Congenital heart defects are congenital heart defects, which are a disorder of the structure or function of the heart, as well as the great vessels, that arise due to improper embryogenesis.
They usually begin between 2 and 4 weeks of pregnancy and progress as organs develop. Defects lead to problems in the intracardiac circulation, and sometimes the entire circulatory system of the body. The danger is associated with heart failure, often resulting in death in childhood.
These pathologies occur in every hundredth newborn and have a different nature, location and degree of risk to the child’s life. Most often they are detected in infancy and childhood, but may first appear in adults.
Causes of occurrence and mechanism of development
Why are children born with heart defects? Congenital defects occur during the intrauterine development of the fetus. The development mechanism is associated with a combination of genetic, endogenous and extragenic factors. The genetic mechanism of etiology includes gene disorders of a point nature and chromosomal mutations (DNA deletion and duplication). The autosomal recessive type predominates in heredity.
In addition to the hereditary mechanism, genetic mutations can be caused by external mutagens:
- Physical nature - radiation and ionizing exposure.
- Chemical exposures - alcohol poisoning, smoking, drug treatment (antibiotics, NSAIDs and others), paint products, nitrates, thalidomide.
- Biological factors - diseases during pregnancy (rubella, measles, chicken pox, enteroviruses), diabetes mellitus, hyper- or vitamin deficiency, hypoxia.
The development of congenital heart disease occurs through two mechanisms: disruption of intracardiac or systemic hemodynamics. In the first case, there is overload of the cardiac sections, blockage of the ducts, depletion of compensatory mechanisms, hypertrophy and dilatation of the organ sections, and heart failure. Systemic failures develop in the form of systemic hypoxia, anemia (excess blood) in the circulatory system.
Hemodynamic disturbance
When these factors-causes are exposed and manifested in the fetus during development, characteristic disturbances occur in the form of incomplete or untimely closure of the membranes, underdevelopment of the ventricles and other anomalies.
Intrauterine development of the fetus is distinguished by the functioning of the ductus arteriosus and the oval window, which is in an open state. The defect is diagnosed when they still remain open.
The presented pathology is characterized by the absence of manifestations in intrauterine development. But after birth, characteristic disorders begin to appear.
Such phenomena are explained by the time of closure of the communication between the systemic and pulmonary circulation, individual characteristics and other defects. As a result, the pathology can make itself felt some time after birth.
Often, hemodynamic disorders are accompanied by respiratory infections and other concomitant diseases. For example, the presence of a pale type pathology, where arteriovenous discharge is noted, provokes the development of pulmonary hypertension, while a blue type pathology with a venoarterial shunt promotes hypoxemia.
The danger of the disease in question lies in the high mortality rate. Thus, a large discharge of blood from the pulmonary circulation, provoking heart failure, in half of the cases ends in the death of the baby before the age of one, which is preceded by the lack of timely surgical care.
The condition of a child over 1 year of age improves noticeably due to a decrease in the amount of blood entering the pulmonary circulation. But at this stage, sclerotic changes often develop in the vessels of the lungs, which gradually provokes pulmonary hypertension.
Symptoms appear depending on the type of anomaly, the nature and time of development of circulatory disorders. When the cyanotic form of the pathology develops in a sick child, a characteristic blueness of the skin and mucous membranes is noted, which increases its manifestation with each strain. The white defect is characterized by pallor, constantly cold hands and feet of the baby.
The baby himself with the presented disease differs from others in hyperexcitability. The baby refuses to breastfeed, and if he starts sucking, he quickly gets tired. Often, children with this pathology are diagnosed with tachycardia or arrhythmia; external manifestations include sweating, shortness of breath and pulsation of neck vessels.
In the case of a chronic disorder, the child lags behind his peers in weight, height, and there is a physical delay in development. As a rule, at the initial stage of diagnosis, a congenital heart defect is listened to, where heart rhythms are determined. In the further development of the pathology, edema, hepatomegaly and other characteristic symptoms are noted.
Complications include bacterial endocarditis, venous thrombosis, including cerebral thromboembolism, congestive pneumonia, angina syndrome and myocardial infarction.
ICD-10 codes and classification
What types of congenital heart diseases are there? It is impossible to list them all. In the international classification system ICD-10, the defects in question are classified as congenital circulatory disorders:
- Code Q20 combines congenital heart defects in the form of defects of cardiac elements, incl. Q20.1, 2 and 4 include disorders of the ventricular inlet or outlet, Q20.3 and 5 defects of the ventricular-arterial and atrioventricular junction, Q20.8 and 9 - anomalies of other and unspecified types.
- Q21 – these are malformations of the septa.
- Q22 – CHD of the pulmonary and tricuspid valves.
- Q23 – defects of the aortic (Q23.0 and 1) and mitral (Q23.2 and 3) valves. This group includes left-sided cardiac hypoplasia (Q23.4).
- Q24 combines various types of congenital heart disease - levocardia (Q24.1), triatrial heart (Q24.2), subaortic stenosis (Q24.4), heart block (Q24.6) and some other disorders.
- Q25 – disadvantages of the formation of large arteries, incl. aorta (Q25.0-Q25.4), pulmonary artery (Q25.5-Q25.7).
- Q26 – congenital venous defects, incl. vena cava (Q26.0 and 1), pulmonary vein (Q26.2-Q26.4), portal vein (Q26.5).
- Q27 affects peripheral vascular pathologies.
- Q28 joins other circulatory system ACHDs.
The classification of heart defects provides a clearer diagnosis of the pathology, which makes it possible to unify the treatment regimen.
The division of pathology based on the presence of cyanosis is quite often used. Based on this feature, 2 types of congenital heart disease are distinguished: white defects (without cyanosis), in which a left-to-right shunt of blood occurs, and venous and arterial blood is not mixed, and blue defects with pronounced cyanosis (right-to-left shunt of blood with mixing of arterial and venous blood ).
Common types of pathology
Among congenital heart diseases, the most common pathologies in children can be identified:
- Triad of Fallot (ICD-10 code Q21.8). Refers to blue defects and includes the following disorders - obstruction of the right ventricular outflow tract, right ventricular hypertrophy and damage to the septum between the atria.
- Tetralogy of Fallot (Q21.3). It is characterized by disruption of the lumen of the pulmonary artery, damage to the interventricular septum, disruption of the location of the initial section of the aorta, and right ventricular hypertrophy. Considered a blue vice. Refers to the most common infant congenital heart disease.
- Pentade of Fallot (Q21.0). In addition to signs of tetrad, it includes destruction of the interatrial septum. This defect is rare, but life-threatening for the child.
- Defective septum between the atria (Q21.1). It consists of non-closure of the septum between the atria. This is a white UPS. Characterized by excess blood entering the small circle.
- Defective septum between the ventricles (Q21.0). Blood flow from the left ventricle enters the right through the patent septum. With this lesion, oxygen starvation occurs and shortness of breath develops.
- Arterial ducts are open type (Q25.0). These are the white type. In newborns, they can be found in the form of the Botallian duct, which is not related to pathologies. The defect becomes dangerous if the duct does not close with age. At an early stage it causes poor functioning of the respiratory system.
- Dextrocardia (Q24.0). The anomaly is characterized by improper placement of the heart, when a significant part of it is displaced to the right side of the chest. The location of blood vessels changes accordingly. There are 2 types - a non-isolated anomaly combined with a violation of the location of other internal organs and an isolated pathology with their usual placement.
- Cantrell Pentad (Q89.7). This is a very rare defect that falls into the lethal category. It includes developmental anomalies of the sternum, anterior abdominal wall, diaphragm, pericardium and heart. It is characterized by a downward displacement of the heart and its protrusion relative to the chest.
- Transposition of the great vessels (Q25.9). The defect is the abnormal placement of the aorta and artery relative to the heart ventricles. The aorta originates from the right ventricle, and the pulmonary artery originates from the left, which blocks the flow of blood and oxygen into the tissues.
- Coarctation of the aorta (Q25.1) or stenosis of the isthmus of the main artery. Its narrowing is noted, usually below the branch of the subclavian artery.
- Pulmonary stenosis (Q25.6). Occurs with the development of cyanosis. With this pathology, a narrowing of the mouth of the artery occurs, which prevents blood outflow into the artery during contraction of the right ventricle.
- Ebstein's anomaly (Q22.5). This is a defect of the tricuspid atrioventricular valve in the form of improper placement of the leaflets. An abnormal right ventricular area forms above the valve and fuses with the atrium.
- Pulmonary atresia (Q25.5). The defect causes dysfunction of the valve leaflets or incomplete opening of the leaflets. The flow of blood from the ventricle into the artery is blocked.
Important! Congenital defects come in many varieties. Some of them appear sharply immediately after birth, but many become noticeable as the child grows older (for example, in adolescence). Knowing the symptoms of heart defects will help you spot the danger in time.
VSP encoding
Heart defects are in the class of congenital anomalies of the structure of the body in the block of anomalies of the circulatory system. VSP in ICD 10 branches into 9 sections, each of which also has subparagraphs.
- Q20 – anatomical disorders in the structure of the cardiac chambers and their connections (for example, various clefts of the oval window);
- Q21 – pathologies of the cardiac septum (defects of the atrial and interventricular septa and others);
- Q22 – problems with the pulmonary and tricuspid valves (insufficiency and stenosis);
- Q23 – pathologies of the aortic and mitral valves (insufficiency and stenosis);
- Q24 – other congenital heart defects (change in the number of chambers, dextracardia, etc.).
Each of the listed points requires further differentiation, which will allow us to determine the treatment plan and prognosis for the child. For example, with lesions of the valves there may be phenomena of insufficiency or stenosis. In this case, the hemodynamic features of the disease will differ.
https://www.youtube.com/watch?v=S6pVzsC8jA4
In ICD, congenital heart disease implies some kind of blood flow disturbance.
That is why in all encodings complete inversion of organs or their structures with full functioning is excluded.
Save the link, or share useful information on social media. networks
How is congenital heart disease determined in the fetus?
Currently, congenital heart disease can be detected in a child before birth, i.e. in the mother's womb. The main method is ultrasound of the fetal heart. By the 10th week of pregnancy, the organ is sufficiently formed to evaluate its structure . The optimal period for the study is 19-23 weeks of pregnancy. If abnormalities are detected during ultrasound, echocardiography is performed using the Doppler method.
Ultrasound and echocardiography of the fetal heart can detect 70-80% of all congenital heart defects in the mother’s womb. It is difficult to detect tiny defects in the septa or valves. Some disorders (cardiomyopathies, tumors, fetal arrhythmias) are not detected because develop at a later date.
VPS ventricular septal defect ICD 10
Ventricular septal defect (VSD) is a congenital heart defect with communication between the right and left ventricles.
Code according to the international classification of diseases ICD-10:
- Q21.0 Ventricular septal defect
Causes
Etiology • Congenital malformations (isolated VSD, part of a combined congenital heart disease, for example, tetralogy of Fallot, transposition of the great vessels, truncus arteriosus, tricuspid valve atresia, etc.) • There is evidence of autosomal dominant and recessive types of inheritance. In 3.3% of cases, this defect is also found in direct relatives of patients with VSD • Rupture of the interventricular septum due to trauma and MI.
Statistical data • VSD accounts for 9–25% of all congenital heart defects • Is detected in 15.7% of live-born children with congenital heart disease • As a complication of transmural myocardial infarction - 1–3% • 6% of all VSDs and 25% of VSDs in infants are accompanied by a patent ductus arteriosus, 5 % of all VSDs - coarctation of the aorta, 2% of congenital VSDs - aortic valve stenosis • In 1.7% of cases, the interventricular septum is absent, and this condition is characterized as a single ventricle of the heart • The ratio of male to female sex is 1:1.
Pathogenesis. The degree of functional impairment depends on the amount of blood discharge and total pulmonary vascular resistance (TPVR). When shunting from left to right and the ratio of pulmonary minute volume to systemic blood flow (Qp/Qs) is less than 1.5:1, pulmonary blood flow increases slightly, and no increase in PVVR occurs.
With large VSDs (Qp/Qs more than 2:1), pulmonary blood flow and pulmonary blood flow significantly increase, and pressures in the right and left ventricles are equalized. As the blood volume increases, the direction of blood discharge may change - it begins to occur from right to left.
Without treatment, right and left ventricular failure and irreversible changes in the pulmonary vessels (Eisenmenger syndrome) develop.
Variants of VSD • Membranous VSD (75%) are located in the upper part of the interventricular septum, under the aortic valve and the septal cusp of the tricuspid valve, often close spontaneously • Muscular VSD (10%) are located in the muscular part of the interventricular septum, at a considerable distance from the valves and conduction system , are multiple, fenestrated and often close spontaneously • Supracrestal (VSD of the outflow tract of the right ventricle, 5%) are located above the supraventricular crest, often accompanied by aortic insufficiency of the aortic valve, do not close spontaneously • Open AV canal (10%) is found in the posterior part of the interventricular septum, near the site of attachment of the rings of the mitral and tricuspid valves, often found in Down syndrome, combined with ASD of the ostium primum type and malformations of the leaflets and chords of the mitral and tricuspid valves, does not close spontaneously • Depending on the size of the VSD, small ones are distinguished (Tolochinov-Roger disease ) and large (more than 1 cm or half the diameter of the aortic orifice) defects.
Symptoms (signs)
Clinical picture
• Complaints: see Atrial septal defect.
• Objectively • Pallor of the skin • Harrison's furrows • Increased apical impulse, trembling in the area of the left lower edge of the sternum • Pathological splitting of the second tone as a result of prolongation of the ejection period of the right ventricle • Rough pansystolic murmur at the left lower edge of the sternum • With supracrestal VSD - aortic diastolic murmur insufficiency.
Diagnosis in newborns and infants
Diagnosis of infants is carried out by a cardiologist . First of all, the doctor examines for the presence of cyanosis, shortness of breath involving the intercostal muscles, and changes in breathing when using an oxygen mask.
The heart is listened to to detect murmurs, blood pressure is measured, and a general blood test is performed.
The mandatory technique is cardiac ultrasound with color Doppler examination. An ECG with parallel recording of a phonocardiogram is highly informative.
Congenital defects in adults
Most congenital heart disease appears in childhood. However, some types of pathology do not manifest themselves for a long time, and only in adults (after 20-25 years) make themselves felt. The percentage of detected congenital heart disease in adults does not exceed 0.3%, which is due to the fact that the pathology has already manifested itself earlier.
Changes in the cardiovascular system are not static. Even small congenital heart defects gradually progress through the following mechanisms:
- proliferation of connective tissue in the arterioles of the lungs with obliteration;
- transformation of myocardial hypertrophy into a pathological form;
- formation of calcification in the valve system;
- progression of valvular dysfunction.
The role of thrombosis, pulmonary hypertension and infective endocarditis is increasing.
Small anomalies of heart development
Small anomalies of heart development: Brief description
Minor anomalies of cardiac development (MADC) are anatomical congenital changes in the heart and great vessels that do not lead to gross dysfunction of the cardiovascular system. A number of MARS are unstable and disappear with age.
Hereditary determined connective tissue dysplasia. A number of MARS are dysembryogenetic in nature. The influence of various environmental factors (chemical, physical effects) cannot be excluded.
Code according to the international classification of diseases ICD-10:
Is treatment always necessary?
The need and principle of treatment for congenital heart disease requires taking into account the severity of the clinical picture and the extent of the lesion . In some cases, cardiovascular disorders detected in newborns heal on their own (for example, open ducts).
Some congenital heart defects may not affect the functioning of the organ at all, unless extreme conditions are created. The question of the need for treatment is decided by a cardiologist after conducting the necessary diagnostic tests. In any case, the behavior of the anomaly must be kept under control.
What additional chords can there be?
So, depending on the location, the chords can be longitudinal, diagonal and transverse. If it is located in the area of the apex, base or in the middle part, it is described accordingly - apical, basal and median. This anomaly can occur not only in the left, but also in the right ventricle. The number of chords can be single or multiple. Depending on the histological structure, additional chords of the left ventricle can be fibrous (connective tissue), muscular and fibromuscular (mixed).
How to treat congenital heart disease: therapy and surgery
Treatment can be carried out surgically and therapeutically . Emergency surgery is performed when there is a direct threat to the child’s life. Elective surgeries are performed when there is an increased risk of severe complications. They take into account the child’s age and are often postponed for a period of 5-7 years.
If surgery is not indicated or contraindicated, then therapeutic treatment may be prescribed. However, even therapy must be carried out carefully. General strengthening and preventive medications are indicated.
Radical therapy with potent drugs is prescribed for acute left ventricular and chronic heart failure, cyanotic attacks, breathing problems, significant cardiac arrhythmia, and myocardial ischemia.
The method is chosen by the cardiologist based on the examination completed, the patient’s age and the type of congenital heart defect.
- Taking medications . Drug therapy is prescribed to patients who have been diagnosed with a birth defect in adulthood. In this case, surgical methods are often not used.
- Long-term treatment in stages . In some cases, children with this condition require lifelong treatment. This includes surgical correction and medication. Patients require constant care. These procedures significantly prolong life.
- Cardiac catheterization . The most common treatment method is cardiac catheterization. This procedure is performed without opening the chest. The doctor inserts a catheter through a vein and repairs defects in the heart muscle using surgical instruments at the end of the catheter. In some cases this method is not applicable.
- Open heart surgery . Surgery is used in cases where the defect cannot be eliminated with a catheter. This method requires long-term recovery for the patient.
- Heart transplant . This method is used when surgery does not bring the desired result.
- Observation by the attending physician and supportive treatment . After surgery, the patient should be monitored by the attending physician. Congenital defects of the heart muscle may be associated with problems with other organs. It is necessary to teach an adult child to monitor his condition and take prescribed medications.
- Limiting activity . Children with congenital heart defects should be limited in activity. Parents should constantly monitor their child's activities and ensure that they are calm and not dangerous. Safe exercises for such patients can be found out from your doctor.
- Infection prevention . In some cases, patients with congenital heart defects are prescribed antibiotic therapy to prevent infections. Patients undergo this procedure before any surgical interventions.
Medical examination and rehabilitation of children with congenital heart defects
PPS - acquired heart defects (valvular defects) - a group of chronic diseases characterized by structural and functional changes in the valvular apparatus of the heart as a result of an infectious-inflammatory or autoimmune disease.
Unlike congenital defects, PPS are not associated with genetic abnormalities and are characterized by a slow progressive course.
Acquired heart defects are found in adults of both sexes aged 25-40 years. Men get sick 1.5-2 times more often than women: the incidence in men is 3.4%, in women - 1.7-2%.
Valvular defects never develop primarily. The causes of acquired heart defects are usually rheumatism (the main cause, the most common), infective endocarditis, syphilis and atherosclerosis.
Damage to the valve begins with the deposition of specific structures on it: a cholesterol plaque, a bacterial colony or auto-antibodies, which have a direct damaging effect on it.
The result of destruction is deposits of calcium and connective fibers (fibrosis), as a result of which the valve loses its elasticity and correct configuration - its folds decrease and shift. This leads to a gradual loss of its function and disruption of the heart.
Usually this disease affects the mitral valve, the others (tricuspid, aortic and pulmonary valve) are affected less frequently. The most common are rheumatic heart defects.
Classification
| Localization | View | Incidence of cases per 100,000 population |
| Mitral valve disease | Stenosis | 1500 |
| Failure | 400 | |
| Aortic valve disease | Stenosis | 2000 |
| Failure | 1000 | |
| Tricuspid valve | Stenosis | 300 |
| Failure | 400 | |
| Pulmonary valve | Stenosis | 200 |
| Failure | 300 | |
| Combined defects | Stenosis of 2 or 3 valves | 25-30 |
| Insufficiency of 2 or 3 valves | Isolated cases | |
| Combination of stenosis and insufficiency of 2 or 3 valves | ||
| Combination of stenosis and insufficiency in 1 valve | 400-1000 |
Non-rheumatic defects (codes for the rest are below in the description):
- Mitral: I34.0, I34.1, I34.2.
- Aortic: I35.0, I35.1, I35.2.
- Tricuspid: I36.0, I36.1, I36.2.
- Non-rheumatic lesions of the pulmonary valve: I37.0, I37.1, I37.2.
Description of common defects:
- Mitral insufficiency (I05.1). It is characterized by inadequate closure of the bicuspid valve, resulting in the return of blood to the left atrium. A blue defect with excessive blood supply to the lungs, manifested by blueness of the skin, increased breathing and rapid exhaustion.
- Mitral stenosis (I05.0). The defect is represented by a decrease in the mitral orifice, as a result of which insufficient blood flows into the left ventricle. The atrium experiences increased pressure and hypertrophies. Blue defect with enrichment of pulmonary blood supply, manifested by cyanosis, shortness of breath, dizziness.
- Aortic insufficiency (I06.1). A defect caused by a loose connection of the semilunar aortic folds, due to which, at the time of diastole, blood moves back into the left ventricle, causing its overflow and hypertrophy. White defect with depletion of blood supply to internal organs, arterial hypertension, chilliness.
- Aortic stenosis (I06.0). Represented by narrowing of the aortic opening. The lesion is manifested by insufficient blood flow into the aorta during systole, which leads to left ventricular hypertrophy. White defect with depletion of the large circle, hypertension, chilliness, physical weakness.
- Triscupidal insufficiency (I07.1). It manifests itself as incomplete or untimely connection of the leaflets of the right atrioventricular valve, resulting in the reflux of blood into the right atrium. Blue defect, manifested by blueness of the skin, swelling of the legs, swelling of the neck veins, and weakness.
- Triscupidal stenosis (I07.0). It is represented by narrowing of the tricuspid ring and poor blood supply to the right ventricle at the moment of cardiac relaxation. Blue defect with insufficient blood supply to the lungs, shortness of breath, enlarged liver.
- Pulmonary valve insufficiency (I37.1). The defect is caused by incomplete connection of the valve leaflets between the right ventricle and the pulmonary artery, as a result of which the blood partially returns to the ventricle, causing its hypertrophy. Blue defect with depletion of pulmonary blood supply, shortness of breath, cyanosis, fainting.
- Pulmonary valve stenosis (I37.0). The lesion consists of a narrowed opening of the pulmonary valve, resulting in insufficient blood flowing into the lungs. Blue defect, accompanied by right ventricular hypertrophy, cerebral hypoxia, edema, and enlarged liver.
It is an irreversible form of pulmonary hypertension acquired due to a congenital cardiac abnormality. It is a combination of a ventricular septal defect, right ventricular hypertrophy and reverse aortic position.
Eisenmeiger syndrome manifests itself with pulmonary edema and cyanosis in adulthood in unoperated individuals with pronounced right-to-left shunting.
General symptoms
At an early stage of the disease, symptoms may be minor or absent altogether, so the patient does not take them into account. Here is a list of the first signs of cardiac muscle dysfunction:
- heartbeat becomes rapid;
- a dry cough appears;
- the voice becomes hoarse;
- shortness of breath bothers you;
- pain and feeling of fullness in the chest;
- the patient may cough up blood;
- loss of consciousness;
- dizziness;
- a blush may appear on the cheeks;
- swelling of the legs.
PPS rarely reveal themselves at the initial stage. Vivid symptoms appear already during the period of active development of the disease, so you should undergo examination at the first signs of disruption of the heart muscle.
- Questioning: history of previous infectious disease or atherosclerosis, complaints of weakness and fatigue, interruptions in heart function, shortness of breath, fainting.
- Examination: cyanosis (blue blemishes) or pallor (white blemishes) of the skin; visible pulsation and swelling of the neck veins, rapid breathing, swelling of the legs, cold skin.
- Measurement of pressure, pulse and respiratory rate: indicators can be either altered or within normal limits.
- Palpation: displaced apical impulse, presence of cardiac impulse, dense swelling of the legs.
- Percussion: increase in cardiac and hepatic boundaries.
- Auscultation: detection of heart murmurs, additional 3rd and 4th sounds, “ri”, specific murmurs (systolic, diastolic, mixed).
- Laboratory data: anemia, increased levels of alkaline phosphatase, aminotransferases, cholesterol, sugar.
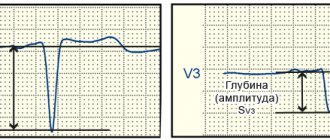
- ECG: arrhythmias, blockades, prolongation of repolarization (change in T wave), non-simultaneous excitation of the cardiac chambers (bifurcated and widened P and R waves).
- X-ray: enlargement of the atria or ventricles, depletion of the pulmonary pattern, displacement of the vascular bundle and dome of the diaphragm.
- Echocardiography: location, type and degree of valve displacement.
- Dopplerography: recording the strength and magnitude of reverse blood flow.
- Probing, CT and MRI help confirm the diagnosis in controversial cases.
PPPs can be compensated, subcompensated and decompensated.
The compensated form is slightly expressed, and therefore treatment of acquired heart disease is limited to taking medications. Subcompensation requires mandatory surgical treatment, and decompensation, as a rule, inevitably causes death (patients need palliative therapy).
Cases when treatment is not required are extremely rare, since all valve defects are characterized by a steadily progressive course.
Types of surgical interventions:
- Commissurotomy - dissection of adhesions between the valves;
- Balloon valvuloplasty – expansion of the valve using a pressurized balloon;
- Prosthetics – complete valve replacement.
Types of operations depending on the location of the lesion:
- Mitral stenosis – prosthetics, commissurotomy, valvuloplasty.
- Mitral insufficiency – valvuloplasty, prosthetics.
- Aortic defects - installation of a prosthesis.
- Tricuspid stenosis – commissurotomy, valvuloplasty, prosthetics.
- Tricuspid insufficiency – valvuloplasty and prosthetics.
- Pulmonary artery defects – prosthetics.
PPS can develop at any age. In children, pathology occurs much less frequently (in 0.5% of cases), since primary diseases are more typical for the adult population.
The clinical manifestations of the acquired defect in a child are the same as in adults (shortness of breath, blue or pale skin, swollen veins, arrhythmia, enlarged liver), but they appear more clearly and are accompanied by crying, refusal to eat, rapid weight loss, and dystrophy.
Detection of the disease occurs faster (more often - in the first year of the disease, while in adults - in 2-4 years).
The leading diagnostic methods for children are ECG, radiography and ultrasound of the heart.
Consequences of PPP
- Pulmonary edema;
- Brain hypoxia;
- Arrhythmias and blockades;
- Ventricular fibrillation;
- Acute decompensation;
- Heart failure;
- Death.
Prevention of PPS:
- Cholesterol level control;
- Elimination of harmful occupational factors;
- Mandatory treatment of streptococcal infection to avoid rheumatism;
- Therapy of chronic diseases;
- Hardening;
- Registration with a cardiologist in the presence of any heart disease.
Forecast
The prognosis without treatment is unfavorable. The disease inevitably leads to heart failure, and acute decompensation leads to the death of the patient. Working capacity is significantly reduced, even to the point of loss.
After treatment, the patient must adhere to the following rules:
- taking medications regularly;
- adherence to diet and regimen;
- maintaining normal weight;
- absence of bad habits;
- exclusion of all harmful foods from the diet;
- frequent walks;
- constant monitoring by the attending physician.
How long do people live with acquired heart disease? Life expectancy with minor valve damage is reduced by 2-3 years. Patients with severe forms live from 8 to 25 years from the moment of diagnosis and often reach the age of 55-60 years.
The presence of a defect is an indication for determining disability.
A decrease in the quality of life is manifested in the loss of physical strength, the inability to cross long distances due to constant shortness of breath. Patients move slowly, are forced to change shoes and clothes due to severe swelling, and suffer from insomnia. Excessive consumption of salt and sugar, stress, and active exercise are contraindicated for them.
Consequences
The degree of danger of congenital heart disease for the life of a child and an adult depends on their type and rate of progression. If measures are not taken, in some cases death is possible. In addition, the progression of the pathology can cause the following complications:
- heart failure;
- bacterial endocarditis with the development of blue type congenital heart disease;
- pneumonia;
- Eisenmenger syndrome;
- hypertension;
- strokes of ischemic or hemorrhagic type;
- myocardial infarction;
- angina pectoris;
- attacks of shortness of breath;
- anemia of a relative nature.
Types of heart defects
Let's find out how many types of heart defects there actually are. The UK National Health Service will help us with this, which has identified more than 30 positions, but it’s worth talking about only the 2 most important:
- Congenital heart defect, ICD code 10 (Q20-Q28) blue type, more precisely, with cyanosis.
This heart failure is caused by low levels of oxygen in the blood. Babies may suffer from fatigue, shortness of breath and sudden fainting. They tend to have blue fingers, toes and lips.
- Acyanotic syndrome.
Unlike the first type, the blood is quite saturated with oxygen, however, it circulates in the body in an unusual way. In newborns, symptoms do not appear immediately, but over time. Blood pressure exceeds the permissible norm, forcing the heart to work in emergency mode.
The patient may experience frequent and rapid fatigue, dizziness, shortness of breath and pulmonary hypertension.
Approximately every 6th child is born with various cardiac abnormalities. Half of them require immediate hospitalization and surgery. The remaining part will be forced to see a doctor several years later.
In addition, genetic diseases such as Down syndrome and infectious diseases (rubella) can become the basis for the development of birth defects.
Lifespan
How long do people live with congenital heart disease? Life expectancy depends on the timeliness and effectiveness of measures taken. CHD is the most dangerous for newborns.
Statistics show that up to 60% of infants with congenital heart disease do not survive to 1 year and up to 80% - to 5 years. Only 15-18% of children survive to conscious age without surgical treatment.
A certain deterioration in the condition is observed at the age of 13-16 years, which is associated with increased workload, psychological stress and hormonal changes.
Modern medicine has made a significant contribution to improving survival rates. Surgical intervention makes the prognosis for cure favorable. On average, with a successful operation, life expectancy is 35-40 years.
How to cure congenital heart disease?
Often such problems do not require serious treatment and go away on their own. But there are exceptions in which surgery and a course of medications are the only correct solution. The operation is prescribed based on the ICD 10 specification for congenital heart disease.
- Under the supervision of doctors. If the defects are not as severe, regular medical examinations may be required to prevent progression of the disease.
- A catheter is a long, flexible tube that is inserted into the heart. This method is considered safe for the baby and does not require any major surgical incisions in the chest area.
- Surgery or heart transplant. It is used only when a person’s life depends on it.
Be sure to consult with specialists if anything worries you. Take care of your health, practice good habits and love the people around you.
There is no need to give up on yourself and accept the fact that you will always have to live with heart failure. We live in the 21st century, when it is possible to cure almost any disease or disorder. The main thing is to believe in a bright future and never give up hope, because it dies last.
Is it possible to prevent development?
It is most effective to exclude external mutagens during pregnancy. To do this, it is necessary to promptly treat diseases that can provoke congenital heart disease in the fetus. Medicines must be taken strictly as prescribed by the doctor. Alcohol and smoking are absolutely prohibited.
Carrying out an ultrasound of the fetal heart at an early stage of pregnancy will allow timely detection of pathology. Modern medicine is capable of treating (including surgery) the fetus even directly in the mother’s womb.