occurs when the heart muscle becomes abnormally thick and stiff.
- Professional sports. Intense, long-term strength training, as well as irregular performance of endurance exercises, can lead to the fact that the heart is not able to quickly adapt and cope with the additional load. As a result, the left ventricle may swell (enlarge).
How is implantation of an artificial heart ventricle performed?
Preparation for the procedure
If you need to have an IHS installed, then most likely you will be on the waiting list for a heart transplant. You may have already been in the hospital. The doctor will prescribe many tests, for example:
- Echocardiogram - the size, shape and movement of the heart are studied using sound waves;
- X-rays – used to take pictures of structures inside the body;
- Cardiac catheterization – used to detect coronary heart disease;
- Psychological and social assessment to ensure you are ready to use the device outside the hospital.
Before the procedure:
- Try not to eat for 8 hours before the procedure;
- Stop taking aspirin or other anti-inflammatory drugs a week before surgery. You may need to stop taking blood thinning medications such as: Clopidogrel;
- Warfarin.
Anesthesia
General anesthesia is used, which blocks any pain and keeps the patient asleep during the operation.
Description of the artificial ventricle implantation procedure
This procedure involves the use of open heart surgery. The doctor will make an incision along the entire length of your breastbone. The sternum will then be divided and opened. You will be connected to a heart-lung machine (CBM). This device performs the functions of the heart and lungs during surgery. The doctor places the GIB into a pocket on the inside of the abdominal wall. Cannulas (tubes for inserting into hollow organs) will be sewn to the heart. The IVC can also be sutured to the aorta, depending on the type of device.
Immediately after the procedure
You will be in the intensive care unit (ICU) after the procedure. Sensors and life support systems are connected to the body. Medical personnel will monitor vital signs.
Causes of ventricular enlargement
Arterial hypertension
In order for the ventricle to enlarge, it must be under volume or pressure overload for a long time. Under such conditions, the heart muscle begins to adapt in order to work as efficiently and without any losses. If the LV is overloaded with pressure, the heart muscle begins to hypertrophy, that is, the wall thickens. If the chamber experiences volume overload, its walls begin to stretch to accommodate all the amount of blood that enters it.
However, at a certain time, the wall of the hypertrophied left ventricle begins to stretch, not due to the fact that it adapts to a large volume of blood. A breakdown of compensatory mechanisms occurs when energy reserves are not enough, and the heart muscle begins to experience a deficiency of oxygen and nutrients. Muscle fibers stretch and lose their former elasticity. The reasons for LV enlargement may be the following:
Hypertrophic cardiomyopathy
- arterial hypertension,
- cardiac ischemia,
- valvular heart defects (aortic valve stenosis, aortic insufficiency),
- congenital heart defects (left ventricular hypoplasia, truncus arteriosus, pulmonary atresia, ventricular septal defect, coarctation of the aorta, etc.),
- hypertrophic cardiomyopathy,
- dilated cardiomyopathy,
- obesity,
- diabetes,
- alcohol abuse,
- smoking,
- atrial fibrillation,
- chronic emotional stress.
Care after implantation of an artificial heart ventricle
Home care
When you return home, follow these steps to ensure a normal recovery:
- Stay in touch with the heart center. You may be awaiting a heart transplant;
- Increase your activity gradually as directed by your doctor. Ask him when you can return to work;
- If prescribed by your doctor, you should take blood thinners. This will prevent the formation of blood clots;
- Be sure to follow your doctor's directions. He will tell you: How to care for individual housing construction;
- In case of any life-threatening condition, you need to go to the hospital.
Ask your doctor when it is safe to shower, swim, or expose the incision site to water.
Heart training. Cardiac hypertrophy (athletic heart) Dilation (stretching) of the left ventricle.
Heart training. Cardiac hypertrophy (athletic heart) Dilation (stretching) of the left ventricle of the heart.
I have already written a short post about the so-called heart training. https://zen.yandex.ru/media/id/5d8f2057e6e8ef00b15b9dcb/o-trenirovke-serdca-5dc42c0f86c4a9c8460bece5
But I decided to add more information inspired by V.N.’s lectures. Seluyanov and his stories about the heart.
It is known that the heart has right and left ventricles and atria. When they do an ultrasound, they look specifically at the size of the left ventricle, since the right one, as a rule. Everyone has almost the same one, regardless. Are you an athlete or not an athlete?
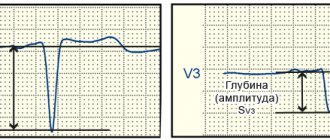
But the left ventricle may differ. To do this, look and determine the transverse size and longitudinal size in different states, namely, during systole and diastole.
Systole is the contraction of the heart muscle, and diastole is its maximum expansion. The difference between full compression and expansion shows the capacity of the heart. Let me remind you that we are talking about the left ventricle.
The thickness of the left ventricle and the thickness of the interventricular septum are also determined.
In normal people, the myocardial thickness is 0.8 cm to 1 cm, and the septal thickness is 0.5 cm.
During extreme training, or more simply put, when the heart is abused, the thickness of the myocardium can be increased to 2.5 cm. Such hearts are called sports hearts and this is very harmful and bad for human health. Such people begin to experience extrasystoles and heart rhythm disturbances. More on this below.
There are legs in the heart - the bundles of His. These are pathways that activate all the cells of the heart. So they start to block. And they are blocked for a reason, but as a result of necrosis of heart tissue. In fact, there is a blockade of the right and left bundle branches. These are a kind of micro-infarctions and the heart becomes disfigured. It is no longer possible to fix it. And if in your youth you get a sports heart due to extreme training, then this remains for the rest of your life. Why does the heart remain like this?
Let's consider this. There are atria - right and left, and between them is the sinoatrial node. This node gives an electrical impulse that spreads through the atria and then through the ventricles. And with this propagation of the impulse, each cell of the heart works in all-or-nothing mode. Simply put, the whole heart works completely. It cannot be that only one part of the heart is working. Consequently, the heart is always in excellent athletic shape. Therefore, ordinary people and many athletes do not need to train their hearts. The heart cannot lose its athletic form, it cannot become decrepit. True, if you get a heart attack or many heart attacks, then this, in fact, will be decrepitude of the heart.
If a blood clot appears, it clogs some part of the blood vessel going inside the heart, and blood and oxygen stop flowing there. Anaerobic glycolysis immediately begins to unfold, which means the appearance of lactate and hydrogen ions. Hydrogen ions accumulate in large quantities (and you need to understand that the heart consists of oxidative muscle fibers - myocardiocytes, which have many mitochondria and which need oxygen to neutralize hydrogen ions, but it just doesn’t exist, since it must come with the blood) and the tissues simply begin to die, since hydrogen ions activate lysosomes, and they begin to destroy everything inside the cell. As a result, the heart begins to die, or rather part of it. And this is called a heart attack.
If a heart attack occurs, then, naturally, the heart weakens and it must be restored. But it is not the regeneration of damaged tissue that occurs, but the hypertrophy of other, healthy tissues, and the result is a distortion in the functioning of the heart. The load on some tissues increases and decreases on others. The heart hypertrophies literally in 5-6 days. There is only one caveat. If the intact piece of the heart remains too small, then it may simply not be enough to deliver oxygen to the body, as before, and then myocardial degeneration and subsequent death results.
If the intact piece of the heart is large enough, then the heart hypertrophies and the person continues to live. But this is already an incomplete life, since another heart attack may happen, a second, a third, and the end.
Athletes can have many heart attacks. When an autopsy is performed on an athlete, they find dozens of microinfarcts in the heart.
Another thing is that myocardial infarctions in athletes do not occur from blood clots or blood clots, but from hypoxia, which occurs in the heart at a very high pulse rate.
There was such a scientist-researcher Meyerson. He dealt with heart problems and its adaptation. He carried out such an experiment. I took the rabbit. He cut him open, leaving him alive, of course, and ligated the coronary vessels (the vessels that feed the heart itself from the aorta). If they are bandaged but not completely, halfway, then the access of blood and oxygen to the muscles of the heart will be limited and cardiac hypoxia will occur. And then the heart begins to adapt to this. In a rabbit, cardiac hypertrophy doubled in five days, i.e. myocardial thickness doubled. It turns out that the heart can hypertrophy very quickly.
Accordingly, a similar thing happens with athletes and Meyerson came up with a rule called diastole defect.
Under normal conditions, the heart works freely at a pulse of 60-70 beats per minute, i.e. systole (full compression) and diastole (full expansion). At full systole, blood from the heart is squeezed into the artery, and at full diastole, blood fills the heart. This is how the left ventricle works.
But when physical activity begins and the pulse rate increases and the stroke volume stabilizes at a pulse of 150-160 beats. Stroke volume is when both systole and diastole can pump blood freely.
It should be noted that stabilization of the stroke volume of the heart at a pulse rate of 150-160 beats per minute is the average value for a human model, and not for a specific living person. Each living person can have its own stroke volume and corresponding pulse rate.
Unfortunately, you can only determine your specific stroke volume in a special laboratory.
If the pulse continues to rise, then when its frequency begins to exceed 190 beats per minute, then the stroke volume, on the contrary, begins to decrease. Thus, it turns out that working at a heart rate of 190 and above is unprofitable and unhelpful, since it does not provide an increase in power. Oxygen delivery, on the contrary, begins to decrease.
What is this connected with?
The fact is that systole works normally, but diastole does not have time to fully open (relax) the left ventricle so that a full portion of fresh blood can enter there. As a result, diastole does not open completely and the muscles of the left ventricle are constantly under tension. And if so, then blood begins to circulate poorly in the heart. A lack of oxygen occurs, anaerobic processes begin, hydrogen ions accumulate, and microinfarctions (cell necrosis) occur in places where blood flows poorly.
After numerous workouts at a pulse rate of 190 and above, many microinfarctions occur and the heart begins to falter even at rest, and extrasystoles appear. These necrotic foci begin to work (shrink) according to their own rules.
If a normal heart, upon receiving a signal from the sinoatrial node, contracts with all its cells, then the disfigured cells work according to their own rules and produce extrasystoles, disrupting the general rhythm of the heart.
If there is a lot of extrasystole, ventricular fibrillation results, i.e. blood stops pumping from him and the person dies.
So is it necessary to train the heart and, if so, how?
A normal person does not need to train the heart, but athletes, and not all and not in all sports, can train the heart.
So, athletes need to train their heart not through increasing the thickness of the myocardium (the so-called D-hypertrophy) and causing microinfarctions, but through stretching the heart (L-hypertrophy), or rather the left ventricle.
If we live quietly with a pulse of 70-80 beats, then the heart hardly stretches and the myocardiocytes of the heart become short, since there is no need to distill large volumes of blood.
Thus, such a training for stretching the heart emerges.
1. Large volumes of blood must be pumped through the heart. To do this, you need to include either a large number of muscles or large muscles or a combination of both.
2. Do exercises no higher than the anaerobic threshold level with moderate intensity.
3. The duration of the workout depends on the equipment and simulator used. For example, for a cyclist this could be the time to ride 100-200 km, for a runner to run 5 km, for a skier 10 km. But this is on the plain. And if you find a sloping but long hill, then the distance and, accordingly, the duration can be significantly reduced.
I repeat, the intensity should be low, but the load should be such that blood flows powerfully into the heart, causing it to stretch.
4. What types of competitive activities can be used.
As already written above, a bicycle, an exercise bike. You can put them in the highest gear and pedal. Under no circumstances should you acidify your muscles.
Another good way for other types of competitive activities would be circuit interval training. They only need to include the largest muscles of the body, and these are the legs (hips, buttocks) and back. You can come up with many options. Again, the main thing is to do this to the level of the anaerobic threshold and the heart will gradually stretch.
If anyone would like to support my efforts and work, you can make a donation using this link https://money.yandex.ru/to/41001612854243
Contacting a doctor after artificial ventricular implantation
After returning home, you should consult a doctor if the following symptoms appear:
- Signs of infection, including fever and chills;
- Redness, swelling, increased pain, severe bleeding or discharge from the incision sites;
- Increased pain;
- weakness on one side of the body, blurred vision, or inability to speak;
- Cold, pale or blue extremities, numbness or tenderness;
- cough, difficulty breathing, or chest pain;
- Nausea, vomiting;
- Problems with urination and bowel movements;
- Redness or swelling in the legs;
- Indication of device failure.
Treatment of hypertrophy
Treatment depends on the underlying cause of the enlarged ventricle and may include medications and/or surgery.
Left ventricular enlargement can be controlled by taking tablets
The most common medications prescribed for hypertrophy are the following.
Angiotensin-converting enzyme (ACE) inhibitors
These drugs dilate blood vessels, lower blood pressure, improve blood flow, and help reduce the workload of the heart. Trade names of the drugs: captopril, enalapril and lisinopril. The most common side effect is a persistent, irritating dry cough.
Angiotensin receptor blockers
These drugs are similar to ACE inhibitors, but do not cause a persistent cough.
Beta blockers
Beta blockers help lower your heart rate and normalize your blood pressure. Beta blockers are not usually prescribed as primary treatment for hypertrophy.
Diuretics
Thiazide diuretics help ease blood flow to the heart and lower blood pressure. Trade names: chlorthalidone and hydrochlorothiazide.
Only an experienced cardiologist will select the right type of pills
Surgical treatment consists of repairing or completely replacing the aortic valve.