The normal weight of the human heart ranges from 250 g in women and 350 g in men. At the same time, for a number of reasons, the main muscle of the body, which ensures its vital functions, can increase in size and exceed half a kilogram. In this case, a pathological situation develops - cardiomegaly, which is otherwise called “bull heart”.
A person has a big heart - this phrase does not always have a figurative meaning and means that he is the life of the party and a disinterested person who wants to help everyone. Sometimes a person has a big heart in the truest sense of the word. This happens at those moments when the heart muscle noticeably increases in size. Moreover, the pathology can be either congenital or acquired. In the first case, it is found more often in children, in the second - in adults.
Article on the topic A year in two. What ages the heart and how to rejuvenate the heart muscle?
Among the main complications that can develop against the background of this pathology are stroke and heart attack as a consequence of circulatory disorders in the heart muscle. Therefore, the situation cannot be ignored. And if there are signs of a pathological condition of the heart muscle, you should not ignore them.
An expert from the National Health League, MD, cardiologist, professor Mehman Mamedov told AiF.ru about what a “bull’s heart” is, how the problem is diagnosed and what needs to be done about it .
What is the essence of the problem
Bull heart syndrome is another name for cardiomegaly. According to the definition, the disease is characterized by an enlargement of all four or one chamber of the heart, as a result of which the main muscle is not able to perform a pumping function and maintain the central hemodynamics of the body. The heart becomes flabby and exhausted due to illness, and muscle fibers do not stretch because there is not enough strength to function normally.
An increase in heart size is a natural process in some people, particularly in athletes or those who frequently engage in physical labor.
In some cases, the disease occurs without obvious clinical manifestations. This most often occurs in the initial stages of the disease.
In the classic version, the disease clinically manifests itself in the form of rhythm disturbances (arrhythmia), or frequent shortness of breath, swelling and pain in the heart area. These signs can also appear in other diseases of the heart muscle. Therefore, you should not delay visiting a specialist in the field of cardiology, because symptoms of an enlarged heart can usually be identified only with the help of a certain medical examination.
Sincere confession. How to preserve your heart during an epidemic? More details
Heart and blood vessels
There are certain age-related relationships between the weight of a child’s body and the weight of his heart, which are also reflected in the functional characteristics of the cardiovascular system in children of different ages. In newborns, the heart is relatively much larger and makes up about 0.8% of the child’s body weight; this is easily explained by the fact that during placental circulation, relatively more blood passes through the fetal heart.
During the first months of life, the relative weight of the heart decreases in children. In a newborn, the heart weighs about 20-24 g. At the age of 5-6 months, the relative weight of the heart is minimal, corresponding to approximately 0.4% of body weight; in further periods of childhood, body weight and heart weight increase approximately in parallel, and the heart by weight makes up about 0.5% of body weight.
The energy of heart growth in different years of a child’s life is not the same; its growth is most intense during the first 2 years and at the age of 14-15 years; The lowest growth energy of the heart is observed from 7 to 12 years. At almost all ages, the weight of the heart in boys is greater than in girls; At the age of about 14 years, the weight of girls' hearts temporarily exceeds the weight of boys' hearts, but after 16 years, when boys also enter puberty, the previous ratios are restored.
It should also be noted that the heart grows unevenly in width, length and thickness; Thus, in boys, the weight of the heart doubles by 1 year, the length of the heart - by 5-6 years, the width - by 9 years, and the thickness - by 13-14 years. During the first 5 years, mainly concentric growth of the heart occurs; The capacity of the cavities increases more strongly after 5 years. In a newborn child, the thickness of the walls of the right and left ventricles of the heart is almost equal and fluctuates around 5 mm; in subsequent years, the thickness of the walls of the left ventricle gradually increases, reaching almost 1 cm by the age of 14. The thickness of the wall of the right ventricle during the same period increases by only 1 mm.
Up to 10-12 years of age, in children the pulmonary artery is wider than the aorta; then their cross-sectional diameters are compared, and after puberty an inverse relationship is established between both vessels. The vessels in children are relatively wide, but their further increase in lumen and increase in the capacity of the cardiac cavities occurs unevenly: in a newborn, the ratio between the volume of the heart and the circumference of the aorta corresponds to 25:20, in the prepubertal period - 140:56 and by the end of puberty - 260:61 . The capillary system in children, on the contrary, is relatively wide, and according to some data, the capillaries of the lungs, kidneys, skin and intestines in newborns are even absolutely wider than in subsequent years of life.
Among the histological features of the children's heart and blood vessels, one can note the more delicate structure of the myocardial muscle fibers; they are thin, poorly developed and short, located more compactly, since the connective tissue layers between them are less developed and do not contain fat cells. As muscle cells grow, their nuclei also increase and they become more elongated, but the total number of nuclei decreases. The elastic tissue in the valves is not fully developed; the nerve ganglia of the arteries of newborns also show a still significant incomplete structure, gradually approaching the structure of adults only by 10-12 years.
Children have a well-developed network of small arteries that provide good blood supply to the heart muscle. The endocardium of a child's heart is loose and poor in elastic and muscle elements. The peripheral endings in the cardiac muscle of the vagus and sympathetic nerves are functionally quite mature, but the tone of the centers of the vagus nerve is reduced, which determines the weak inhibitory effect of the latter on the strength and frequency of heart contractions; in contrast, the tone of the centers of the sympathetic nerve is expressed quite well, which affects the prevalence of its influence on the child’s cardiac activity (Arshavsky) and affects the rhythm of heart contractions.
The relationship between the influences of vagal and sympathetic innervation in the direction of strengthening the former noticeably changes in children by the age of 2.5-3 years. There is no doubt that in children of different ages, especially in newborns and the first years of life, as well as during puberty, several details of the nervous regulation of the heart change, which, however, cannot be considered sufficiently well studied. The main points of regulation of cardiac activity, established by I. P. Pavlov in animals, and by his colleagues and students in adults, remain in full force in relation to the heart of children. The vagus nerve has a slowing and weakening effect on the heart, while the sympathetic nerves have an accelerating and strengthening effect. The law of the trophic influence of the enhancing nerve on the heart retains its significance for the heart of children.
Various elements of the morphological structure of the child’s heart do not mature simultaneously; maturation proceeds in leaps and bounds, the morphological differentiation of the nervous apparatus of the heart in children ends by the beginning of school age, and from prepubertal age the children's heart in its histological characteristics does not differ from the heart of an adult.
The electrocardiogram in children has some features that reflect the anatomical and biological characteristics of the child’s heart.
In the first lead (right and left hands), it is especially clearly possible to note that in newborns the R wave is very low, and the S wave, on the contrary, is very well pronounced. In an adult, the S wave is approximately equal to 5% of the R wave; in a newborn, on the contrary, the latter is almost 3 times smaller than the S wave. During infancy, wave 5 is approximately 2 times larger than the R wave, and in the remaining periods of childhood - an average of 2 times smaller than the R wave. The same properties of the newborn’s electrocardiogram can be noted, although less clearly, in the second lead (Fig. 49).
Rice. 49. Electrocardiogram of a newborn. Rice. 50. Electrocardiogram of a 6-month-old child. Rice. 51. Electrocardiogram of a 5-year-old child.
With age, the electrocardiogram gradually approaches that of an adult; According to some authors, these features disappear already at the beginning of the 2nd year of life, according to others, a child’s cardiogram approaches that of an adult somewhat more slowly, and even at school age, the S wave exceeds the R wave. In infancy, the atrial P wave and T wave are relatively high .
The duration of excitation from the atrium to the ventricles (P - Q interval) in newborns and children in the first 3 months of life ranges from 0.09 to 0.12 seconds, in older children - 0.13-0.14 seconds and upon reaching maturity - 0.148 seconds. The duration of systole in a newborn is 0.21 seconds, in older children - 0.34 seconds and in an adult - 0.36 seconds.
Thus, the right type of electrocardiogram is typical for very young children (Fig. 50). At preschool and school age, most children have a normogram (Fig. 51), although sometimes they also have a right type of electrocardiogram in the absence of other objective deviations from the norm on the part of the heart. The electrocardiogram, undoubtedly, can be affected by the influence of extracardiac moments, especially in adolescents of the pubertal period with age-related physiological changes in the endocrine-vegetative system. Therefore, the electrocardiogram cannot be assessed in isolation without taking into account other objective and anamnestic data.
The minute volume of the heart (the amount of blood ejected by the heart within 1 minute) in a newborn is about 330 ml, by the end of the 1st year of life it reaches approximately 1200 ml, by 6 years - 1800 ml, by 10 years - 2500 ml and by 15 years —3150 ml. Somewhat larger figures are given by Shalkov, who used the gas analytical method.
The minute volume is more or less proportional to the body's need for oxygen. The amount of oxygen consumed by the body at rest, per 1 kg of weight in children at the end of the 1st year of life, is 2-3 times greater than in an adult; throughout childhood, this value, gradually decreasing, approaches adult norms. Accordingly, the minute volume calculated per 1 kg of weight in infants is more than 2 times greater than in adults.
The pulse in children is much higher than in adults;
this is explained not only by the faster contractility of the child’s heart muscle and less influence of the vagus nerve, but also by his more intense metabolism. The increased blood needs of the tissues of a growing organism are satisfied by a relative increase in the cardiac output, but not due to an increase in its pulse volume, but due to an increase in heart rate. Table 7. Pulse rate in children (according to most authors)
| Age | Pulse per minute | Age | Pulse per minute | Age | Pulse per minute |
| Newborn 6 months 1 year 2 years 3 » 4 » | 120—140 130—135 120—125 110—115 105—110 100—105 | 5 years 6 » 7 » 8 » 9 » 10 » | 98—100 90—95 85—90 80—85 80—85 78—85 | 11 years 12 » 13 » 14 » 15 » | 78—84 75—82 72—80 72—78 70—76 |
The highest pulse rate (Table 7 and Fig. 52) is observed in newborns; however, during the first days of life, they also experience a temporary slowdown in heart rate to 80 and even 70 beats per minute.
Rice. 52. Blood pressure, respiration and pulse in children (according to Popov).
Throughout childhood, the heart rate gradually decreases; in children of the same age, heart rate can vary within very wide limits.
Girls, as a rule, have a higher pulse rate than boys at all ages. Children with small, droplet hearts usually have a faster pulse.
Screaming, restlessness, muscle movements and even slight increases in body temperature always cause a noticeable increase in heart rate in children. Even in completely healthy people, a certain unevenness of pulse periods can be noted. The sphygmogram of newborns is characterized by wavy, low height of individual pulse waves and the absence of secondary rises on the descending knee of the curve (monocroticism). These phenomena are explained by the weakness of heart contractions, rapid pulse, low elasticity of the arteries and the influence of respiratory movements.
In school-age children, the sphygmogram shows a slight tendency toward predicrotism rather than dicrotism. During the puberty period (14-15 years), the pulse becomes somewhat dicrotic and gradually approaches the normal pulse of adults (Fig. 53).
Rice. 53. Sphygmogram in children and adults. 1 - in a premature baby 3 weeks old; 2 - the baby is 5 weeks old; 3 - the child is 6 weeks old; 4 - in a child of 2 months; 5 - in a child of 3.5 months; 6 - the child is 6 months old; 7 - a child is 6 months old; 8 and 9 - in an adult.
Children are characterized by the so-called respiratory arrhythmia , which is especially clearly visible when the pulse slows down, for example in sleep; one might think that this arrhythmia is one of the manifestations of the peculiarities of the age-related mood of the autonomic nervous system.
Why is it developing?
There are several factors that may cause the disease:
- hypertension;
- kidney disease;
- coronary heart disease (angina pectoris);
- viruses or infections that affect the heart;
- drug or alcohol abuse;
- genetic factors, since the symptom sometimes occurs in newborns or fetal children;
- development of a heart valve with abnormalities;
- consequences of pregnancy and childbirth.
Article on the topic
Don't give in to pressure. How to protect yourself from hypertension
Therefore, those who are at risk for such triggers should undergo regular examinations with a cardiologist to identify the problem in a timely manner. Any disease detected as early as possible is easier to correct.
Anatomical and physiological features
To understand the structure of the human heart, let's first look at it from the outside. We see a cone-shaped hollow muscular organ, to which branches of large vessels of the human circulatory system approach from all sides, like tubes or hoses to a pump. This is the living pump of our body, consisting of several functional sections (chambers), separated from each other by partitions and valves. Every eighth grade student knows how many chambers there are in the human heart. For those who missed biology classes, we repeat - there are four of them (2 on each side). What are these heart chambers and what is their role in the circulatory system:
- The cavity of the right atrium receives two vena cava (inferior and superior), carrying oxygen-free blood collected from all over the body, which then enters the lower section (right ventricle), bypassing the tricuspid (or tricuspid) heart valve. Its valves open only during compression of the right atrium, then close again, preventing blood from flowing in a retrograde direction.
- The right heart ventricle pumps blood into the common pulmonary trunk, which then divides into two arteries that carry oxygen-free blood to both lungs. In the human body, these are the only arteries through which venous rather than arterial blood flows. In the lungs, the process of oxygenation of blood takes place, after which it is delivered to the left atrium through two pulmonary veins (again, an interesting exception - the veins carry oxygen-rich blood).
- In the cavity of the left atrium there are pulmonary veins that deliver arterial blood here, which is then pumped into the left ventricle through the cusps of the mitral valve. In the heart of a healthy person, this valve opens only in the direction of direct blood flow. In some cases, its valves can bend in the opposite direction and allow part of the blood from the ventricle to pass back into the atrium (this is mitral valve prolapse).
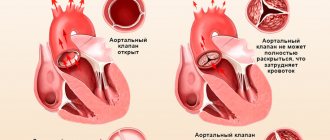
- The left ventricle plays a leading role; it pumps blood from the pulmonary (lesser) circulation to the systemic circle through the aorta (the most powerful vessel in the human circulatory system) and its numerous branches. The ejection of blood through the aortic valve occurs during systolic compression of the left ventricle; during diastolic relaxation, another portion from the left atrium enters the cavity of this chamber.
Diagnostic nuances
Bull heart syndrome is determined using complex diagnostics. It is the combination of several methods and techniques that allows for maximum assessment of the appearance, volume, and function of the heart. The list of studies to make such a diagnosis includes:
- blood analysis;
- chest x-ray;
- electrocardiogram;
- echocardiography;
- CT scan;
- sometimes - a biopsy of the inner surface of the heart ventricles.
All necessary studies are determined by the observing cardiologist. It is based on the severity of symptoms and the person’s condition.
A quieter pulse means you live longer. What should it be like normally? More details
Pathology therapy
Naturally, many are concerned about the treatment of this problem. And it must also be comprehensive.
First of all, it is necessary to determine the cause of cardiomegaly, that is, to establish the underlying disease. If a person has this pathology, basic therapy is carried out. For example, coronary heart disease or hypertension is corrected.
At the first stage, drug therapy is used to treat cardiomegaly. It includes the prescription of diuretics to remove excess fluid from the body, antithrombotic drugs to reduce the risk of developing a blood clot, and beta blockers to slow the rhythm and reduce the load on the heart.
Article on the topic
No interruptions! How are cardiac arrhythmias treated?
In some cases, surgical interventions are used to restore the damaged valve and improve the performance of blood vessels.
A special pump is also implanted to help the heart work. In some cases, devices are used to regulate the heartbeat: with an enlarged heart, a pacemaker is used to coordinate the contractions of the heart muscle.
Internal structure
The heart wall consists of several layers represented by different tissues. If you mentally draw its cross-section, you can highlight:
- the inner part (endocardium) is a thin layer of epithelial cells;
- the middle part (myocardium) is a thick muscle layer that, through its contractions, provides the main pumping function of the human heart;
- outer layer - consists of two leaves, the inner one is called the visceral pericardium or epicardium, and the outer fibrous layer is called the parietal pericardium. Between these two leaflets there is a cavity with serous fluid, which serves to reduce friction during heart contractions.
If we consider the internal structure of the heart in more detail, it is worth noting several interesting formations:
- chords (threads of tendons) - their role is to attach the valves of the human heart to the papillary muscles on the inner walls of the ventricles, these muscles contract during systole and prevent retrograde blood flow from the ventricle to the atrium;
- heart muscles - trabecular and comb formations in the walls of the heart chambers;
- interventricular and interatrial septa.
In the middle part of the interatrial septum, the oval window sometimes remains open (it functions only in the fetus in utero, when there is no pulmonary circulation). This defect is considered a minor developmental anomaly; it does not interfere with normal life, unlike congenital defects of the interatrial or interventricular septum, in which normal blood circulation is significantly impaired. Whatever blood fills the right half of the human heart (venous), this will also enter the left side during systole, and vice versa. As a result, the load on certain parts increases, which over time leads to the development of heart failure. The blood supply to the myocardium is carried out by two coronary arteries of the heart, which are divided into numerous branches, forming the coronary vascular network. Any disruption of the patency of these vessels leads to ischemia (oxygen starvation of the muscle), up to tissue necrosis (infarction).
Preventive actions
As with any other disease, it is better to try to prevent it than to treat it later. And here the issue of preventing “bull’s heart” is important.
When an enlarged heart occurs, the consequences can manifest themselves in different ways, so with the least risks you should pay attention to your health. Ideally, you should adhere to the principles of a healthy lifestyle and eliminate bad habits such as alcohol and smoking. A person who does not want to face the consequences of an enlarged heart should constantly monitor blood pressure, consume less salt, engage in suitable physical activity, and lose excess weight. The recommendations are simple, but they will help you keep yourself in good shape.