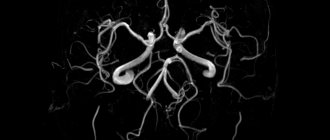
Peculiarities
The brain is reliably protected by the cranium from adverse environmental conditions. Being an organ regulating all physiological processes occurring in the body, it uses enormous amounts of nutrients. The brain weighs only 1-3% of the total human body weight (approximately 1,800 g). But for it to work well, 15% of the total blood volume (about 800 ml) must constantly flow through the vessels feeding the organ. It metabolizes up to 100 g of glucose per day.
That is, normal functioning of the brain will occur only if there is an adequate blood supply, with a large amount of nutrients, oxygen and a complete absence of substances toxic to humans. Plus, there must be a constant and adequate outflow of venous fluid.
Symptoms of chronic cerebrovascular insufficiency
Important: the main clinical features of CNM include syndromicity, stages and a progressive course!
It is customary to distinguish 2 main stages of chronic cerebral ischemia:
- initial manifestations;
- encephalopathy.
The initial stage develops when the flow of blood decreases from normal levels of 55 ml/100 g/min to 45-30 ml.
Typical patient complaints:
increased fatigue;- short-term episodes of dizziness;
- sleep disorders (difficulty falling asleep at night and daytime sleepiness);
- periodic feeling of heaviness in the head;
- memory impairment;
- slowing down the pace of thinking;
- decreased clarity of vision;
- episodes of headache;
- a transient feeling of instability when walking (impaired balance).
In the early stages of development of cerebral blood flow insufficiency, symptoms appear after physical exertion or psycho-emotional stress, fasting and drinking alcohol.
During the examination, when determining the neurological status, no signs of focal changes in the central nervous system are revealed. Special neuropsychological tests can identify disorders of thinking functions (in a mild form).
Please note: up to 450 thousand cases of acute cerebrovascular accidents – strokes – are diagnosed in our country every year. According to various sources, vascular dementia affects from 5% to 22% of elderly and senile people.
Discirculatory encephalopathy (DE) develops against the background of a decrease in blood flow to 35-20 ml/100 g/min. Changes, as a rule, occur due to general vascular pathologies.
Please note: significant changes in hemodynamics are noted if there is a narrowing of the great vessels to 70-75% of normal.
DE forms:
- venous;
- hypertensive;
- atherosclerotic;
- mixed.
Discirculatory encephalopathy is divided into 3 stages depending on the severity of neurological symptoms.
Signs of stage 1:
- memory impairment (problems with remembering new information are noted);
- decreased ability to concentrate;
- decreased mental and physical performance;
- high fatigue;
- dull headache (cephalgia), which increases with psycho-emotional experiences and mental stress;
- problems with switching from one task to another;
- frequent dizziness;
- unsteadiness when walking;
- insomnia;
- worsening mood;
- emotional instability.
The working capacity of patients with stage 1 is preserved. A neurological examination reveals moderate memory impairment and decreased attention. Reflexes are moderately increased; their intensity on the right and left is slightly different.
Signs of stage 2:
- progression of memory disorders;
- severe deterioration in sleep;
- frequent cephalgia;
- transient dizziness and instability in a vertical position;
- darkening of the eyes when changing body position (standing up);
- touchiness;
- irritability;
- reduction of needs;
- slow thinking;
- pathological attention to minor events;
- obvious narrowing of the circle of interests.
Stage 2 is characterized not only by decreased ability to work (disability group II-III), but also by problems with the patient’s social adaptation. During the examination of the neurological status, vestibulo-cerebellar disorders, poverty and slowdown of active movements with a specific increase in muscle tone are revealed.
Signs of stage 3:
- thinking disorders progressing to dementia (dementia);
- tearfulness;
- sloppiness;
- epileptic seizures (not always);
- a pronounced decrease in self-criticism;
- pathological lack of will;
- weakening of sphincter control (involuntary urination and defecation);
- frequent drowsiness after eating.
Please note: for patients at this stage of development of the pathology, the Winscheid triad is very typical, i.e., a combination of memory impairment, headaches and episodes of dizziness.
Patients with stage 3 discirculatory encephalopathy are disabled; they are given disability group I.
Etiology (causes)
A powerful system of self-regulation of cerebral blood flow ensures excellent adaptation to labile environmental conditions.
During hypoxia, which is caused, for example, by acute bleeding, the flow of biological fluid into the central nervous system remains normal. In these situations, a powerful compensatory reaction is activated to force the centralization of this system, which is aimed, first of all, at increasing the blood supply to the circle of Willis (cerebral) and, as a consequence, maintaining normal circulation in general.
When hypoglycemia occurs, the body dilates the blood vessels that supply the brain. Because of this, the supply of glucose to the organ increases. But metabolic acidosis leads to an increase in blood outflow in order to quickly remove metabolic products from it.
With significant brain damage or insufficiency of regulatory mechanisms, hypercompensatory reactions occur. This causes a disruption in the regulation of blood flow in the vessels that supply biological fluid to the cranial cavity. Under such conditions, this area is a closed trap for the brain. Thus, even the slightest increase in the contents of the cranial cavity by at least 5% leads to profound disturbances in consciousness and the regulation of higher nervous activity.
Excessive blood filling of the cerebral vessels leads to hypersecretion of the choroid plexus of cerebrospinal fluid. As a result, compression of the brain occurs, edema develops, which leads to a disorder in the regulation of vital functions and the circulation of biological fluid in the vessels.
Traumatic compression of brain tissue, impaired blood supply, edema, increased pressure in the cranial cavity, changes in liquor dynamics (that is, circulation of cerebrospinal fluid) lead to significant disorders of the central nervous system. This is manifested, first of all, by clouding of consciousness.
Belkin A.A., Zislin B.D., Leiderman I.N., Domansky D.S.
Andrey Avgustovich Belkin, Doctor of Medical Sciences, Professor Director of the Clinical Institute of the Brain, SESC RAMS
Clinical Institute of the Brain, Scientific Research Center of the Russian Academy of Medical Sciences,
Clinic of Nervous Diseases and Neurosurgery of the Ural State Medical Academy,
Service of Nervous Diseases and Neurosurgery of City Clinical Hospital No. 40
Summary:
In connection with the introduction into clinical practice of a number of medical institutions of the concept of acute cerebral insufficiency syndrome, many questions arise regarding clinical interpretation and approaches to diagnosis, monitoring and treatment of patients who meet its criteria. Trying to find methodologically adequate solutions to this problem, neuroreanimatology specialists are conducting a comprehensive scientific development of reproducible methods of neuromonitoring and cerebrotropic intensive therapy. The theory of OCN is becoming the direction that determines scientific research in the development of new methods of intensive cerebrotropic therapy, as well as methods of neuroreparation and neuroprotection as components of complex pathogenetic therapy of neuropathological syndromes developing as a result of the formation of pathological systems. in response to the influence of pathological determinants.
Modern resuscitation is distinguished by the increasing pathophysiological validity of the used treatment and tactical approaches. Symptomatic therapy gives way to syndromic therapy, aimed at correcting the main systemic damage: acute respiratory, cardiovascular, hepatic, renal failure and sepsis. There remains less and less disagreement among resuscitators regarding clinical criteria, monitoring and treatment of these conditions. What about damage to the central nervous system? Is there a syndrome of acute cerebral insufficiency? In an Internet search engine, we found more than 30 citations mentioning “acute cerebral insufficiency,” which convinced us that resuscitators have intuitively already determined for themselves the clinical meaning of a condition for which there is currently no acceptable physiological basis. In other words, the status of the organ, which is the object of constant attention of the resuscitator, does not have an assessment methodology. This situation motivated us to try to find arguments in favor of recognizing the independence of acute cerebral insufficiency syndrome (ACI) and to formulate the principles of its intensive therapy.
At the present stage of development of resuscitation and intensive care, the dominant role of systemic inflammatory reactions in the formation of a critical condition of any etiology is generally recognized. Firstly, the post-aggressive reaction itself is a manifestation of SVR. Secondly, organ dysfunction occurs due to the progression of SVR. Thirdly, even focal ischemia as a variant of cerebral insufficiency occurs with symptoms of endothelial dysfunction, which also indicates a generalization of the inflammatory reaction in response to damage to the nervous system. More and more publications confirm the fact that acute cerebral damage is a manifestation of the classical post-aggressive reaction (SIRS- CARS-CHAOS) [3.6, 73.8, 3.11] (Fig. 1).
Picture 1
Modern scheme of the pathogenesis of a generalized inflammatory reaction [6]
We are interested in the pathogenesis of organ dysfunction. In this regard, the concept of the formation of pathological systems in the central nervous system (CNS) formulated by academician G.N. Kryzhanovsky can be considered the most productive [3.3]. In a condensed presentation, it looks like this (Fig. 2): as a result of damage to the central nervous system, loss of functions occurs through the mechanism of neural inhibition (focal ischemia) and (or) interruption of structural connections (concussion), the scale of which corresponds to the volume of damage. The high plasticity of the nervous system makes it possible to compensate for organ dysfunction of the central nervous system by activating reserve neural networks and redistributing functions according to a genetically determined algorithm. But adaptive mechanisms are not always rational. Not only “useful” neurons are activated, but also “aggregates of hyperactive neurons”, producing an increased, uncontrolled flow of impulses as a result of insufficiency of inhibitory mechanisms. By generating pathological excitation, they form a focus in the nervous system, defined as a pathological determinant (PD), which establishes a system of connections with the structures of the central nervous system. Thus, a pathological system (PS) is created, which determines the appearance of neuropathological syndromes based on neurochemical and molecular processes. When exposed to substances that directly disrupt inhibitory mechanisms (neurotropic poisons, pharmaceuticals), PS is primary. The formation of secondary PS occurs due to excessive accumulation of excitatory neurotransmitters (glutamate) as a result of extracerebral endotoxicosis (sepsis) or diffuse brain damage (traumatic brain injury). In this case, several PS can be formed that can develop self-sustaining activity without additional stimulation. Depending on the topical localization of the PS, it can have access to the periphery, while its “targets” are somatic organs, which is realized in the form of various manifestations of autonomic dysautonomia.
Figure 2
Pathological integrations in the central nervous system (according to G.G. Kryzhanovsky, 2003) [3]
Sanogenetic antipathological systems (SAS) and complex pathogenetic therapy (CPT) are capable of blocking the formation of PS at the stage of formation of a pathological determinant, which, with effective interaction, can completely prevent the development of a neuropathological syndrome (Fig. 2). CBT is a set of therapeutic measures aimed at stabilizing pathological systems by influencing their various links. Today, the main therapeutic measures are tied to neuropathological syndromes, which corresponds to the concept of syndromic treatment in intensive care. The development of scientific ideas about the pathogenesis of ACN contributes to the creation of treatment protocols that have a preventive focus on suppressing pathological determinants and the formation of PS. In other words, the closer the point of application of therapy is in the pathological determinant (Fig. 3), the lower the likelihood of developing a neuropathological syndrome. It is noteworthy that most treatment protocols are nothing more than a controlled model of natural antipathological sanogenetic systems (SAS), which in the optimal case increase or at least do not affect their effectiveness, in the unfavorable case they suppress their manifestations. The phenomenon of “miraculous” recovery of some patients who did not receive adequate intensive therapy becomes clear. There is no miracle. It’s just that in these patients the natural sanogenetic antipathological systems (SAS) turned out to be quite active.
Figure 3
Scheme of the formation of a neuropathological syndrome
Figure 4
Sanogenetic antipathological systems (SAS)
Thus, the SAS is a physiological element in the PS formation system, acting on the principle of “antisystem”, that is, carrying out antagonistic regulation aimed at preventing the development and suppressing the activity of existing pathological systems. Examples of SAS are shown in Figure 4. SAS should include well-known and clinically identifiable symptom complexes, the most striking of which is a coma, as the highest point of development of protective inhibition in response to the appearance of a pathological determinant in the form of a focus of hyperactive neurons. Another example is the increase in blood pressure and opening of collaterals in response to acute cerebral artery occlusion. On the one hand, there is a clear, specific version of protection against ischemia, on the other, the action of SAS, aimed at preventing the formation of ischemic stroke PS. The number of SAS is indefinitely large, therefore, in the SAS diagram (Fig. 3), we leave free space to continue the list of proven or hypothesized mechanisms of cerebral protection - SAS N.
For neuroreanimatology, the greatest interest is SAS 1, which we designated as a complex (system) of cerebral protection against ICH.
Figure 5
Stages of implementation of the cerebral protection system
Figure 6
Evolution of acute cerebral insufficiency
Let us briefly recall the main stages of the implementation of this protection system from the point of view of the SAS theory (Fig. 4). First of all, as a result of the resulting primary damage, a population of affected cells appears in the brain parenchyma in a state of cytotoxic edema due to impaired transmembrane transport of electrolytes (a pathological determinant is formed). Due to the increased volume, edematous cells have a compressive effect on neighboring cells, thereby causing a mass effect. This is how edema spreads to intact cells. The continued increase in the pathological volume causes compression of the capillary-pial bed. This disrupts microcirculation, causes hypoxia-ischemia in areas not directly related to the primary mass effect, and leads to pathological separation of various parts of the contents of the skull. As a result of the separation of these sections, the pressure created by the cerebrospinal fluid and the pulse fluctuations of the arteries can no longer spread freely along the tissues and spaces of the cerebrospinal fluid located inside the skull and spinal canal. A difference in parenchymal pressure occurs between the structures involved in edema and the intact structures, which initiates dislocation in the direction of lower pressure. The result of this process is diffuse cerebral edema and its displacement towards the only (if there is no trepanation defect) open exit from the cranial cavity - the foramen magnum. There, the final compression of the stem structures occurs, with the suppression of the primary centers of respiration and circulation and the cessation of brain activity. This is how the pathological system of intracranial hypertension is formed and develops. At each stage, it is counteracted by 5 elements of the cerebral defense system or SAS 1 (Fig. 4). The complex of compensation mechanisms is determined by the property of compliance (1-2 in Fig. 1), that is, the ability to adapt to an increase in the volume of the craniospinal system. The first response to the appearance and spread of additional volume is to use the elasticity reserve of the medulla and free spaces inside the cranium (1 in Fig. 4). The compliance of the craniospinal system (craniospinal compliance - Cc) is ensured by the correspondence between the production and resorption of cerebrospinal fluid (2 in Fig. 4). It is the predominance of resorption that makes it possible to free up additional spaces for the “swelling” brain, inhibiting the development of microcirculatory disorders. As the craniospinal compliance reserve is depleted, effective cerebral perfusion pressure (CPP) is achieved by increasing systemic pressure (3 in Fig. 5), which allows it to overcome the increased peripheral resistance to blood flow. The system of autoregulation of cerebral circulation counteracts this due to the reserve of vasodilation. If SAS and CPT fail, the perfusion pressure begins to decrease. In clinical conditions [3.1], we obtained evidence of the presence of all of the listed components with the exception of the last stage of SCS—increased O2 extraction. But according to the literature [3.2], it provides only a very short-term slowdown of the process of equalization of cerebral perfusion and mean arterial pressure, which is already slightly reversible and, most often leading to brain death. This is the nature of the action of SAS 1. In parallel with it, SAS 2 and 3 also operate. We do not have our own evidence confirming the participation of these systems in implementing the sanogenetic reaction of the body, but this theorizing quite logically follows from the concept of plasticity of the nervous system. While maintaining the viability of the organism, a period of formation of the pathological system of the subacute and residual period begins. If SAS 4 is sufficiently effective, the patient has a chance of recovery (Figure 6). It is necessary to emphasize once again that CBT can be positive only in case of synergy with SAS 1-4.
Figure 7
Neuropathological syndromes of ACN
Moving on to the clinical presentation of acute cerebral insufficiency syndrome, we should dwell on the neuropathological symptom complexes (Figure 7). The above classification is based on the principle of topical and functional implementation of the pathological system. Topical identification of the syndrome, based on classical neurological symptoms, makes it possible to localize the pathological determinant. Focal or diffuse manifestations clarify the nature of the process (structural or metabolic). The nature of the effect on the brain is assessed by the presence of symptoms of irritation or loss of function (for example: a hematoma causes irritation, and a heart attack causes loss of function). Determining the functional meaning of symptoms (motor, muscular-tonic, neurotransmitter and neurohumoral) is one of the key tasks of diagnosis and monitoring, as they determine the direction and activity of intensive care. We do not claim completeness of the above classification, but its clinical feasibility has been proven by our many years of experience.
Let's summarize some results. We believe that there is every reason to consider acute cerebral insufficiency an independent resuscitation syndrome.
Firstly, because it has a pathophysiological basis (pathogenesis): ACN is a polyetiological, but monopathogenetic process associated with the formation of pathological systems, the leading of which is intracranial hypertension (PS ICH) with variants of its evolution.
Secondly, ACN syndrome has a specific complex of neuropathological syndromes.
Thirdly, ACN syndrome has special, unique to it, principles of intensive therapy aimed at enhancing the action of sanogenetic antipathological systems.
Practical confirmation of the validity of these provisions is the actual implementation of the concept of acute cerebral insufficiency syndrome within the framework of the regional “intensive care” program, which has been operating in the Sverdlovsk region for 5 years. In the structure of the standard of intensive care for central nervous system (Fig. 7), several sections are distinguished:
· a tactics algorithm that describes the system of interaction between emergency care entities (ambulance, diagnostic services, neurosurgical departments, resuscitation and anesthesiology units) when providing step-by-step care to patients with ACN. The most important point of the algorithm should be noted: patients with ACN should be hospitalized in the RAO;
· therapeutic recommendations for the treatment of major neuropathological syndromes, based on international protocols and consensuses;
· drug formulary, including a minimum sufficient list of medications and consumables for the implementation of treatment recommendations, including for monitoring;
· scales for assessing the condition and outcomes - a set of classifications and scales necessary for a unified approach to the clinical assessment of the condition of patients with ACN.
An analysis of the activities of the resuscitation and anesthesiology service in the Sverdlovsk region [12] showed that the introduction of the standard significantly improved the rates of treatment of patients with cerebral damage, especially with traumatic brain injury.
Figure 8
Structure of the regional standard for intensive care of the central nervous system
Table 1
| Nosological forms of neuroresuscitation pathology in 2005 | Postoperative | Conservative | TOTAL | Ud. weight, % | USA, A.Rooper% |
| Intracranial arterial aneurysms of cerebral vessels (IAC) | 147 | 55 | 192 | 15 | 13 |
| AVM | 6 | 3 | 9 | 0,7 | 2 |
| Occlusive cerebrovascular diseases | 19 | 5 | 24 | 1,9 | |
| Acute traumatic brain injury | 104 | 33 | 137 | 11 | 11 |
| Spinal cord injury | 6 | 4 | 10 | 0,8 | 3 |
| Ischemic stroke | 0 | 115 | 115 | 9 | 18 |
| Hemorrhagic stroke | 0 | 8 | 8 | 0,6 | 7 |
| Post-resuscitation illness | 1 | 3 | 4 | 0,3 | 4 |
| Convulsive syndrome (epistatus) | 0 | 0 | 1 | 0,00 | 3 |
| Myasthenic condition | 0 | 2 | 2 | 0,2 | 4 |
| Encephalomyelopolyradiculoneuropathy (EP) | 0 | 0 | 0 | 0 | 6 |
| Meningitis/meningoencephalitis | 0 | 3 | 3 | 0,2 | 2 |
| Tumors of the pituitary gland and pituitary-sellar region, chiasm and optic nerves, bottom of the 3rd ventricle | 71 | 1 | 72 | 34 | 25 |
| Tumors of the base of the skull | 25 | 1 | 26 | ||
| Intracerebral tumors of supratentorial localization | 215 | 7 | 222 | ||
| Intracerebral tumors of subtentorial localization | 112 | 7 | 119 | ||
| Spinal cord tumors | 53 | 1 | 54 | ||
| Occlusive lesions of the cerebrospinal fluid pathways of the brain | 89 | 4 | 93 | 7,3 | |
| Functional neurosurgery, epilepsy | 17 | 2 | 19 | 1,5 | |
| Neurosurgery of inflammatory lesions of the brain, skull, spinal cord, spine | 9 | 7 | 16 | 1,3 | |
| Degenerative lesions of the spine | 122 | 1 | 123 | 13 | 2 |
| Consequences of traumatic damage to the peripheral nervous system | 20 | 0 | 20 | ||
| Trigeminal neuralgia | 14 | 0 | 14 |
Another important argument in favor of the legitimacy of the existence of the ACN syndrome can be recognized by the fact of the presence of specialized neuro-resuscitation departments. The patient population of these departments is united by the homogeneity of nosological forms and the possibility of widespread use of uniform protocols. The feasibility of establishing such branches has been proven in different countries. Although there are significant differences in the organizational aspects of the work of these departments, there is a similarity in the nomenclature of nosologies. Table 1 shows the structure of patients treated in the neuroreanimation department of the City Clinical Hospital No. 40 of Yekaterinburg and the University Hospital of Boston (USA) [3.4]. The existing differences relate mainly only to the nomenclature of neurosurgical operations performed in these hospitals.
CONCLUSIONS
1. The existence of a pathophysiological model of acute cerebral insufficiency, a reproducible standard of therapeutic, diagnostic, and tactical actions make it possible to recognize the classification of ACUTE CEREBRAL INSUFFICIENCY (ACI) syndrome along with other resuscitation syndromes (ADN, AHF, ARF, etc.) as legitimate.
2. The theory of OCN is becoming the direction that determines scientific research in the development of new methods of intensive cerebrotropic therapy, as well as methods of neuroreparation and neuroprotection (stem cell therapy) as components of complex pathogenetic therapy of neuropathological syndromes developing as a result of the formation of pathological systems. in response to the influence of pathological determinants.
3. Familiarity with the basics of neuroreanimatology should be included in the training program for neurologists, neurosurgeons and general resuscitators.
Literature
1. Belkin A.A. Pathogenetic understanding of the cerebral protection system in intracranial hypertension and the ways of its clinical implementation in patients with acute cerebral insufficiency. Intensive Care, 2005, no.1.
2. Plum F., Posner D. Diagnosis of stupor and coma. Moscow, M., 1986, pp. 148-155.
3. Kryzhanovsky G.N. Pathological integrations in the central nervous system. Brain. Theoretical and clinical aspects. Medicine, M., 2003, pp. 52-67.
4. A. Rooper. Neurological and Neurosurgical Intensive Care. Lippincott Williams, 2004. 391p.
5. Chereshnev V.A., Gusev E.Yu., Yurchenko L.N. Systemic inflammation as a typical pathological phenomenon - myth or reality? Bulletin of the Russian Academy of Sciences, No. 3, 2004, p. 18-23.
6. Bone R.S. Toward a theory regarding the pathogenesis of the systemic inflammatory response syndrome: what we do and do not know about cytokine regulation // Critical Care Medicine. - 1996. - V. 24 - N 1 - P. 163-72.
7. Bone RC Sir Isaac Newton, sepsis, SIRS, and CARS. Crit. Care Med. 1996; 245:1125–1128.
8. Bucci MN. Elevated intracranial pressure associated with hypermetabolism in isolated head trauma Acta Neurochir (Wien). - 1988. - N 93. - P. 133-136.
9. Hill AG. Initiators and propagators of the metabolic response to injury World J Surg. - 2000. -Vol. 24, N 6. -P.624-629.
10. Ott M., Schmidt J., Young B. Nutritional and metabolic variables correlate with amino acid forearm flux in patients with severe head injury. Crit Care Med. - 1994. - Vol 22. - P. 393.
11. Rixen D., Siegel JH, Friedman HP “Sepsis\SIRS”, physiologic classification, severity stratification, relation to cytokine elaboration and outcome prediction in posttrauma clinical illness. Journal of Trauma. - 1996. - Vol 41, N 4. - P. 581-598/
12. Levit A.L. Organization of the work of the resuscitation and anesthesiology service in the Sverdlovsk region in the 21st century. Problems solved and unresolved. Intensive Care, 2005, ? 1, p. 23-27.
Pediatric cerebral insufficiency
Causes of the disease in children:
- placental abruption, which eventually leads to intrauterine fetal hypoxia;
- severe infectious diseases during pregnancy certainly affect the normal development of the embryo;
- psycho-emotional overload of the mother;
- unfavorable environmental situation in the country;
- unbalanced diet;
- bad habits;
- infectious diseases in childhood;
- influence of radiation (ionizing radiation);
- hemolytic disease of newborns;
- anesthesia, which is mandatory for caesarean section;
- intrapartum trauma;
- traumatic brain injury;
- sedentary lifestyle and physical inactivity;
- premature birth.
Measures for the treatment and prevention of CNMK
When identifying the first symptoms of chronic cerebral ischemia, it is strongly recommended to periodically carry out a comprehensive course of treatment. It is necessary to prevent or slow down the development of pathological changes.
Primary prevention of CNM is within the competence of general practitioners - family doctors and local therapists. They must carry out explanatory work among the population.
Basic preventive measures:
- maintaining a normal diet;
- making adjustments to the diet (reducing the amount of carbohydrates and fatty foods);
- timely treatment of chronic diseases;
- rejection of bad habits;
- regulation of work schedule, as well as sleep and rest;
- combating psycho-emotional stress (stress);
- active lifestyle (with dosed physical activity).
Important: primary prevention of pathology should begin in adolescence. Its main focus is eliminating risk factors. It is necessary to avoid overeating, physical inactivity and stress. Secondary prevention is needed to prevent episodes of acute cerebral blood flow disorders in patients with diagnosed chronic ischemia.
Treatment of vascular insufficiency involves rational pharmacotherapy. All medications should be prescribed only by a local doctor or specialist, taking into account the general condition and individual characteristics of the patient’s body.
Patients are advised to take a course of vasoactive drugs (Cinnarizine, Cavinton, Vinpocetine), antisclerotic drugs and antiplatelet agents to reduce blood viscosity (Acetylsalicylic acid, Aspirin, Curantil, etc.). Additionally, antihypoxants are prescribed (to combat oxygen deprivation of brain tissue), nootropics and vitamin complexes (including vitamins E and B). The patient is recommended to take neuroprotective drugs that contain amino acid complexes (Cortexin, Actovegin, Glycine). To combat certain secondary disorders of the central nervous system, the doctor may prescribe drugs from the group of tranquilizers.
Important: antihypertensive therapy is of great importance to maintain blood pressure levels at the level of 150-140/80 mm Hg.
It is often necessary to select additional combinations of drugs if the patient is diagnosed with atherosclerosis, hypertension and (or) coronary insufficiency. Making certain changes to the standard treatment regimen is necessary for diseases of the endocrine system and metabolic disorders - diabetes mellitus, thyrotoxicosis and obesity. Both the attending physician and the patient must remember: the medications should be taken in full courses, and after a break of 1-1.5 weeks, begin a course of another medication. If there is an obvious need to use different drugs on the same day, it is important to maintain a time interval of at least half an hour between doses. Otherwise, their therapeutic activity may decrease, and the likelihood of developing side effects (including allergic reactions) may increase.
People who have clinical signs of cerebrovascular insufficiency are advised to refrain from visiting baths and saunas to avoid overheating of the body. It is also advisable to reduce your time in the sun. Climbing into the mountains and staying in areas at an altitude of over 1000 m above sea level poses a certain danger. It is necessary to completely abandon nicotine, and reduce the consumption of alcohol-containing drinks to a minimum (no more than 30 ml of “absolute alcohol” per day). The consumption of strong tea and coffee should be reduced to 2 cups (approximately 100-150 ml) per day. Excessive physical activity is unacceptable. You should not sit in front of a TV or PC monitor for more than 1-1.5 hours.
Plisov Vladimir, medical observer
16, total, today
( 165 votes, average: 4.47 out of 5)
Hemorrhagic stroke: treatment, consequences and prognosis
Lumbago: symptoms and treatment
Related Posts
Pathogenesis
The main pathogenetic factors in the development of this pathology include:
- intrapartum trauma;
- intrauterine infections;
- hypoxia during the intrapartum period.
Since the thinking organ needs a large amount of oxygen, a slight deficiency can cause massive damage to the nervous tissue. The consequences of intra- and perinatal pathology may be delayed cerebral edema. As well as vegetative-vascular dystonia and cerebral insufficiency. The latter, in fact, is also a delayed manifestation of organic brain damage.
Causes of residual cerebral organic failure
In essence, residual RCN is a pathology that represents residual effects from damage to the nervous system in
perinatal labor or infancy
Researchers note that the risk of giving birth to a child with residual cerebral organic insufficiency increases in older women in labor. There may be several reasons for the development of this pathology
And, as a rule, this disease is formed under the influence of a whole complex of these factors.
Placental abruption during pregnancy and, as a consequence, intrauterine damage to the fetal brain Severe viral and infectious diseases suffered by a woman during the perinatal period Unstable emotional state of the expectant mother - stress, depression, hysterics, fears, etc. Unwanted pregnancy Unsuccessful attempt by the expectant mother to have an abortion Unhealthy lifestyle that the woman led while expecting a child - smoking, use of alcohol and drugs Exposure to radiation and unfavorable environmental conditions Various chemical damage to the body of a woman and child, including potent drugs Abuse of untested biological drugs active food additives Poor nutrition of a pregnant woman Sedentary lifestyle and lack of adequate physical activity Limiting the intake of fresh, clean air into the body of the mother and child The birth of a child before the due date - prematurity Immunological incompatibility of mother and child, Rh conflict General anesthesia received by a woman and baby during pregnancy during a cesarean section Various birth injuries resulting from drug-induced, prematurely induced or ill-conducted childbirth Mechanical head injuries received by a child in early childhood All kinds of infectious diseases in early childhood
Clinical symptoms of residual cerebral insufficiency in children
With this disorder, various conditions can be observed. Astheno-vegetative syndrome is manifested by the following clinical symptoms:
- fast fatiguability;
- lethargy;
- drowsiness;
- weakness;
- headache.
Nervous tics:
- The patient experiences involuntary movements.
Violation of autonomic regulation:
- excessive sweating due to a malfunction of the sweat glands of the feet and palms;
- disturbances in the regulation of blood flow in the terminal sections of the cardiovascular system.
Weather dependence (i.e. strong dependence of a person’s physical condition on weather conditions and time of year):
- possible loss of consciousness;
- tachycardia (acceleration of heartbeat);
- change in blood pressure.
Vestibular disorders:
- nausea, which in extreme cases leads to vomiting;
- motion sickness in transport and on swings.
Lability of the human psycho-emotional sphere:
- mild irritability;
- lability of mood (frequent changes);
- capriciousness.
Photophobia (intolerance to bright light).
Motor activity disorders. As a rule, it manifests itself in two contradictory syndromes. The first arises as a result of the predominance of inhibition processes in the brain. The second is a consequence of excessive activation, which leads to inadequate functioning of the structures responsible for maintaining attention (these are structures such as the thalamus).
Also, with residual organic cerebral insufficiency, inhibition is characteristic:
- it is difficult to motivate such children to do any work;
- if they do agree to complete tasks, they do it very slowly;
- They have difficulty switching between different tasks at the same time.
Or hyperactivity:
- children experience great difficulty maintaining attention;
- They are characterized by strong restlessness, even to the point of ADHD (attention deficit hyperactivity disorder).
Acute and chronic forms
It is typical for ischemic brain damage that the acute and chronic variants of the course can alternate with each other. Ischemic stroke and transient attack often occur against the background of encephalopathy. A sharp disruption of blood circulation causes changes in the brain, only some of them end in the acute period.
Most neurological manifestations remain for a long period or for the rest of life. They develop into chronic cerebrovascular insufficiency.
The post-stroke period is characterized by the following processes in the brain:
- the blood-brain barrier is damaged;
- microcirculation is disrupted;
- the protective function of the immune system decreases;
- the ability to resist cell damage (antioxidant protection) is depleted;
- the vascular endothelium does not prevent the formation of new cholesterol plaques, and the old ones also grow;
- increased blood clotting is noted;
- secondary metabolic disorders appear.
All these factors increase cerebral ischemia that was present before the stroke, and the progression of cerebrovascular insufficiency, in turn, leads to recurrent strokes and dementia.
Diagnostics
As practice shows, to make a final diagnosis there are few positive clinical symptoms; it is recommended to conduct additional laboratory and instrumental examinations.
Among them are:
- measurement of intracranial pressure (with this pathology the indicator will be increased);
- echoencephalography;
- electroencephalogram (to determine convulsive readiness);
- ophthalmoscopy.
Symptoms of cerebrasthenic syndrome in children
It is important for parents to know that RCON is a diagnosis by a neurologist, which is made mainly in the first months of a child’s life. In this regard, if alarming signs appear, it is necessary to show the baby to a specialist.
Clinical manifestations of pathology:
- Irritability.
- Moodiness.
- Frequent mood changes.
- Increased degree of fatigue.
- Restless sleep.
- Grinding of teeth.
- Passivity.
- Meteor dependence.
- Tremor.
- Increased sensitivity to bright lights and loud sounds.
- Nausea and vomiting while traveling on any type of transport.
- Cold extremities.
- Deformations of the skull, including a protruding upper jaw.
Neurologists often attribute asthenoneurotic syndrome to the diagnosis of “RCON”. What is this? In this case, it is customary to say that, due to pathology, the child has lost the ability to endure prolonged mental or physical stress. There are also a number of syndromes characteristic of RCON: cerebroasthenic (weakness, increased fatigue), neurosis-like (development of phobias and enuresis), hyperactivity, encephalopathy (memory impairment, sleep disturbances), psychopathy (aggression, antisocial behavior).
Cerebroasthenia is manifested by physical weakness, fatigue, drowsiness, and autonomic dysfunction. Infants are restless, often cry, sleep a lot during the day, and are awake at night. Decreased appetite, slow weight gain, general developmental delay. Young children have decreased interest in toys. They do not like outdoor games and do not adapt well to unfamiliar surroundings. With stuffiness, heat, cold, sharp sounds, the state of health worsens, the child asks to be held and is capricious. Doesn't like trips, rides or swings.
READ MORE: How to identify a concussion at home. How to check for a concussion - diagnosis
Preschool children are anxious and have fears (of the dark, monsters, heights). Frequent symptoms are nocturnal enuresis, weather dependence, excessive sweating or chilliness. Emotions are labile and unstable - patients get upset easily, cry, get angry, and quickly calm down. They rarely take part in games and are not inquisitive enough. Stressful situations lead to functional physiological disorders - vomiting, diarrhea, rapid heartbeat, dizziness.
Schoolchildren continue to have symptoms of physical illness, and signs of cognitive deficits become more pronounced. Inattention, decreased stability of attention, and inability to remember educational material are noted. During writing lessons, the child misses letters, swaps them, does not have time to take dictation, and asks again. When giving oral answers, he has difficulty constructing a monologue, takes a long time to find the right words, and remembers information. The daily dynamics of performance are noticeable: lessons are much easier in the morning, and exhaustion sets in in the evening.
Treatment
The following treatment regimens are the result of many years of world practice in the treatment of this type of pathology.
According to modern protocols, treatment of cerebral insufficiency should be carried out in two main directions. This is a general strengthening therapy and a local effect on pathologies directly in the brain.
Such treatment for chronic and acute cerebral insufficiency syndrome includes:
- normalization of hemodynamics;
- restoration of normal respiratory activity;
- normalization of metabolic processes;
- local effect on pathology:
- restoration of normal functioning of the BBB (blood-brain barrier);
- increased hemodynamics in the brain;
- treatment of edema.
According to modern standards, the main treatment for cerebral edema is the administration of the following drugs:
- osmodiuretics;
- saluretics;
- glucocorticoids.
As practice shows, taking one of the above groups of drugs in monotherapy does not provide a significant clinical effect, so treatment must be combined.
Also, the use of bioflavonoids at the prehospital stage greatly increases the effectiveness of further therapy, since they influence a significant number of links in the pathobiochemical process of the development of this pathology.
The following drugs are widely used in modern clinical practice:
- "Troxevasin";
- "Venoruton";
- "Corvitin";
- "Escuzan";
- "L-lysine aescinate."
To improve the rheological properties of blood in the cerebral circle, patients are recommended to take anticoagulants under the control of the prothrombin index. This group of drugs is especially effective for cerebral insufficiency, which arises as a result of impaired venous outflow.
Infusion therapy is mandatory when this pathology occurs due to an acute decrease in circulating blood volume. In a situation where the cause of the disease is acute intoxication, detoxification therapy is considered a necessary measure. As a rule, the following solutions are used for these purposes:
- "Trisol";
- "Reosorbilact";
- "Acesol".
Acute cardiovascular failure
Acute cardiovascular failure is a sharp decrease in the frequency of heart muscle beats, resulting in a drop in blood pressure in the vessels and impaired circulation of the lungs and heart.
A common cause of this condition is myocardial infarction. Other causes of the disease include inflammation of the heart muscle (myocarditis), heart surgery, pathologies of the valves or chambers of the organ, stroke, brain injury, and more. Classification of heart failure according to ICD10 – I50.
Acute cardiovascular failure is accompanied by many unpleasant symptoms
There are failures of the left and right ventricles of the heart. In the first case, the following symptoms are noted:
- shortness of breath - from minor breathing difficulties to suffocation;
- discharge from the upper respiratory tract in the form of foam, accompanied by a strong cough;
- wheezing in the lungs.
The patient is forced into a sitting or semi-sitting position, with his legs lowered down.
Clinical picture of right ventricular failure:
- swelling of the veins in the neck;
- bluish coloring of the fingers, limbs, ears, chin, tip of the nose;
- the skin acquires a slight yellowish tint;
- the liver enlarges;
- mild or severe swelling occurs.
Intensive therapy for acute cardiovascular failure is carried out in a hospital setting. If the cause of the disease is an abnormal heart rhythm, medical measures are aimed at restoring it. In the case of myocardial infarction, therapy involves restoring blood flow in the affected artery. For this purpose, thrombolytic drugs are used. These medications dissolve blood clots, thereby restoring blood flow. In case of myocardial rupture or damage to the heart valves, the patient requires urgent hospitalization followed by surgical treatment and care.
What is recommended
It is necessary to create social conditions in which the patient will feel as comfortable as possible. The following components must be included in the complex of rehabilitation measures:
- drug therapy;
- Exercise therapy (therapeutic physical culture);
- occupational therapy.
When diagnosing delayed complications of cerebral insufficiency, it is imperative to create living conditions in which the patient does not feel limited.
Rehabilitation in children is much easier and more effective due to their high level of regenerative processes and significant opportunities for neuroplasticity. Therefore, as a rule, they do not experience delayed complications.
Residual cerebral organic failure treatment
Naturally, the elimination of this pathology should be carried out comprehensively. Official medicine advises prescribing drug treatment for a child with such a diagnosis. In addition, teachers should work with the little patient. However, the main role in getting rid of the disease should be played by the parents of a special child
We offer you to use a proven, effective and natural method of treating various neurological disorders, including residual cerebral organic insufficiency
See also:
Treatment of autism in children. Autism. Recovery method
Find out more about free recovery programs for RCN or RCN, autism, cerebral palsy and epilepsy based on the principles of biomed and naturopathy with a diet that includes natural products Tentorium
Seminar plan HERETentorium beekeeping products restore every cell of the body naturally according to the principles of biomedical correction of the body
They saturate the body with necessary enzymes, vitamins and microelements
Disclaimer The information provided in this article is for the reader's information only. It is not intended to be a substitute for advice from a medical professional