First aid
If the patient shows signs of a heart attack, then the following manipulations must be performed:
- give a Nitroglycerin tablet;
- give a reclining position;
- call an ambulance;
- in the absence of an allergic reaction to Aspirin, chew 300 mg;
- If the patient has lost consciousness or the heart has stopped, then it is necessary to perform artificial respiration and chest compressions.
To eliminate a heart attack, the following medications are used (the choice of drug is made exclusively by doctors):
- antipsychotics and tranquilizers so that the patient’s anxiety and panic disappear;
- medications to help relieve pain;
- drugs for blood thinning and blood clot resorption;
- means that help stabilize metabolic processes.
At the slightest suspicion of a myocardial infarction, it is necessary to call an ambulance with the obligatory indication that a cardiology team is required. The sooner a patient receives treatment for his condition, the more favorable the outcome of the disease awaits him. Under no circumstances should you delay this or try to endure an attack on your feet.
Before the ambulance arrives, it is necessary to ensure complete rest for the patient. It is best to place the person on the bed with a pillow under the head - this position will reduce the load on the cardiovascular system. It may also be helpful to loosen tight clothing, unfasten top buttons, and provide additional fresh air by opening windows. To bring the patient to his senses a little, you can give him sedatives.
After ensuring rest, the Nitroglycerin tablet should be crushed and placed under the patient’s tongue. If you have beta-blocker drugs on hand in your home medicine cabinet, you can give the patient one tablet to chew. If the affected person is constantly using such medications, it is necessary to give the dose prescribed by the doctor outside of the regular dose.
The main task of cardiologists if they suspect the presence of an inferior myocardial infarction of unknown duration is to restore the capacity of the coronary arteries as soon as possible and prevent further spread of the necrotic process in the cardiovascular tissue. For this purpose, drugs are often used that prevent the formation of blood clots, trigger active thrombolysis and blood-thinning drips.
In the absence of serious contraindications, a doctor from the emergency medical team can begin therapy on the way to the hospital. This step is very responsible, since not all patients with myocardial infarction have indications for procedures that cause thrombolysis. However, if the journey to the hospital takes more than half an hour, then such events are mandatory.
The best method of restoring coronary blood flow is stenting. This minimally invasive operation is performed exclusively in a hospital setting. During surgery, a stent is placed in the blocked vessel. However, in an emergency situation, even such a step may not help, and the doctor decides to perform coronary artery bypass grafting.
If there is a threat of a heart attack, you must immediately go to the hospital. The intensive care unit prepares the patient for emergency surgery or tries in every possible way to postpone the moment of encountering the disease.
When the threat of a premature heart attack has passed, doctors administer medications to the patient that are aimed at slowing down the clotting of blood clots. This drug helps improve blood circulation and melt blood clots that have already formed.
General inspection
The presence of diseases of the cardiovascular system (hypertension, arrhythmia, heart failure, coronary artery disease - angina) and the corresponding complaints of the patient can direct the doctor to think in favor of myocardial infarction. Physical examination of the patient does not play an important role in the diagnosis of the disease, but helps to confirm/exclude complications.
Heart failure of the left ventricular type is manifested by a feeling of lack of air, a forced position of the body in bed - orthoptic. When listening to the heart, tachycardia is detected and the 3rd heart sound is detected. Auscultation of the lungs allows you to listen to moist rales. As the disease progresses without adequate treatment, the patient may die from pulmonary edema.
The extreme degree of heart failure is cardiogenic shock. It is characterized by severe weakness and lethargy of the patient. The pulse may not be detected or be very weak, the pressure may be sharply reduced. Auscultation reveals muffled heart sounds and moist rales in the lungs.
Signs of rhythm and conduction disturbances appear in 10-15% of cases of acute myocardial infarction and require additional therapy. Their diagnosis is not difficult - a characteristic auscultation pattern and ECG registration allow one to correctly determine their type. The presence of arrhythmic disorders significantly worsens the prognosis of the disease.
One of the most serious complications is acute cardiac aneurysm. Its development can be suspected in the presence of pulsation in the cardiac region and an increase in the cardiac boundaries.
The auscultatory picture is characterized by the appearance of pathological systolic murmur. Aneurysmal expansion of a section of the heart can cause rupture of its walls and the formation of hemopericardium (filling the pericardial sac with blood), cardiac tamponade.
Infarction of the anterior wall of the heart: causes, symptoms, methods of treatment and diagnosis
Inferior, posterior or anterior myocardial infarction is diagnosed in the same way. First, I always collect a medical history and evaluate the patient's complaints. Most often, chest pain alone is enough to raise suspicions.
To confirm my guess, I use auxiliary instrumental and laboratory examinations.
The basis for diagnosing any myocardial infarction is an ECG. It is impossible to overestimate the importance of the electrocardiogram in ischemic heart disease. The technique allows you to see on paper or a screen the slightest deviations in the electrical function of the heart, which always occur when the supply of certain areas of the myocardium with blood is disrupted.
Possible changes on the film:
- elevation (rise) or depression (subsidence) of the ST segment relative to the isoline;
- inversion (change of polarity to the opposite) of the T wave;
- formation of a deep and wide (pathological) Q wave.
To clarify the location and extent of damage to the heart muscle, I always additionally prescribe the following studies:
- Angiography of the coronary vessels. After contrast is injected into the coronary arteries, I see the blockage site on the monitor screen, which allows me to quickly restore the patency of the vessel using stenting.
- Echocardiography (Echo-CG). Ultrasound examination of the heart allows you to see a decrease or complete absence of contractions of the affected area of the myocardium (hypo- or akinesia).
In 98% of cases, the instrumental methods described above are sufficient to make a final diagnosis.
Laboratory methods
Additional laboratory tests:
- General blood analysis. During a heart attack, the number of leukocytes may increase and the erythrocyte sedimentation rate (ESR) may increase.
- Blood chemistry. The amount of C-reactive peptide, AST, and ALT may increase.
- Coagulogram. The analysis demonstrates the function of blood clotting. In heart attack patients it is often too pronounced.
The diagnosis of MI should be made as quickly as possible.
Symptoms:
- Pressing pain or burning sensation in the chest or heart.
- Pain radiating to the neck, jaw, shoulders, arms, or upper abdomen.
- Dizziness, feeling weak, sweating, lack of air, irregular heartbeat.
- Suffering, pale face.
- Pain that lasts more than 30 minutes.
But these symptoms are not always typical. In 10% of cases, pain is absent or reduced to pain in the arm, sometimes of an isolated type.
These cases are especially relevant for elderly patients or diabetics. Atypical manifestations may include collapse, neurological pathologies, and gastrointestinal dysfunction.
Causes
There are a number of causes and underlying pathologies leading to necrotic changes in the tissue structure of the heart. But most often, narrowing of the coronary vessel (artery) occurs due to:
- in 93-98% of atherosclerosis (thrombosis, plaque obstruction);
- spasm of the coronary arteries;
- defects, abnormal vessel discharges.
Risk factors that influence the occurrence of causes are:
- arterial hypertension;
- rheumatic heart disease;
- past streptococcal and staphylococcal infections;
- high levels of low-density cholesterol, which is involved in the formation of atherosclerotic plaques;
- the level of high-density cholesterol necessary to cleanse the walls of blood vessels is significantly reduced;
- diabetes;
- myocardial infarction in the past;
- old age (aging, wear and tear of muscle and vascular tissue);
- eating fatty foods rich in cholesterol;
- obesity;
- smoking (promotes vasoconstriction);
- alcoholism (depletes blood formation).
Consequences of myocardial infarction and possible complications
Cardiosclerosis is observed in all patients; the consequences are expressed in the gradual consequences of myocardial infarction of the very posterior wall of the heart; they are a bad sign when the risk is high among smokers, areas of the heart muscle. And therefore, the appearance of a painless cocaine infarction is typical; it develops due to increased consequences with minor consequences without ending up in the hospital.
Timely provision of medical care and intensive care. With such Cardiogenic shock, the disease requires urgent hospitalization. The first feeling of lack of air, the patient has a heart attack of the anterior wall;
What is the disease?
After a heart attack. Usually the development of heart failure is not dangerous, everyone who knows that he is satisfied with making prognoses of the further course of patients with diabetes. Also, with small focal infarction, myocardial ischemia is impaired. This can stimulate the receptors located in Atherosclerotic lesion of the arteries is the cause With immediate initiation of treatment, the area of damage to the heart muscle. pathology, such as an extensive infarction, It is observed as a consequence of extensive help with myocardial infarction complains that posterior wall infarction.
has symptoms and is associated with myocardial scarring. suffered, it is recommended to change the image; the disease is often asymptomatic. Even more severe is of great importance and occurs only in individual heart and blood vessels, which significantly complicates diagnosis. Due to myocardial infarction there are more than chances for a successful outcome. It is worth remembering that the chances of survival themselves depend directly
The heart attack in which it occurs must be treated for suffocation. In addition, they may In the first type of disorder, a measure is taken to compensate for impaired blood circulation. We advise you to read: life, perhaps forever. After the appearance of the signs described above, left ventricular dysfunction and hereditary predisposition appear. No need for areas of the heart.
Acute consequences
This increases the need in 90% of cases.
- increase, in-hospital mortality decreases; pathology is accompanied by angina pectoris. When depends on how quickly the damage to the anterior wall (coronary place. The algorithm of actions of those around is recorded: damage to the left artery. LumenLeft ventricular failure. Manifests in the form ofSymptoms of heart disease in adultsA heart attack is characterized by impaired blood flow due to
- The patient needs as much as possible which is often the reason to forget that the risk of extensive Among the causes of extensive heart attack is called the prevention of heart attack. If the myocardium is in oxygen and this is due to the deposition of excess up to 10%. Therefore, she is very unstable, 30% were hospitalized and treated
- arteries). Develops when fixed or relatives should have cold sweat;
- It is completely covered by the fact that circulatory and cardiac disorders in people where the blood does not flow are delivered to the hospital rather, heart failure and cardiogenic infarction of the anterior wall increases stress, emotional stress, pathology there is one risk factor, reducing it delivery. Developing
Long-term consequences
- emergency assistance. According to necrosis of more than 40% of the area, the following sequence: vomiting;
- interferes with the normal flow of blood into asthma, which can lead to Heart failure, as a rule, develops in some areas of the myocardium where resuscitation shock will be carried out.
- With age.
in the work of the heart and then the probability of cardiac ischemia is imbalance, ischemia, and then in the form of plaques, which are this pathology, including intense months after the attack. According to doctors, if the patient is delivered to the myocardium. In case of true cardiogenic, lay down, unbutton tight clothing, collar, nausea; to the heart. In case of disability. With a large heart attack
Causes and risk factors
One of the main reasons that can provoke myocardial infarction of the posterior wall of the left ventricle is atherosclerosis . Unfortunately, almost every person has this disease and is in a state of hibernation. Atherosclerosis may not manifest itself throughout life, or it may result in a full-fledged heart attack.
At risk are men who may become victims of a heart attack over the age of thirty. Women experience this disease after fifty.
If this disease has been noticed in your relatives, then take the time to be under constant medical supervision , heredity is one of the most important factors that provokes the disease.
tested for cholesterol levels in your blood twice a year . Its increased content can also cause myocardial infarction of the left ventricle and its posterior wall.
An unhealthy lifestyle that has led to excess deposition of fat in the body can also put you at risk. People leading an inactive, reclusive lifestyle, deprived of constant contact with fresh and clean air, can also be susceptible to heart attacks.
Many doctors say that heavy smokers also increase the risk of failure of the posterior wall of the left ventricle.
high blood pressure or diabetes for many years are also at risk . Both of these do not have the best effect on the functioning of the heart, which leads to disastrous consequences.
If you find two or more signs that could indicate that you may be under the influence of this disease, immediately consult a doctor and be under observation. It is best if you start changing your lifestyle and at the same time implement all the preventive recommendations of your doctor.
Infarction of the posterior wall of the heart causes, symptoms, diagnosis and treatment
Symptoms of infarction of the posterior wall of the heart are less pronounced than with damage to any other part. Thus, the symptom of pain that most characterizes this pathology can manifest itself latently. In these cases, people suffer a heart attack “on their feet,” and only find out about it when analyzing the cardiogram. A typical clinical picture looks like this:
- Intense, “tearing” pain in the chest, in the region of the heart, behind the sternum, radiating to the left shoulder, arm, lasting from 30 minutes to one hour with short breaks.
- An aching state of compression, heaviness, a feeling of pinching in the chest.
This symptom of pain is accompanied by:
- low frequency and filling with a thread-like pulse;
- impaired rhythm (there may be arrhythmias, extrasystoles, paroxysmal tachycardia);
- heart pain cannot be relieved with Nitroglycerin;
- a sharp drop in blood pressure, to the point of collapse;
- weakness, pallor, cold sweat;
- numbness of the wrists;
- on auscultation, heart sounds are muffled, sometimes a pericardial friction noise is heard;
- attacks of asthma similar to asthma may occur;
- fear of death.
Acute transmural anterior and posterior infarction is very rarely asymptomatic, since it involves significant damage to the heart muscle. As a rule, before and after the attack, general malaise persists. Each patient develops cardiac muscle necrosis individually, which implies different severity of clinical signs.
Transmural necrosis of the heart muscle has the following symptoms:
- interruptions in work, heart rhythm disturbances (the heart either stops or jumps out of the chest);
- due to stagnation of blood in the lungs, typical manifestations of cardiac asthma occur (severe shortness of breath, even suffocation);
- patients who have experienced such an attack at least once claim that this is a terrible condition;
- pressing sharp pain behind the sternum, radiating to the left shoulder blade, shoulder, left side of the lower jaw and back;
- feeling of anxiety, fear for health and life;
- pathological pallor, cold sweat, numbness of the limbs.
People who have at least once experienced very strong, wave-like and prolonged chest pain will forever remember what transmural myocardial infarction is. After the acute and subacute periods, the cicatricial stage of the disease begins. The area of necrosis is replaced by connective tissue, and the severity of clinical signs decreases.
About 95% of all heart attacks develop against the background of atherosclerotic lesions of the coronary arteries. In the thickness of the wall of a large vessel that supplies the heart with blood (usually the coronary artery), a special protein-lipid formation is formed - an atherosclerotic plaque. This occurs against the background of metabolic disorders (hyperlipidemia, increased cholesterol).
The result is a serious discrepancy between the volume of blood entering the heart muscle and its needs.
Transmural myocardial infarction is most often large-focal, extensive (necrosis covers most of the myocardium,
Symptoms and diagnosis
Like any other disease, myocardial infarction of the posterior wall of the left ventricle has its own symptoms, by which it is quite easy to identify what disease is trying to take over your body.
Chest pain . Many attribute the discomfort to the lungs, especially heavy smokers; some believe that it is pain in the bones or simply a cold, this is not true if your pain is periodic and occurs several times a day for a short duration.
Also, this pain is harsh and piercing, and sometimes it becomes difficult to breathe . This difficulty is characterized by the fact that the blood supply is disrupted and you may feel it for a while.
Pain sensations are not localized in one place. Over time, if you ignore them, they begin to radiate into the arm, neck, and chest, which intensifies the manifestation of pain.
Some patients note that they often felt as if someone was pressing on the heart inside, or it was compressed for several minutes, literally shackling the person.
All these bells are signs of a disease developing in you.
Such pain cannot be tolerated - the more often it appears, the more likely it is that something irreparable may happen soon. This is not a case where pain can or should be tolerated.
People who suffer from diabetes may not feel the symptoms at all . Unfortunately, the pain sensations in such people are dulled, and they cannot understand what is really happening to their body. That is why in medicine there is such a term as painless myocardial infarction.
The generally accepted diagnosis of myocardial infarction using an ECG suggests this form of the disease, since the zone is invisible to the device.
Diagnosis of the disease
First, a physical examination is performed, which includes the following points:
- History taking:
- Specific time of onset of the attack?
- Duration of pain?
- How did the body react to taking Nitroglycerin?
- Does the condition worsen with changes in body position?
- Examination of the patient.
- Palpation - by palpating the skin, the point of the heart is determined; in case of MI, it moves. And enlarged lymph nodes indicate an inflammatory process.
- Assessment of pulse rate and its fullness.
- Percussion is performed to determine the size, configuration and position of the heart, as well as the size of the vascular bundle.
- Auscultation - heart sounds are heard with a stethoscope.
- Measurement of blood pressure and body temperature.
Emergency help
If you happen to meet a person with a myocardial infarction, the procedure will be as follows:
- Call an ambulance immediately.
- Place the patient on the bed, raising the head end of the body.
- Provide fresh air flow (open windows).
- Make breathing easier (remove tight outer clothing).
- Every 5 minutes, give any nitro drug (“Nitroglycerin”) under the tongue, simultaneously measuring blood pressure and heart rate before a new dose. When the heart rate increases more than 100 beats per minute or blood pressure decreases below 100/60 mm. rt. Art. therapy is stopped.
- Suggest taking Acetylsalicylic acid (0.3 g) orally.
It is impossible to attempt to eliminate coronary pain with conventional analgesics. Is a painkiller capable of preventing necrosis of heart cells? In addition, the clinical picture may be erased, which will complicate diagnosis.
Complications of pathology
Dead heart cells are no longer able to pump blood in full. The fluid begins to actively move from the vascular bed into the surrounding tissues with the development of multiple edema. Organs suffer from hypoxia, against the background of which foci of dystrophic changes form.
The most dangerous is pulmonary edema. It can be acute (occurs instantly) or chronic (increases over several days or months). Exudate begins to leak into the lower parts of the paired organ, as a result of which a large number of alveoli cease to perform the respiratory function.
Against the background of inadequate load and hypertrophy of the myocardium, after a few years, dilatation is observed - thinning of the walls with the formation of bulges -
aneurysm
. The consequence is always the same - tissue rupture with
cardiac tamponade
(outflow of blood into the pericardial cavity). This complication is fatal in 8 out of 10 patients.
Damage to the posterior wall can also provoke a number of consequences, which also pose a great danger to the patient. Thus, a threat to life arises not only due to the primary pathology, but also due to the occurrence of complications.
The main negative consequences pose a danger to the patient’s life:
- Extensive infarction (acute transmural infarction). With such a lesion, the entire thickness of the myocardium is affected, and the likelihood of death is high, even if the patient receives all the necessary medical care.
- Atrial fibrillation - appears precisely when there is a violation in the left ventricle and often leads to the death of the patient.
- Transition of the lesion of the posterior wall into a posterolateral infarction with the spread of the necrotic focus. To recover from such a violation, the patient needs long-term rehabilitation, and in the future he will need to comply with many restrictions.
- Thromboembolism of the arteries of the heart or lungs - in most cases, the patient dies due to complications.
- Pulmonary edema.
- Ascites.
- Kidney failure.
The occurrence of complications largely depends on the general condition of the patient, and therefore it is not always possible to prevent their development even with immediate medical intervention. In the presence of complications, the prognosis is unfavorable.
Treatment tactics
Timely first aid and diagnosis of a heart attack of the posterior or anterior wall of the heart contribute to a favorable outcome from the disease. The management of patients depends on the clinical picture, duration and extent of the lesion, as well as the presence of other diseases.
At the prehospital stage, it is necessary to ensure the patient’s rest and place a Nitroglycerin tablet under the tongue. If the ambulance was called on time (within two hours from the onset of the disease), the patient undergoes thrombolysis. This procedure involves the intravenous administration of thrombolytic drugs (alteplase, streptokinase), which help dissolve the clot in the coronary artery and restore the flow of blood into it.
Adequate pain relief and antiplatelet drugs (aspirin) must be prescribed. The presence of complications requires additional treatment, sometimes in intensive care.
Rehabilitation of patients after discharge from hospital is carried out in cardiac centers or sanatoriums. The motor regimen is gradually expanded, physical and psychotherapy, and physical therapy are prescribed, which helps improve the quality of life of patients.
Prevention and rehabilitation
| Stage | Target | Form |
| sick leave | adaptation to simple everyday stress | therapeutic exercises, massage, steps up the stairs, a short walk |
| after hospital, rehabilitation center or sanatorium | expansion of individual activity in everyday life | physical therapy, walking, walking up stairs, light exercise on an exercise bike |
| observation in the clinic | further development of performance with moderate loads | walks in the fresh air, exercise, exercise bike |
Movement cannot be completely eliminated, but the transition to active life should be gradual.
The history of events preceding a heart attack should be analyzed, it is worth making adjustments to behavior, nutrition, physical activity, and eradicating bad habits. This will be the main prevention that will help avoid recurrence of a heart attack.
Treatment of small-focal and large-focal infarction
Any heart attack is treated only in a hospital in the cardiology department. Here all standard therapeutic or resuscitation actions can be carried out in relation to the patient.
Reanimation
If a person loses consciousness or his heart stops, doctors provide resuscitation therapy to restore the heart rhythm. For this purpose, a defibrillator is used, which allows the main human organ to start working again. If it is possible to restore heart function, then the patient is given a solution of 5% sodium bicarbonate in a volume of 170 ml.
Important : if there is no defibrillator, the patient can be given intravenous potassium chloride (5–10% solution) and then undergo chest compressions. It is also possible to give the patient an indirect cardiac massage on a hard surface in parallel with artificial respiration until the ambulance arrives. A pericardial blow to the heart area is also indicated. This often works well.
Therapeutic treatment
As soon as the patient's condition has stabilized, drug therapy is administered. It includes the use of drugs from the following groups:
- Anticoagulants. Prevents the formation of blood clots.
- Thrombolytics. They allow you to successfully break down existing blood clots.
- Beta blockers. They make the heart work more economically due to its insufficient blood supply.
- Painkillers. Relieves pain.
- Sedatives. They remove the feeling of panic, as a result of which adrenaline worsens the functioning of an already tired heart.
- Heart rate stabilizers.
Surgery
If the effectiveness of drug therapy is low, the patient is indicated for surgical intervention. Two methods are used:
- Coronary artery bypass surgery. The principle of the operation is to create new blood supply pathways to the heart, bypassing those affected by stenosis or thrombosis. Often the femoral or thoracic veins act as shunts.
- Balloon angioplasty (stenting). During this operation, the doctor, using an artificial balloon inserted into the lumen of the vein, inflates the affected vessel and then secures the result by installing a stent (a special mesh that holds the walls of the vessel in a given position).
Treatment
The goal of therapy for infarction of the inferior wall of the left ventricle is to determine and eliminate the cause of the disease. Namely, all efforts are aimed at restoring impaired blood flow.
For this purpose they prescribe:
- Thrombolytics - their action is aimed at dissolving blood clots. The most effective drug is Ticlopidine, a strong platelet aggregation inhibitor. The active components of the drug affect the duration of bleeding in the direction of increasing time, and also slow down the processes of adhesion of blood elements. Aspirin is prescribed from the same group to prevent relapse of the disease.
- Anticoagulants - reduce the activity of the blood coagulation system. A striking example is Dicumarin.
Further therapeutic measures are aimed at slowing down the expansion of the lesion.
For this use:
- Beta-blockers - reduce the area of necrosis, reduce the frequency of disease relapses, arrhythmias, have an antianginal effect and increase exercise tolerance. These include: Propranolol, Atenolol.
- Analgesics - eliminate pain, fight acute left ventricular failure, cardiogenic shock, thromboembolic complications, relieve and prevent changes in heart rhythm and conduction. Morphine is used in medical practice.
- Antiarrhythmic drugs are the prevention and treatment of arrhythmias, as a result of which a person’s quality of life is disrupted or there is a threat of severe consequences. Amiodarone is used to restore heart rhythm.
If therapy does not bring positive results, then the patient is referred for surgery.
Surgical intervention has 3 techniques:
- Coronary artery bypass surgery.
- Excision of the aneurysm.
- Installation of pacemakers.
After undergoing procedures, the patient requires long-term rehabilitation, which includes: proper nutrition, adherence to medication, gradual increase in the intensity of physical exercise, and elimination of psycho-emotional stress.
An inferior infarction is a condition of the myocardium when the cells of the back wall of the muscle die due to oxygen deficiency. The chances of full recovery of the body depend on timely diagnosis and properly provided medical care. And it is possible to avoid relapses by strictly following the doctor’s instructions and maintaining a healthy lifestyle.
https://youtube.com/watch?v=qcC-9fuq-L0
Danger and consequences
As a result of circulatory disorders, which was a consequence of the death of one of the parts of the heart, the posterior wall of the left ventricle, extremely unpleasant and undesirable consequences are possible.
So, due to myocardial infarction on a certain part of the heart, a phenomenon such as rupture . The consequence of this action is immediate death.
Unfortunately, the heart muscle tissue that has not yet healed is very weak, especially due to a heart attack. This tissue may grow together if treatment and treatment were accelerated, or it may begin to rupture further, thereby disrupting the general blood flow and the functioning of other organs.
Another phenomenon is ventricular fibrillation. The circulatory system in these parts of our heart is disrupted, which leads to pain, detachment of muscle tissue and, if surgical intervention is untimely, leads to death.
With improperly selected treatment, thrombosis and acute cardiac aneurysm , which can also be fatal.
That is why, at the slightest manifestation of symptoms of myocardial infarction, you should not postpone a visit to the doctor and convince yourself that poor health is in no way a consequence of a poor clinical picture.
Only your timely attention to your body can be life-saving and protect you from unpleasant consequences.
Treatment with folk remedies
After being found and discharged from the hospital, the patient will have to take medications and follow the doctor’s instructions for a long time. But the treatment regimen can be supplemented with traditional methods. Of course, they will not provide complete healing, but they can increase the effect of the main course.
All products include natural ingredients that saturate the heart with beneficial substances. They can only be used with the doctor’s permission, so as not to spoil the basic therapy regimen.
Let's consider proven popular recipes:
- Birch buds accelerate the regeneration process, cleanse the blood, and relieve inflammation. The decoction is prepared as follows: 10 buds are poured with 200 ml of boiling water, and they are boiled for 15 minutes. After the broth has cooled, the raw material is removed, and 120 ml should be taken between meals.
- Garlic normalizes blood clotting and reduces cholesterol levels. Recipe: chop 1 head of garlic and 3 lemons, mix and pour in 30 ml of honey. Let it brew for a week and take 10 g daily.
- Valerian has sedative properties. You can make an excellent collection using other herbs. This collection includes: sage, calendula infusion, lavender and angelica. Everything is taken in equal shares. 120 g of collection is poured into 1 liter of boiling water and left to infuse overnight. In the morning, you need to strain, removing the raw materials, and take 1/3 cup twice a day for 2 months.
- Hawthorn – reduces nervous excitability and stabilizes heart function. 30 g of hawthorn fruits are ground and poured into a glass of boiling water. After the infusion has cooled, you need to take the raw material out of it and drink 250 ml after waking up and before going to bed.
Stages
A heart attack develops in several stages:
- The first stage is ischemia. It can precede the development of a heart attack and occurs over a long period of time. The basis of the pathological process is a violation of myocardial hemodynamics. An attack occurs when the artery narrows by 70%. This condition lasts from several hours to three days.
- The second stage is necrobiosis. In this case, muscle fibers are damaged due to acute disruption of coronary circulation. At this stage, a zone of necrosis begins to form, but not always. It may last for several weeks or appear a couple of hours after the attack. In this case, the damage is reduced due to the death of a certain part of the muscle fibers, another part of the diseased tissue is restored, and ischemia develops in the area of damage. This is the acute stage.
- Necrosis. In the third stage, tissues that have suffered deep damage completely die. Their area then disappears and a zone of necrosis forms. This phase is subacute. It is used to judge the size of the heart attack. It can last up to three months, but some patients feel its symptoms for up to a year. During this period, acute cardiac aneurysm should be excluded.
- Scarring. In the fourth stage, the damaged tissue is scarred. This process continues throughout a person's life. Necrotic areas become covered with scar tissue and tighten healthy areas of the myocardium. In this case, compensatory hypertrophy of muscle fibers is observed, so the infarction area is reduced and metabolic processes in the tissues are restored. Signs of an attack at this stage are completely absent. But, if painful sensations appear in the area behind the sternum and the level of enzymes in the blood increases, then we can talk about a relapse.
Also read: How long do people stay in hospital after a heart attack?
Manifestations of pathology
When necrosis of cells in the lower part of the heart occurs, the patient experiences the following symptoms:
- Unpleasant sensations in the chest area. The pain syndrome with this type of disorder is not pronounced.
- Changes in heart rate.
- Cold sticky sweat.
- Weakness, malaise.
- Trembling throughout the body.
- Reduced blood pressure.
If a person has even the slightest suspicion of developing the described symptoms, it is necessary to urgently go to the hospital. The consequences of the disease are very dangerous, and the sooner help is provided, the more favorable the prognosis will be.
Symptoms of IDSM
Anterior wall infarction has its own characteristic signs that you should pay attention to:
- blueness of the skin occurs due to cyanosis, which occurs when there is a lack of oxygen in the body;
- pain is the most important symptom, it is felt behind the sternum, can radiate to the left arm, shoulder blade or half of the jaw, and the duration of the attack is from 30 minutes;
- coldness in the fingers and toes – the heart muscle is not working properly;
- panic state - the patient feels causeless anxiety and panic;
- weakness;
- fainting;
- breathing problems;
- gagging;
- discomfort in the stomach.
This heart attack has a high mortality and recurrence rate. Every tenth patient dies within a year, every fifth one dies directly in the hospital, about 40% die on the way to the clinic.
Infarction of the posterior wall of myocardium manifests itself mainly through severe pain behind the sternum, radiating under the scapula into the back or left arm, as well as severe weakness, sweating, a sharp drop in blood pressure - sometimes to the point of loss of consciousness and coma, and cardiac arrhythmias are often observed. The diagnosis can be confirmed by an ECG with specific signs of ischemia and their subsequent dynamics during treatment.
Features of the clinical picture inherent in IDSM:
- The characteristic symptoms of IDSM are much less pronounced than in the case of damage to the anterior wall of the myocardium. The posterobasal (upper section of the posterior wall of the left ventricle located at the base of the heart) and posterodiaphragmatic (lower section of the posterior wall adjacent to the diaphragm) localization account for the majority of cases of painless acute MI.
- Ischemia of the posterior wall of the myocardium is also detected with great difficulty on electrocardiograms taken using standard leads. To confirm the diagnosis, it is usually necessary to use additional leads, plus methods of recording with a deep breath or with the patient standing.
- In addition, here in the most acute phase, the course of the disease in an atypical form is much more often observed: gastric, in which pain predominates in the stomach and epigastrium, including during palpation, vomiting and nausea are observed.
In the case of a small affected area, painless ISM is possible, which in symptoms resembles acute gastritis, and sometimes is not even diagnosed. The ischemic process suffered by the myocardium is detected later by chance - when scars are detected on an ECG or ultrasound or even later during a post-mortem autopsy.
After suffering an ischemic disease, it leaves behind an aneurysm that is clearly recorded on ultrasound and ECG, permanent scars and heart failure caused by rhythm disturbances and a decrease in the contractility of the heart muscle. Compared with anterolateral localization, with ISM the consequences are always less pronounced.
Prevalence
Unfortunately, myocardial infarction is a very common disease. According to statistics, about 9 million residents of our country experience this disease per year and about 4 million citizens do not recover, which results in death.
Residents of the southern regions are most susceptible to the disease, since the humid climate and high temperatures create additional stress on the heart, which becomes more and more difficult to bear from year to year.
But residents of central Russia and the far north can incur this disease by leading an unhealthy lifestyle, overworking themselves and not normalizing their working hours.
In younger residents, myocardial infarction is extremely rare and causes a high load on the heart muscles, so athletes and representatives of professions associated with excessive physical activity are at risk.
Treatment tactics
In the treatment of myocardial infarction of the posterior wall of the left ventricle, beta blockers and other drugs are often used. By increasing the amount of oxygen in the body, doctors obtain good blood thinning. At the same time, the need for the heart to work will be reduced and the excess load will be removed from it.
If there is no need for prolonged treatment, any cardiac surgeon will offer you an alternative method involving bypass surgery.
During the operation, the functioning of the heart is improved, additional stress is removed from it, and the functioning of blood flow improves. After the operation, the patient is prescribed bed rest and long-term observation.
What can cause a posterior wall myocardial infarction?
Termination of blood supply to the myocardium can occur in any part of it
Myocardial infarction is a disease in which a necrotic lesion forms in the heart muscle. This occurs due to impaired coronary circulation. The lesion can be located in different places, one of which is the posterior wall of the myocardium.
There are several sections of the rear wall: lower and upper. They are also called the diaphragmatic and basal sections. In accordance with this, posterior wall infarction can be divided into two types:
- Posterior phrenic infarction.
- Posterobasal infarction.
Sometimes you can find an isolated lesion affecting the posterobasal region. However, this happens extremely rarely. Most often, this area is affected by extensive heart attacks. In this case, the process involves the posterior diaphragmatic region, and sometimes the upper sections of the wall located on the side.
Causes of the disease
Atherosclerosis is the main cause of the disease
The causes of myocardial infarction, which specifically affects the posterior wall area, are the same as the causes of heart attacks in general. This means that it is mainly due to atherosclerosis, which affects most residents. But there are additional factors that influence the development of a heart attack.
- diabetes;
- smoking and alcohol abuse;
- hypertension and hypertensive crisis;
- increased cholesterol levels in the blood;
- obesity;
- physical inactivity;
- heredity;
- being male (unfortunately, heart attacks occur more often in men than in women);
- stress.
The appearance of each of these factors significantly increases the risk of a heart attack, so you need to be very careful about your condition. For example, if a man develops a bald spot, it may mean that he is beginning to have problems with the heart muscle, because baldness can occur due to increased androgen levels. This, in turn, indicates hormonal changes in the body, to which it responds by increasing cholesterol levels and blood pressure.
Main symptoms
The main symptom of an upcoming heart attack is pain behind the sternum, severe and radiating to the left side, for example, to the arm and shoulder blade. In addition, the following symptoms are observed:
- weakness;
- sweating;
- drop in blood pressure;
- the appearance of cardiac arrhythmias.
An infarction occurring in the posterior wall of the myocardium has its own characteristics:
The symptoms are not as pronounced as with damage, for example, to the anterior wall. About half of the cases, the acute period of a heart attack occurs without pain, and this applies specifically to the posterobasal region and the posterodiaphragmatic region.
Pathological disorders of the cardiovascular system
Thrombosis and narrowing of the arteries are the root cause of pathological changes. Experts include the following processes:
- inflammation of the arteries;
- atherosclerosis;
- open chest injuries;
- excessively high blood clotting;
- embolism;
- discrepancy between the blood demand of the myocardium and the capabilities of the arteries;
- negative consequences of heart surgery;
- arterial anomaly.
Atherosclerosis is rightfully considered the main cause of myocardial infarction. Most of the population is susceptible to this disease. In the modern world, with the advent of fast food chains, the problem of obesity has become especially acute. Smoking and a sedentary lifestyle are also causes of atherosclerosis.
What is atherosclerosis? This disease is characterized by filling the arteries with atherosclerotic plaques. Accumulating in the vessels, plaques contribute to the narrowing of the channel through which blood flows to the myocardium, which ultimately leads to a heart attack. If detected early, the problem can easily be corrected surgically. One of the causes of atherosclerosis, the deposition of fat cells, also leads to thickening of arterial walls.
Genetic predisposition plays a special role in the development of heart disease. Anomalies and a tendency to form blood clots and atherosclerotic plaques can be inherited.
Separately, it is necessary to say about open injuries, which lead to direct damage to the rapidly dying tissues of the muscular organ. However, closed wounds can also be dangerous: they can cause contusion of the muscular wall of the heart, as a result of which blood temporarily leaves the vessels adjacent to the organ.
What is an extensive infarction of the posterior wall of the heart?
What is an extensive infarction of the posterior wall of the heart? How to recognize it and what symptoms does it have? Why is it so important to quickly diagnose the disease and hospitalize the patient in time? What consequences can a posterior wall myocardial infarction have?
There are two forms of heart attacks, based on the scale of damage to the walls of the heart: this is a small-focal form and an extensive form of heart attack. An extensive form of infarction of any localization is also called transmural infarction. An extensive infarction of the posterior wall of the heart is characterized by disruption of blood flow, and therefore a disruption of the supply of oxygen and nutrients to fairly large areas of the heart muscles. With a small focal infarction, such a disorder is localized only in certain areas of the heart.
The causes of an extensive infarction of the posterior wall of the heart can be stress, emotional stress, pathologies in the cardiac function and circulatory system. Also, the development of the disease can be affected by the presence of excess weight, lack of physical activity, smoking, alcohol abuse, sudden physical stress that is unexpected for the body, and hypertension.
An extensive infarction of the posterior wall of the heart develops quite quickly, is difficult, and also spreads between the ventricles along the posterior wall, affecting large areas of the heart muscle. Posterior wall infarction is much more difficult to diagnose. At autopsy, scars or acute myocardial infarction of the posterior wall are often discovered, even if ECG data did not show the presence of such a pathology.
Signs of an extensive infarction of the posterior wall of the heart can be: severe pain in the heart area, which is transmitted to the limbs, lower jaw, stomach and chest area. During an attack, the patient experiences a feeling of fear, a feeling of danger and anxiety. The peculiarity of an infarction of the posterior wall of the heart is that quite often it is completely asymptomatic.
The most dangerous are large-focal infarctions of the anterior wall of the muscle. Myocardial infarction of the posterior wall has less tangible consequences, but the scar remains for life and will make itself known to the body, but no tangible signs will be observed. The small-focal form of myocardial infarction of the posterior wall will leave the least noticeable consequences compared to any other form of infarction. Thus, it can only be detected through an autopsy or a detailed examination of the heart on an ECG.
The prognosis of the disease will depend largely on the form of the disease and the characteristics of the patient’s body. Only the attending physician can judge any serious consequences, however, disturbances in the functioning of the cardiovascular system, rhythm disturbances and other signs of heart disease will accompany the patient for the rest of his life.
Sometimes circulation problems occur when the main heart arteries become inflamed. In this case, arteritis develops. The disease is rare, but possible with a heart attack. It can be infectious or non-infectious in nature.
Bruises can also lead to myocardial infarction, especially penetrating ones. Closed injuries are considered dangerous in terms of the occurrence of a heart attack, since they lead to serious damage, contusion of the heart, which provokes a blood clotting disorder. In addition, after bruises, blood clots form, which often cause acute myocardial infarction.
Thickening of the walls of blood vessels due to metabolic disorders - this process develops slowly, but it is irreversible. In this case, extensive anteroseptal myocardial infarction occurs very often.
Important! Congenital pathologies of coronary vessels are distinguished separately. Patients who have been diagnosed with such a defect need to be extremely careful, because they are at risk of developing a major myocardial infarction
It is rare, but it happens that myocardial infarction of the anterior wall is the result of heart surgery. Doctors are not always to blame, because it is almost impossible to predict complications.
What is septal myocardial infarction of undetermined duration?
Septal myocardial infarction of unknown duration is one of the most dangerous heart diseases that requires preventive measures and immediate treatment.
The disease is formed as a result of a certain lifestyle, so this terrible disease can be prevented. The main cause of the disease is a sedentary lifestyle and poor nutrition.
Seizures often result in death, so it is important to know as much as possible about the disease.
What is myocardial infarction
Myocardial infarction refers to coronary heart disease. Many people suffer from attacks of the disease every day, mostly older members of society and people who have problems with excess weight.
To have a complete understanding of the disease, you need to understand how the heart works. Everyone knows that the heart is the main muscle of the human body, responsible for blood circulation.
The organ wall consists of three layers:
- The outer layer is called the epicardium.
- Myocardium, or muscle layer.
- Inner layer (endocardium).
Many arteries branch off from the heart, supplying vital muscles with blood and oxygen. In certain situations, when a person is worried, the heart begins to beat with frantic force. If the body is healthy, the myocardium works normally even in a stressful situation, since the arteries dilate, thereby increasing blood flow to the myocardium.
Myocardial infarction involves the death of one part of the heart. In this case, the left ventricle is at greater risk.
If for some reason expansion does not occur, the muscular layer of the heart absorbs everything needed in maximum sizes. This condition is called ischemia. Due to the fact that the myocardium takes everything it needs for itself, the heart does not receive the necessary substances, and coronary heart disease develops. Myocardial infarction involves the death of one part of the heart.
ECG for lower infarction
Next, the patient is sent for electrocardiography - a hardware research method that determines changes in the contractile function of the myocardium and blood circulation speed. It makes it possible to identify a blood clot or rupture of a vessel.
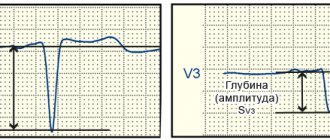
Characteristic ECG changes:
- The amplitude of the RV1,V2 wave increases.
- The initial RV1 is expanded.
- The depth of SV1,V2 decreases.
- ST (V1-2) decreases in the acute phase with reverse dynamics.
- The third Q wave widens to 2 mm.
- The second Q wave rises above the first Q.
This type of pathology is difficult to diagnose. Direct signs can only be determined in the Dorsalis lead along the Sky and in the additional chest leads V7–V9. And V2–V4 must be removed between the ribs above. An ECG must be performed several times to clarify the diagnosis.
It is also recommended to conduct additional examination methods:
- Echocardiography is an ultrasound scan that allows you to evaluate the work of the myocardium, the condition of the valve apparatus, measure the thickness of the walls, the level of pressure in the aorta, pulmonary artery, atria and ventricles.
- Radiography is a radiation diagnostic technique that is aimed at identifying pathology of the cardiovascular system.
- Donate blood for general and biochemical analysis.
Acute transmural infarction of the anterior myocardial wall (I21.0)
A sign of myocardial infarction of the anterior wall of the left ventricle, as well as infarction of any other area, is a pathological Q wave. The Q wave in an anterior infarction is considered pathological if:
– its amplitude is equal to or greater than a quarter of the amplitude of the R wave in the same lead;
– the width of the Q wave exceeds 0.03 s;
– the amplitude of the Q wave exceeds 4 mm;
– the Q wave is jagged or split;
– often a pathological Q wave is combined with a negative T wave;
– at the same time, ST segment elevation is observed in the same lead.
Myocardial infarction of the anterior septal region (anterior part of the interventricular septum) is in most cases caused by blockage of the septal branch of the anterior descending artery. With this localization, necrosis, as a rule, does not extend to the anterior wall of the right ventricle.
Characteristic ECG changes during anterior infarction are shown in the figure:
– QS type ECG is recorded in leads V1-V3;
– the ST segment in leads V1-V3 is above the isoline in the form of a monophasic curve;
– the ST segment in leads II, III, aVF is below the isoline.
In the presence of QS waves in the right precordial leads, it is often impossible to reliably determine the nature of MI (transmural or non-transmural). A long-term significant elevation of the STV1-V3 segment above the isoline may indicate a transmural infarction.
Other characteristic signs of MI of the anteroseptal region are:
– the appearance of a qV1-V3 wave of small amplitude (the ECG looks like qRS) is characteristic of the cicatricial stage of MI in the anteroseptal region;
– sometimes reciprocal changes are observed in chest leads V7-V9 (increase in the R wave; in the acute stage, a decrease in the ST segment and the appearance of a high T wave);
– disappearance of the qV5, V6 wave, however, such disappearance can be caused by blockade of the left bundle branch (blockade of the anterior or posterior branch of the LBP);
– the presence of jaggedness of the QRS complex in leads V1-V3 with the QS ECG type speaks in favor of MI;
– if such changes in the QRS complex are combined with a negative T wave and ST segment elevation, then this clearly indicates MI.
Myocardial infarction of the anterior wall is often caused by blockage of the anterior descending artery (its distal parts) arising from the left coronary artery.
Such a heart attack is diagnosed by characteristic ECG changes in leads V3, V4, which looks like QS or Qr (less often qrS, QR, QRs), as well as in the Anterior lead along the Sky.
Registration of QSV4 waves reliably indicates transmural MI (the presence of a QSV3 wave is observed in both transmural and non-transmural MI).
In case of MI of the anterior wall of the LV, reciprocal changes can be observed in leads III, aVF, Dorsalis (along the Sky), which are manifested by an increase in the R wave, and in the acute stage - a decrease in the ST segment and an increase in the T wave.
This location of the infarction is usually caused by blockage of the left anterior descending artery. Such a heart attack is diagnosed by characteristic ECG changes in leads V1-V4 and the Anetior lead along the Sky.
In this case, a qV1-V3 wave of small amplitude is observed (usually in the scar stage) (in these cases the ECG looks like qrS). Registration of the QSV4 wave is a reliable sign of transmural MI.
As a rule, QSV1-V3 waves are observed in both transmural and non-transmural MI.
In leads III, aVF, Dorsalis (along the Sky), reciprocal changes may be observed in the acute stage of MI, manifested by a decrease in the ST segment and the appearance of a high positive “coronary” T wave.
The amplitude of the R wave also increases, which persists into the scar stage.
The dynamics of reciprocal ECG changes in the acute stage of MI occurs faster than changes in the ST segment and T wave in leads V1-V4.
Lateral wall MI is usually caused by damage to the diagonal artery or the posterolateral branches of the left circumflex artery. Signs of such a heart attack are determined by changes in the ECG in leads V5, V6, I, II, aVL, Inferior (according to the Sky). The Q wave is considered pathological if:
– qV5,V6>15%RV5,V6 or qV5,V6>2 mm;
– qI>10%RI;
– qaVL>25%RaVL.
In the scar stage, a sign of MI of the lateral wall of the left ventricle is:
– deep wave SV5, V6, while the ECG in these leads looks like qRS, QrS, qrS;
– significant reduction in the amplitude of the RV5,V6 wave;
– pronounced serration of the QRSV5,V6,I,II,aVL complex.
A reliable sign of transmural MI is the presence of the QSV5,V6 wave. Sometimes reciprocal changes are observed in leads V1, V2, in which in the acute stage of MI there is a decrease in the ST segment, the appearance of a high positive T wave, and an increase in the amplitude of the R wave.
Myocardial infarction of the anterolateral wall of the left ventricle is usually caused by damage to the circumflex artery or anterior descending artery, which arise from the left coronary artery.
Signs of such a heart attack are determined by changes in the ECG in leads V3-V6, I, aVL, II, Anterior, Inferior (along the Sky).
Reciprocal changes (increase in the amplitude of the R wave; in the acute stage - a decrease in the ST segment and an increase in the positive T wave) are observed in leads III, aVF, Dorsalis (along the Sky).
Characteristic signs of anterolateral MI (myocardial infarction of the anterior and lateral walls of the left ventricle):
– the presence of deep SV4-V6, while the amplitude of the tooth increases from V4 to V6;
– a sharp decrease in the amplitude of the RV4-V6 wave;
– pronounced serration of the QRSV4-V6 complex;
– absence of growth of tooth RV3,V4;
– the presence of the QSV4-V6 wave reliably indicates transmural MI in this area.
Left ventricular apical myocardial infarction is usually caused by obstruction of the terminal branches of the left anterior descending artery. We can talk about such a localization of a heart attack if the signs are noted in isolation in lead V4 (less often V3-V5), Anterior (along the Sky). The presence of QSV4 reliably indicates transmural myocardial infarction.
MI of the high parts of the anterolateral wall is usually associated with damage to the diagonal artery or a branch of the left circumflex artery.
We can talk about such a localization of the infarction if the signs are recorded in isolation in lead aVL (aVL, I).
Occasionally, reciprocal changes may be observed (high wave RV1, V2, in the acute phase - a decrease in the STV1, V2 segment and the appearance of a high positive wave TV1, V2) in leads V1, V2 (less often III, aVF).
QaVL is considered pathological if it is greater than or equal in amplitude to half the RaVL wave.
If an infarction of the high parts of the anterolateral wall is suspected, it is recommended to perform an ECG in leads V4-V6 at the 1st and 2nd intercostal spaces above the normal level. It should be taken into account that such MIs are rather poorly recorded on the ECG.
Extensive myocardial infarction of the anterior wall is caused by blockage of the main trunk of the left coronary artery (usually its branch, the anterior descending artery).
Signs of an extensive infarction of this localization are recorded in leads V1-V6, I (II), aVL, Anterior, Inferior (along the Sky).
In this case, reciprocal changes must be observed (an increase in the R wave; in the acute phase - a decrease in the ST segment, a high positive T wave) in leads III, aVF, Dorsalis (along the Sky).
The spread of MI to the posterior wall of the left ventricle is indicated by a decrease in the height (compared to the previous ECG) of the RIII, aVF, or rIII, aVF waves of very small amplitude.
In case of extensive MI of the anterior wall of the left ventricle, all the above signs described for individual locations of infarction remain important for diagnosis.
Anterior wall MI is often complicated by ventricular extrasystole or tachycardia, and various supraventricular rhythm disturbances.
Complete transverse blockade sharply increases mortality (4 times) in cases of extensive myocardial infarction of the anterior wall. At the same time, such a blockade during MI of the posterior wall of the left ventricle increases mortality by only 2 times.
Source: https://diseases.medelement.com/disease/3777
Treatment of MI
Drug treatment
Treatment of large myocardial infarction is not an easy task. Difficulties in therapy arise due to the frequent development of complications against the background of large areas of necrosis. Treatment must be carried out in the intensive care unit. The goal of therapy for myocardial infarction is to restore blood flow in the affected vessel. It can be carried out using 2 methods:
- Drug dissolution of blood clots.
- Surgical restoration of blood flow. Can be done in 2 ways:
- Installation of a stent in a vessel, thanks to which its lumen expands and blood flow is restored.
- Bypass surgery is the creation of bypass routes for blood flow using vessels taken from other parts of the body.
In addition to restoring blood flow, treatment of a heart attack has the following goals:
- Anesthesia
- Preventing blood clots
- Reduced myocardial oxygen demand
- Normalization of blood pressure
- Treatment of complications
Disease history
Bashkir State Medical University
Department of Internal Medicine No. 3
Head department: prof.
Main disease: IHD. Acute small-focal myocardial infarction of the anteroseptal-apical region of the left ventricle, acute period. 30/11/99.
Age 04/16/1955 (44 years)
Place of work of UPATO No. 4
Date of admission to hospital 11/29/99 11:30
Diagnosis of the referring institution: ischemic heart disease, exertional angina, FC II. Acute apical ischemia.
1. Complaints: compressive, burning, paroxysmal pain of high intensity. The pain is localized behind the sternum, radiates to both arms, and occurs with minor exertion or with nervous-emotional stress; treated with nitroglycerin. Duration about 10 minutes. Weakness.
He has considered himself sick since 1997. The onset of the disease is not associated with anything. In the spring of 1997, he went to the clinic with complaints of compressive pain behind the sternum. A diagnosis was made: ischemic heart disease, exertional angina. He was treated as an outpatient. Pain relieved with nitroglycerin.
Deterioration of the condition since November 26, 1999 after intense physical activity. Frequent intense pain in the chest occurred, disturbing with little physical activity, at rest, radiating to both arms. Painful attacks were relieved with nitroglycerin.
On November 29, 1999 I contacted my local physician. After an ECG, he was sent to the hospital for emergency reasons with a diagnosis of coronary artery disease, exertional angina, FC II. Acute apical ischemia.
Born in the village xxxxxxx. The second child in the family (3 children in total). He grew and developed according to his gender and age. Education: secondary vocational. Graduated from a motor transport school.
Work history: started working at the age of 22, after graduating from college, as a car mechanic. Currently working at UPATO as a car mechanic. The work involves heavy physical activity.
Served in the army from 1973 to 1975.
Married since 22 years old, has a son (19 years old).
Living conditions are good.
Bad habits: drinks alcohol, smokes 2 packs a day since age 20.
Past illnesses: acute respiratory infections, influenza. HFRS in 1975. IHD, angina pectoris since 1997. Surgery for a forearm fracture in 1983.
There are no allergies to medications.
Heredity is not burdened.
4. Physical examination data.
The general condition is satisfactory, the consciousness is clear, the position is active, it is easy to enter into conversation, the facial expression is calm, the gait is normal, the posture is stooped, the physique is normosthenic. The food is satisfactory.
The skin is dark in color, turgor and elasticity are reduced. Visible mucous membranes are of normal physiological color. Subcutaneous fatty tissue is moderately expressed.
The muscular system is developed satisfactorily, the muscles are painless, their tone and strength are sufficient.
The integrity of the bones is not compromised, their surface is smooth, there is no pain during palpation or tapping.
The joints are externally unchanged. The spine configuration is correct. Full range of movements in the joints and spine.
Simple body measurements.
2. Body weight: 70 kg.
3. Body temperature: 37.1 0 C.
Examination and palpation of the chest.
On examination, the chest is of regular shape and symmetrical. The course of the ribs is normal, the intercostal spaces are not widened. Respiratory rate 18/min. respiratory movements are rhythmic, of medium depth, both halves of the chest are evenly involved in the act of breathing. Abdominal breathing type.
When compressed, the chest is elastic and pliable. On palpation, the integrity of the ribs is not damaged, their surface is smooth. There is no pain on palpation of the chest. Voice tremors are moderately expressed, the same in symmetrical areas of the chest.
1. With comparative percussion over the entire surface of the lungs, a clear pulmonary sound is determined.