Aortic valve defects often require surgical intervention. Depending on the indications, partial or complete replacement of the valve apparatus can be performed, which improves hemodynamics in the heart and reduces the risk of developing heart failure.
Aortic valve replacement is a surgical procedure used to treat a heart disorder caused by damage to the aortic valve. In most cases, in the absence of surgical intervention of a heart defect, severe disorders occur, leading to changes in the functioning of internal organs.
The aortic valve helps regulate blood flow from the heart to all organs and tissues. The valve also ensures that blood flows in one correct direction.
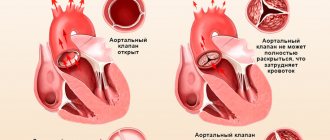
When the left ventricle contracts, the aortic valve opens, allowing blood to flow into the aorta through the aortic orifice. As the ventricle relaxes, the aortic valve closes, preventing blood from returning from the aorta. As a result, oxygenated blood enters the brain and all internal organs related to the systemic circulation.
Video: Aortic valve replacement
Story
Early surgical approaches to aortic valve disease were limited by the need to deal with a constantly beating heart. In the 1950s, the Hufnagel valve was implanted into the descending thoracic aorta in patients with aortic regurgitation.
The first successful aortic valve replacement was reported in 1960 under the leadership of Harken.
Introduction of the presented technique proceeded slowly, based on the limitations of available replacement valves and the relatively primitive methods of protecting the heart during surgery that were available at the time. With the gradual introduction of mechanical heart valves, the development of cardiopulmonary bypass (heart-lung machine) and cardioplegia, which allow the heart to be stopped safely during surgery, aortic valve replacement has become available to patients with severe aortic regurgitation or regurgitation.
Other recommendations
There are a few other mandatory tips that patients undergoing valve replacement surgery must follow.
- If you experience symptoms of cardiac problems (chest pain, a feeling of interruptions in the heart), signs of circulatory problems (swelling in the legs, shortness of breath) and other unexpected symptoms, you should immediately consult a doctor.
- Patients who have had a biological valve installed are not recommended to take calcium supplements. In their diet, it is advisable for them not to overuse products containing it: milk and dairy products, sesame seeds, nuts (almonds, Brazilian), sunflower seeds, soy.
- All doctors, including the dentist, need to warn the patient that he has an artificial valve installed.
Following the necessary recommendations will help the patient maintain excellent health for a long time and live a full life.
Description of aortic valve defects
Diseases (defects) of the aortic valve occur when, for various reasons, the structure of its valves or aortic opening is disrupted. In particular, the following aortic valve defects are distinguished:
- Aortic valve stenosis (a narrowing of the aortic valve that restricts blood flow).
- Smoothing of the aortic valve (valve insufficiency, which leads to incomplete closure of its leaflets).
- Aortic valve regurgitation (blood that is released into the aorta immediately returns to the cavity of the left ventricle, causing the heart to stop beating normally).
Facts about aortic valve defects:
- They cause the death of 25,000 people a year.
- It is detected in 7% of the world's population over the age of 65 years.
- Two years after diagnosis of severe aortic stenosis, untreated patients have a 50% survival rate.
It is when the aortic valve does not work properly that hemodynamics become difficult and blood flows poorly to organs and tissues. With defects, the load on the heart also increases, which has an even more negative impact on maintaining uniform blood circulation throughout the body.
Symptoms of aortic valve defects
In some patients, significant changes are not observed for many years, while in other patients, symptoms appear very quickly and severely. The most common symptoms of aortic valve dysfunction are:
- Pain in the chest or behind the breastbone.
- Arrhythmia (sinus tachycardia, atrial flutter).
- Dyspnea (breathing difficulty).
- Disorder of consciousness.
- Fainting.
- Fatigue.
- Heart failure.
- Heart failure.
Diagnosis of aortic valve defects
With an objective examination of the patient, sometimes the doctor can immediately diagnose aortic insufficiency. In particular, cyanosis of the skin, earlobes and nasolabial triangle may appear. During auscultation, changes such as weakening of the first sound at the apex of the heart, dancing of the carotid, etc. can also be heard.
Additional research methods:
- Electrocardiography (ECG).
- Echocardiography (echoCG or ultrasound of the heart).
- Radiography.
- Doppler study.
- Phonocardiography.
Depending on the patient's condition and prognosis, aortic valve replacement may be recommended. This surgical option is very effective in treating severe valve disease. A successfully performed operation alleviates or completely eliminates painful symptoms by regulating hemodynamics in the body. As a result, surgical therapy helps prolong life and enhance the dynamics of the heart muscle.
Preparing for valve replacement surgery
Preparation for surgery begins with a thorough examination, including:
- General and biochemical blood tests;
- Urine examination;
- Determination of blood clotting;
- Electrocardiography;
- Ultrasound examination of the heart;
- Chest X-ray.
Depending on the accompanying changes, the list of diagnostic procedures may include coronary angiography, vascular ultrasound, and others. Consultations with narrow specialists, opinions of a cardiologist and a therapist are required.
On the eve of the operation, the patient talks with the surgeon, anesthesiologist, takes a shower, has dinner - no later than 8 hours before the start of the intervention. It is advisable to calm down and get some sleep; many patients benefit from talking with the attending physician, clarifying all questions of interest, knowing the technique of the upcoming operation and getting to know the staff.
Aortic valve replacement procedure
There are various factors that are taken into account when deciding whether to carry out a replacement procedure. Some of these factors:
- Patient's age.
- Health status.
- Concomitant diseases that may contribute to the progression of aortic valve disease.
Typically, doctors choose heart valve reconstruction because this method has the lowest level of risk. Using various methods of restoring valve flaps, the condition and functioning of the heart improves. Additionally, the need for anticoagulants (blood thinners), which are often recommended for many years after some types of valve replacement, is significantly reduced.
Difference between aortic valve reconstruction and replacement
In some patients, there is a violation of the structure of the aortic opening, which leads to improper closure of the aortic valve leaflets. In such cases, doctors suggest a reconstruction procedure. This decision mainly depends on the severity of the patient’s condition, because valve defects cannot always be “repaired.”
It is important to know that valve reconstruction is a more complex process compared to valve replacement. Only after careful research and meetings of doctors of various specializations can a decision be made to restore the damaged valve.
Aortic valve replacement can be performed in two ways:
- Through open heart surgery.
- Through transcatheter surgery (TAVR), that is, replacing the aortic valve using a catheter.
During open heart surgery, a large incision is made in the patient's chest. During TAVR, all required manipulations are performed through a small hole in the sternum. As a result, the second option for aortic valve replacement is less complex, more effective, and carries less risk than open-heart surgery. Only a doctor can decide which of the proposed options is the best, most effective and safe for a particular patient. Much depends on the person’s health status and medical history.
Reasons for installing an artificial valve
In medical circles, a heart valve is compared to a door that needs to be repaired if it loses its original functionality. In the case of the heart valve, doctors use the same approach. Damage to the heart valve, requiring radical approaches and choice of treatment methods, is classified into three types.
The first involves processes of narrowing or agglomeration, which causes a slowdown in blood flow, which negatively affects the nutrition of the heart, leading to oxygen starvation. The second is due to processes of expansion or hyperextension, leading to a violation of the tightness of the heart and increased stress. The third is a combined version of the two previous types.
A diagnosis of heart failure is not a reason to panic. Implantation is not always indicated. Doctors perform other operations, for example, organ reconstruction.
Aortic valve replacement in Israel is recommended when its functional capacity is clearly limited. The reasons leading to surgical intervention are: infection, atherosclerosis, organ tissue disorders and other diseases.
Valve types
There are two main types of artificial heart valve:
- Mechanical valves.
- Tissue valves.
Mechanical valves
Mechanical valves are designed so that the patient can use them for a long time. Although mechanical valves are durable and usually a one-step solution, there is an increased risk of blood clots with their use. For this reason, all patients who have had mechanical valves implanted must take anticoagulants (blood thinners) such as warfarin for the rest of their lives. As a result, there is a pronounced tendency to bleeding. Also, the sound of mechanical valves can be heard by the naked ear, which sometimes reduces the patient’s quality of life.
Fabric valves
Tissue heart valves are typically made from animal tissue, part of an animal heart valve, or animal pericardial tissue. The selected material is subjected to special treatment to prevent rejection and calcification.
There are alternatives to fabric valves. In some cases, a homograft, a human aortic valve, may be implanted. Homograph valves are provided to patients and can be repaired after another person (the valve donor) dies. The durability of homograph valves is comparable to valves made from porcine and bovine tissue.
Another aortic valve replacement procedure is the Ross procedure (or pulmonary autotransplantation). In the Ross procedure, the aortic valve is removed and replaced with the patient's own pulmonary valve. A pulmonary homograft (pulmonary valve taken from a deceased person) is then used to replace the patient's own pulmonary valve. This procedure was first used in 1967 and is used primarily in children because the surgery allows the patient's pulmonary valve (placed at the site of the aorta) to grow with the child.
Valve selection
Tissue valves tend to wear out faster due to increased exposure to blood flow. This condition is especially true for active (usually younger) people. Today, tissue valves can typically last about 20 years, but they definitely wear out faster in younger patients.
When a tissue valve fails and needs to be replaced, a person must undergo repeat surgery to have a new valve installed. For this reason, younger patients are more likely to receive mechanical valves, thereby avoiding the increased risk and associated inconvenience associated with re-implantation of a different valve.
Life with an artificial heart valve
An artificial heart valve is installed when the activity of one of the 4 valves of the organ is impaired, for example, due to narrowing or excessive expansion of the heart openings.
It is a prosthesis with the help of which the blood flow is directed in the correct direction, while the mouth of the venous and arterial vessels is intermittently blocked.
If there is a gross change in the valve leaflets, which clearly impairs blood circulation, doctors prescribe the installation of an artificial valve.
There are 2 types of heart valves:
The following diseases may be indications for surgery:
- Congenital heart disease in infants.
- Rheumatic diseases.
- Changes in the valve system due to ischemic, traumatic, immunological, infectious and other reasons.
Open heart aortic valve replacement
Aortic valve replacement is most often performed through a middle sternotomy, which means the device is implanted by cutting through the sternum. After opening the pericardium, the patient is connected to a heart-lung machine. This device takes over the breathing and blood pumping functions needed for the patient while the surgeon replaces the heart valve.
After the patient is connected to all the necessary equipment, the surgeon removes the diseased aortic valve through special incisions, and a mechanical or tissue valve is placed in its place. Once the device is in place and the aorta is closed, the patient is disconnected from the heart-lung machine.
Transesophageal echocardiography (TE echocardiography, ultrasound of the heart performed through the esophagus) may be used to check that the new valve is functioning correctly. Sometimes complications arise after surgery; to prevent their development, sensors are installed in the necessary places, which allow the heart to be adjusted if necessary. Drainage tubes are also inserted to remove accumulated fluid from the chest and pericardium after surgery. They are usually removed within 36 hours, while stimulation probes are usually left in until the person leaves the hospital.
Hospital stay and recovery
After aortic valve replacement, the patient will most often remain in the intensive care unit for 12-36 hours. You are allowed to return home after about four days have passed, without complications such as heart block.
Recovery from aortic valve replacement usually takes about three months if the patient is in good health. At the same time, those who have undergone surgery are not recommended to do heavy work for 4-6 months, which avoids damage to the sternum and suture dehiscence.
Heart valve transplantation and possible complications
According to experts, a patient who comes for a medical consultation in a timely manner practically reduces the risk of complications to zero. All other scenarios for the development of the event indicate a minimal risk of the operation itself and the danger of non-compliance with medical recommendations in the period after implantation.
A careful attitude towards one’s own health is a principle that the person undergoing surgery must adhere to. The patient must follow the doctor’s recommendations regarding: daily routine, nutrition, and medication. This is the only way a person with an artificial implant can ensure a long life.
Transcatheter aortic valve replacement
This minimally invasive surgical procedure allows a new valve to be implanted without removing the damaged one. If the operation is successful, the new valve, after its installation, begins to perform the functions of the old aortic valve. The surgery may be called transcatheter aortic valve replacement (TAVR) or transcatheter aortic valve implantation (TAVI).
Valve-in-valve operating principle
During the operation, a device, somewhat similar to a stent, is placed in the artery and then a replacement device is delivered through a catheter to the location of the damaged valve, completely disassembled.
As the new valve expands, it pushes the old valve flaps out of the way while the replacement device begins to do the job of regulating blood flow.
The procedure presented is innovative and FDA-approved for people with symptomatic aortic stenosis who are considered intermediate or high risk for standard valve replacement surgery. The differences between conventional and minimally invasive techniques are significant.
Performing the TAVR procedure
Conventional valve replacement is performed through an open approach to the heart, which is performed through a sternotomy. As a result, the chest is surgically opened for surgery. Unlike conventional treatment, TAVR or TAVI can be performed through very small holes that leave all the bones of the chest intact.
There are also risks associated with TAVR, but it is a more affordable treatment option for people who have not previously been eligible for surgery. At the same time, there is the added bonus of faster recovery in most cases. The patient experience with the TAVR procedure may be comparable to cardiac balloon surgery or angioplasty in terms of completion time and recovery. As a result, after surgery, patients are discharged from the hospital faster (on average after 3-5 days).
The TAVR procedure is performed using one of two different approaches, allowing the cardiologist or surgeon to choose which provides the best and safest access to the valve.
Ways to perform TAVR:
- Transfemoral approach - insertion of a catheter through the femoral artery (large artery in the groin area), performed without a surgical incision in the chest
- The transapical approach is to insert a catheter through a small incision in the chest and enter through a large artery in the chest or through the apex of the left ventricle.
Indications for TAVR
Currently, the procedure is performed in cases where the patient is classified as intermediate risk for open access to the heart. For this reason, most people who have this type of surgery are between the ages of 70 and 80 and often have other medical conditions for which this type of surgery is performed.
TAVR can be an effective option to improve the quality of life for patients who would otherwise have limited options and whose aortic valve reconstruction is not possible for some reason.
Types of heart valves
Today, doctors operate with two types of artificial valves: mechanical and biological. Each of them has its own advantages and disadvantages.
Mechanical valves are a kind of prosthesis that is designed to replace the function of the natural human heart valve. The main job of the valves is to carry blood through the heart and release it back out. Mechanical valves are installed when the function of the native heart valve is no longer restored.
Tests of modern man-made valves estimate a service life of 50,000 years when placed under accelerated wear conditions. This means that if it takes root in a person, it will work until the moment the person is measured out. The only thing worth remembering is that all artificial valves require additional support and the use of anticoagulants that thin the blood so that blood clots do not form in the heart. You will also have to undergo regular tests.
Biological valves are prosthetic valves made from animal tissue. Very often they use a pig heart valve. Naturally, it is pre-processed to make it suitable for implantation into the human body. Biological valves, in comparison with mechanical valves, are noticeably inferior in durability.
Complications after aortic valve replacement
Some of the serious complications associated with aortic valve replacement surgery are:
- Formation of blood clots, which can cause pulmonary embolism or ischemic stroke.
- Uneven heartbeat, which can be expressed in atrial flutter/fibrillation, sinus tachycardia.
- Bleeding.
- Infection.
- Valve dysfunction.
- Fatal outcome.
All of these complications are most often associated with aortic valve replacement through open access to the heart. In such cases, it is very important to take timely measures to eliminate them, otherwise the person may die.
Video: Minimally invasive aortic valve replacement
4.00 Aug. rating ( 80 % score) – 7 votes – ratings
Heart valve replacement: mitral, aortic - surgery, before and after
Have you been struggling with HYPERTENSION for many years without success?
Head of the Institute: “You will be amazed at how easy it is to cure hypertension by taking it every day.
Heart valves are the basis of the internal frame of the heart, which are folds of connective tissue. Their functions boil down to delineating the volumes of blood in the atria and ventricles, allowing these chambers to alternately relax after pushing out blood at the time of contraction.
Purpose of the operation
Stenosis is a heart defect in which the lumen of the valve narrows, resulting in the disruption of blood flow from the left ventricle. There are 2 types of illness:
- congenital;
- acquired.
This disease often occurs among the stronger sex. Typically, patients under 30 years of age have a congenital form, and after this age an acquired form.
The valves of a healthy person have 3 valves in the shape of a triangle. However, if there is a congenital pathology, then some of the valves are missing. Such a problem may not cause discomfort for a certain period of life. With age, a gradual narrowing of the lumen will occur and urgent heart valve replacement will be required.
Development of the disease
Acquired stenosis develops for the following reasons:
- During the process of age-related changes, salts are deposited on the valves; this phenomenon is dangerous for people who lack them. The pathology is typical for patients after 60-65 years of age.
- Rheumatism develops as a result of a sore throat. With such a deviation, gradual tissue growth and salt deposition occurs on the valve flaps.
The average life expectancy for patients with this diagnosis is 4-5 years. However, if cardiac arrest occurs periodically, there is a risk of sudden death.
Why is surgical treatment necessary?
Most cardiac diseases initially require conservative management. However, it is often ineffective, which leads to suffering for patients, a decrease in their standard of living, and disability. In such cases, surgical treatment is recommended. The indications are:
- Severe aortic calcific stenosis, accompanied by a characteristic clinical picture:
- fainting;
- severe shortness of breath;
- pain in the heart area of a pressing or squeezing nature (similar to angina attacks);
- reduced ejection fraction according to ultrasound scanning results - less than 40%.
- Acute rheumatic attack with the formation of a defect and the development of chronic rheumatic heart disease (CRHD).
- Infectious endocarditis.
- Congenital heart defects (Ebstein's anomaly).
- Idiopathic disease of the aortic valve.
Surgical intervention is performed only with the written consent of the patient.
Causes of aortic valve disease
There are many pathological conditions that over time can lead to degenerative changes, calcium deposition on the aortic valve leaflets, and changes in its function.
The human heart is able to compensate for poor circulation for some time. Sooner or later, clinical manifestations occur: dizziness, shortness of breath, fainting, palpitations, angina syndrome. Conservatively (with the help of medications) it is possible to partially compensate for the patient’s condition, but it will not change it radically and will not improve the quality of life.
What can you eat after heart surgery? Nutrition after heart surgery for recovery
It is necessary to reduce the content of animal fats and easily digestible carbohydrates in the diet, as well as reduce the consumption of table salt, coffee and other stimulants. At the same time, you should enrich your diet with vegetable oils, fresh vegetables and fruits, fish and protein products.
Young patients who do not have atherosclerosis and its complications may not be so strict about their diet, although it is best for them to formulate a diet in accordance with the canons of a healthy diet - to prevent IHD. Middle-aged and elderly patients, especially those with coronary heart disease, are advised to adhere to a special diet.
Postoperative period and rehabilitation
For a full rehabilitation process, doctors recommend completely changing the nutritional system. A diet plan is prescribed immediately after a heart attack. For overweight people, the attending physician, as a rule, prescribes an additional diet plan for weight loss, since losing excess weight removes additional stress from the heart muscle.
The diet after a heart attack has several main features, following which the patient quickly recovers.
The key point of the diet after heart surgery is to reduce the caloric intake to kcal per day. Reduce the amount of liquid to 1.5 liters per day, not counting first courses and dairy products. Protein should be sought in fish and seafood, low-fat dairy products. Particular attention should be paid to white fish - omul, flounder, cod, hake. It contains fatty acids that lower blood cholesterol levels.
Firstly, after a heart attack, meals must be divided: up to 7 times a day. Food intake should occur in reduced portions. Secondly, patients who have had a heart attack are advised to drink carrot juice. You need to add a tablespoon of vegetable oil to the drink. The fourth rule is to prepare porridges in a special way.
They should be slightly overcooked, pureed and liquid. It is better to cook soups with a vegetable base or broth made from lean meats. Food should be salted in a minimal amount. Herbs and spices should be excluded. With a large heart attack, after one and a half to two months, a period of scarring begins, during which the diet can already be varied as much as possible.
A person needs a healthy lifestyle and a balanced diet even when his heart and blood vessels are in a healthy state and perform their basic functions. If you have diseases of the cardiovascular system or after surgery, you must follow a special diet to restore heart health. A concomitant result of any cardio diet is the effect of weight loss. Many cardiology specialists recommend that their patients lose excess body weight. By getting rid of extra pounds, you will reduce the load on the depressed heart muscle.
You can eat dishes prepared with salt, but still in moderation. After a heart attack, the body needs to restore the water-salt balance. To do this, you should drink plenty of fluids: drink at least three glasses of water a day, eat soups and fruit drinks. After the first stage of rehabilitation after a heart attack, the number of meals should be reduced and the portion size gradually increased.
As for drinks, it will be useful to include fermented milk products in your diet: kefir and fermented baked milk. Throughout the rest of their lives, people who have had a heart attack should eat cholesterol-rich foods in moderation, mainly boiled eggs, pickles, spicy and fatty foods, alcoholic beverages and strong coffee.
Surgery must be reported to all physicians prior to the procedure. To extend the life of the valve made from biological materials, patients should not use medications or products enriched with calcium. If you have complaints of pain or deterioration in health, you should immediately consult a doctor.
Only at high operational risk
“At present, only patients with a clearly increased surgical risk or contraindications to conventional surgery should be considered for interventional cardiology [referring to TAVI], since long-term results are not yet available and high-quality results have not yet been achieved after surgical cardiac replacement. valve (mortality rate of about 3%) or surgical repair of the heart valve (mortality rate of about 2.5%),” the congressional document states.
However, this rule is often ignored, because Many TAVI interventions are performed at significantly lower risk and therefore in younger patients. This is confirmed by statistics from the DGTHG (Association of German Thoracic and Cardiovascular Surgeons) 2010, which were presented by Prof. Mohr, Director of the Cardiac Surgery Clinic, Heart Center in Leipzig.
In addition, the figures confirm the limits of the use of TAVI, since - as pointed out by Prof. Mortality – in patients without a clearly increased risk (Figs. 3 and 4), in-hospital mortality with surgical aortic valve replacement is clearly lower than with TAVI. Even in the group with a clearly increased risk (log EuroSCORE of 20% or more), it is not higher than with TAVI (11.7 and 11.4%, respectively). Also, when distributing patients by age (Fig. 5 and 6), according to the DGTHG graph, up to 85 years of age, there are no noticeable advantages of TAVI compared to surgery, explained Prof. Mor.
In addition, during the discussion it was noted that log. EuroSCORE is not sufficient to evaluate both methods.
Meanwhile, the results of two large studies on TAVI (PARTNER) were published. The PARTNER I study showed that in patients with aortic valve stenosis who are contraindicated for surgery, TAVI is preferable to conservative treatment. The PARTNER II trial showed that in patients with high-risk aortic valve stenosis, TAVI was noninferior to open valve replacement surgery. However, to date, patients have been followed up for an average of only one year, i.e. It is unknown what the long-term results of these methods are in comparison with each other.
Experts have warned about the high potential for abuse of TAVI . Patients with log. A EuroSCORE greater than 20% and those over 75 years of age should not automatically be considered candidates for TAVI.
The figures demonstrate in-hospital mortality after catheter-based TAVI aortic valve implantation on the left (Figs 3+5) and after standard surgery on the right (Figs 4+6) in 2010. The results are presented depending on the age group, etc. "log. EuroSCORE". Log. EuroSCORE shows predicted operative mortality and is calculated based on individual comorbidities and risk factors (eg age, diabetes, renal failure, hypertension...).
Patients with log. have a very high risk. EuroSCORE is above 15-20. Previous experience shows that EuroSCORE actually overestimates operative mortality by 2-3 times, but largely determines the long-term prognosis of the patient. It is clear that younger patients with a low EuroSCORE have excellent outcomes after surgery, while TAVI patients in the younger age groups with a low Euroscore have an unexpectedly high mortality rate. (Prof., MD Friedrich-Wilhelm Mohr, Leipzig)
Types of operations
Prostheses that are implanted in place of a damaged heart valve are called grafts. They are classified according to the materials from which they are made. There are 2 main types:
- Mechanical artificial valves.
- Biological:
- xenografts obtained from tissues of pigs and calves;
- homografts are made from human tissue (cadaver);
- autografts – taken from the patient himself.
The cardiac surgeon decides which prosthesis is preferable.
The advantages of artificial valves are:
- theoretically unlimited service life.
The disadvantages of such a prosthetic valve are:
- lifelong use of anticoagulants;
- diet;
- high risk of bleeding;
- inability to carry a pregnancy to term;
- mechanical noise of the valve operation, audible from a distance.
Among the advantages of xenografts it is worth noting:
- no need for lifelong medication and diet;
- there is no noise from the valve operation.
However, this type of prosthesis has a number of disadvantages:
- high risk of foreign material rejection;
- after 10 years, replacement is necessary due to degenerative changes and calcification of the biological implant.
Homografts have only one disadvantage - their small number. The advantages of this type of prosthesis are:
- no need for repeated surgery;
- the possibility of bearing a child for women with preserved reproductive function;
- low incidence of postoperative and thromboembolic complications;
- not taking anticoagulants;
- 100% positive effect in patients with endocarditis;
- Possibility of use in the youngest patients.
The most commonly used types of cardiac homografts are:
- cryopreserved;
- treated with antibiotic;
- fresh valve
The starting material is tissue from the aorta or pulmonary artery.
The operations themselves for implanting prostheses can be divided into 2 large groups:
- transthoracic (with dissection of the chest);
- transcatheter with installation of a bioprosthesis;
- transaortic implantation.
The type of intervention is selected taking into account the patient’s age, type of aortic valve damage, and concomitant pathology.