What is myocardial hypertrophy
This autosomal dominant disease is characterized by hereditary traits of gene mutation and affects the heart. It is characterized by an increase in the thickness of the walls of the ventricles. Hypertrophic cardiomyopathy (HCM) has a classification code according to ICD 10 No. 142. The disease is often asymmetric, with the left ventricle of the heart more susceptible to damage. This happens:
- chaotic arrangement of muscle fibers;
- damage to small coronary vessels;
- formation of areas of fibrosis;
- obstruction of blood flow - an obstacle to the ejection of blood from the atrium due to displacement of the mitral valve.
With heavy loads on the myocardium caused by diseases, sports, or bad habits, the body’s protective reaction begins. The heart needs to cope with increased work volumes without increasing the load per unit of mass. Compensation begins to occur:
- increased protein production;
- hyperplasia – increase in the number of cells;
- increase in myocardial muscle mass;
- wall thickening.
Pathological myocardial hypertrophy
With prolonged work of the myocardium under loads that are constantly increased, a pathological form of HCM occurs. A hypertrophied heart is forced to adapt to new conditions. Myocardial thickening occurs at a rapid pace. In this situation:
- growth of capillaries and nerves lags behind;
- blood supply is disrupted;
- the influence of nervous tissue on metabolic processes changes;
- myocardial structures wear out;
- the ratio of myocardial sizes changes;
- systolic and diastolic dysfunction occurs;
- repolarization is disrupted.
Myocardial hypertrophy in athletes
Abnormal development of the myocardium—hypertrophy—occurs unnoticed in athletes. During high physical activity, the heart pumps large volumes of blood, and the muscles, adapting to such conditions, increase in size. Hypertrophy becomes dangerous, causing stroke, heart attack, sudden cardiac arrest, in the absence of complaints and symptoms. You should not suddenly stop training to avoid complications.
Sports myocardial hypertrophy has 3 types:
- eccentric - muscles change proportionally - typical for dynamic activities - swimming, skiing, long-distance running;
- concentric hypertrophy - the ventricular cavity remains unchanged, the myocardium increases - observed in gaming and static types;
- mixed - inherent in activities with the simultaneous use of immobility and dynamics - rowing, cycling, skating.
Myocardial hypertrophy in a child
It is possible that myocardial pathologies may appear from the moment of birth. Diagnosis at this age is difficult. Hypertrophic changes in the myocardium are often observed during adolescence, when cardiomyocyte cells actively grow. Thickening of the anterior and posterior walls occurs until the age of 18, then stops. Ventricular hypertrophy in a child is not considered a separate disease - it is a manifestation of numerous ailments. Children with HCM often have:
- heart disease;
- myocardial dystrophy;
- hypertension;
- angina pectoris.
Left ventricular hypertrophy on the ECG: recommendations from a cardiologist
Anatomical hypertrophy of the left ventricle is manifested on the electrocardiogram (ECG) by a number of signs. A functional diagnostics doctor or cardiologist takes into account the number and severity of such signs.
There are several diagnostic criteria that more or less correctly identify hypertrophy (from 60 to 90% probability). Therefore, not all people with signs of left ventricular hypertrophy on the ECG actually have it.
Not all patients with anatomical hypertrophy show it on the ECG.
Moreover, the same ECG can be described differently by different doctors if they use different diagnostic criteria in their work.
What diseases does this happen in?
- Left ventricular hypertrophy occurs in young people who are constantly involved in sports. Their heart muscle works intensely during training and naturally increases its mass and volume;
- occurs in diseases associated with difficulty in the exit of blood from the left ventricle into the aorta and with an increase in vascular resistance in the body;
- this ECG sign may be the first symptom of severe heart defects - aortic stenosis and aortic insufficiency. These diseases cause deformation of the valve separating the left ventricle and the aorta. The heart works under a heavy load, but the myocardium copes with it for a long time. A sick person does not feel any discomfort for a long time;
- Left ventricular hypertrophy occurs in a serious disease – hypertrophic cardiomyopathy. This disease is manifested by severe thickening of the walls of the heart. Thickened walls “block” the exit from the left ventricle, and the heart works under load. The disease does not appear immediately; shortness of breath and swelling gradually appear. In advanced cases, this disease may be an indication for heart transplantation.
- This is one of the manifestations of heart damage due to arterial hypertension. It can also develop with a moderate but constant increase in pressure. It is precisely to stop the progression of left ventricular hypertrophy that recommendations are aimed at constantly taking medications for hypertension, even with normal pressure.
- may appear in older people with severe atherosclerosis of the heart valves. This narrows the opening from the left ventricle into the aorta.
What could this lead to?
If a person has signs of left ventricular hypertrophy on an ECG, but it is not confirmed by echocardiography (ultrasound of the heart), there is no reason to worry. This ECG feature is probably due to increased body weight or a hypersthenic constitution. The ECG phenomenon of left ventricular hypertrophy itself is not dangerous.
If hypertrophy on the ECG is accompanied by a real increase in muscle mass, in the future this can cause heart failure (shortness of breath, edema) and severe heart rhythm disturbances (ventricular extrasystole, ventricular tachycardia). Athletes should not forget about this when creating a training regimen.
What to do and how to treat
If a person's ECG shows left ventricular hypertrophy, he needs to undergo an ultrasound examination of the heart, or echocardiography (EchoCG).
This method will help to accurately determine the cause of the increase in myocardial mass, as well as evaluate heart failure.
If it is not possible to conduct echocardiography, it is recommended to perform radiography of the heart in two projections, sometimes with contrasting of the esophagus.
To exclude heart rhythm disturbances, it is recommended to undergo
daily ECG monitoring. To diagnose hypertension during the day, it is necessary to undergo 24-hour blood pressure monitoring.
Left ventricular hypertrophy is irreversible. However, treating the underlying condition helps prevent the condition from progressing. For example, angiotensin-converting enzyme inhibitors (enalapril, captopril and many others) widely used in the treatment of hypertension not only stop the development of hypertrophy, but also cause some regression.
Thus, if signs of left ventricular hypertrophy are detected on the ECG, it is necessary to contact a physician or cardiologist for further examination.
Prepared based on the article: https://doctor-cardiologist.ru/gipertrofiya-levogo-zheludochka-na-ekg-rekomendacii-kardiologa
Take care of yourself and subscribe to our Zen channel, good luck!
The information is provided for informational purposes only. Do not self-medicate. At the first sign of disease, consult a doctor.
Source: https://zen.yandex.ru/media/id/5a294b285a104f22356138b9/5bc85379b3358100a919aa36
Causes of cardiomyopathy
It is customary to distinguish between primary and secondary causes of hypertrophic development of the myocardium. The first ones are influenced by:
- viral infections;
- heredity;
- stress;
- alcohol consumption;
- physical overload;
- excess weight;
- toxic poisoning;
- changes in the body during pregnancy;
- drug use;
- lack of microelements in the body;
- autoimmune pathologies;
- malnutrition;
- smoking.
Secondary causes of myocardial hypertrophy are provoked by the following factors:
- mitral valve insufficiency;
- arterial hypertension;
- heart defects;
- neuromuscular diseases;
- electrolyte imbalance;
- parasitic processes;
- pulmonary diseases;
- IHD;
- aortic stenosis;
- violation of metabolic processes;
- ventricular septal defect (VSD);
- lack of oxygen in the blood;
- endocrine pathologies.
Left ventricular hypertrophy
More often, the walls of the left ventricle are susceptible to hypertrophy. One of the causes of LVH is high pressure, which forces the myocardium to work at an accelerated rhythm. Due to the resulting overloads, the left ventricular wall and IVS increase in size. In this situation:
- the elasticity of the myocardial muscles is lost;
- blood circulation slows down;
- normal heart function is disrupted;
- there is a danger of a sudden load on it.
Left ventricular cardiomyopathy increases the heart's need for oxygen and nutrients. Changes in LVH can be noticed during instrumental examination. Low output syndrome appears - dizziness, fainting. Among the signs accompanying hypertrophy:
- angina pectoris;
- pressure changes;
- heartache;
- arrhythmia;
- weakness;
- high blood pressure;
- bad feeling;
- shortness of breath at rest;
- headache;
- fatigue;
- palpitations under light exertion.
Right atrial hypertrophy
Enlargement of the wall of the right ventricle is not a disease, but a pathology that appears when there is overload in this department. It occurs due to the receipt of a large amount of venous blood from large vessels. The cause of hypertrophy can be:
- birth defects;
- atrial septal defects, in which blood enters the left and right ventricles simultaneously;
- stenosis;
- obesity.
Right ventricular hypertrophy is accompanied by symptoms:
- hemoptysis;
- dizziness;
- night cough;
- fainting;
- chest pain;
- shortness of breath without exertion;
- bloating;
- arrhythmia;
- signs of heart failure - swelling of the legs, enlarged liver;
- malfunction of internal organs;
- cyanosis of the skin;
- heaviness in the hypochondrium;
- dilation of veins in the abdomen.
Hypertrophy of the interventricular septum
One of the signs of the development of the disease is hypertrophy of the IVS (interventricular septum). The main cause of this disorder is gene mutations. Hypertrophy of the septum provokes:
- ventricular fibrillation;
- atrial fibrillation;
- mitral valve problems;
- ventricular tachycardia;
- impaired blood flow;
- heart failure;
- cardiac arrest.
Dilation of the heart chambers
Hypertrophy of the interventricular septum can provoke an increase in the internal volume of the heart chambers. This expansion is called myocardial dilatation. In this position, the heart cannot perform the function of a pump, and symptoms of arrhythmia and heart failure occur:
- fast fatiguability;
- weakness;
- dyspnea;
- swelling of the legs and arms;
- rhythm disturbances;
Prevalence and causes of hypertrophy
Genetic defect
Geographically, the prevalence of HCM is variable. In addition, different regions take different age categories. It is difficult to provide precise epidemiological data because a disease such as hypertrophic cardiomyopathy does not have specific clinical symptoms. It is safe to say that the disease is more often detected in men. The third part of cases is represented by a familial form, the remaining cases are related to HCM, which has no connection with a hereditary factor.
The reason that leads to hypertrophy of the interventricular septum (IVS) is a genetic defect. This defect can occur in one of ten genes, each of which is involved in encoding information regarding the functioning of the contractile protein in the muscle fibers of the heart. To date, about two hundred such mutations are known, as a result of which hypertrophic cardiomyopathy develops.
Cardiac hypertrophy - symptoms
The danger of myocardial disease in asymptomatic progression for a long time. It is often diagnosed accidentally during medical examinations. As the disease progresses, signs of myocardial hypertrophy may be observed:
- chest pain;
- heart rhythm disturbance;
- shortness of breath at rest;
- fainting;
- fatigue;
- labored breathing;
- weakness;
- dizziness;
- drowsiness;
- swelling.
What is the danger of developing pathology
The progressive course of hypertrophy leads to ineffective cardiac output, which is manifested by the following complications:
- acute or chronic cardiac decompensation,
- sudden cardiac arrest,
- ventricular fibrillation,
- ischemia or infarction of the heart muscle,
- arterial thromboembolism,
- stroke.
Ventricular fibrillation as a consequence of left ventricular hypertrophy
Myocardial hypertrophy - classification
For convenience of work in medicine, it is customary to distinguish between the following types of myocardial hypertrophy:
- obstructive – at the top of the septum, over the entire area;
- non-obstructive – symptoms are mild, diagnosed by chance;
- symmetrical – all walls of the left ventricle are affected;
- apical - the heart muscles are enlarged only from above;
- asymmetrical - affects only one wall.
Eccentric hypertrophy
With this type of LVH, the ventricular cavity expands and at the same time a uniform, proportional compaction of the myocardial muscles occurs, caused by the growth of cardiomyocytes. With a general increase in heart mass, the relative thickness of the walls remains unchanged. Eccentric myocardial hypertrophy can affect:
- interventricular septum;
- top;
- side wall.
Concentric hypertrophy
The concentric type of disease is characterized by maintaining the volume of the internal cavity while increasing the mass of the heart due to a uniform increase in wall thickness. There is another name for this phenomenon - symmetrical myocardial hypertrophy. The disease occurs as a result of hyperplasia of myocardiocyte organelles, provoked by high blood pressure. This development of events is typical for arterial hypertension.
Pathogenesis
Changes in hypertrophy of the interventricular septum
What happens with hypertrophy of the interventricular septum? There are several interrelated pathological changes that occur during myocardial hypertrophy. First, thickening of the myocardium occurs in the specified area separating the right and left ventricles. The thickening of the interventricular septum is not symmetrical, so such changes can occur at any site. The most unfavorable option is thickening of the septum in the outflow tract of the left ventricle.
This causes one of the leaflets of the mitral valve, which separates the left atrium and ventricle, to come into contact with the thickened IVS. As a result, the pressure in this area (outflow section) increases. At the moment of contraction, the myocardium of the left ventricle has to work with greater force so that blood from this chamber enters the aorta. Under conditions of continued increased pressure in the outflow tract and in the presence of hypertrophy of the IVS of the heart, the myocardium of the left ventricle loses its former elasticity and becomes stiff or rigid.
Losing the ability to adequately relax during diastole or filling, the left ventricle begins to perform its diastolic function worse. The chain of pathological changes does not end here; diastolic dysfunction entails a deterioration in the blood supply to the myocardium. Ischemia (oxygen starvation) of the myocardium occurs, which is subsequently supplemented by a decrease in the systolic function of the myocardium. In addition to the IVS, the thickness of the walls of the left ventricle may also increase.
Diagnosis of hypertrophic cardiomyopathy
At the initial stage, with a slight development of wall hypertrophy, it is very difficult to identify the disease. The diagnostic process begins with interviewing the patient, finding out:
- presence of pathologies in relatives;
- the death of one of them at a young age;
- past diseases;
- fact of radiation exposure;
- external signs during visual inspection;
- blood pressure values;
- indicators in blood and urine tests.
A new direction is being used – genetic diagnosis of myocardial hypertrophy. The potential of hardware and radiological methods helps to establish the parameters of HCM:
- ECG - determines indirect signs - rhythm disturbances, hypertrophy of sections;
- X-ray - shows an increase in the contour;
- Ultrasound – assesses myocardial thickness, blood flow disturbances;
- echocardiography – records the location of hypertrophy, diastolic dysfunction;
- MRI – gives a three-dimensional image of the heart, determines the degree of myocardial thickness;
- ventriculography – examines contractile functions.
Atrial hypertrophy
A relatively common pathology in children. It is observed in the case of simultaneous violation of the mitral valve and tricuspid valve, with other heart defects that are congenital in nature, as well as with an atrial septal defect. Also, hypertrophy of both atria occurs as a concomitant disorder with carditis.
Doctors note that diagnosing biatrial enlargement (atrial hypertrophy) is more difficult than with isolated atrial defects. As with other types of hypertrophy, the main diagnostic methods are ECG and ultrasound of the heart.
How to treat cardiomyopathy
The main goal of treatment is to return the myocardium to its optimal size. Activities aimed at this are carried out in a comprehensive manner. Hypertrophy can be cured when diagnosed early. An important part in the system of myocardial health is played by lifestyle, which implies:
- diet;
- giving up alcohol;
- smoking cessation;
- weight loss;
- drug exclusion;
- limiting salt intake.
Drug treatment of hypertrophic cardiomyopathy includes the use of drugs that:
- reduce blood pressure - ACE inhibitors, angiotensin receptor antagonists;
- regulate heart rhythm disturbances - antiarrhythmics;
- drugs with a negative ionotropic effect relax the heart - beta blockers, calcium antagonists from the verapamil group;
- remove fluid - diuretics;
- improve muscle strength - ionotropes;
- if there is a threat of infective endocarditis, antibiotic prophylaxis.
An effective method of treatment that changes the course of excitation and contraction of the ventricles is dual-chamber pacing with a shortened atrioventricular delay. More complex cases - severe asymmetric hypertrophy of the IVS, latent obstruction, lack of effect of the drug - require the participation of surgeons for regression. Help save a patient's life:
- installation of a defibrillator;
- pacemaker implantation;
- transaortic septal myectomy;
- excision of part of the interventricular septum;
- transcatheter septal alcohol ablation.
Diagnosis and treatment
Echocardiographic examination
Despite the fact that standard diagnosis should begin with the patient’s complaints, for the first time, hypertrophy of the IVS and left ventricle can be detected using an echocardiographic study (EchoCG, cardiac ultrasound). In addition to physical methods for diagnosing hypertrophy of the IVS and left ventricle, carried out in the doctor’s cabin, laboratory and instrumental methods are used. The following instrumental diagnostic methods are used:
- Electrocardiography (ECG). The main ECG signs of myocardial hypertrophy of the interventricular septum and left ventricle are: signs of overload and enlargement of the left heart, negative T waves in the chest leads, deep atypical Q waves in leads II, III aVF; disturbance of rhythm and conduction of the heart.
- X-ray of the chest organs.
- 24-hour Holter ECG monitoring.
- Ultrasound of the heart. Today, this method is the leading one in diagnostics and represents the “gold standard”.
- Magnetic resonance imaging Coronary angiography.
- Genetic diagnosis uses a mapping method. DNA analysis of mutant genes is used.
All of these diagnostic methods are not only used to make a diagnosis of HCM, but to carry out differential diagnosis in relation to a number of similar diseases.
Normalization of body weight
Treatment of hypertrophic cardiomyopathy has several goals: to reduce the manifestations of the disease, slow down the progression of heart failure, prevent life-threatening complications, etc. Like most, if not all cardiac diseases, HCM requires non-drug measures that contribute to the progression of the disease. The most important are normalizing body weight, giving up bad habits, and normalizing physical activity.
The main groups of drugs for the treatment of IVS and left ventricular hypertrophy are beta-blockers, calcium channel blockers (verapamil), anticoagulants, angiotensin-converting enzyme inhibitors, angiotensin receptor antagonists, diuretics, class 1A antiarrhythmics (disopyramide, amiodarone). Unfortunately, HCM is difficult to treat with medication, especially if there is an obstructive form and insufficient effect of drug therapy.
Today, there are the following options for surgical correction of hypertrophy:
- excision of hypertrophied cardiac muscle in the area of the IVS (myoseptectomy),
- mitral valve replacement, mitral valve repair,
- removal of hypertrophied papillary muscles,
- alcohol septal ablation.
Cardiomyopathy - treatment with folk remedies
On the recommendation of the treating cardiologist, you can supplement the main course with herbal remedies. Traditional treatment for left ventricular hypertrophy involves the use of viburnum berries without heat treatment, 100 g per day. It is useful to consume flax seeds, which have a positive effect on heart cells. Recommend:
- take a spoonful of seeds;
- add boiling water - liter;
- hold in a water bath for 50 minutes;
- filter;
- drink per day - dose 100 g.
Oat infusion for regulating the functioning of the heart muscles has good reviews in the treatment of HCM. According to the healers' prescription, it is required:
- oats – 50 grams;
- water – 2 glasses;
- heat to 50 degrees;
- add 100 g of kefir;
- pour in radish juice - half a glass;
- stir, stand for 2 hours, strain;
- put 0.5 tbsp. honey;
- dosage – 100 g, three times a day before meals;
- course – 2 weeks.
Diagnostic methods
Patients' complaints are not specific, so they are guided by data from instrumental research methods.
ECG indications
The main signs of an increase in LV size are:
- axis shift to the left,
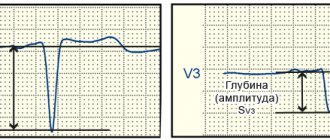
- R waves are high in the left, and S waves are high in the right leads,
- Q is deepened in the left leads,
- ST is shifted below the isoline,
- There may be a left bundle branch block.
Ultrasound
A thickened apex of the heart, septum, anterior and posterior walls are revealed; there may be areas of decreased contractility. The level of pressure in the ventricles and atria, the difference between the aorta and the LV, and cardiac output are measured. In addition, changes in the size of the heart cavities are detected. The method is especially informative for diagnosing defects.
MRI
Allows you to obtain a layer-by-layer picture of changes in the LV, assess its ability to eject blood during systole and the distensibility of the walls in the diastolic phase, detect areas with ischemia, and also measure basic parameters (wall thickness, chamber sizes), and the condition of the valve apparatus.
Watch the video about left ventricular hypertrophy:
What causes age-related cardiac hypertrophy in children?
Hypertrophic changes in the myocardium may in some cases be a physiological variant of the norm, but in most cases they represent a syndrome that reflects the presence of a congenital or acquired cardiovascular pathology in the body.
Of all parts of the heart, the left ventricle (LV) is most often subject to hypertrophic changes. The cause of LV hypertrophy not associated with diseases is physical activity. Left ventricular hypertrophy is a common heart change in athletes, as well as people whose work involves physical labor. Pathological causes leading to the development of hypertrophy in the left ventricle:
- Arterial hypertension;
- Hypertrophic cardiomyopathy;
- Aortic valve stenosis or insufficiency;
- Obesity.
The insidiousness of cardiac hypertrophy in the left ventricular region lies in the long absence of symptoms.
Later, when the hypertrophied myocardium cannot cope with the increased load, the following manifestations will be observed:
- Pressing pain behind the sternum;
- Dyspnea on exertion/at rest;
- Rapid or irregular heart rhythm due to hypertrophy;
- Fast fatiguability;
- Fainting;
- Dizziness.
This localization of phenomena
appears to be quite rare.
The main etiological factors that can lead to cardiac hypertrophy in the right ventricle are:
- Congenital heart anomalies: tetralogy/pentade of Fallot, VSD (ventricular septal defect);
- Diseases of the bronchopulmonary system: chronic obstructive bronchitis, pneumosclerosis, bronchial asthma, emphysema;
- Pathology of the valve on the pulmonary artery: its stenosis or insufficiency;
- Pulmonary hypertension.
Just like LV hypertrophy, at first the symptoms of the pathology are scanty and uninformative.
The most characteristic manifestations of the progression of the pathology are:
- Swelling of the lower extremities;
- Frequent fainting;
- Dizziness;
- Difficulty breathing;
- Pain in the heart area;
- Arrhythmic heartbeat.
Most often, cardiac hypertrophy in the left atrium is associated with heredity.
In addition, the reasons for its development are:
- Disturbances in the functioning of the mitral valve: more often its stenosis leads to the development of hypertrophy, less often – insufficiency;
- Hypertrophic cardiomyopathy;
- Arterial hypertension;
- Excess weight;
- Aortic stenosis;
- Myocarditis.
Symptoms of left atrium enlargement usually appear at later stages of pathology development and are characterized by such manifestations.
- Decreased endurance for physical activity, including everyday activities: walking, running, swimming.
- Rapid onset of general fatigue.
- Chest pain.
- Difficulty breathing.
- Attacks of shortness of breath.
- Cardiopalmus.
Venous blood from the organs and systems of the whole body flows into the cavity of the right atrium, and from it through the right ventricle it is sent to the lungs to be enriched with oxygen there. The main reasons that cause hypertrophic changes in the right atrium (RA) are associated with lung pathology.
- Diseases of the respiratory system: COPD (chronic obstructive pulmonary disease), obstructive or regular bronchitis, pulmonary hypertension, etc.
- Pathology of the tricuspid valve: its stenosis or insufficiency.
- Pulmonary thromboembolism: an acute situation of blockage of a pulmonary vessel by thrombotic masses.
- Congenital heart anomalies: tetralogy of Fallot, atrial septal defect.
In most cases, manifestations of right atrial hypertrophy are directly related to the pathology that caused it.
In severe cases, when the reserve capacity of the right atrium is depleted, pulmonary symptoms and a group of symptoms associated with congestion in the systemic circulation appear.
Signs from the respiratory system:
- Cough, mainly at night;
- Hemoptysis;
- Shortness of breath during normal activities or at rest;
- Difficulty breathing.
Signs associated with right atrium decompensation:
- Swelling of the extremities;
- Increased belly size;
- Dull pain under the right hypochondrium (liver enlargement);
- The appearance of a venous network on the anterior surface of the abdomen.
The patient's subjective complaints are usually non-specific and uninformative.
An objective examination, including mainly auscultation of the heart, can reveal murmurs at different points depending on the underlying pathology. Also, by listening, you can detect irregularity of tones, which indirectly indicates the presence of a complication of cardiac muscle hypertrophy.
Instrumental methods include electrocardiography and ultrasound of the heart (echocardiography).
Thus, ECHO-CG can serve as the best diagnostic method, since it allows not only to identify hypertrophy, but often also to determine the cause that led to its development: heart disease, valve pathology, etc.
Treatment of cardiac hypertrophy should be approached differentiated depending on age, underlying cause, presence of concomitant diseases and other factors.
After a set of examinations, the cardiologist will be able to prescribe adequate treatment, which includes non-drug methods (correction of lifestyle, nutrition, etc.) and medications (vasodilators, antihypertensives, etc.) that need to be taken for a long time.
Hypertrophy of the heart is an increase in the thickness of the heart muscle (myocardium), associated with an increase in the number of muscle fibers. Causes of hypertrophy of parts of the heart: most often, hypertrophy appears due to increased load on any part of the heart or when it is difficult to eject blood into the main vessels. Thus, hypertrophy of the heart parts occurs: 1) with congenital and acquired heart defects - hypertrophy of the corresponding parts of the atria and ventricles; 2) with hypertension and other hypertension (for example, with renal hypertension), when left ventricular hypertrophy develops; 3) in athletes during intense physical activity, hypertrophy of the left and sometimes the right ventricle is possible; 4) in coronary heart disease, hypertrophy develops as compensation for the reduced function of individual areas of the myocardium; 5) with hypertrophic cardiomyopathy; 6) with cor pulmonale, hypertrophy of the right ventricle develops; 7) hypertrophy is possible with various other diseases, metabolic disorders, in particular with obesity.
Symptoms. Cardiac hypertrophy has no specific symptoms. The symptoms are caused by the underlying disease, which leads to the development of hypertrophy of the heart.
Development. The development of hypertrophy of the heart can lead to disruption of normal metabolism in the myocardium and disruption of the supply of oxygen to myocardial cells. Therefore, hypertrophy contributes to the development of rhythm disturbances (see arrhythmias), the appearance of pain in the heart, and subsequently - manifestations of heart failure.
Diagnostics. Diagnosis of cardiac hypertrophy is based on data from electrocardiography, x-ray examination of the heart, and echocardiography.
The blood entering the left atrium, and then the left ventricle, is oversaturated with oxygen, as it comes directly from the lungs. From the right ventricle, blood is distributed throughout the body.
Often, the causes of left atrial hypertrophy are associated with genetic changes, as a result of which it can be inherited. In addition, the development of hypertrophy can be caused by high blood pressure. There are other reasons due to which hypertrophy of the walls of the left ventricle develops:
- Obesity. It is worth noting that in recent years, obesity has been the leading cause of the development of cardiac hypertrophy in young patients. According to recent studies, a patient suffering from obesity already in childhood is at risk of heart pathologies.
- Hypertrophic cardiomyopathy. During the development of this disease, excessive thickening of the walls of the cardiac ventricles is observed. As a result, the heart is under constant tension, since in order to function normally it must contract more actively. Constant excessive loads lead to an increase in the size of the left atrium. Hypertensive cardiomyopathy occurs due to genetic predisposition.
- Lung diseases. The presence of any lung diseases, no matter what causes their occurrence, significantly reduces the functionality of the organ, thereby causing the development of atrial hypertrophy.
- Malfunction of the mitral valve. This valve is located in the heart, allowing blood to move from the atrium to the ventricle. The valve opens only after a certain volume of blood fills the left atrium and closes after the blood moves into the ventricle. Two types of disorders can be associated with this valve: stenosis and insufficiency. With stenosis, the lumen between the parts of the heart, with hypertrophy of the heart muscle, is greatly narrowed, and the atrium works more intensely to pump a sufficient volume of blood into the ventricle. If there is insufficiency, the valve does not close completely, which leads to free movement of blood in the opposite direction. Insufficiency can lead to inflammation of the atrium.
- Aortic stenosis. In this case, we are talking about the malfunction of the aortic valve. The aorta connects to the ventricle, and it is through it that blood flows out. If the opening between the heart and the aorta is too narrow, the heart has to work harder to push blood through. When the valve narrows, the heart is unable to remove the required amount of blood, and the atrium suffers greatly.
- An increase in blood pressure can also trigger the development of cardiac hypertrophy. Thanks to blood pressure, blood circulates normally throughout the body. When it increases, the load on the heart increases many times over.
- A stressful state in which a person remains for a long time can also provoke changes in the heart.
The degree of manifestation of symptoms depends entirely on the stage of the syndrome, or more precisely on how enlarged the heart is. With a significant increase in the organ, a person will constantly feel discomfort, and with minor changes, even indirect signs of left ventricular hypertrophy may be completely absent. Symptoms characteristic of the syndrome are:
- difficulty breathing;
- painful sensations in the chest;
- excessive fatigue;
- change in heart rate.
If a person suffers from such a syndrome, it is extremely difficult for him to engage in active sports, and if overexerted, severe shortness of breath may occur.
Constantly increased pressure can provoke the development of ventricular hypertrophy, as a result of which the heart works much more actively. Due to the excessive amount of blood in the heart, its walls increase in size, which leads to a complete loss of elasticity and further inability to work in the desired mode.
It should be noted that the reasons for the enlargement of the ventricle and atrium are similar, since these organs work in pairs. The main reasons are:
- Increased blood pressure.
- Hypertensive cardiomyopathy, in which there is excessive growth of the heart muscle.
- Aortic valve stenosis.
- Cardiac hypertrophy in athletes. With constant training, the heart works harder. To cope with constant stress, the organ adapts and begins to increase in size. Heart problems can be avoided only with a properly structured training system and constant monitoring of its condition. If you do not approach this issue responsibly, a heart attack may occur.
- Due to obesity, the body requires more oxygen, which provokes the development of hypertrophy.
- Pregnancy. Left ventricular hypertrophy during pregnancy occurs quite rarely. The reason for its development lies in the additional stress that the mother’s body experiences. The heart has to work more intensely in order to ensure sufficient blood circulation and oxygen saturation of the fetus. Patients who already have any heart disease are susceptible to the development of hypertrophy.
Initial left ventricular hypertrophy may occur unnoticed by the patient. Obvious symptoms of the disease appear in later stages. These include:
- pain in the sternum;
- shortness of breath;
- the appearance of fainting;
- too fast heartbeat;
- dizziness;
- increased fatigue.
Through the left ventricle, the heart is connected to the entire circulatory system, through which oxygen supplies all organs and tissues. It is for this reason that its excessive growth can provoke the occurrence of extremely severe complications, such as:
- Arrhythmia.
- Heart failure. In the presence of this disease, the heart cannot cope with pumping the volume of blood necessary for the normal functioning of the body.
- Heart attack.
- Ischemic disease, in which the heart does not receive enough oxygen.
- Heart failure.
Left ventricular hypertrophy of the 1st degree can be detected during regular examinations by a cardiologist, since only in dynamics it becomes possible to diagnose such changes. By identifying changes at an early stage, severe consequences can be avoided.
Minor left ventricular hypertrophy, detected at an early stage, can be treated quite successfully. When this syndrome is detected, it is necessary to identify the cause of its occurrence. If the cause of hypertrophy is a heart defect, surgical intervention is necessary. In addition, treatment should consist of slowing down the hypertrophy process as much as possible.
In some cases, hypertrophy may be the result of an incorrect, sedentary lifestyle of the patient. In such a situation, radical therapy is not required. To improve your health, you need to introduce small physical activities and adjust your diet. The diet should include a large number of foods containing vitamins, magnesium, omega, calcium and potassium. These substances have a positive effect on the heart muscles, making them more elastic. Swimming, aerobics or running are excellent for physical activity.
Drugs for left ventricular hypertrophy are indicated for use regardless of the cause of its development. They help restore normal nutrition to the heart muscle. Necessary medications include an antiarrhythmic drug, for example, Verapamil, as well as beta-blockers. While taking these medications, you should abstain from alcohol. In most cases, taking such drugs is necessary throughout the patient's life. Additional drugs, due to which in some cases regression of left ventricular hypertrophy is observed, are Ramipril and Enalapril.
You should get rid of bad habits, such as smoking, as nicotine significantly reduces the level of oxygen in the blood, which leads to insufficient nutrition of the heart and further development of the disease.
Living with a diagnosis
The level of activity and work capacity of patients depends on the underlying disease that led to left ventricular hypertrophy. If blood pressure is slightly elevated or is corrected with antihypertensive drugs, and there are no complications, then there is no reason to limit work activity.
In the event of an acute disorder of cerebral or coronary circulation, or severe heart failure, working patients with hypertrophy are referred to an expert commission to determine the disability group. A decision may be made regarding partial or total disability.
If the deterioration of the condition is temporary, there is no permanent loss of vital functions, then treatment is carried out in a hospital setting, and the patient is issued a sick leave certificate. After normalization of blood circulation, he can continue to work in his specialty.