- What kind of pathology is this and why is it dangerous?
- Causes and symptoms of rheumatic endocarditis
- Classifications of pathology
- How is it diagnosed?
- Treatment
With rheumatism, rheumatoid endocarditis can develop, which is a consequence of an inflammatory process that affects the connective tissue of the heart valves and chordae tendineae. The disease often leads to the formation and development of heart disease. To prevent such complications, pathology must be identified and treated in a timely manner.
Characteristics of the pathology
Rheumatic endocarditis mainly progresses in the valvular apparatus of the myocardium. Over time, the pathology can spread to the chordal filaments and the parietal endocardium of the ventricles or atria. This disease belongs to rheumatism syndromes. Endocarditis, if not treated promptly, during scarring can change the appearance of the valve, disfiguring it for the worse. In this case, problems may arise with closing the special hole, which leads to valve insufficiency, that is, blood circulation becomes more difficult. Subsequently, such a pathology can cause stenosis of the orifice, which also negatively affects the full flow of blood.
The rheumatoid process very often leads to shortening of the tendon threads, which also ends in valve insufficiency. The narrowing of the openings is mainly a consequence of the fusion of individual leaflets or valves. Experts have found that endocarditis is always accompanied by similar myocarditis.
Rheumatic endocarditis is one of the most common heart diseases; only congenital myocardial defects are more common.
Types of disease
Experts divide the disease into 4 types:
- Acute warty endocarditis. In this case, the deep layers of the endothelium are affected. Gray-brown formations, similar to warts, begin to appear on certain areas of the organ. If therapy is not started in time, these formations become larger and merge with each other, which leads to the occurrence of polypous endocarditis.
- Recurrent wart. This type of endocarditis differs from the previous one in that it progresses on valves affected by sclerosis.
- Simple endocarditis is characterized by tissue swelling and does not have deep lesions. Timely therapy guarantees rapid recovery of the myocardium and its structures without complications and consequences.
- Fibroplastic endocarditis is a consequence of any of the above types of diseases that were not treated in time. In this case, complications and negative consequences are possible.
Fibroplastic, simple, recurrent and acute wart endocarditis are diseases that require only diagnosis from a specialist and do not accept self-medication.
In patients over 30 years of age, the valves are damaged in 30% of cases after a rheumatic attack on the heart, and in children - in 90%.
Complications
Endocarditis can lead to damage to the heart valves, conduction problems, and heart failure.
Neoplasms that occur with endocarditis can break off and move with the bloodstream throughout the body. This can lead to blockage of blood vessels and organ death.
Heart valve affected by infection.
The prognosis of endocarditis is often serious. Complete healing is achieved only with the earliest possible recognition of the disease and precisely selected effective treatment. Broad-spectrum antibiotics greatly improve the chances of rapid healing.
Read also: Endocarditis classification
No doctor can guarantee to prevent a possible relapse of the disease, which can develop within four weeks after stopping therapy.
In the long term, the chances of endocarditis returning are high, so you need to constantly undergo medical examinations and identify the disease at the earliest stage.
What is the basis of pathology
Streptococcus bacteria are the cause of the disease
The main and main cause of rheumatic endocarditis is group A streptococcus. This is especially a common manifestation of endocarditis in children, since they can get tonsillitis or pharyngitis, if treatment is not started in time, the disease can cause serious complications.
To cope with the infection on its own, the body begins to actively produce antibodies that can attack the cardiovascular system, which causes an inflammatory process and leads to rheumatism.
The parts of the heart affected by the disease include:
- Tendon chords.
- Aortic valve.
- Deep layers of the heart.
- Mitral valve.
- Parietal endocardium.
- Tricuspid valve.
In this regard, rheumatic inflammation of the heart tissue proceeds differently than the infectious and septic varieties of the disease, but the main cause is still streptococcus that has entered the body.
Prevention measures
Inflammation of the inner lining of the heart can be prevented with certain measures. Since rheumatism is the result of infection with certain bacteria - beta-hemolytic A-streptococci - in order to prevent endocarditis, appropriate treatment of infections - tonsillitis and pharyngitis is in any case important.
If antibiotics are prescribed, it is recommended that you take them as prescribed and do not stop therapy prematurely once symptoms subside. Anyone who has had rheumatic or post-infectious endocarditis can prevent it from recurring by taking antibiotics for more than 10 years.
Penicillin is then taken to prevent streptococcal infections before any procedure in which streptococci may enter the bloodstream, such as surgery or dental work. It is also recommended to lead a healthy lifestyle - drink enough fluids, eat a balanced diet and exercise.
Andrey Yurievich
Clinical picture as a fact
Endocarditis very often begins completely unexpectedly and may not manifest itself for a long time. In most cases, the disease is long-term and acute, has different types of manifestations, which very often complicates diagnosis.
When the body becomes very weak, you should immediately see a specialist!
Over the course of two weeks, the clinical picture of the disease develops, at which time the patient notices fever, chills and excessive sweating. Body temperature constantly changes its values; it can be quite high for a long time and slightly elevated for several days, followed by normalization. During endocarditis, the following symptoms are noted:
- Decreased appetite, red eyes.
- Muscle, chest, abdominal and joint pain.
- Arthritis of the joints of all extremities and visible changes in the phalanges of the fingers and nails.
- Progressive heart failure, heart murmurs.
- Renal dysfunction caused by nephritis or heart attack.
- Enlarged lymph nodes and damage to the central nervous system.
- Pericarditis, damage to the aortic or mitral valve.
- Increased heart rate, arrhythmia and increased heart rate.
Intoxication of the body is noted: loss of strength, decreased performance, weight loss, anorexia, headaches, arthralgia. Changes that appear on the skin are hemorrhagic rashes, redness on the palms of the hands, soles of the feet and body, pale skin with yellowing.
The consequences of the disease depend on its course and what form the pathology is in. Experts include children under 7 years of age, adolescents and older people who have had infectious diseases at risk.
Read also: ICD 10 infective endocarditis
Symptoms
Symptoms of endocarditis are always based on the cause of the disease. The first warning sign of endocarditis is fever. It can be confusing and chaotic - the temperature rises and falls, you do not see the external reasons for the change in temperature and you do not know whether to fight to lower or increase it.
With syphilis and tuberculosis, the appearance of endocarditis is not manifested by fever, and the temperature is unlikely to cause concern - it usually rises only to 37.5 degrees.
A striking symptom is a change in skin color to a “café au lait” shade, but less commonly the shade can be pale or sallow. Such changes scare people enough to see a doctor.
Most likely, symptoms appear only a week or two after infection, but powerful strains of infection can cause a more rapid development of the disease and its severe course. The first signs may resemble regular flu or ARVI - high fever, weakness, chills.
Symptoms of endocarditis may be similar to signs of blood poisoning. If pathogens accumulate on the heart valves, inflammation occurs. The cause of the infectious agent can be purulent otitis media, sinusitis, cystitis, salpingo-oophoritis.
Palms of a patient with infective endocarditis.
Possible symptoms of endocarditis:
- fever;
- sweating, especially at night;
- weight loss;
- muscle or joint pain;
- severe coughing attacks;
- dyspnea;
- hemorrhages under the nails and skin (spots - petechiae), on the mucous membranes, fundus of the eye;
- painful thickening of the fingertips (Osler's nodes);
- skin rashes.
In addition to signs of sepsis, the disease is characterized by severe intoxication with headaches, enlargement of the spleen and liver. Blood tests reveal leukocytosis, anemia, and elevated ESR. Bacterial emboli of various organs with the formation of purulent metastases may be observed.
Heart sounds are muffled, new heart murmurs are added, and arrhythmia begins. If the infection is not eliminated in time, endocarditis takes on the characteristics of acute heart failure.
Note that high fever, nausea, aches and pains in the muscles and some other symptoms may be absent. However, diagnosing the disease is not difficult - a blood test is used, since infectious agents are found in arterial blood.
What does the outcome depend on?
Before you find out what the outcome of rheumatic endocarditis depends on, you need to understand what this pathology is. Pathological disorders are localized in the myocardial valves at the initial stages of development, and as they progress, they spread to the atrium ventricles (the region of the parietal endocardium) and chordal filaments. The disease is a rheumatism syndrome that appears against the background of infection. Over time, tissue scarring occurs, which leads to deformation of the valve. In this case, the hole is blocked, organ failure occurs, and blood circulation is disrupted. There is a risk of developing stenosis. Next, the tendon threads begin to shorten, and the flaps or valve fuse.
Why is this happening? The fact is that at the very beginning of the development of pathology, collagen fibers undergo swelling, which causes a proliferative reaction. This leads to a change in the surface of the valve, and in places where the valves touch, fibrins and platelets accumulate and settle. As a result, warty growths are formed. Under these warts, swelling of the tissue occurs, leading to scarring.
The prognosis largely depends on the symptoms that appear, which may indicate certain pathological changes. The patient may experience the following:
- increased heart rate;
- pain in the heart area;
- acceleration of pulsation;
- shortness of breath and impaired breathing abilities;
- weakness and fatigue;
- high body temperature;
- diastolic, protodiastolic and systolic murmurs.
If the body of such a patient is examined, atrioventricular blockade and friction noise of such an element as the pericardium are detected. To do this, it is enough to do an electrocardiogram.
Loeffler's endocarditis
Lasts 5-6 weeks, inflammatory changes affect the ventricles and apex of the heart muscle. Foci of dead cells appear with an accumulation of eosinophils, lymphocytes and plasma cells. Similar changes can be observed in the vessels of internal organs and skin.
Thrombotic;
Blood clots of various sizes form on the endocardium of the left ventricle; in some cases, this can also be observed in the right parts. There is a gradual thickening of the endocardium with the formation of a zone rich in vessels and various blood cells. In this case, one part of the muscle fibers hypertrophies, while the other, on the contrary, atrophies. Focal sclerosis develops and young connective tissue grows.
In adults
If rheumatic endocarditis progresses and there is no adequate treatment, pathological disorders affect not only the cardiovascular system, but also other internal organs. But it is known that the main cause of this disease is infection with streptococci from group A. Consequently, infection of the entire body is possible. Therefore, it is not surprising that such a complication as valvulitis is discovered.
During the course of the disease, the erythrocyte sedimentation rate increases, and leukocytosis becomes moderate. After therapy aimed at restoring these processes, the patient is cured of endocarditis, but the defect still remains in the valve mechanism of the heart.
If the treatment of rheumatic endocarditis was not carried out in a timely manner, or the patient simply did not complete treatment, secondary endocarditis (recurrent) occurs in the future. If we talk about the clinical picture, it does not differ from the primary manifestation of the pathology, but is aggravated by the fact that the joints begin to be affected, which is why severe pain appears in them.
The most common outcomes of rheumatic endocarditis in the adult population:
- Congestive heart failure (HF) develops due to valvular incompetence. If the mitral and aortic valves are affected, and an acute and subacute course of the pathology is noted, then congestive heart failure develops very rapidly. This outcome is observed in 55-60 percent.
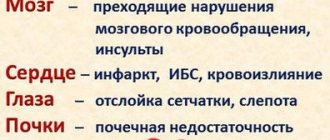
- Embolism occurs in 40% of all cases of rheumatic endocarditis. The blood vessels of the brain, kidneys, spleen, retina of the visual apparatus, and mesentery are affected. As a result, partial or complete blindness, stroke and heart attack, kidney failure, and acute abdominal syndrome occur.
- 25% is given to diseases of an autoimmune nature - allergic myocarditis, pericarditis, glomerulonephritis, inflammatory pathologies of the joints, effusions in the joint capsules.
- In only 10 percent, peripheral arteries are affected, resulting in an aneurysm in the vessels of the brain. And this is fraught with bleeding, ruptures and death.
Pediatric endocarditis is considered a dangerous condition because it is difficult to treat. Children get sick much more often than adults because their immune system is not yet fully developed. Because of this, the body is exposed to colds and infections, against which rheumatic endocarditis develops.
Early diagnosis is complicated by the fact that the main symptoms are similar to those of many other pathologies. In preschool age, healthy valves are most affected, and in older age, heart disease is also detected.
As a rule, such children are constantly monitored by doctors. In addition, they must periodically undergo prophylaxis.
If we talk about the recovery rate in childhood, it is a minimum of 35-40%, and a maximum of 85. This depends on the severity of the disease, the type of infection and many other factors. If treatment is not started in a timely manner or the wrong drugs are used, the prognosis will be worse. Therefore, it is strictly forbidden to engage in independent therapy. In this case, you need to completely rely on the opinion of doctors.
Read also: Infective endocarditis in children
Diseases of the circulatory system in children
- In rheumatism in children, tissue is predominantly affected
a) epithelial
b) connecting
c) muscular
d) nervous
- Rheumatism most often develops in children aged (years)
a) 1–3
b) 3–6
c) 7–15
d) 15–17
- In rheumatism in children, the system is predominantly affected
a) cardiovascular
b) respiratory
c) digestive
d) musculoskeletal
- The leading role in the development of rheumatism in children belongs to
a) Escherichia coli
b) Pseudomonas aeruginosa
c) Staphylococcus aureus
d) -hemolytic streptococcus group A
- Damage to the nervous system in rheumatism in children is manifested by the development of:
a) anular erythema
b) spasmophilia
c) eclampsia
d) chorea
- With rheumatism in children, it appears on the skin
a) anular erythema
b) acrocyanosis
c) jaundice
d) pinpoint rash
- The leading clinical symptom of rheumatic myocarditis in children
a) weakness
b) loss of appetite
c) malaise
d) pain in the heart area
- Outcome of rheumatic endocarditis in children
a) malnutrition
b) rickets
c) heart defect
d) spasmophilia
- Rheumatic chorea in children manifests itself
a) grimacing
b) laryngospasm
c) pyloric stenosis
d) suffocation
- Rheumatic arthritis in children is characterized by damage to:
a) joints of the spine
b) small joints of the limbs
c) large joints of the limbs
d) costosternal joints
- For rheumatism in children, a biochemical blood test determines
a) increased cholesterol
b) lower cholesterol
c) the appearance of antistreptolysin-O
d) decrease in fibrinogen
- Etiotropic therapy for rheumatism in children - use of drugs
a) antibacterial
b) hypotensive
c) diuretic
d) anti-inflammatory
- Secondary prevention of rheumatism in children is carried out
a) bicillin-5
b) diphenhydramine
c) biseptol
d) korglykon
- The most common cause of non-rheumatic carditis in children
a) bacteria
b) viruses
c) hypothermia
d) overheating
- In rheumatic endocarditis in children, the heart valve is most often affected
a) aortic
b) mitral
c) pulmonary
d) tricuspid
- Of great importance in diagnosing heart defects in children is
a) general blood test
b) biochemical blood test
c) ultrasound examination of the heart
d) bicycle ergometry
- Congenital heart defects include
a) tetralogy of Fallot
b) aortic insufficiency
c) mitral stenosis
d) mitral insufficiency
- For congenital heart defects in children, treatment is recommended
a) cardiac glycosides
b) diuretics
c) vitamins
d) operational
- Clinical signs of vegetative-vascular dystonia of the sympathicotonic type in children
a) tachycardia, increased blood pressure
b) bradycardia, decreased blood pressure
c) hyperhidrosis and hypersalivation
d) bright red dermographism
- Clinical signs of vegetative-vascular dystonia of the parasympathicotonic (vagotonic) type in children
a) tachycardia, increased blood pressure
b) bradycardia, decreased blood pressure
c) pale and dry skin
d) bright eyes, exophthalmos
- With vegetative-vascular dystonia in children, a syndrome occurs
a) jaundice
b) hemorrhagic
c) edematous
d) psychovegetative
- In the treatment of vegetative-vascular dystonia in children, non-drug medications are important
a) jars, mustard plasters
b) positional drainage
c) oxygen therapy through defoamers
d) normalization of work and rest regime, exercise therapy
- In the treatment of vegetative-vascular dystonia in children, a plant with a sedative effect is used
a) marshmallow
b) wild rosemary
c) valerian
d) bearberry
- If a child faints, the child should be placed in a position
a) lying down with the head end raised
b) lying on your side
c) lying down with the leg end raised
d) sitting with legs down
- For pulmonary edema in children, it is carried out
a) oxygen therapy
b) oxygen therapy through defoamers
c) placing cans
d) installation of mustard plasters
Listen (6,184 KB): The "audio/mpeg" object is not supported. .
The heart is a muscular organ that moves the blood through its rhythmic contractions. The muscle tissue of the heart is represented by special cells - cardiomycytes.
As in any tubular organ, the wall of the heart contains membranes:
- inner lining, or endocardium,
- middle layer, or myocardium,
- outer membrane, or epicardium.
The heart develops from several sources. Endocardium, connective tissue of the heart, including blood vessels, is of mesenchymal origin. The myocardium and epicardium develop from the mesoderm, more precisely, from the visceral layer of the splanchnotome, the so-called. myoepicardial plates.
Structure of the heart
Endocardium
The inner lining of the heart, the endocardium, lines the inside of the heart chambers, papillary muscles, tendon filaments, and heart valves. The thickness of the endocardium varies in different areas. It is thicker in the left chambers of the heart, especially on the interventricular septum and at the mouth of large arterial trunks - the aorta and pulmonary artery, and on the tendon threads it is much thinner.
There are 4 layers in the endocardium: endothelium, subendothelial layer, muscular-elastic layer and outer connective tissue layer.
The surface of the endocardium is lined with endothelium lying on a thick basement membrane. This is followed by a subendothelial layer formed by loose fibrous connective tissue. Deeper is the muscle-elastic layer, in which elastic fibers intertwine with smooth muscle cells. Elastic fibers are much better expressed in the endocardium of the atria than in the ventricles. Smooth muscle cells are most strongly developed in the endocardium at the exit of the aorta. The deepest layer of the endocardium, the outer connective tissue layer, lies on the border with the myocardium. It consists of connective tissue containing thick elastic, collagen and reticular fibers. These fibers directly continue into the fibers of the connective tissue layers of the myocardium.
The endocardium is nourished mainly diffusely by the blood in the chambers of the heart.
Myocardium
The middle, muscular layer of the heart (myocardium) consists of striated muscle cells - cardiomyocytes. Cardiomyocytes are closely connected to each other and form functional fibers, the layers of which surround the chambers of the heart in a spiral shape. Between the cardiomyocytes there are layers of loose connective tissue, blood vessels, and nerves.
There are three types of cardiomyocytes:
- contractile, or working, cardiac myocytes;
- conductive, or atypical, cardiac myocytes, which are part of the so-called conduction system of the heart;
- secretory, or endocrine, cardiomyocytes.
Contractile cardiomyocytes form the main part of the myocardium. They contain 1-2 nuclei in the central part of the cell, and myofibrils are located along the periphery. The junctions between cardiomyocytes are called intercalated discs and contain gap junctions (nexuses) and desmosomes. The shape of cells in the ventricles is cylindrical, in the atria it is irregular, often branched.
Cardiomyocytes are covered with a sarcolemma, consisting of a plasma membrane and a basement membrane, into which thin collagen and elastic fibers are woven, forming the “external skeleton” of cardiomyocytes - endomysium. The basement membrane of cardiomyocytes contains a large number of glycoproteins that can bind Ca2+ ions. It takes part in the redistribution of Ca2+ ions in the contraction-relaxation cycle. The basement membrane of the lateral sides of cardiomyocytes invaginates into the tubules of the T-system (which is not observed in somatic muscle fibers).
Cardiomyocytes of the ventricles are much more intensively penetrated by the tubules of the T-system than somatic muscle fibers. The tubules of the L-system (lateral extensions of the sarcoplasmic reticulum) and the T-system form dyads (1 tubule of the L-system and 1 tubule of the T-system), less often triads (2 tubules of the L-system, 1 tubule of the T-system). In the central part of the myocyte there are 1-2 large oval or elongated nuclei. Between the myofibrils there are numerous mitochondria and tubules of the sarcoplasmic reticulum.
Unlike ventricular cardiomyocytes, atrial myocytes often have a process-like shape and are smaller in size. Atrial myocytes have fewer mitochondria, myofibrils, and sarcoplasmic reticulum, and the T-system of tubules is poorly developed. In those atrial myocytes where there is no T-system, numerous pinocytotic vesicles and caveolae are located on the periphery of the cells, under the sarcolemma. It is believed that these vesicles and caveolae are functional analogues of T-tubules.
Between the cardiomyocytes there is interstitial connective tissue containing a large number of blood and lymphatic capillaries. Each myocyte contacts 2-3 capillaries.
Secretory cardiomyocytes are found predominantly in the right atrium and appendages of the heart. In the cytoplasm of these cells there are granules containing a peptide hormone - atrial natriuretic factor (ANF). When the atria are stretched, the secretion enters the blood and affects the collecting ducts of the kidney, the cells of the zona glomerulosa of the adrenal cortex, which are involved in the regulation of extracellular fluid volume and blood pressure levels. PNF causes stimulation of diuresis and natriuresis (in the kidneys), vasodilation, inhibition of the secretion of aldosterone and cortisol (in the adrenal glands), and a decrease in blood pressure. The secretion of PNF is sharply increased in patients with hypertension.
Conducting cardiac myocytes (myocyti conducens cardiacus), or atypical cardiomyocytes, provide rhythmic coordinated contraction of various parts of the heart due to their ability to generate and quickly conduct electrical impulses. A collection of atypical cardiomyocytes forms the so-called cardiac conduction system.
The conduction system includes:
- sinoatrial, or sinus, node;
- atrioventricular node;
- atrioventricular bundle (bundle of His) and
- its branches (Purkinje fibers), transmitting impulses to contractile muscle cells.
There are three types of muscle cells, which are found in different proportions in different parts of this system.
- The first type of conducting myocytes is P-cells, or pacemaker myocytes, the pacemakers. They are light, small, branched. These cells are found in the sinus and atrioventricular nodes and in the internodal tracts. They serve as the main source of electrical impulses that ensure the rhythmic contraction of the heart. The high content of free calcium in the cytoplasm of these cells with weak development of the sarcoplasmic reticulum determines the ability of sinus node cells to generate impulses to contract. The supply of necessary energy is provided mainly by the processes of anaerobic glycolysis.
- The second type of conducting myocytes are transitional cells. They form the main part of the conduction system of the heart. These are thin, elongated cells, found mainly in the nodes (their peripheral part), but also penetrate into the adjacent areas of the atria. The functional significance of transitional cells is the transfer of excitation from β-cells to the His bundle cells and the working myocardium.
- The third type of conducting myocytes are Purkinje cells, often lying in bundles. They are lighter and wider than contractile cardiomyocytes and contain few myofibrils. These cells predominate in the bundle of His and its branches. From them, excitation is transmitted to the contractile cardiomyocytes of the ventricular myocardium.
The muscle cells of the conduction system in the trunk and branches of the legs of the trunk of the conduction system are located in small bundles; they are surrounded by layers of loose fibrous connective tissue. The bundle branches branch under the endocardium, as well as in the thickness of the ventricular myocardium. The cells of the conduction system branch in the myocardium and penetrate the papillary muscles. This causes tension on the valve leaflets (left and right) by the papillary muscles even before contraction of the ventricular myocardium begins.
Purkinje cells are the largest not only in the conduction system, but in the entire myocardium. They have a lot of glycogen, a sparse network of myofibrils, and no T-tubules. The cells are connected by nexuses and desmosomes.
Epicardium and pericardium
The outer, or serous, membrane of the heart is called the epicardium. The epicardium is covered with mesothelium, under which there is loose fibrous connective tissue containing blood vessels and nerves. The epicardium may contain a significant amount of adipose tissue.
The epicardium is a visceral layer of the pericardium (pericardium); The parietal layer of the pericardium also has the structure of a serous membrane and faces the visceral layer of the mesothelium. The smooth, moist surfaces of the visceral and parietal layers of the pericardium easily slide over each other when the heart contracts. If the mesothelium is damaged (for example, due to an inflammatory process - pericarditis), the activity of the heart can be significantly impaired due to the formation of connective tissue adhesions between the layers of the pericardium.
The epicardium and parietal layer of the pericardium have numerous nerve endings, mainly of the free type.
Fibrous skeleton of the heart and heart valves
The supporting skeleton of the heart is formed by fibrous rings between the atria and ventricles and dense connective tissue at the mouths of large vessels. In addition to dense bundles of collagen fibers, the “skeleton” of the heart contains elastic fibers, and sometimes even cartilaginous plates.
Valves are located between the atria and ventricles of the heart, as well as the ventricles and large vessels. The surfaces of the valves are lined with endothelium. The basis of the valves is dense fibrous connective tissue containing collagen and elastic fibers. The bases of the valves are attached to the fibrous rings.
(see also lecture on muscle tissue from general histology)
Some terms from practical medicine:
- cardiosclerosis - excessive development of connective tissue in the myocardium;
- Cardiophobia - obsessive fear - fear of death from heart disease;
- hanging heart, asthenic - a constitutional variant of the heart shape, characterized by an approaching vertical position of the anatomical axis and relatively small linear dimensions of the x-ray shadow; usually observed in persons of asthenic physique;
- recumbent heart, hypersthenic - a constitutional variant of the heart shape, characterized by an approaching horizontal position of the anatomical axis and relatively large linear dimensions of the x-ray shadow; observed in persons with a hypersthenic physique or with a high diaphragm;
- hairy, villous heart - a heart whose surface is completely covered with sclerosing and fresh fibrin fibers; observed with massive fibrinous pericarditis;
- glazed heart - a heart with a sharply thickened pericardium, looking like a whitish translucent plate; observed in chronic serous pericarditis;
- armored heart - a heart with a sharply thickened, compacted and calcified pericardium; observed as a result of adhesive pericarditis;
- beer heart - a severe form of alcoholic myocardial dystrophy, characterized by severe dilatation of all parts of the heart, disturbances in its rhythm and conduction, and heart failure;
- bovine heart - significant degree of cardiomegaly;
- tiger heart - a heart on a section of which under the endocardium, especially on the papillary and pectineus muscles, thin yellow-white stripes reminiscent of tiger skin are visible; observed with a sharp degree of fatty degeneration of the myocardium;
| Part one - Functional characteristics, general plan of the structure of blood vessels, development | circulation1.mp3, 3 348 kB |
| Part two – Arteries and veins | circulation2.mp3, 6 187 kB |
| Part three - Microvasculature vessels | circulation3.mp3, 6 855 kB |
| Part Four – Lymphatic Vessels | circulation4.mp3, 3 773 kB |
| Part five – Age-related changes in blood vessels, regeneration | circulation5.mp3, 2 673 kB |
| Part Six – Heart | circulation6.mp3, 6 185 kB |
Does the outcome of the disease depend on its type?
The outcome of rheumatic endocarditis depending on the type of disease:
- In the acute warty form of the pathology, the deepest layers of the endothelium are affected, resulting in growths of considerable size. They have a gray-brown tint and a dense structure. Over time, the warts grow and stick together, developing polypous endocarditis.
- In the recurrent warty form of rheumatic endocarditis, the valves are affected by sclerosis.
- If the disease is simple, there is no deep damage, then the tissues swell. As a rule, the outcome is quite favorable, subject to adequate and timely treatment.
- With the fibroplastic form of rheumatic endocarditis, there is a risk of all complications. Therefore, this type requires special therapeutic intervention.
Treatment
Treatment of endocarditis has two directions - medication and surgery. Surgery is quite dangerous, but in cases where drug treatment does not produce results, heart failure may develop and surgery is the only way to save the patient’s life.
During treatment, the level of microorganisms in the blood and the condition of the heart are constantly monitored using ECG and echocardiography.
For subacute endocarditis, benzylpenicillin sodium salts in high doses or cephalosporins in combination with gentamicin are prescribed. Antibiotics are administered primarily intravenously. As a last resort, replacement of a damaged heart valve is used.
For the infectious type of endocarditis, treatment with antibacterial drugs is used.
When treating endocarditis, attention is primarily paid to the treatment of the underlying pathology - rheumatism, sepsis, systemic lupus erythematosus. The method of using antibacterial drugs has proven itself to be excellent. In most cases they are used. Antibiotics are selected according to the results of blood cultures for microflora in order to strike an accurate blow to the infection, while minimizing the toxic effect on the body.
As a rule, the patient is hospitalized in order to monitor his condition and administer antibiotics through an intravenous drip. Blood samples are constantly taken from the patient; the results of the analysis will clearly show progress in treatment. Then you can return home and take the antibacterial drugs prescribed by your doctor on your own.
A significant effect is achieved through a combination of drugs, which complicates the selection procedure. The classic options are ampicillin and sulbactam, as well as vancomycin and ciprofloxacin.
70% of the success in the antibacterial treatment of endocarditis comes from drugs that stimulate the immune system.
Endocarditis can cause serious damage to the heart. Surgical treatment of endocarditis is based on excision and removal of the affected area. About 20% of patients with endocarditis may require surgical treatment. Operations are recommended in cases:
- Symptoms and/or test results indicate the occurrence of heart failure (a serious condition in which the heart is unable to meet the body's needs).
- For a long time, despite treatment with antibacterial and antifungal drugs, high temperature and fever persist.
- The patient has an artificial heart valve.
The three main surgical procedures for treating endocarditis are:
- repair of a damaged heart valve;
- replacement of damaged heart valves with prostheses;
- removing any abscesses that may form in the heart muscle.
Surgery is offered only to patients with severe disease. Unfortunately, even in the case of a successful operation, every tenth patient dies during or some time after the operation. If possible, your own valves are preserved through plastic surgery. In cases where the valve is deformed too much, it must be replaced with an artificial one.
A successful operation transfers the person to outpatient monitoring with constant collection of tests and examinations. For the next 6 months, the person undergoes monthly examinations - this is a very dangerous zone for recurrent infections. Further inspection must be carried out twice a year.
Treatment of endocarditis is based on the main goal - the need to completely restore or remove tissue that has undergone inflammatory processes.
Bactericidal drugs are used in high doses, with intravenous drip administration. Often the use of one drug is ineffective, then combination drugs are used.
Depending on the causative agent of the disease, the following are used: benzylpenicillin, gentamicin or amikacin intramuscularly (infection with viridans streptococcus); semisynthetic penicillins in combination with cephalosporins or aminoglycosides (for staphylococcal endocarditis); if you are intolerant to penicillins, macrolides can be prescribed;
Immunocorrection
Passive immunization is used to neutralize microbial toxins circulating in the bloodstream with ready-made antitoxic sera. The most effective are hyperimmune plasma and human immunoglobulin, which are administered intravenously daily for 3–5 days.
How to increase the chances of a favorable outcome?
In order to achieve a favorable outcome, it is necessary to promptly pay attention to symptoms, undergo diagnostic measures and carry out appropriate treatment.
In general, you need to do the following:
- Physical activity is limited, in some cases eliminated altogether.
- Stressful situations must be avoided.
- You will have to adhere to the diet prescribed by your doctor. Salty, fatty, fried, smoked and canned foods are excluded. You cannot drink alcoholic beverages or smoke.
- It is imperative to adhere to drug therapy. Most often, rheumatic endocarditis occurs against the background of beta-hemolytic streptococci, so benzylpenicillin solution is injected intramuscularly four times a day for at least 10 days. It is mandatory to take glucocorticosteroids, which eliminate the inflammatory process in the heart muscles. For this purpose, the drug Prednisolone is prescribed in tablet form. The tablets are taken on an empty stomach once a day.
- If there is a risk of an unfavorable outcome, the doctor prescribes surgery. Most often this happens in the presence of purulent accumulations, the rapid development of complications and massive growths. The operation is considered complex, since it is an open method - the chest cavity is opened, the patient is connected to the artificial circulation system, after which the surgeon cleans the valves and cuts out the damaged areas. If necessary, an organ is implanted.
- It is very important to strengthen the immune system, so the patient is recommended to take vitamin complexes and hardening.
- During treatment, the recovery period and further time, the patient must visit a doctor for a preventive examination.
The outcome for a person’s life with rheumatic endocarditis is quite favorable, but complete recovery is difficult to achieve. For older people, the prognosis is less favorable than for younger people. But the most important thing is timely and adequate treatment. Thus, the outcome largely depends on the patient himself and the prescribed therapy.
Pathomorphological changes
It was possible to find out about pathological changes in internal organs only by autopsy of the dead. This continued until the introduction into medical practice of modern technologies that make it possible to visualize internal organs in 3D format. With the help of devices, you can accurately establish a diagnosis and see structural changes in the membranes of the heart.
Atypical warty endocarditis includes pathomorphological disorders due to damage to the body by SLE (systemic lupus erythematosus). Changes on the macroscopic specimen are observed in the form of the location of warts at the base of the leaflets of almost the entire valve apparatus. According to the morphological classification, there are diffuse and acute warty, recurrent verrucous, acute ulcerative and polypous-ulcerative, fibroplastic endocarditis. Let us consider in more detail pathological structural disorders in the structure of the valve apparatus:
- diffuse endocarditis occurs against the background of rheumatic changes. By examining a microslide, mucoid and fibrinoid swelling of the affected valve can be detected. The endothelium is not affected by the pathological process, and there are no blood clots.
- Acute warty endocarditis. Due to damage to the body by rheumatism, systemic lupus erythematosus, and severe infections, the structural structure of the endocardium changes with the formation of characteristic warts on the surface of the valves.
- Acute polypous-ulcerative accompanies septic processes in the human body. When examining a gross specimen of the heart, ulcers, perforations of the valves and polypous deposits are visible.
- Fibroplastic. Most often it manifests itself against the background of rheumatism. Characterized by inflammation of the endocardium and sclerotic damage to the valve.
Features of the disease
It should be noted that patients initially experience swelling of collagen fibers followed by a proliferative reaction. In the early stages, the surface of the valve begins to change. At the points of contact of the valves, platelets and fibrin begin to accumulate and settle, which leads to the appearance of growths (warts). The valve tissue under the growths is swollen. The tricuspid valve leaflets are subject to rheumatoid changes half as often as those of the mitral valve. Subsequently, the valves become scarred, wrinkled and deformed, and thickening or fusion of the walls is observed. This leads to the development of heart disease.
As a result of rheumatic endocarditis, valve insufficiency or stenosis may develop. Insufficiency is the incomplete closure of the valve leaflets, and stenosis is the narrowing of its opening. The most common complication is mitral valve insufficiency of the heart muscle.
Most often, rheumatic endocarditis develops between the ages of six and sixteen years, but recently there has been a decrease in the incidence in children. There are no specific features of the disease in children and adults; it progresses in exactly the same way.
Clinical picture of rheumatic endocarditis
Non-infectious thromboendocarditis
Occurs in most cases on the lining of the heart valves. Morphological changes are ulcerative or ulcerative-polyposis in nature and lead to the development of myocardial valve defects. Initially, ulcerations of the cusps of the mitral (less often the aortic) valve appear, measuring from 2 to 10 mm. They quickly increase and spread to the parietal endocardium and chordae tendineae, which leads to the formation of aneurysms (protrusion of the leaflet wall).
Platelets accumulate on the damaged surface, and fibrin accumulates in the depths. Accordingly, the tissue of the valve apparatus swells and is permeated with fibrin, which entails very serious complications: separation of the tendon chords or parts of the valve, blockage of blood vessels with blood clots and microbial particles with the formation of a septic infarction.
When the process “attenuates” due to physiological and morphological factors, the valves shrink and become deformed, which contributes to the occurrence of arrhythmias, hypertrophy of individual parts of the heart, various hemodynamic disorders and the development of heart failure.
A form of sepsis that develops after infection with common or hemolytic streptococcus, less commonly pneumococcus. It is characterized by the formation of ulcers on the endothelium of myocardial valves and thrombotic deposits. More often it develops on sclerotic and altered valves, mainly the aortic, less often the mitral and tricuspid.
The morphology and dynamics of this type of disease practically repeats the development of acute infective endocarditis, but with some features. Ulcerative defects of the leaflets, tendinous chords and parietal endocardium are inherent. Lymphocytes and giant cells are localized around zones of tissue destruction next to colonies of microorganisms.
Under the thrombotic formations there is granulation tissue, which has a granular appearance and, when maturing, deforms the valve. Since the course of the pathology is chronic and relapsing, blockage of blood vessels and infarctions of various organs, focal inflammation of the kidneys with predominant damage to the glomeruli, enlarged spleen, and progressive anemia are inevitable.
A group of inflammatory diseases of the endocardium of a non-infectious nature (minimal endocarditis, abacterial, degenerative verrucous and other forms). It can occur as a result of external and internal intoxication, with senile insanity, and in weakened patients. The disease manifests itself on the endocardium of the valves, more often in the left ventricle, by the formation of thrombotic deposits, while obvious signs of the inflammatory process may be absent or manifested only slightly by the accumulation of monocytes, macrophages, fibroblasts in the affected areas.
Types and forms
According to the foci of occurrence, rheumatic endocarditis can be:
The valve is considered the most common. In turn, it is divided into four categories:
- diffuse (valvulitis according to the classification of V. T. Talalaev). Affects the valve leaflets, but without the formation of growths;
- sharp warty. It occurs with damage to the endothelium and the formation of warts on the trailing edge of the valve leaflets;
- fibroplastic. Appears as a consequence of the two forms described above and is characterized by fibrosis and scarring;
- recurrent verrucous. Occurs repeatedly on altered valve flaps. Accompanied by the new appearance of growths.
Causes of rheumatic endocarditis
Doctors believe that the main cause of rheumatism is group A beta-hemolytic streptococcus. In childhood, a patient who comes into contact with it can develop pharyngitis or tonsillitis. Without consulting a doctor for qualified help, the disease goes away on its own, but causes consequences.
Heart structures most often affected by rheumatic endocarditis:
- mitral valve;
- tricuspid valve (usually in combination with other localizations);
- aortic valve;
- parietal (parietal) endocardium;
- chordae tendineae;
- deep layers of the myocardium.
Therefore, with rheumatic endocarditis, inflammation occurs a little differently and differs from the infectious and septic varieties, although the initial cause of its appearance was the entry of streptococcus into the body. Read more about the symptoms and signs of endocarditis in children and adults.
Read also: Septic endocarditis treatment
The symptoms of all forms of endocarditis are very similar and very often do not indicate its rheumatic variety. When examining a patient, a cardiologist usually reveals:
- shortness of breath. Especially during physical activity;
- pain in the heart area. This is not such a common symptom and may appear in the later stages of the disease;
- increased heart rate (tachycardia). The main distinguishing feature of endocarditis is that it has nothing to do with physical stress and is completely independent of body temperature;
- nails in the shape of watch glasses. The nail formations on the fingers expand and become more rounded, the central part of the nail plate rises, forming a dome;
- drumstick-shaped fingers (Hippocratic fingers). A similar symptom may occur in patients at a late stage of the disease. Characterized by the fact that the fingers become narrower, and the last phalanx widens. With rheumatic changes it appears most often. But it also happens with other diseases;
- pale skin. In advanced stages of the disease, blue discoloration of the fingertips and nose may occur;
- fast fatiguability. It appears in the initial stages, especially during physical activity.
One of the main symptoms when diagnosing rheumatoid endocarditis can be a pronounced heart murmur, which appears in the fifth week after the onset of the process.
When taking a blood test, an increased number of leukocytes is detected. C-reactive protein appears and fibrinogen levels increase. Distinct conduction disturbances appear on the ECG.
Polypous-ulcerative endocarditis - classification of the disease, symptoms and treatment
First, we need to define endocarditis. This medical term describes inflammation of the inner layer of the heart, the endocardium. It is important to know that heart valves, in fact, are duplications (doubling in the form of plastic surgery) of the endocardium, and therefore with endocarditis, it is the valve system of the organ that is primarily affected.
From the point of view of pathological anatomy, endocarditis is a complex inflammatory process that includes all stages of inflammation from alteration (damage and death of cells and structures) to proliferation (formation of new cellular elements).
It is characteristic that the intermediate process of exudation, that is, the sweating of plasma and the release of blood cells through thinned and stretched vascular walls, is not expressed, since the endocardium contains few vessels.
However, the processes of thrombus formation are active due to the constant washing of the damaged endocardial walls with blood from the heart cavities.
Classification
There are several classifications of endocarditis. Depending on the location of the lesion, the following forms of the disease are distinguished:
- Valvular endocarditis - when the heart valves are directly affected, occurs most often due to the high physiological load on the valve system.
- Parietal endocarditis - when the endocardium lining the heart walls is affected.
- Chordal - when the chord of the heart is affected, that is, a bundle of fibers connecting the opposite walls of the left ventricle.
- Trabecular - when the trabeculae are affected, that is, the plates that form the frame of the heart from the inside.
Depending on the current, we can distinguish:
- acute form - about two weeks,
- subacute form – up to three months,
- chronic form - months and years.
Based on the nature of morphological and structural changes in the heart, endocarditis is divided into forms:
- Simple or initial endocarditis - it is often based on an infectious disease, an autoimmune pathology such as rheumatic disease or severe intoxication. The most common target is the mitral valve, with the aortic and tricuspid valves being the second most commonly affected valves.
- Warty endocarditis - most often develops with rheumatic disease or after infectious diseases or intoxications. It is characterized by the formation of warty blood clots over the altered endocardium. Acute warty endocarditis is characterized by the presence of multiple small blood clots that are easily removed from the surface of the endocardium. Recurrent warty endocarditis is characterized by the presence of both fresh thrombotic deposits and sclerotic changes in the endocardium with its deformation and the formation of focal growths (granulomas). On a gross specimen of the heart after autopsy: the valve leaflets are thickened, with foci of sclerosis, deformed, thrombotic “warts” at the edges, chords are shortened, the tissue is pale.
- Fibrous or fibroplastic endocarditis - it is also often based on rheumatic disease, but a characteristic feature is early fibrosis, that is, thickening, compaction of tissue with scar changes, replacement with connective tissue and more aggressive proliferative-destructive processes. Gross specimen of the heart after autopsy: the heart is enlarged, fibrin threads in the form of hair (“hairy heart”) are on the pericardium, the septa are thickened.
- Polypous-ulcerative or septic endocarditis - develops with sepsis of various etiologies, it is based on the predominance of destructive processes over reparative ones, which causes the formation of rough and large ulcers on the endocardium. The ulcerative process leads to the formation of blood clots due to the release of vasoactive substances by damaged endothelium and impaired blood circulation due to changes in the structure of the endocardium. Thrombi also serve as a breeding ground for various types of bacteria, which can cause the initiation of endocardium and the development of necrosis of valve tissue. In acute polyposis-ulcerative endocarditis, the target is the mitral valve, and in subacute - the aortic valve. The inflammatory process actively moves from the valves to other tissues of the heart, which leads to massive thrombus formation, infection of blood clots, their separation and spread of infection throughout the body. Thus, ulcerative endocarditis is considered a form of sepsis. On a gross specimen of the heart after autopsy: there are foci of sepsis on the valves, defects, the valves are sclerotic, the tissue is dull.
- Recurrent endocarditis is the most typical form among all endocarditis. It is based on rheumatic disease, sepsis (usually caused by streptococcus). The patient experiences relapses of previously occurring endocarditis with a layering of fresh destructive changes on top of the old ones.
Symptoms
The clinical picture of endocarditis is extremely diverse and can vary from a long course without specific symptoms to full-blown sepsis affecting all organs and systems. Typically, the first signs of endocarditis begin to appear within two weeks after infection.
Advanced endocarditis is characterized by the development of the following symptoms:
- severe intoxication of the body, high temperature with chills, loss of body weight, loss of appetite, headache, joint and muscle pain,
- the presence of rashes, spots on the skin of the palms, soles and body, slight jaundice and pallor,
- arthritis of the knee, ankle, elbow, wrist joints,
- formation and separation of blood clots with the development of infarctions in various organs (where a vessel is blocked by a thromboembolus),
- pericarditis of the heart,
- enlarged lymph nodes,
- renal failure, development of kidney inflammation,
- damage to the central nervous system due to thromboembolism in the vessels of the brain, the development of meningoencephalitis,
- AHF, CHF.
Diagnostics
Important! When diagnosing endocarditis, the doctor takes into account the general condition of the patient, that is, the severity of fever, data from a study of the heart valves, the presence of thromboembolic complications and the results of laboratory diagnostics.
Among laboratory methods, the following are highly informative:
- Complete blood count - according to the CBC data, one can judge the developing anemia and the state of the leukocyte system, as well as changes in the level of ESR.
- Biochemical blood test - biochemistry data can indicate the level of specific inflammatory markers (C-reactive protein and others).
- Immunological blood test - using an immunological test, the rheumatic etiology of endocarditis can be established when rheumatoid factor is detected.
- Blood culture for sterility is a key verification method for diagnosing bacterial endocarditis. A prerequisite is repeated blood sampling and analysis outside of antibiotic therapy.
To clarify the diagnosis of “polyposis-ulcerative endocarditis”, instrumental diagnostic methods are used:
- Based on the ECG results, the localization of the lesion, the presence or absence of left ventricular hypertrophy, and cardiac conduction disorders are determined.
- Based on the results of echocardiography, it is possible to characterize the condition of the tissue and valves of the heart, determine the presence or absence of ulcerative defects, calcium deposits, and chordal ruptures. EchoCG also allows one to determine heart defects with the development of mitral or aortic insufficiency, which may be an indication for surgical intervention.
Treatment
When treating patients with polyposis-ulcerative endocarditis (and other forms), there are several main lines of therapy:
- Massive and long-term antibacterial therapy - intravenous drip administration of antibiotics in maximum doses is prescribed, taking into account the sensitivity of the pathogen. Taking into account the etiology of endocarditis, antibiotics of the penicillin group, for example Benzylpenicillin, and aminoglycoside groups, for example Gentamicin, Amikacin, are used. If the penicillin series is ineffective, macrolides and fluoroquinolones are used.
- Correction of the immune system - antitoxic serums based on ready-made antibodies to pathogen antigens are used as immune preparations. Human immunoglobulin and hyperimmune plasma are highly effective; intravenous administration is prescribed for five days.
- Surgical treatment - in the absence of effect from conservative therapy, progressive deterioration of the patient’s condition with the development of heart failure, thromboembolism and other complications, the issue of surgical removal of foci of infection in the endocardium and affected valves is resolved with mandatory reconstruction of the valve system with artificial prostheses.
- Symptomatic treatment of heart failure and complications of other organs.
Thus, the treatment of endocarditis, especially septic, is not strictly specific and should be selected individually for each patient, taking into account the characteristics of his immune system.
Loading…
Source: https://dlja-pohudenija.ru/serdcze/vospalenie-serdcza/formy-endokarditov-pochemu-nuzhno-opasatsya-polipozno-yazvennogo-endokardita
Diagnostics
When diagnosing rheumatic endocarditis, several methods are used:
- examination of the patient. Performed by a therapist or cardiologist. No preliminary diagnosis is made. Necessary for detecting non-cardiac symptoms of the disease and an initial examination of the state of the cardiovascular system;
- analysis of laboratory results. Thanks to the tests, the cause of the disease is mainly revealed. They can be a sufficient argument for making a diagnosis and prescribing treatment. To confirm rheumatic endocarditis, tests must be taken for the titer of streptococcal antibodies and rheumatoid factor;
- bacteriological tests. Blood tests to detect the causative agent of endocarditis;
- examination using medical equipment. Cardiac examinations are performed using electrocardiography, echocardiography, radiography, ultrasound, magnetic resonance therapy and computed tomography.
Treatment of rheumatic endocarditis is carried out by all known methods and includes taking medications and following doctor’s orders. If heart failure continues to develop, surgical intervention is performed.
Therapeutic method
Includes fulfillment of such doctor’s requirements as:
- limiting physical activity or completely refusing it;
- avoidance of stress;
- diet, avoiding salt, alcohol, spicy and fatty foods;
- to give up smoking.
Medication method
This method of treating endocarditis involves the use of antibiotics, which are aimed at the complete destruction of beta-hemolytic streptococcus. As we have already mentioned, it is he who causes rheumatic changes in the heart. An intramuscular injection of benzylpenicillin is prescribed. It must be done four times a day for ten days.
After this, treatment with glucocorticosteroid drugs is prescribed. It is aimed at relieving inflammation of the heart muscle. Prednisolone tablets of 20 mg per day are used, you need to drink them one at a time after your morning meal. The main purpose of the patient taking these drugs is to prevent the development of heart disease.
Surgical intervention is performed only in case of unfavorable development of the disease and if the patient’s condition allows. Indications:
- formation and accumulation of pus in the endocardial area;
- heart failure continues to worsen;
- massive growths on the valve flaps;
The operation is performed by opening the chest and connecting the patient to a heart-lung machine. The heart surgeon cleans the valves and removes the affected areas. If necessary, a decision is made to replace severely damaged valves with artificial ones, but this is a separate operation.
Clinical manifestations of endocarditis
To make a correct diagnosis, it is necessary to take into account the entire complex of manifestations of the pathological process. In typical cases, the diagnosis of endocarditis is based on the following signs: the presence of fever with chills, valvular defects with the appearance of myocardial murmurs, thromboembolic complications and positive results of bacteriological examination.
An electrocardiogram (ECG) shows signs of hypertrophy of the left ventricle (with inflammation of the aortic or mitral valve) or right ventricle (damage to the tricuspid or pulmonary valve). Conduction disturbances, atrial and ventricular extrasystole are possible, sometimes atrial fibrillation or flutter is detected.
An ECG examination allows one to determine the presence of the disease in the early stages, which becomes a determining factor for subsequent successful treatment. You can examine your heart using a cardiovisor device, which will detect minimal deviations in the functioning of the heart muscle.
Echocardiography (EchoCG) is recommended in all patients with suspected infective endocarditis. The method allows you to objectively assess the condition of the valve apparatus, timely detect calcification, rupture of the valve leaflet or chords, and abscess of the valve ring. EchoCG is often used to clarify the nature of the heart defect, as well as to determine the need for urgent surgical treatment when aortic or mitral valve insufficiency develops acutely.
Blood tests are quite informative: general, biochemical and immunological. Generally, it may show anemia and a shift in the leukocyte count to the left, the most significant sign being an increase in ESR. Biochemical analysis reveals the presence of C-reactive protein, an increase in the amount of fibrinogen, a decrease in albumin, and an increase in the fraction of γ-globulins. An immunological test will help detect rheumatoid factor and increased levels of compliment components.
Blood cultures are also carried out to ensure sterility - one of the most important steps when infective endocarditis is suspected. The technique of blood sampling is important here; such an analysis is repeated two to three times in order for the diagnosis to be reliable, the results should be the same. When a diagnosis of “endocarditis” is established, it is important to correctly identify the form of the disease in order to increase the effectiveness of treatment.
fever, general malaise, loss of strength, darkening of the eyes, sometimes palpitations and increased blood pressure. Later, symptoms characteristic of morphological changes in the structure of the endocardium appear: shortness of breath at rest, pain in large joints, severe coughing attacks due to associated cardiovascular failure, hemorrhages under the nail plates and on the mucous membranes of the skin, hardening of the fingertips in the form of Osler’s nodes. Only an experienced cardiologist can differentiate between various pathological types of lesions of the inner wall of the heart.
Problem No. 1 is to assume this disease in a patient. Signs of a pathological condition almost always appear in advanced forms of septic damage to the valve apparatus. Therefore, death may occur before this condition is suspected. If, nevertheless, the doctor suspects that a pathogenetic change has occurred in the patient, he will prescribe a number of studies to confirm the diagnosis.
Diagnosis of endocarditis is made difficult by the fact that the disease can begin in various ways. The main criteria are: fever with chills, results of bacteriological examination confirming infection and valve defects detected on echocardiography (ultrasound of the heart).
An electrocardiogram (ECG) can reveal signs of ventricular enlargement and conduction disturbances, which can occur already in the early stages of endocarditis.
Blood tests can differentiate different types of endocarditis from each other.
Clinical manifestations of endocarditis in various diseases have similar symptoms of damage to the valvular apparatus of the heart and a general tendency towards thromboembolic complications, but differ in features determined by the picture and pathogenesis of the underlying disease. Subacute bacterial endocarditis and rheumatic endocarditis are described in the articles Subacute bacterial endocarditis (see.
Acute infective endocarditis is manifested by a picture of general sepsis, caused, as a rule, by virulent flora - Staphylococcus aureus, streptococcus pyogenes, gram-negative bacteria, etc., and the entrance gates of infection are often detected (damaged skin or mucous membranes, infectious focus in the lungs, genitourinary tract, etc. .).
High fever (of the wrong type or hectic), chills, sweating, and signs of general intoxication with damage to the central nervous system are typical. Embolism in various organs with the development of purulent metastatic foci is often observed. Usually there is an enlargement of the liver and spleen, signs of kidney damage up to the picture of apostematous nephritis.
The diagnosis is confirmed by identifying signs of damage to the heart valves with their insufficiency. In contrast to subacute bacterial endocarditis, acute infective endocarditis often affects intact valves, mainly the tricuspid and pulmonary trunk, less commonly the aorta. The blood usually reveals high leukocytosis with a shift to the left and anemia, a significant acceleration of ROE.
Antibacterial therapy, carried out according to the general rules for the treatment of sepsis (see), taking into account the identified pathogen, is of primary importance in the treatment of acute infective endocarditis. If the pathogen has not been identified, it is advisable to begin therapy by prescribing high doses of benzylpenicillin sodium salt (60,000,000 - 80,000,000 units per day) or semi-synthetic penicillins (ampiox 12-15 g per day) in combination with gentamicin (3 -5 mg per 1 kg of body weight per day).
For endocarditis of staphylococcal etiology, anti-staphylococcal plasma is used (6-8 infusions of 200 ml once a day or every other day), human anti-staphylococcal immunoglobulin (at the rate of 10 IU per 1 kg of body weight per day). When bacterial shock develops, glucocorticoids are used. Detoxification therapy and correction of disturbances in the electrolyte composition of the blood are carried out. If necessary, surgical treatment of primary and metastatic purulent foci is carried out.
Endocarditis caused by fungi - Candida genus, Aspergillus, Histoplasma (less commonly Blastomycetes, Coccidoides and Cryptococci) is sometimes observed in people who have been receiving antibiotics and corticosteroids for a long time, in those who have undergone heart surgery, in drug addicts who inject themselves with drugs intravenously. In this case, not only the aortic and mitral valves are often affected, but also the tricuspid valve, and in operated patients, the prosthetic valve.
The clinical picture of fungal endocarditis usually corresponds to that of subacute bacterial endocarditis (see Subacute bacterial endocarditis). Along with fever, the appearance or change of heart murmurs, the presence of hepatosplenomegaly, and damage to the nervous system, thromboembolism with blockage of large vessels of the extremities is often observed.
Recognizing the etiology of this endocarditis is very difficult. The ineffectiveness of antibiotics, progressive deterioration of the condition in the absence of acceleration of ROE, uveitis or endophthalmitis may give rise to the assumption of the presence of endocarditis caused by fungi. Isolation of fungi from blood is very difficult and is rarely possible, even when using special methods.
Fibroplastic parietal endocarditis with eosinophilia (Leffler's endocarditis) is characterized by damage to the parietal endocardium with severe fibrosis and thickening, which impairs the compliance of the heart chambers and leads to the development of heart failure. The disease is accompanied by high eosinophilia in the blood, as well as the development of widespread eosinophilic vasculitis in the skin, muscles, and internal organs.
The disease was first described in 1936 by W. Loeffler and is classified as rare. Its etiology is unknown. It has been suggested that Loeffler's endocarditis and endomyocardial fibrosis, described in 1948 by D. Davis, widespread in some areas of South Africa, represent a single form of pathology.
In the pathogenesis of the disease, disturbances in immunological reactions are apparently of great importance, as indicated by the frequent detection in patients of a decrease in complement titer, LE cells, and changes in the level of immunoglobulins. The clinical picture is characterized by pronounced polymorphism. Often the first manifestation of the disease is high eosinophilia in the blood; severe fever (in acute cases) and thromboembolism of blood vessels in different areas are possible.
Signs of heart damage, in particular the appearance of cardiac murmurs due to damage to the chordae tendineae or the formation of mitral, or less often tricuspid, valve insufficiency, are detected in the first weeks of the disease, but may appear only after a few months. Subsequently, the disease is characterized by increasing heart failure, refractory to cardiac glycosides, and high eosinophilia.
In this case, damage to the skin, muscles, kidneys, liver, and lungs may occur, caused by the development of eosinophilic vasculitis in them (so-called eosinophilic collagenosis). The diagnosis is not difficult in cases where, against the background of hypereosinophilia, signs of heart damage with the development of heart failure are revealed.
In the acute course of the disease, the differential diagnosis is made with periarteritis nodosa, which often (especially in the case of lung damage) occurs with hypereosinophilia (see Periarteritis nodosa). The diagnosis of the latter is helped by identifying paresis of peripheral motor nerves, signs of kidney damage, large arteries, and arterial hypertension.
With hypereosinophilia, there is often a need to exclude parasitic diseases - strongyloidiasis (see), opisthorchiasis (see), fascioliasis (see). Treatment of Loeffler's endocarditis consists of long-term use of glucocorticoid hormones, and in some cases, cytostatics. If heart failure occurs, the use of cardiac glycosides and diuretics is indicated.