Right ventricular hypertrophy is an increase in myocardial volume and mass due to thickening of muscle fibers. Develops due to myocardial overload with volume or pressure.
At the same time, pulmonary pressure increases and the gap between upper and lower blood pressure decreases. With such changes in the cardiac system, health deteriorates sharply, and the load on the heart rapidly increases.
The mechanism of pathology development
The pathogenic process is formed in several stages. In any case, the basis is an increase in blood pressure. This is not an axiom, there is another option.
As blood pressure rises, a change occurs in the entire bloodstream. Liquid connective tissue is thrown into the chambers with great force.
The impact also occurs on the mitral valve, but the right ventricle takes the main blow.
This chamber is responsible for the release of blood into the small or pulmonary circle.
As a result of the influence of certain factors, the vessels narrow and resistance increases.
The body compensates for the condition by intensifying contractions and greater force of blows. The heart, unable to work in this mode for a long time, builds muscle mass.
Due to the proliferation of new cardiomyocytes (active heart cells), an anatomical defect occurs - hypertrophy. If it is isolated, there is no significant difference in functional activity.
The second option is excess volume. If there is a lot of blood coming in, the heart cannot adequately pump it around the body.
Dilation occurs (expansion, enlargement of the chamber) and proliferation of the myocardium, as a compensatory mechanism. This condition occurs mainly in athletes and manual workers.
The danger of this condition
Any disturbances in the functioning of the heart have serious consequences, because it is this organ that provides our body with oxygen. An increase in the right side indicates that the load on this area increases significantly. Subsequently, the heart may no longer cope with a large amount of work. There are disruptions in the functioning of the heart muscle and arrhythmia.
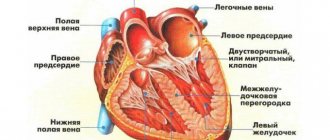
The walls of the chambers of the heart consist of muscle tissue - the myocardium, which allows them to push blood into the vessels when contracting. For various reasons, the chambers of the heart may experience increased stress, which affects the structure and function of the heart.
The human heart consists of four chambers: two atria and two ventricles, which, alternately contracting, pump blood throughout the body. The largest vessel, the aorta, departs from the left ventricle. From the aorta, oxygen-rich arterial blood flows to all cells and tissues of the human body.
As soon as gas exchange has occurred in the blood, the blood has given up oxygen and is saturated with metabolic products and carbon dioxide; it flows through the superior and inferior vena cava into the right atrium. This closes a large circle of blood circulation that connects the left ventricle and the right atrium. Thus, venous blood from tissues and organs enters the right atrium.
Types of hypertrophy
Based on the mechanism of development of the pathological process, two forms of deviation are distinguished. They have already been named.
- The first is hypertensive. The essence is an increase in pressure, narrowing of blood vessels, including the pulmonary arteries. Blood does not flow in sufficient quantities due to the resistance of the stenotic (narrowed) hollow structures. Hence the need for greater blood pressure to push an adequate volume into the channel.
Symptoms of this form develop almost immediately: shortness of breath, rhythm disturbances, chest pain.
However, episodic manifestations. Only in the later stages do they stabilize and haunt the person constantly.
- The second is dilation. A combined process arises. On one side, the right chamber stretches, increases in volume and fills with blood. Hence the increase in pressure at the local level. The further scheme is identical.
Regardless of the form, the condition will require mandatory treatment.
Attention:
RVH is the first step towards heart failure. Once it develops, it is no longer possible to radically help. The likelihood of death increases dramatically.
Is the condition dangerous if a load on the right atrium is detected on the ECG?
If the right atrium (RA) is overfilled with blood or pressure overload, myocardial hypertrophy subsequently occurs. Signs of this condition are shortness of breath, dizziness, fainting, and irregular contractions. Treatment requires an impact on the disease that caused overstrain of the heart muscle (lung disease, valvular heart disease).
Causes of increased load on the right atrium of the myocardium
In order for the load on the cardiac muscle of the RA to increase when blood is ejected into the ventricle, the pressure in it must increase due to an obstruction (tricuspid valve stenosis) or the blood volume must increase.
This situation occurs with reverse reflux (valvular insufficiency), high pressure in the right ventricle (heart defects).
Diseases leading to overload, and subsequently hypertrophy of the PP, may differ in adulthood and childhood.
In adults
The most common pathologies accompanied by a large load on the right atrium:
- chronic bronchitis (obstructive);
- bronchial asthma;bronchial asthma
- emphysema of pulmonary tissue;
- hardening of the lungs (pneumosclerosis);
- multiple cysts;
- bronchiectasis;
- tuberculosis infection;
- sarcoidosis;
- pneumonia;
- occupational lung diseases;
- chest injuries and deformities, operations;
- obesity;
- pulmonary hypertension (primary and secondary forms);
- autoimmune diseases;
- thrombosis, embolism and atherosclerosis of pulmonary vessels;
- tumors in the chest.
All these processes disrupt the ejection of blood from the right ventricle into the lungs, which leads to its overstrain and subsequent hypertrophy, and the RA is affected for the second time.
Also causes of pathological changes include rheumatism, endocarditis involving the tricuspid valve.
Excessive load on the RA occurs with tricuspid stenosis, insufficiency and combined acquired defect of this valve.
We recommend reading the article on myocardial hypertrophy. From it you will learn about the mechanism of development and types of myocardial hypertrophy, as well as about the diagnosis and treatment of the disease.
And here is more information about left atrial hypertrophy.
The child has
The first place among the factors of PP overload is taken by heart defects, in which circulatory disorders occur in the pulmonary circulation:
Right atrium overload
The addition of hypertrophy of the right parts of the heart occurs with decompensation of circulatory failure of the left ventricular type. This is due to the increase in congestion in the lungs, which over time complicates the work of the right atrium.
Signs and symptoms of stress
If overstrain of the PP occurs against the background of acute inflammatory processes or exacerbation of bronchial asthma, bronchitis, then there are no characteristic symptoms, or the overload is manifested by an excessive increase in shortness of breath during physical activity. If the underlying diseases are heart defects, then the signs are:
- increasing weakness and fatigue;
- cardiopalmus;
- pain and heaviness in the liver area;
- indigestion;
- cyanotic or icteric skin tone;
- swelling in the legs;
- accumulation of fluid in the abdominal cavity;
- pulsation of neck veins.
Is it dangerous
Increased load on the right atrium does not have negative consequences if it is possible to eliminate its cause - through medical or surgical treatment of the underlying disease. With unoperated heart defects, heart failure and congestive processes in the internal organs develop quite early, many of which have irreversible consequences.
In the later stages, fluid accumulates in the abdominal cavity (ascites), chest (hydrothorax), pericardial sac (hydropericardium), liver cirrhosis and severe rhythm disturbances occur.
ECG readings of load on the right atrium
Short-term manifestations of PP overload can be detected by recording an ECG at the time of an asthma attack, thromboembolism, or extensive pneumonia:
- pulmonary (pulmonary) P wave;
- increase in the first (right atrial part) P;
- high and pointed P in leads 2 and 3, aVF.
These symptoms disappear after the patient’s condition normalizes, or their severity decreases significantly. With hypertrophy, the P waves are high-amplitude, pointed, and have a normal duration.
ECG changes with increasing pulmonary hypertension and chronic overstrain of the RA are usually combined with symptoms of right ventricular hypertrophy . If an overload is detected, chest X-ray, cardiac ultrasound with Doppler ultrasound, CT and MRI are indicated to find the cause of the abnormalities.
How to reduce indicators
To correct circulatory disorders due to heart defects, surgical treatment with plastic surgery or valve replacement is required.
For lung diseases, anti-inflammatory therapy is needed, the use of drugs that dilate the bronchi and improve the function of external respiration (Teopek, Eufillin).
For the treatment of pulmonary hypertension, vasodilators (Corinfar retard, Diacordin), diuretics (Lasix, Veroshpiron), and oxygen inhalations are prescribed.
A decrease in the manifestations of heart failure occurs with the use of ACE inhibitors (Diroton, Enap), beta blockers (Corvitol, Concor), angiotensin antagonists (Lorista, Diovan).
We recommend reading the article about heart dilatation. From it you will learn about the types of heart dilatation, symptoms, as well as methods for diagnosing and treating the disease.
And here is more information about right ventricular hypertrophy.
High load on the right atrium occurs in diseases of the lungs and heart. It can be temporary or permanent, leading to myocardial hypertrophy. Often appears secondary to overstrain of the right ventricle.
Clinical symptoms (shortness of breath, cyanosis, edema, liver enlargement) occur when heart failure occurs. To identify it, it is enough to conduct an ECG, but to find the cause, additional examination is required. Treatment depends on the underlying pathological condition.
Watch the video about atrial hypertrophy on the ECG:
Source: //CardioBook.ru/nagruzka-na-pravoe-predserdie-na-ekg/
Causes
Numerous, almost always pulmonary, less often vascular and cardiac. But not all are pathogenic.
Sports activities
The first and most pronounced factor is long-term sports at a professional or amateur level. Not just activity, but grueling training to the limit.
If you look at the Borg scale, it’s 7-10 points. Essentially wear and tear on the body.
The body is not adapted to such extreme overloads. The heart responds accordingly with a dilated form of right ventricular hypertrophy.
The body has its own margin of safety, relatively speaking. Having crossed a certain line, it cannot perceive activity at the same level. Possible heart attack, dangerous arrhythmia, acute asystole.
Manual workers are also at risk, but not to the same extent. In any case, the question of the possibility of continuing this lifestyle is decided at an appointment with a cardiologist after diagnosis.
Pneumonia
Especially with frequent relapses. Another name is pneumonia. Develops as a result of damage by bacteria, less often by viruses.
There is a narrowing, then destruction and scarring of active tissues. The vital capacity of the lungs decreases, hence respiratory failure. A small amount of oxygen leads to increased pressure in the artery of the same name.
And further along the chain: all the vessels of the small circle suffer, they become stenotic and narrow. This leads to an increase in pressure in the right ventricle, and the tissues grow.
A one-time disease, especially in the acute phase, can result in cor pulmonale, but persistent anatomical defects are extremely rare.
Chronic obstructive disease (COPD)
The development pattern is approximately the same. With one exception - this diagnosis is made once and for life. Treatment helps correct the condition, but does not eliminate it.
Sooner or later, patients begin to develop cardiovascular problems.
Since many people turn to a pulmonologist after many years of stable progression of COPD, a whole bunch of diseases of different profiles are diagnosed.
The main contingent of patients are heavy smokers and workers of hazardous chemical, textile, and metallurgical enterprises.
Bronchiectasis
Formation of pus-filled cavities - “bags”. After opening, including as part of treatment, they disintegrate. Large tissue defects remain, shaped like tuberculosis cavities.
Emphysema
It is similar in nature to the previous process. Only a pathological expansion of the alveoli occurs, their rupture and the formation of cavities that do not participate in normal activity.
It is also impossible to help radically. Lifelong maintenance therapy is required.
If started early, the prognosis is good. The main contingent is the same - smokers, workers in hazardous industries.
Asthma
Usually of allergic origin. Rapid narrowing of the bronchi due to exposure to a negative factor. The quality of breathing decreases, gas exchange worsens.
Advanced forms are not fully controlled even with hormonal drugs. Attacks occur several times a day, including at night.
Persistent respiratory failure of degrees 1-3 develops. The pressure in the pulmonary artery and pulmonary vessels increases.
The right ventricle enlarges, CPS (chronic cor pulmonale) is diagnosed. In rare cases - acute form.
Cystic fibrosis
A chronic condition affecting the digestive tract as well as the lungs.
All diseases of the respiratory system are characterized by one phenomenon, common in symptoms. It is characterized by a stable increase in pressure and a change in cellular structure.
We're talking about cor pulmonale. Acute rarely leads to visible defects in the organ. Chronic pathology is much more dangerous.
Heart defects
Congenital defects of cardiac structures are represented by a group of disorders, for example, tetralogy of Fallot and others. As a rule, patients with severe abnormalities in heart development die within the first year without urgent treatment, sometimes faster.
Acquired defects are much more common. For a long time they do not produce symptoms and remain unnoticed until the last moment.
The diagnosis can be made based on the results of an autopsy (autopsy). If you're lucky, earlier, when cure is still possible. Therefore, it is recommended to undergo regular preventive examinations.
Mitral valve insufficiency is a special case. Accompanied by reverse blood flow or regurgitation.
Disturbances in the functioning of the tricuspid valve (three leaflets) affect approximately the same way, but cause hypertrophy of the right ventricle more often.
It is extremely rare that tumors are the culprits of the defect. The heart itself or the respiratory organs. They are easily determined by the results of a simple x-ray or echocardiography. It is already more difficult to say about the histological structure; a biopsy will be required.
Diagnostic methods
Most often, a comprehensive examination is performed to detect right ventricular hypertrophy, since ECG data does not always allow it to be detected. This is due to the fact that the mass of the left ventricle is larger, its potentials overlap the signs of enlargement of the right part. In the most typical cases, we can talk about an increase in the mass of the right ventricle if the following signs are present:
- deviation to the right of the electrical axis up to 100 degrees (on average);
- in three standard leads deep S;
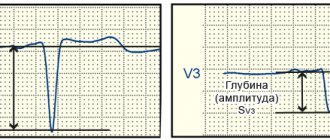
- high R in V1 (occurs with congenital defects) or large amplitudes of S and R (with mitral disease and lung diseases);
- along with the increased amplitude of the ventricular complex, the ST shifts and the T wave becomes negative.
Chest X-ray
To clarify the diagnosis, patients undergo chest X-ray , which provides information about the structure of the lung tissue, the presence of pathological changes in the respiratory tract and the expansion of the cardiac shadow due to myocardial hypertrophy.
Using ultrasound, the thickness of the walls of the heart chambers, the presence of valve defects, reverse blood flow, cardiac output, and myocardial contractility are determined. To detect changes in the liver, an additional ultrasound of the abdominal organs may be prescribed.
Cardiac catheterization, ventriculography, myocardial scintigraphy, angiography, and MRI are recommended for candidates for cardiac surgery. Also, when making a diagnosis and determining treatment tactics for inflammatory lesions of the myocardium and valves, the blood is examined for the level of leukocytes, ESR, C-reactive protein, and a coagulogram is prescribed. To study lung function, spirometry, blood gas analysis, and sputum analysis are performed.
Symptoms
Signs of HPV are relatively easy to identify. But they are nonspecific, therefore they are associated with a lot of conditions, and differential diagnosis is required. It’s impossible to say anything for sure based on signs alone.
The clinical picture includes:
- Regular chest pain. The intensity is minimal. The discomfort is burning, pressing. They resemble angina, but are weaker and last longer.
- Tachycardia. Heart rate varies from 100 to 150 beats per minute. Sinus type, paroxysms are extremely rare. There is a possibility of atrial fibrillation, which significantly worsens the prognosis and indicates the onset of heart failure.
- A drop in blood pressure followed by an increase. The level is unstable. The assessment is carried out over time.
- Cough. Dry, unproductive. A small amount of blood may be released. An alarming sign. Requires mandatory differential measures, since we may be talking about a tuberculosis process.
- Dyspnea. Decreased exercise tolerance. The patient is unable to walk normally, let alone play sports. The disturbance is observed even at rest.
- Fatigue, drowsiness, weakness for no apparent reason. The patient is unable to perform daily activities. Over time, a once healthy person without treatment turns into a deeply disabled person.
These symptoms are accompanied by signs of the underlying process itself. Against the background of bronchopulmonary pathologies, suffocation, impaired gas exchange of an objective nature (decrease in the level of oxygen saturation in the blood), cough, whistling, and wheezing are noted.
Thickening of fingers and nails is possible. Pallor of the skin, cyanosis of the nasolabial triangle.
Against the background of hypoxia (oxygen starvation), fainting develops, often repeatedly. Headaches, vertigo, and inability to navigate in space should alert the patient and his doctor - this is a direct indication of cerebral ischemia.
There is a high probability of a stroke. It is difficult to say in what time frame; it is necessary to evaluate all factors: from age to the moment of development of pathology. Read about the signs of a pre-stroke condition here.
Diagnostics
It is carried out under the close supervision of a cardiologist. It is possible to involve a specialist pulmonologist, a doctor to identify and treat pathologies of the bronchi and lungs, and the respiratory system as a whole.
An approximate list of activities consists of the following components:
- Oral survey regarding complaints. When did it arise, how much does it interfere, are there any breaks in the clinic?
- Anamnesis collection. Lifestyle, bad habits, past pathologies, current diseases, nature of professional activity, leisure time and other points.
- Measurement of blood pressure, heart rate. Using routine methods.
- 24-hour Holter monitoring. Using a special programmable device with sensors, pulse and blood pressure are recorded. In 24 hours. It is better if the patient is in a familiar environment, at home or at work. This will help detect deviations much more accurately.
- Electrocardiography. Study of the functional status of the heart. Used as a second method. Gives an idea about arrhythmias.
- Echocardiography. Used to identify anatomical disorders. The main method of early diagnosis or determination of the severity of the disease.
- Spirography. The respiratory function is subject to assessment, that is, how much the ability of the entire system to adequately operate is preserved. For a more accurate result, it is carried out with a sample of drugs like Salbutamol (with a load).
- Auscultation. Listening to heart sounds.
- X-ray of the chest organs.
- MRI of the same area. CT is often used to verify problems with pulmonary structures.
It is possible to prescribe a general blood test, biochemistry, and hormonal tests. As needed.
Attention:
Fluorography cannot replace x-rays, so doctors offer it for routine detection of gross, advanced defects. This is more of a formality than a real diagnosis.
Treatment of hypertrophy
The operation can be performed in two ways. During the first, the chest is cut and blood circulation is stopped for some time. At this time, defects are eliminated or an organ transplant occurs. The second type of intervention is performed through an artery (femoral) or vein (jugular). At the same time, the heart continues to work as usual, with minimal trauma. If the disease is detected on time, then it responds well to treatment. Regular visits to the doctor and taking medications are the measures that can stop the enlargement of heart tissue.
Signs on ECG
The features on the cardiogram are:
- Change in the width of the QRS complexes, its significant deformation. Especially in leads V1, V6.
- Incorrect placement of STV1, 6, SV1, 6 segments.
Changes can be detected in this way only in moderate and severe forms of the pathological process. The technique is not suitable for early diagnosis due to insufficient information content.
However, signs of right ventricular hypertrophy on the ECG are taken into account and compared with the results of echocardiography.
If there is a significant discrepancy, they focus on the worst option and make a diagnosis based on it. But then you need to re-evaluate the condition; perhaps a mistake was made.
Features of the pathology, the degree of its development
With the disease in question, cardiologists record the growth of the myocardium. It can provoke many violations. Enlargement of the right ventricle (RV) is usually associated with the growth of cardiomyocytes.
When conducting a cardiogram in healthy people, doctors often observe increased signals from the left side. It is considered to be stronger. Experts explain this feature by the large weight of this area. It is 3 times larger than the right one. Signals from the LV always predominate in the electrocardiogram. Sometimes this norm is violated. This is explained by the development of right ventricular hypertrophy.
Experts distinguish 3 degrees of the pathology in question:
- Sharply expressed. A noticeable increase in pancreas weight is recorded. It is much heavier than the left ventricle (LV).
- Classic. This situation is characterized by an increase in the pancreas, but this area is lighter than the left one. Excitation in the pancreas is much longer lasting.
- Moderate. Doctors record the growth of the pancreas visually. The mass remains less than that of the left section.
Overload of the right zones of the heart muscle is considered a serious symptom. It is much more dangerous than overloading the left half of the muscle. This is explained by the work of this area with the pulmonary circulation. Usually there is insignificant load in it, so pulmonary stenosis and the discharge of excess blood from the LV increases the load. The pancreas is not used to it, it is unable to withstand it. Therefore, it increases its size and mass. Thus, pancreatic hypertrophy occurs.
Hypertrophy of the right ventricular wall
Cardiologists can detect signs of RPG using an ECG. Electrocardiography is considered the leading method of initial diagnosis. But this method cannot indicate the exact dimensions of the ventricle being studied. It only shows conductivity disturbances caused by changes in size. This research method is considered indirect, capable only of showing signs of pathology. But he cannot provide more detailed information.
Echocardiography is considered a more accurate diagnostic method. When studying the heart using ultrasound, the size of the cardiac muscle chambers is assessed, the location of defects is determined, and blood discharge is established. It is also possible to determine the pressure inside the chambers.
Treatment
Carried out by a group of methods. The basis is eliminating the root cause. Medicines are usually used. Which ones exactly depend on the diagnosis.
Basic therapy is required against the background of bronchopulmonary problems; the issue of selecting medications is decided by the doctor, since there are a lot of options.
As for the symptomatic measure, it is aimed at relieving manifestations and preventing dangerous complications.
What drugs are used to treat:
- ACE inhibitors. Like Prestarium and its analogues. Help eliminate excess pressure in the bloodstream.
- Calcium antagonists. Verapamil, Diltiazem, others with great caution.
- Centrally acting medications. Moxonidine.
- Nitroglycerin to relieve attacks. It is possible to use analogues in the group.
- Cardioprotectors. Mildronate and others. To restore metabolic processes.
- Diuretics as needed. These products are not suitable for continuous use.
Surgical treatment is rarely indicated to eliminate anatomical defects and defects. The issue is decided at the discretion of the practicing operating cardiologist.
If right ventricular hypertrophy occurs as a result of long-term grueling physical training, a significant reduction in the intensity of exercise is indicated.
Although this is a physiological variant of the deviation, its naturalness is very conditional. With further progression, which will inevitably happen, the patient's death is likely. GPG is the basis for exclusion from professional and even amateur sports.
Forecast
Depends on the diagnosis. Against the background of potentially incurable pulmonary conditions, the likelihood of complete recovery is minimal. But you can take control of the disease.
Symptomatic and etiotropic therapy are associated with high survival. The risk of death is about 7%, approximately 1-3% during supervision, which is quite small, considering the essence of the pathological process.
If heart failure begins, the outcome worsens significantly. The probability of death is 20-25% or higher.
Negative factors based on age, gender, physical condition, general history, family history, lifestyle, addictions, and other factors are taken into account.
The response to the treatment is also taken into account, and whether there is a possibility of radial intervention. As a result, a complex, systemic picture emerges. It will not be possible to average it; a qualified assessment by a specialist is needed.
Possible complications
Among the consequences:
- Heart failure. As a result of overload and the development of dangerous forms of arrhythmia.
- Heart attack. Death of active cells of cardiac structures. If the patient does not die, coronary heart disease occurs, which at a minimum significantly worsens the quality of life.
- Stroke. Necrosis of cerebral structures with the formation of a persistent neurological focal defect. Death is also possible, depending on the extent of the lesion and location.
- Vascular dementia.
- Pulmonary edema.
- Asthma.
Preventing dangerous complications is perhaps the main goal of treatment. Because it is these consequences that lead to death.
Hypertrophy of the right ventricle of the heart is the result of bronchopulmonary pathologies or defects of cardiac structures, less often the own achievement of a patient with sports merits.
Despite the relatively favorable prognosis, we cannot relax. Without treatment, the condition develops into a deficiency, which is almost guaranteed to lead a person to the grave sooner or later.