- Amoebic meningoencephalitis
Meningoencephalitis is an inflammatory process affecting the membranes and substance of the brain. Despite the fact that the brain is protected by the blood-brain barrier, which prevents most foreign and toxic substances from entering it, some pathogens are still able to pass through it and cause inflammation. Meningoencephalitis, given the importance of the anatomical area it affects, is a life-threatening disease.
Meningoencephalitis is characterized primarily by headache and various nervous system disorders
Causes and risk factors
Meningoencephalitis is most often infectious, but can also be toxic and autoimmune.
Infectious inflammation can be triggered by viruses, bacteria, fungi, protozoa and parasites.
The most common infectious agents of meningoencephalitis are:
| Bacteria | Viruses | Protozoa |
| Neisseria meningitidis, Listeria monocytogenes, Rickettsia rickettsii, Rickettsia conorii, Rickettsia africae, Ehrlichia chaffeensis, Mycoplasma pneumonia, Treponema pallidum, Mycobacterium tuberculosis, Borrelia burgdorferi, Leptospira. | Epstein-Barr virus, herpes simplex virus type 1 and type 2, enterovirus, rabies virus, tick-borne encephalitis virus, West Nile virus, measles virus, varicella zoster virus, mumps virus, HIV. | Naegleria fowleri, Balamuthia mandrillaris, Sappinia Diploidea, Trypanosoma brucei, Toxoplasma gondii. |
Infectious (parasitic) pathogens include Halicephalobus gingivalis from the class of nematodes, the causative agent of cysticercosis (Taenia solium), and echinococcus.
The disease can be caused by the fungus Cryptococcus neoformans. It should be noted that meningoencephalitis of parasitic and fungal origin is extremely rare.
Autoimmune inflammation is spoken of when the cause of tissue damage, in this case the brain tissue and its membranes, is an attack of one’s own immune system. Autoimmune encephalitis can be caused by antibodies to amyloid beta peptide proteins, antibodies to anti-N-methyl-D-aspartate receptor (anti-NMDA; anti-NMDA receptor encephalitis), and several others.
In extremely rare cases, post-vaccination meningoencephalitis occurs.
Treatment of meningoencephalitis
Therapy of the disease is carried out in several directions at once: etiotropic, symptomatic and pathogenetic. The first type of treatment involves eliminating the cause of the disease. Depending on it, the following medications are used:
- Antifungal. Indicated for the treatment of fungal inflammation of the membranes and substance of the brain. Fluconazole and Amphotericin B are considered effective.
- Antibacterial. Used for bacterial diseases. Antibiotics include cephalosporins or their combination with penicillins, more often with Ampicillin. Before receiving the results of an analysis to identify the type of pathogen, the doctor prescribes a broad-spectrum antibacterial agent. After determining the type of infectious agent, therapy is adjusted taking into account the sensitivity of bacteria to specific drugs.
- Antiviral. For the herpetic form of the disease, Ganciclovir is used, for the arboviral form, Ribavirin is used. Among antiviral drugs, Acyclovir is most often prescribed. It increases the patient's chances of life, but does not protect against severe meningeal consequences. Antiviral therapy is combined with immunomodulatory drugs such as Interferon.
- Antiparasitic. They are prescribed for brain damage by amoebas or toxoplasma. They are often used together with antibiotics and antifungal drugs.
The second direction of treatment of the disease is pathogenetic. It is carried out to eliminate the main meningeal symptoms. The objectives of such therapy:
- Relieving cerebral edema. For this purpose, diuretics are used, which increase the amount of fluid excreted in the urine. As a result, brain swelling decreases. Additionally, glucocorticosteroids are used - hormonal agents that have a strong anti-inflammatory effect.
- Preservation of the vital activity of brain cells - neurons. To achieve this goal, the patient is prescribed neurometabolic and neuroprotective drugs.
The last direction of treatment is symptomatic. The goal is to eliminate signs of the disease and alleviate the patient’s condition. Taking into account the manifestations of the disease, a person may be prescribed the following drugs:
- psychotropic;
- anticonvulsants;
- antipyretics (antipyretics);
- improving the activity of the cardiovascular system;
- sedatives;
- antioxidants;
- improving blood microcirculation;
- multivitamins;
- anticholinesterase.
Stages of the disease
During meningoencephalitis, the beginning (the appearance of the first signs), the height and the outcome are distinguished. Infectious types of disease also have a prodromal, or latent (latent) stage, which can be asymptomatic or have minor and nonspecific clinical manifestations. The latent period, i.e. the time from infection to the appearance of the first signs of the disease, can last from several hours to several months, depending on the etiology. The height of the disease is characterized by severe and progressive symptoms. The outcome can be recovery or death if brain damage reaches a critical level and affects vital centers.
Some types of disease have stages that are characteristic of them. For example, during meningoencephalitis, three periods are distinguished: the precursor stage (corresponding to the prodromal stage), the stage of excitation, and the stage of paralysis.
Pathogenesis of the disease
The brain and spinal cord are covered by 2 types of membranes: hard and soft. Depending on which membranes of the brain were inflamed, the following types of meningitis differ:
- Pachymeningitis. This type of pathology develops when the dura mater is damaged. Very rare.
- Meningitis. The disease is diagnosed by inflammation of the soft membranes. This is the most common form of meningitis.
- Panmeningitis. It is detected when the infection captures the hard and soft membranes at the same time.
Meningitis is one of the most dangerous diseases. Before the advent of antibiotics, this disease led to the death of 95% of patients. A significant decrease in death statistics occurred only after the invention of penicillin.
Today, doctors successfully fight meningitis using powerful synthetic drugs. Moreover, vaccines have been developed against the most active pathogens of the disease, which help prevent the development of pathology.
Outbreaks of meningitis are seasonal. Most patients are identified between November and April. This frequency is due to vitamin deficiency, large crowding of people in the premises, and insufficient ventilation of buildings.
According to scientists, this disease has an annual cycle. Once every 10 years there is a significant increase in incidence.
Primary meningitis is an infectious disease. It is caused by viruses and bacteria and spreads in the following ways:
- Airborne. The causative agent of the disease enters the external environment when coughing and sneezing.
- Contact and household. The infection can be transmitted through direct contact with its carrier or through the use of common household items.
- Oral-fecal. We are talking about non-compliance with hygiene rules: eating food that has not been processed; eating with unwashed hands, etc.
- Hematogenous. The infection spreads throughout the body through the bloodstream.
- Lymphogenic. The disease spreads through the lymph flow.
- Placental. The infection is transmitted to the baby through the placenta or during movement in the birth canal.
- Oral. Infection occurs through ingestion of untreated water or swimming in dirty bodies of water.
The disease develops gradually. The infection first enters the child's body through the lungs or gastrointestinal tract. Then it takes hold in the body and begins to multiply. At a certain point, infectious agents are carried through the bloodstream throughout the body and reach the meninges of the spinal cord and brain. Direct inflammation of these membranes occurs only if the infection manages to overcome the blood-brain barrier. After this, the patient experiences the first symptoms of meningitis.
The full clinical picture of the disease becomes visible after the waste products of bacteria cause irritation of the ventricles in the brain. This will provoke an excess of cerebrospinal fluid, which, in turn, causes hypertensive-hydrocephalic syndrome.
Symptoms
The clinical picture of meningoencephalitis is generally similar to that of meningitis. Common signs are changes in personality, behavior, disturbances in thinking, as well as physical symptoms: intense headache, neck pain, stiff neck muscles, hypersensitivity to light and sound stimuli, convulsions. An increase in cranial pressure as a result of inflammation is manifested by blurred vision, dizziness, and nausea.
Let us take a closer look at the clinical manifestations using examples of some types of meningoencephalitis.
Tick-borne meningoencephalitis
Inflammation of the brain and its membranes, caused by a viral infection transmitted by ticks, begins acutely, with an increase in body temperature to feverish values (38 ° C and above), chills, severe malaise, headache accompanied by nausea and vomiting, pain and aches in the muscles and joints. The initial stage is characterized by hyperemia of the face, neck and upper chest, mucous membranes, scleral injection (bleeding in the eyes), inhibited consciousness, which can later turn into a coma. Later, muscle weakness, paresthesia (tingling, numbness) appears, then these muscle groups undergo paresis and paralysis.
Ticks are carriers of viral encephalitis pathogens
Herpetic meningoencephalitis
It has a prodromal (latent) period, lasting several days, during which increasing malaise is noted: body temperature rises, headache, nausea, sometimes vomiting, weakness, fatigue. There are behavioral disturbances that gradually progress, as well as hypersensitivity to external stimuli, especially odors, which can later transform into olfactory hallucinations. In some cases, there is no prodromal period. The height of the disease is characterized by local neurological symptoms (unilateral paralysis, paresis), cognitive impairment (disorders of thinking, memory), lethargy, and the appearance of seizures.
Meningoencephalitis caused by the rabies virus
The onset of the disease is characterized by the appearance of anxiety, increased sensitivity to external stimuli (light, sound, tactile), a slight increase in body temperature, and sleep disturbances. Appetite decreases, dry mouth appears, sweating, tachycardia, sore throat when swallowing, and sometimes nausea. Changes in behavior are noticeable; the patient becomes nervous, rude, irritable, and avoids contact with people.
At the stage of excitation, neurological symptoms develop, photophobia, exophthalmos, breathing disorders appear, and body temperature rises. A characteristic symptom of hydrophobia is: the patient is thirsty, but when he tries to drink, he experiences a strong, very painful spasm of the muscles of the pharynx and larynx, this phenomenon increases, and later the spasm can be caused by just the sight of water, its murmur, or the mention of it. As the disease progresses, painful spasms of the muscles of the pharynx and larynx occur in response to any irritant, even a breath of wind. The patients do not have enough air, and they begin to rush about, looking for a position in which relief will come, which is perceived by others as an attack of rabies. Patients may experience hallucinations and delirium. If death does not occur at this stage, the stage of paralysis develops, during which the patient becomes motionless and stops responding to light. Due to damage to the pelvic nerves, urinary and fecal incontinence develops. Body temperature continues to rise (42 °C). And although it becomes easier for the patient to breathe and drink, this stage ends in death.
Clinical manifestations
Meningoencephalitis is a disease that is characterized by a certain symptom complex, which allows one to suspect pathology before receiving the result of a cerebrospinal fluid analysis. General cerebral signs:
- Pain in the head area of a bursting, widespread nature. Patients describe the painful sensations as excruciating, unbearable, and intense.
- Vomiting attacks, often spontaneous, without preceding nausea, do not lead to relief.
- Psychomotor agitation, agitation, followed by periods of depression of consciousness (stupor, stupor, coma).
- Delirium, hallucinations.
- Convulsive syndrome.
Meningeal symptoms of meningoencephalitis in adults and children include hyperesthesia (increased sensitivity) to light, sound stimuli, and tactile touch. Other meningeal signs:
- Tension of skeletal muscles of the tonic type (muscle rigidity in the back of the head, difficulties when trying to tilt the patient’s head towards the chest).
- Kernig's sign. Painful sensations and involuntary resistance to attempts to passively straighten the leg, previously bent at the joints of the knee and hip.
- Brudzinski's sign. An attempt to passively tilt the patient's head towards the chest is accompanied by an uncontrolled pulling of the lower extremities towards the abdomen, bending them at the joints of the knees and hips.
Rigidity (inflexibility, tension) of the skeletal muscles in the back area leads to a forced posture known as the “pointing dog.” In this case, the patient’s back is maximally straightened, the head is thrown back, the lower limbs are bent at the knees and pulled towards the stomach.
Meningoencephalitis in newborns is manifested by Lessage's symptom - holding the child in a suspended state with fixation by the armpits is accompanied by a reflex pulling of the lower limbs bent at the knees towards the stomach while maintaining a static pose. In a healthy baby, in this position, the legs hang freely and move.
Meningoencephalitis in infants is accompanied by swelling and protrusion of the fontanel, which is caused by an increase in intracranial pressure. Hydrocephalic syndrome is complemented by a “brain” cry - monotonous, constant, piercing sounds without changing intonation.
During the differential diagnosis, it is necessary to exclude diseases such as myositis (inflammation of muscle tissue, accompanied by pain and tension), radiculopathy (damage to the nerve endings of the spinal cord, manifested by disturbances in the innervation zone - pain in the joints and muscles, sensitivity disorder, motor dysfunction), which may cause muscle stiffness.
For meningococcal encephalitis, meningeal signs in the form of reflexively occurring pain syndromes are typical. Percussion (tapping) on the area of the zygomatic arches and the surface of the skull is accompanied by increased pain and the appearance of a painful grimace. Painful sensations arise as a result of pressure on trigger zones:
- Eyeballs covered by eyelids.
- Areas of innervation of the facial and occipital nerve.
- Anterior segment of the auditory canal.
Purulent meningoencephalitis, which is often caused by a bacterial infection, is manifested by changes in reflexes - tendon, periosteal (unconditioned reflexes obtained as a result of stretching of muscle fibers). At the initial stages of the disease, revival of reflexes is observed, at later stages – uneven extinction.
Purulent and serous meningoencephalitis are equally characterized by the appearance of signs of an infectious lesion - fever, general intoxication of the body, an increase in the size of the liver and spleen, which is revealed during palpation. Other typical symptoms: lymphadenopathy (increase in the diameter of the lymph nodes), exanthema (skin rash), enanthema (change in the appearance of the mucous membranes).
Meningococcal
Occurs mainly in newborns. The clinical picture is dominated by encephalitic signs - confusion, signs of damage to cranial nerves, convulsive syndrome, paralysis, paresis. Sometimes the symptoms are supplemented by ataxia (impaired coordination of movements) of the cerebellar type and decreased muscle tone. In this case, meningeal signs may appear weakly.
Impaired consciousness is of a different nature; signs are often observed: stupor, disorientation, unmotivated fear, delirium (disorder of attention, changes in emotions, perception, thinking), coma. The level of confusion correlates with the degree of damage to brain tissue. Stupor and coma usually occur against the background of cerebral edema. Confusion of consciousness and motor agitation accompany a condition such as infectious-toxic shock.
This form of meningoencephalitis is accompanied by mental disorders - hallucinations (auditory, visual), euphoria, amnesia, delirium, behavioral disorders. Patients with damage to the cortical area of the brain often experience aphasia (speech impairment), seizures, and hemiparesis (muscle weakness in one half of the body).
The clinical picture of damage to the deep structures of the brain includes extrapyramidal disorders (affecting the volume and quality of movements), hyperkinesis (pathological, uncontrolled movements), sleep disorder, severe thirst, stem-vestibular symptoms (nystagmus, dizziness, inability to hold a pose). In 7% of young patients, a complication occurs in the form of cerebral edema, which occurs within 1-2 days from the onset of symptoms.
In elderly patients, edema often develops after the first week and is accompanied by signs of intracranial hypertension and encephalopathy of infectious-toxic origin. In weakened children, subdural effusion (accumulation of cerebrospinal fluid in the space between the meninges) is often observed. The prognosis is relatively unfavorable. Deaths are common.
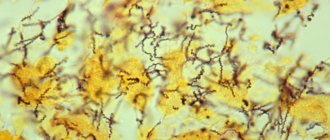
Amebic
Amoebic encephalitis is more often detected in the summer. The reason for suspicion is the fact that the patient bathed in fresh water bodies in July and August. This form is characterized by high mortality (up to 90% of cases). Without etiotropic treatment, death occurs within 1 week. The disease develops rapidly and suddenly. The onset symptoms resemble the development of pharyngitis - sore throat, dry cough, difficulty breathing, increased body temperature.
These symptoms are accompanied by painful, intense pain in the head area. Body temperature indicators quickly increase, reaching high values – 39-40°C. At the same time, signs are observed: repeated bouts of vomiting, confusion (stunning, stupor). The patient's perception of taste and olfactory stimuli is impaired. Meningeal signs are strongly expressed.
Mycoplasmosis
The mycoplasma form is rare. Meningeal syndrome manifests itself after 1-2 weeks of subacute, acute infection caused by mycoplasmas. The clinical picture is represented by intoxication syndrome, catarrhal symptoms (sore throat, dry cough, nasal congestion, lacrimation, hyperemia, redness of the sclera - the white membrane of the eye), myalgia (severe pain in the muscle area).
As meningoencephalitis progresses, symptoms are observed: intense pain in the head area, nausea, vomiting, smoothed meningeal signs. This form is characterized by a rapid (2-4 days) improvement in the patient's condition during therapy with antibacterial drugs. The prognosis is favorable with adequate treatment.
Brucellosis
Acute meningoencephalitis of brucellosis etiology is rare, as a complication of brucellosis in 1-5% of patients. The clinical picture shows weak signs of damage to the brain matter and membranes. Symptoms observed: moderate, persistent pain in the head area, increased body temperature, repeated bouts of vomiting, chills, increased sweating, asthenic syndrome (general weakness, apathy, drowsiness). Deaths are rare.
Aspergillus
A form of fungal etiology that develops as an endogenous (caused by internal factors) infection against the background of aspergillosis, which affects the external ear, paranasal sinus, and lungs. With this form, the severity of meningeal signs increases gradually. The pathology is characterized by the formation of hematomas, foci of abscess of epidural, subdural (between the meninges) localization at the base of the brain.
The number of deaths is about 50% of cases. Otogenic (the primary focus of infection is in the area of the hearing organs) secondary forms also include meningoencephalitis, which developed against the background of acute maxillary ethmoiditis (an inflammatory process in the maxillary and ethmoid sinuses), otitis (an inflammatory process in the ear area) of a chronic or acute form.
Herpetic
Herpetic meningoencephalitis occurs with a frequency of 10-20% in the general structure of viral forms. WHO data show that in terms of mortality, herpetic meningoencephalitis ranks second among all deaths associated with viral infection. The causative agent is the herpes simplex and herpes zoster virus, as well as chickenpox. Occurs with a frequency of 2-4 cases per 1 million population annually. About 30% of patients are children.
First of all, damage occurs to the mucous membranes, skin, central nervous system tissues, and organs of vision. More often it occurs in the classical version, accompanied by syndromes - meningeal, hyperthermic, clouding of consciousness, convulsive. It develops quickly, the debut symptoms are observed 1-5 days after the clinical manifestations of ARVI. Initial symptoms include a sustained increase in body temperature above 39°C.
It is not possible to lower the temperature even with the help of antipyretics. Impaired consciousness is manifested by lethargy, apathy, and lethargy. The progression of the pathology leads to deafness, stupefaction, manifested in a severe form - a coma.
Meningococcal meningoencephalitis
Damage to the brain and its membranes caused by meningococci is characterized by an acute onset - an increase in temperature to febrile levels, intense headache, and increased sensitivity to any irritants. A characteristic feature of this disease, which distinguishes it from meningoencephalitis of other bacterial etiologies, is that it is often combined with meningococcemia, i.e., the circulation of meningococci in the bloodstream. It is accompanied by the appearance of skin rashes, initially roseolous or roseolous-pustular, and later hemorrhagic, forming rather large blood-red or purple spots on the skin of irregular shape.
Viral meningoencephalitis (using the example of herpes)
Herpetic meningoencephalitis, the main cause of which is the DNA-containing herpes simplex virus of both the first and second types, can occur as an independent form (in adults against the background of a decline in immunity) or act as a component of a generalized viral infection (in newborns and young children age). It is known that HSV is detected in adults in more than 90% of cases. Due to the wide distribution of the pathogen, only a few manage to avoid encountering HSV, but the highest probability of “catching” it is present when passing through the birth canal of an infected woman and in early childhood (airborne transmission). The most dangerous is considered to be intrauterine infection of the fetus, which leads to serious consequences (up to 2/3 of newborns die in infancy, the rest face the fate of disabled children).
It is impossible to predict in advance what to expect from herpetic meningoencephalitis; its course is quite variable:
- Acute meningoencephalitis;
- Chronic process;
- The development of the disease under the guise of other pathological conditions of the central nervous system (neoplasms, epilepsy, strokes, dementia);
- Almost asymptomatic.
The first signs of this disease:
- Intense headache, localized in most cases in the frontal and parietal region;
- High body temperature;
- Impaired consciousness, changes in behavioral functions, up to complete inadequacy;
- General cerebral symptoms, against the background of which focal manifestations can often be observed.
The viral nature of the disease (especially in the case of acute meningoencephalitis) does not bode well for the patient: often DIC syndrome is added to the destructive changes in the brain, aggravating the patient’s already serious condition.
The therapeutic effect is carried out mainly through the antiviral drug - acyclovir (Virolex), which significantly increases the chances of life, but, unfortunately, does not protect against severe consequences.
Video: lecture on herpetic encephalitis in children
Features of the course of meningoencephalitis in children
The course of the disease in children is similar to that in adults, perhaps the difference is a more rapid course of the disease, but also a slightly better prognosis - children are less likely to develop long-term consequences, and they are usually transient in nature.
The disease begins acutely, with high fever (40-41 °C), severe headache, which is not relieved by analgesics and is accompanied by nausea and vomiting, which does not bring relief. The child may be inhibited or, on the contrary, excited; small children may scream monotonously (meningeal cry). Hallucinations, stupor, and coma may occur. Meningeal syndrome is pronounced (rigidity of the neck muscles, pointer dog position - on the side with the head thrown back and legs pulled up to the stomach, positive Kernig and Brudzinsky symptoms, paresthesia, pain phenomena). Seizures occur, but keep in mind that seizures in children can be caused by high fever (called febrile seizures), so they do not necessarily indicate brain damage and should only be assessed in conjunction with other symptoms.
Measles and chickenpox meningoencephalitis are more common in pediatric patients because they are caused by infections that mainly affect children.
Forms of meningoencephalitis
Table 1. Forms of meningoencephalitis and features of the pathology
| View | Nature of the disease |
| Influenza hemorrhagic | May occur as a result of influenza. Its main symptoms are high fever, loss of consciousness, chills and epileptic seizures. |
| Herpetic meningoencephalitis | This type of disease can be independent (in adults) or occur against the background of a viral infection (in children), as well as serous or hemorrhagic. In some cases, the herpetic type of pathology occurs without pronounced symptoms. |
| Viral meningoencephalitis | Associated with the penetration of the tick-borne encephalitis virus into the body through contaminated animal milk. Usually the disease is diagnosed in the warm season. At the very beginning, the patient experiences chills, fever, headache, vomiting and sleep disturbances. After 10 days, neurological symptoms are added to them. One of its varieties is two-wave meningoencephalitis. |
| Granulomatous amoebic type of encephalitis | This pathology occurs infrequently and is considered very dangerous, as the mortality rate is high. The latent period of development of amoebic meningoencephalitis can last from 1 to 14 days. You can become infected with it while swimming in open water. |
| Brucellosis | Causes damage to the soft meninges and is characterized by the appearance of brucellosis granules. This form of meningoencephalitis is characterized by an extremely severe course. The patient's mental state is disturbed, paresis or paralysis occurs. Lumbar puncture and tomography help to identify pathology. |
| Purulent meningoencephalitis | Brain damage has a bacterial development associated with the penetration of staphylococci and meningococci. The disease can be primary or secondary. |
| Tuberculous | It is characterized by secondary damage to the meninges of an inflammatory nature. It is mainly diagnosed in patients with tuberculosis. Its main manifestations include: sleep and appetite disturbances, high fatigue and irritability, headaches, and depression. |
| Chickenpox | This form of the disease occurs in children and is associated with complications after chickenpox. It occurs against the background of a rash and lymphadenitis characteristic of the disease and occurs in a severe form. The following symptoms help make a diagnosis: headache and dizziness, fever, vomiting, adynamia, convulsions and apathy. |
| Listerose | Caused by aerobic or anaerobic microorganisms that can enter the body with food. |
| Toxoplasmosis | Associated with the penetration of bacteria into the fetus during intrauterine development. |
| Aseptic meningoencephalitis | Caused by some viruses. Usually the disease is mild, but sometimes it can pose a danger to the patient. |
| Fungal meningoencephalitis | Associated with the development of fungal infection. In patients with normal immunity, cryptococcosis may be the causative agent. In HIV-infected people, this is often aspergillus or candidiasis. |
| Necrotizing meningoencephalitis | It is characterized by a severe course and causes serious damage to the central nervous system. |
Diagnostics
Clinical diagnosis consists of assessing the patient’s mental status, consciousness, and focal neurological symptoms. The presence of hyperthermia and convulsions is determined, and functional tests are performed. When collecting anamnesis, attention is paid to recent events: previous viral diseases, swimming in ponds with dirty water, tick or animal bites, contacts with sick people, etc.
Instrumental and laboratory examination includes:
- spinal cord puncture with analysis of cerebrospinal fluid, i.e. cerebrospinal fluid (an admixture of blood, pleocytosis, and sometimes microbial agents may be detected);
- serodiagnosis (PCR, laboratory blood test, which allows you to determine the type of viral pathogen);
- laboratory analysis of nasopharyngeal swabs;
- laboratory blood test for the presence of specific antibodies (if the autoimmune nature of the disease is suspected);
- magnetic resonance imaging (allows you to assess the condition of the brain and membranes);
- computed tomography (for the purpose of differential diagnosis);
- electroencephalogram (assessment of the degree of brain damage and its functions);
- brain biopsy.
Purulent meningoencephalitis
Differential diagnosis is carried out with other diseases with similar symptoms, depending on the form. For example, amoebic meningoencephalitis can mimic a malignant tumor or abscess (purulent melting of an area) of the brain, some types of autoimmune inflammation are similar to manifestations of schizophrenia or drug intoxication, etc.
It is important that the disease is diagnosed accurately, with the identification of the etiological factor, since the timeliness and effectiveness of treatment depends on this.
Diagnosis of meningoencephalitis
To diagnose meningoencephalitis, the doctor will prescribe:
- Lumbar puncture. With meningoencephalitis, the cerebrospinal fluid becomes cloudy. It reveals high blood pressure, high protein levels and decreased glucose levels.
- PCR helps determine the presence of pathogenic bacteria.
- Computer or magnetic resonance imaging.
Carrying out a computed tomography
- Blood analysis.
- Nasopharyngeal swab.
- Chest X-ray.
Treatment
Suspicion of meningoencephalitis is a reason for hospitalization; treatment is carried out in a hospital setting. Measures are being taken to maintain vital functions and prevent infectious-toxic shock.
Etiotropic treatment depends on what causes meningoencephalitis. For diseases of infectious etiology, antibiotics or antiviral agents are used. Antiviral therapy should be started as early as possible if possible.
Symptomatic treatment is prescribed; specific medications depend on the manifestations of the disease. At high temperatures, antipyretics are used, for convulsions and seizures, anticonvulsants (anticonvulsants, antiepileptic drugs) can be prescribed, and for increased intracranial pressure, diuretics (diuretics).
At the recovery stage, brain stimulants, vitamin therapy, and physical therapy are prescribed.
Treatment and prevention
The nature of treatment depends on the type of meningitis (serous or purulent), the type of pathogen, and the severity of symptoms.
For viral meningitis, antibiotics are not prescribed, since they are powerless against viruses. Dehydration therapy with diuretics is carried out to reduce intracranial pressure. Anticonvulsants and antiallergic drugs are prescribed to reduce the body's sensitivity to allergens and toxins. Painkillers and antipyretics are also used. As a rule, recovery occurs within 1-2 weeks.
Bacterial meningitis is treated with antibiotics, to which various types of bacteria are sensitive. Since the analysis of cerebrospinal fluid taken during puncture takes 3-4 days, treatment is started with complex antibiotics, and after receiving the results of the analysis, the treatment is adjusted. If the patient’s condition does not improve 2 days after starting medication, a repeat puncture is performed to clarify the diagnosis.
The most effective measure to prevent infection with meningitis is vaccination, which is recommended if there is an outbreak of the disease in a child care facility or if a family member becomes ill. It is advisable to do it in cases where there is a genetic predisposition to meningitis or the child is at risk. The disadvantage of such vaccinations is that they only protect against diseases caused by Haemophilus influenzae (the most common type of pathogen). The vaccination is valid for 4 years. Some children have a hard time with it. However, doctors recommend vaccination, since complications from vaccination are not comparable to those of meningitis.
Possible complications and consequences
The consequences of meningoencephalitis can be short-term and long-term. Both the first and second include neurological deficits of varying severity, depending on how much brain tissue is damaged. These may be disturbances in hearing, vision, coordination, speech, gait, motor function disorders, paresis, paralysis, and personality changes. To minimize damage to the brain, a quick and accurate diagnosis, timely and correct medical care, and after recovery, in most cases, neurological rehabilitation, the scope of which is determined individually, are necessary.
Symptoms of meningoencephalitis
In most cases, the development of meningoencephalitis is associated with a complication of another infection.
Symptoms characteristic of the disease:
- High body temperature.
- Vomit.
- Headache.
- Cramps.
The disease is characterized by: headache, vomiting, weakness
- State of excitement.
- Photophobia.
- Impaired coordination of movements.
- Aphasic disorders.
Forecast
The prognosis is generally unfavorable, although it varies depending on the form of the disease and the state of the patient's immune system. Poor prognostic signs include the occurrence of cerebral edema, status epilepticus and thrombocytopenia. Good – normal encephalogram results.
Some species extremely rarely cause death, in most cases passing without a trace - these include meningoencephalitis in children caused by the chickenpox virus. However, this is the exception rather than the rule.
Meningoencephalitis often leads to severe damage to brain tissue and ends in death. If the patient is saved, he is often left with lifelong neurological deficits that result in disability.
Possible complications
Most often, serious complications occur with the viral form of the disease. If the pathology was detected late or the patient has disturbances in the functioning of the immune system, then he may experience paresis, paralysis or epileptic seizures.
Neurosurgeon Fayyad Akhmedovich Farhat will talk about the causes and symptoms of hydrocephalus:
With herpetic meningoencephalitis, postnecrotic cysts appear. Patients may develop hydrocephalus or mental retardation.
Most complications are associated with disturbances in brain function. His life will depend on how much a person’s central nervous system is affected by meningoencephalitis. An illness suffered in childhood often causes mental or mental retardation.
Causes
The development of the disease is caused by the penetration of infectious agents into the brain structures. If the disease appears as a result of a tick bite, they speak of the primary form of encephalitic meningitis.
The secondary type of pathology develops in people with weakened immunity. In addition, it is observed in persons who have suffered from certain infectious diseases, including rubella, mumps, measles, pneumonia, sinusitis or otitis media.
The development of encephalitic meningitis, the causes of which are a decrease in immune defense, is due to the lack of a proper barrier to prevent viral elements from entering the brain tissue or membranes, as well as the activation of severe inflammatory processes.
The development of encephalitic meningitis begins with the penetration of an infection into the brain through the bloodstream, affecting brain tissue and membranes.
The main route of infection is a tick bite. In most cases, infection with encephalitic meningitis occurs through the bites of infected ticks.
The duration of the incubation period of this disease in such cases ranges from two days to one month. Primary encephalitic meningitis is characterized by increasing symptoms.
In addition, you can become infected with the disease through the milk of animals: goats or cows (if it has not been subjected to heat treatment). With this method of infection, symptoms appear much faster: within 7-10 days.
Secondary encephalitic meningitis can develop in people with weakened immune systems and people who have had other infectious diseases:
- purulent sore throat;
- measles;
- mumps (mumps);
- flu;
- herpes infection;
- periodontal disease and oral caries;
- otitis;
- pneumonia;
- sinusitis.
The occurrence of the disease in such cases is associated with reduced immunity, which does not provide adequate protection against the penetration of the virus through the blood into the brain and the development of a severe inflammatory process. Due to decreased immunity, infection enters the cells of the membranes of the brain and its further spread occurs almost unhindered.
Only timely diagnosis and initiation of treatment can prevent the development of complications and negative consequences of encephalitic meningitis.
Classification
In modern medicine, meningoencephalitis is classified according to several different criteria.
From the point of view of the etiology of the disease, the following types are distinguished:
- Viral - its development is provoked by influenza , measles , herpes , enteroviruses, cytomegalovirus , etc. It is distinguished by the serous nature of the changes.
- Bacterial - it is provoked by pneumo-, strepto-, meningococci, Klebsiella , Haemophilus influenzae. This type is characterized by a purulent nature of the changes.
- Protozoal is a rare type of disease that is caused by toxoplasma, amoeba and other protozoa.
- Fungal - mainly develops in people with impaired immune system functions. Sometimes diagnosed in people with HIV/AIDS.
Taking into account the type of inflammatory process, the following classification of the disease is used:
- Purulent - during the development of the inflammatory process, pus is formed, which leads to clouding of the cerebrospinal fluid. There is a predominance of leukocytes .
- Serous - during the development of inflammation, a serous discharge is formed. The cerebrospinal fluid is transparent, lymphocytes .
- Hemorrhagic - this type is characterized by a violation of the permeability of the walls of cerebral vessels. As a result, petechial hemorrhages occur in the tissues.
Taking into account the peculiarities of the clinical process, the following classification is used:
- Lightning fast - develops very quickly, over several hours. In most cases, this form of the disease is fatal.
- Acute - in this case, the symptoms increase more slowly. Their development is observed over 1-2 days.
- Subacute – the process develops gradually, the deterioration of the patient’s condition takes a period from 1 day to 1 week.
- Chronic – inflammation can last a long time, from several months to several years. Exacerbations and remissions occur periodically. Acute and subacute types of the disease can gradually develop into a chronic form.
In turn, acute meningoencephalitis can be primary and secondary.
- Primary - this form develops directly in the brain due to exposure to various pathogens.
- Secondary - is a complication of another disease due to weakened immunity .
There are also several types of disease depending on the pathogen:
- Tuberculous - develops against the background of tuberculosis or as a result of contact with people suffering from an open form of tuberculosis. Treatment of this disease is carried out in a specialized hospital by phthisiatricians.
- Herpetic - the disease threatens with serious consequences. During development, pronounced cerebral and toxic symptoms, increasing cerebral edema, and neuronal death are observed. This type of disease can occur in newborns, since infection often occurs during childbirth, or even before birth - through the placenta. However, this form also affects adults.
- Purulent meningoencephalitis - this type of inflammatory process is caused by group B or D streptococci, Haemophilus influenzae or Escherichia coli, etc. Most often, this form of the disease affects people with immunodeficiency , as well as those who have recently suffered a head injury or surgery in this area. Pathogenic microorganisms that provoke the development of this form of the disease multiply more actively if there are foci of chronic infection in the body. As a rule, the course is acute, but a fulminant or chronic course is also possible.
- Influenza hemorrhagic - develops after influenza. In this case, the person’s body temperature quickly rises, clouding of consciousness is noted, and the patient may fall into a coma.
- Double-wave viral meningoencephalitis - the disease is carried by ixodid ticks, which infect animals, and people, in turn, become infected by consuming contaminated milk. It usually develops in spring and summer, when tick activity increases. It's going hard. The disease begins with headache, fever, and vomiting. After a few days, the patient’s condition improves, but after another ten days the second stage of the disease begins, when the work of the brain centers is disrupted.
- Toxoplasmosis - this form is provoked by protozoa. As the disease develops, internal organs and the nervous system are affected, and there is a lack of coordination and muscle pain.
- Vaccinal - appears 1-2 weeks after vaccination.
- Gummous - manifests itself in tertiary syphilis.
- Ornithosis is a serous-hemorrhagic form that develops with severe ornithosis.
- Mumps – provoked by the mumps virus.
- Rheumatic - develops against the background of rheumatism .
- Cytomegalic – affects newborns and infants with cytomegaly.
- Amoebic is a rare form. Infection can occur in freshwater bodies. It is caused by the single-celled organism Naegleria Fowler. Negleriosis occurs rapidly and affects the nervous system.
- Brucellosis - damage occurs to the soft tissues of the meninges, where brucellosis granulomas are formed. It is difficult to treat and causes paralysis and mental disorders.
Treatment methods
To treat encephalitic meningitis, drugs are used that are aimed at stopping the development and reproduction of pathogenic agents. These include:
- Antibacterial drugs. Among them, the most effective are Azithromycin, Cefuroxime, Ampicillin, Amoxicillin.
- Antifungal agents. Nystatin, Lavorin, Ketoconazole, Fluconazole are prescribed to treat the disease.
- Antiviral drugs. For this purpose, Interferon, Kipferon, Tsitovir, Amiksin are used.
In addition, doctors use drugs that can eliminate the symptoms of the disease. These are droppers with saline solution to relieve intoxication of the body, non-steroidal anti-inflammatory drugs, corticosteroids, drugs to reduce body temperature, as well as drugs that increase the body's immune defense.
Establishing diagnosis
The first and most basic method for diagnosing this disease is to analyze the cerebrospinal fluid in the laboratory. It is carried out using a puncture.
If a person is sick, the analysis will show that the cerebrospinal fluid is characterized by a cloudy consistency. This is due to cellular impurity. It will also show increased protein levels, decreased glucose concentrations and increased blood pressure.
Along with this, the following methods are used:
- polymerase chain reaction - to identify bacterial antigens;
- blood test and swabs from the oral and nasal cavities - to clarify the diagnosis;
- chest x-ray;
- CT and MRI - to exclude a purulent process in the brain.
Meningoencephalitis - what is it?
Diseases of brain structures, regardless of their location, are serious, dangerous and fraught with irreversible consequences. While the anatomy and histology of the brain are known in detail, the details of its functioning are still studied and researched to this day.
Brain structure
Brain structure
The brain is the controlling and governing organ of the human body. Coordinates the organs and systems of the body through the loci of the central nervous system on the cortex. It is located in the “cranial box”, performing it completely (95%) in the process of growing up. The Greek term for the brain is encephalon, and its Latin equivalent is cerebrum.
Morphologically and anatomically, the brain represents a variety of mutual positions and relationships of nerve cells (neurons) and their processes (dendrites and axons) and glial cells.
It is divided into the following sections: cerebral hemispheres, midbrain, pons, medulla oblongata, cerebellum. In each of them there are centers responsible for controlling various functions of the body.
The brain is connected to the rest of the structures of the skull and neck by 12 pairs of cranial nerves. The parenchyma (tissue) of the brain is separated from the bones of the skull by protective membranes:
- Soft – pia mater (vasculosa), the inner choroid containing microvessels and capillaries filled with blood, penetrating the brain tissue. Performs a trophic function.
- The arachnoid - arachnoid (archnoidea), an ultra-thin transparent formation, is a highly permeable membrane through which cerebrospinal fluid is transported. Has a regulating and shock-absorbing function.
- Hard – dura mater, tissue with the maximum concentration of nerve receptors, responsible for any type of brain sensitivity, in particular pain. There are no such receptors in brain tissue. Performs a protective function.
Based on structure and functional similarity, they are distinguished:
- Leptomeninx is a combination of soft and arachnoid membranes.
- Pachimeninx is a hard outer shell partially connected to the periosteum of the skull.
There are spaces (spatium) between the membranes, which represent a system for the circulation of cerebrospinal fluid (CSF):
- Subarachnoid - located between the soft and arachnoid.
- The subdural is the gap between the dura mater and the arachnoid membrane.
- The epidural is located between the bones and the dura mater.
Classification of meningoencephalitis
Ixodid tick is a carrier of meningoencephalitis
Inflammation of the membranes and brain tissue itself is called meningoencephalitis. The disease is characterized by possible death and frequent irreversible changes. Based on the time of occurrence, they are distinguished:
- Primary meningoencephalitis, discussed above, the cause of which is directly caused by the pathogen.
- Secondary meningoencephalitis develops as a consequence of acute or chronic diseases of an inflammatory or infectious nature: mumps, sinusitis, childhood infections (measles, rubella, chickenpox), tuberculosis, toxoplasmosis, malaria, streptococcal infection, herpes, influenza, syphilis, rabies, brucellosis.
- Degenerative demyelination in diseases of the central nervous system: multiple sclerosis, leukodystrophy, myelopathy.
- Post-vaccination syndrome.
Based on the type of inflammatory process and corresponding exudate, there are:
- serous;
- hemorrhagic;
- purulent.
One of the classifications of this disease is based on the etiological factor:
Viral meningoencephalitis
African mosquito
Viral meningoencephalitis develops when infected:
- RNA-containing neurotropic arbovirus of tick-borne encephalitis. The carrier of which is the ixodid tick, respectively, it is seasonal, characteristic of the late spring and early summer period. More common in children.
- The flavivirus that causes the disease is West Nile fever. Carried by special mosquitoes. The virus is tropic to brain tissue. In connection with the development of tourism, it occurs in adults after tours to Asian countries, and is often registered in the south of Russia and coastal regions.
Bacterial meningoencephalitis
Meningococcal infection
Bacterial meningoencephalitis is caused by the following microorganisms:
- Rickettsia prowazekii (Rickettsia Provachek) is an intracellular parasite that causes the disease rickettsiosis, the causative agent of epidemiological typhus. The carrier is the body louse.
- Neisseria meningitides (meningococcus), for which the nasopharynx is the entry gate and breeding site, then two more pathognomic symptoms are added: septicemia (the virus enters the blood) and meningitis.
- Listeria monocytogenes is a gram-positive bacillus that causes listeriosis. It enters the body through the alimentary route and from the intestines it penetrates into the blood and affects the body. Tropic to the spleen, liver and brain.
Amoebic meningoencephalitis
Amoebic meningoencephalitis is caused by mutated freshwater amoebae - naegleria fowleri. It is often diagnosed in children in the summer, as it gets into the nose when diving and moves along the olfactory nerve to the brain. It is characterized by lightning-fast development of the disease and a high percentage of deaths.
Symptoms of meningoencephalitis
The clinical picture of meningoencephalitis is the manifesting symptoms of meningitis:
- Intoxication syndrome is extremely pronounced - hyperthermia, delirium, hallucinations, convulsive syndrome in children.
- Tormenting, bursting, aggravated by turning or any movement of the head, unbearable migraine pain, often in the back of the head and forehead.
- “Hydrocephalic cries” are sharp, sudden cries in young children.
- The meningeal position of the “pointing dog” is a thrown back head, a retracted stomach and spastically bent all limbs, pressed as much as possible to the stomach.
- Dyspeptic symptoms - gushing vomiting and constant nausea, spastic constipation, complete loss of appetite, abdominal pain.
- Impaired consciousness - agitation or retardation.
- Lack of coordination – a staggering “drunk” gait, inability to stand up on your own.
- Analyzer dysfunctions – photophobia, hyperesthesia of the skin and mucous membranes, hyperaccusia.
- Epileptiform seizures are possible in both children and adults.
- Hydrocephalic syndrome is manifested by petechiae on the skin and mucous membranes, palpitations and shortness of breath, increased blood pressure.
- The clinical picture with the gradual development of the disease in infants manifests itself as ARVI or acute respiratory infections - redness of the posterior pharyngeal wall, polymorphic rash, enlarged tonsils, serous rhinitis, coughing, generalized lymphadenitis.
Consequences of meningoencephalitis
Abscessation
Treatment of meningoencephalitis must be carried out quickly and comprehensively, since the consequences of this disease are the following complications:
- Abscess formation is a purulent process in the brain and cerebellum.
- Generalized necrosis of the skin and subcutaneous tissue.
- Strabismus, uveitis and deafness of varying degrees of reversibility.
- Coma is more often observed in children.
- Meningococcal sepsis - meningococcemia.
- Bacterial shock.
- Death.
Diagnosis of the disease
Meningoencephalitis
Diagnosis of meningoencephalitis is carried out on the basis of:
- Pathological reflexes:
- Kerera - pain on palpation of the back of the head in the area where the occipital nerves exit.
- Brudzinsky - bending the legs in the “baby pose” with passive tilting of the head or pressing on the pubic symphysis.
- Kernig - a leg bent at the hip does not extend at the knee, due to spasm of the muscles of the back of the thigh.
- Ankylosing spondylitis - pain from tapping on the zygomatic arch and increased headache.
- Stiff neck.
- Pulatov's craniofacial reflex - tapping on the skull causes a characteristic grimace.
- Flatau - dilation of the pupils with sharp flexion of the neck.
- Mondonesi - pain in the eyeball when pressing on closed eyelids.
- Lessange - a symptom of “suspension” in infants is expressed in persistent long-term bending of the legs while hanging, while supporting the armpit and fixing the head with the fingers.
- Meningeal symptoms depend on the locus of the lesion - hemiparesis, anisoreflexia, alexia, apraxia, aphatia, mental disorders. In children, bulging and tension of the large fontanelle, which lasts for a long period.
- Symptoms of dysfunction of cranial nerve pairs are pain, motor and sensory dysfunctions.
- Swabs from the nasopharynx and throat for bacteriological and bacterioscopic methods.
- Viral meningoencephalitis is detected by virological and immunological methods.
- Amoebic meningoencephalitis is difficult to diagnose and is detected through specific blood tests.
- Study of the composition of cerebrospinal fluid - radionuclide cisternography. Biochemistry, macroscopy and microscopy are assessed: volume, pressure, outflow rate, color and transparency, the presence of cells (cytosis) and their percentage, bacteriological analysis.
- Diagnostic puncture and assessment of the patient's condition.
- X-rays, computed tomography or magnetic resonance imaging.
Treatment of meningoencephalitis
Treatment of meningoencephalitis often requires urgent care and resuscitation measures, especially in children.
Patients are subject to immediate hospitalization, emergency diagnostics and early initiation of therapeutic measures.
Drug treatment is prescribed according to the causative factor and the degree of brain damage: antiviral or antibacterial, symptomatic and detoxification therapy.
Rehabilitation after meningoencephalitis
Rehabilitation after a serious illness and elimination of local reversible consequences of meningoecephalitis is carried out comprehensively with long-term follow-up with a neurologist.
Drugs are used for a general restorative effect - multivitamins, antioxidants, venotonics. Correction of mental and mental balance is possible to improve sleep and return to work capacity.
It is necessary to use physiotherapeutic methods for recovery. Regular courses of sanatorium-resort treatment are desirable.
Source: https://headcure.ru/encefalit/chto-eto.html
Main symptoms
Meningitis encephalitis can cause a variety of symptoms. Much depends on the type of pathology, the cause of its occurrence, and the type of course. Once the infection enters the body, an incubation period begins. At this time, the human immune system tries to resist the pathogen, causing:
- attacks of headache;
- lethargy;
- increased sensitivity of the skin;
- loss of appetite;
- aching muscles and joints.
The duration of the incubation period depends on the strength of the immune system and the general condition of the body. It often ends after a few hours, giving way to an acute stage. Then the following symptoms are observed:
- increased body temperature;
- chills;
- runny nose;
- cough.
Penetration of infection into the brain can cause psychosis, hallucinations, sleep disturbances, and drowsiness. The onset of meningeal syndrome is accompanied by:
- hearing and vision impairment;
- photophobia;
- red rashes that disappear with pressure;
- hypertonicity of the occipital muscles;
- loss of movement coordination;
- nausea;
- cephalgia.
The most dangerous signs are bulbar disorders, in which speech and swallowing functions are impaired, and the functioning of the respiratory and cardiovascular organs is disrupted. Such defects are often fatal.
Meningitis, like encephalitis in newborns, is often viral in nature. In rare cases, intrauterine infection is possible, occurring against the background of an infectious disease of the mother that appeared in the first trimester of pregnancy. General symptoms do not differ from signs of the disease in adult patients (convulsive syndrome, shortness of breath, fever, vomiting, skin rash, involuntary twitching of the eyeball). Pathology can be accurately diagnosed by identifying early symptoms:
- grasping (with tonic extension of the toes with stroke stimulation of the sole);
- Brudzinsky (with spontaneous flexion of the lower limbs when the head is tilted);
- Kernig (with the inability to straighten the leg at the knee joint on a bent hip joint at an angle of 90 C);
- severe pain that occurs when pressing on the eyelids.
Meningoencephalitis (encephalitic meningitis): causes, symptoms, diagnosis and treatment
Encephalitic meningitis is a viral, fungal or bacterial disease manifested by inflammation of the membranes of the brain and spinal cord. It can be fatal if immediate diagnostic and therapeutic measures are not taken.
Story
There is an opinion that in the times of Hippocrates and Avicenna they knew about the existence of this disease. Could they cure her? More likely no than yes, because even in the modern world it is not always possible to identify a problem in time and respond to it.
The first documented case was recorded in Scotland in 1768, but at that time the connection with the pathogen was not clearly visible. They started talking about the epidemic at the beginning of the nineteenth century in Geneva, and although it was managed, it was not the last.
Throughout the last and century before last, encephalitic meningitis appeared in Africa, Europe and the USA.
Until the end of the twentieth century, the mortality rate from meningitis reached almost one hundred percent, but after penicillin was successfully used against the disease in 1944, the number of lives saved began to increase. Vaccines against common bacterial pathogens also helped, as did the invention of glucocorticoid drugs.
Causes
Based on etiology, this disease can be divided into three categories:
– infectious (provoked by a specific pathogen); – infectious-allergic (autoimmune damage to the membranes of the brain in response to infection, vaccination or rheumatic disease);
– toxic (exposure to irritating substances that provoke inflammation).
There are also primary and secondary encephalitic meningitis. As you might guess, a disease is called primary when the source of infection is located directly in the brain. This occurs with internal injuries (bruise, hematoma), viral or infectious diseases. A secondary disease appears as a complication, for example, of otitis media, sinusitis, tuberculosis or syphilis.
Epidemiology
Previously, due to overcrowding, non-compliance with sanitary and hygienic standards and poor nutrition, encephalitic meningitis occurred mainly in children under five years of age. But now such cases are rare thanks to the development of medicine and improved living conditions.
Most often they get sick in late winter - early spring. At this time, vitamin deficiency and decreased immunity are clearly manifested, as well as sudden changes in temperature and humidity. Constant stay in closed, poorly ventilated areas also contributes.
Encephalitic meningitis is widespread throughout the world, but it is most common in African countries. In Russia, the first outbreak of this disease occurred before the outbreak of World War II, the second in the eighties of the last century, and the last in 1997.
Pathogen
The most common are meningococcal and pneumococcal encephalitis meningitis. Streptococcus pneumoniae has more than eighty antigenic species. The organism itself is motionless, prefers aerobic space, but in critical situations it can temporarily do without oxygen.
The bacterium is oval in shape, less than a micrometer in diameter, it is immobile and does not have spores. It develops well on blood media at human body temperature. Pneumococcal encephalitis meningitis is transmitted by airborne droplets from a sick or recovering person.
The microorganism is quite resistant to the effects of drugs, including antibiotics.
Pathogenesis
The disease begins when the pathogen enters the upper respiratory tract and attaches itself to the mucous membrane of the nasopharynx or oropharynx. The virulence factors that pneumococcus has (capsule, teichoic acid, substance C) stimulate the production of prostaglandins and activate the complement system and neutrophilic leukocytes.
All this together does not cause encephalitic meningitis. The reasons for its appearance are deeper. Where the pathogen has colonized the mucous membrane, inflammation develops in the form of otitis, sinusitis, frontal sinusitis or tonsillitis.
Bacteria multiply, their toxins suppress the body's immune system, and through the bloodstream they spread throughout the body, affecting the heart, joints and, among other things, the lining of the brain.
Clinic
In the clinic, there are three forms that encephalitic meningitis takes:
– acute, accompanied by adrenal insufficiency and often ending in death; – prolonged, when symptoms increase gradually;
– recurrent, with small light intervals.
The acute form is characterized by a sudden onset against a background of complete well-being with a sharp increase in temperature to pyretic levels (39-40 degrees). There is pallor, sweating, cyanosis, possible loss of consciousness and convulsions, as well as paresis of the facial muscles. In infants and infants, anxiety manifests itself as a monotonous, incessant cry.
Increased intracranial pressure may cause divergence of the sutures of the skull, as well as bulging of the fontanel. On the second day of the disease, characteristic meningeal symptoms appear, such as stiffness of the neck muscles. After three to four days, the patient falls into a coma, and progressive swelling (due to the inflammatory reaction) leads to herniation of the medulla oblongata.
Meningeal symptoms
These are signs characteristic of inflammation of the meninges. They appear in the first hours after the onset of the disease and help to accurately diagnose.
- Pointer dog pose (head thrown back, limbs brought towards the body).
- Rigidity of the muscles of the neck and back of the head (the doctor is unable to passively bend the patient’s head due to increased tone of the extensor muscles).
- Kernig's sign (the doctor bends the patient's leg at the hip and knee joint, but when trying to straighten it, he encounters resistance).
- Upper Brudzinski symptom (when the head is bent, the legs are pulled towards the body).
- Medium Brudzinski's sign (bending of the legs when pressing in the suprapubic region).
- Lower Brudzinski's symptom (When one leg is passively flexed, the other is also brought toward the abdomen).
- Lessage's sign (the infant is lifted, supported by the armpits, while his legs are drawn closer to the body).
- Mondonesi's sign (painful pressure on the eyeballs).
- Bekhterev's symptom (pain when tapping on the zygomatic arch).
- Increased sensitivity to irritants, fear of light and sound.
In children
For an adult, it is difficult to endure a disease such as encephalitic meningitis. The consequences in children can be even more tragic, since they rarely complain of illness, do not notice insect bites and have reduced immunity. Boys get sick more often than girls, and the disease is more severe.
To protect your child, you need to dress him warmly in the spring and autumn, consult a doctor promptly at the slightest sign of illness, and examine him outside every couple of hours in the summer for tick bites and other blood-sucking insects.
Diagnostics
It is first of all important for the doctor to confirm the diagnosis of “encephalitic meningitis”. Is he contagious? Undoubtedly.
Therefore, the patient must be placed in a separate box or in the infectious diseases department, having previously conducted an epidemiological survey. Then you need to collect an anamnesis of life and health, find out complaints.
Physical examination consists of checking meningeal signs and taking temperature. For laboratory tests, blood and cerebrospinal fluid are taken.
A general blood test shows an increase in the level of leukocytes with a predominance of young forms, the absence of eosinophils and a sharply increased ESR to sixty millimeters per hour.
The liquor will be cloudy, opalescent, with a greenish tint. It is dominated by neutrophils and protein, and the amount of glucose is reduced.
To determine the pathogen, blood, sputum or cerebrospinal fluid are inoculated onto a nutrient medium.
Treatment
If an emergency room doctor or emergency room suspects encephalitic meningitis, the patient is immediately hospitalized in a neurological hospital. Treatment begins immediately, without waiting for laboratory confirmation of the diagnosis. Strict bed rest and a high-calorie diet are observed.
They begin with symptomatic and pathogenetic therapy. First of all, you need to cleanse the body of toxins produced by bacteria, as well as reduce intracranial pressure and thin the blood.
To do this, the patient is given intravenous saline with glucose and diuretics. Because excessive flooding of the body can lead to herniation of the medulla oblongata and instant death.
In addition, drugs to improve microcirculation, vasodilators and nootropics support brain activity.
Etiological therapy consists of antibiotic therapy (benzylpenicillins, fluoroquinolones, cephalosporins).
Exodus
It all depends largely on how quickly and successfully the encephalitic meningitis was treated. The consequences may be minor if help is provided in a timely manner. And at the same time, with a severe and rapid course of the disease, the mortality rate reaches eighty percent. There may be several reasons for this:
– cerebral edema and herniation; – cardiopulmonary failure; – sepsis;
– DIC syndrome.
Prevention
Encephalitic meningitis can be prevented; for this purpose, children from two to five years of age are vaccinated among those who are at risk. It is also recommended for people over sixty-five years of age. This vaccine is included in the official WHO vaccination schedule and is used in most countries of the world.
At the moment, in third world countries the public is still afraid of the diagnosis of “encephalitic meningitis”. Can he be cured? Yes, definitely. But success depends on how quickly help was provided and how.
Source: https://FB.ru/article/258508/meningoentsefalit-meningit-entsefalitnyiy-prichinyi-simptomyi-diagnostika-i-lechenie
How does the pathogen get into the GM?
The most expressive (and the leader in frequency) is the route of infection, which is associated specifically with ixodid ticks. When they bite a person, they introduce a neurotropic virus into his blood. By the way, a tick is also dangerous because it can introduce several pathogens together with its bite - this is called a mixed infection. And the danger here is that it is often simply impossible to identify them in a short time using a laboratory method. Clarification of the diagnosis is delayed, which affects the effectiveness of treatment.
Tick-borne meningoencephalitis can only be prevented by healthy prevention. This does not mean that you need to sit at home and completely refuse forays into the forested area. But you need to carefully consider your appearance - wear something that will not allow the tick to bite you, be sure to wear hats. Finally, you can use special tick repellents; there are plenty of them in pharmacies today.
Other ways the pathogen itself enters the body:
- Meningococcal infection is especially insidious - it is transmitted by airborne droplets, which is why it is more often found in children with reduced immunity.
- Meningoencephalitis of newborns is usually associated with intrauterine infection. That is, this disease is not acquired at birth, it began during gestation. But the very fact of a child passing through the birth canal increases the risk of morbidity if the mother is infected.
- Amoebas enter the human nervous system when the latter bathes in unsuitable places. The nose and throat are the widest entrance gates for pathogens. How to protect yourself? Firstly, consider whether the health station allows swimming in a particular place. Secondly, from an early age, teach children not to swallow water from a lake/river, try not to plunge their heads into the water, and take a shower after swimming.
As for the specific routes of penetration, we can say that in the first place is the hematogenous route (through the blood), in the second place is the lymphogenous route.
But the direct penetration of pathogenic flora cannot be ruled out if we are talking about breakthrough processes in purulent cavities or open head injuries.
Meningoencephalitis
Encephalitis is an inflammation of the brain. Meningitis is an inflammation of the lining of the brain. If these two processes are observed simultaneously, they speak of meningoencephalitis.
Causes of meningoencephalitis
Encephalitis is a polyetiological disease that can be infectious, infectious-allergic, or toxic.
Meningoencephalitis is a serious disease of the brain and meninges. May be a complication of encephalitis and meningitis.
In any case, such a complication is a serious pathology, aggravates the course of the disease, has an unfavorable prognosis with possible death , and residual neurological deficit.
The severity of residual effects depends on the degree of damage to the central nervous system.
Causes
The main cause of this disease is infection. Neurotropic pathogens penetrate the cerebral structures, or the infectious process spreads from nearby foci or as a result of common infectious diseases.
Infection is possible due to the following phenomena:
- When the pathogen enters the nasopharynx. A person becomes infected through airborne droplets and nutritional methods. The infection enters the cranial cavity through the hematogenous route.
- When a person is bitten by an insect. Infection occurs through transmission. The insect carries a pathogen that, during a bite, enters the blood and with it into the cerebral tissue.
- When infectious processes develop in the body. If a person is sick with syphilis , tuberculosis , or develops purulent processes (otitis, sinusitis , etc.), hematogenous spread of a bacterial infection can occur. Sometimes meningoencephalitis in children and adults develops after suffering from acute respiratory viral infection . The disease can become a complication of encephalitis, meningitis, chickenpox , rubella, measles.
- After a traumatic brain injury has occurred. If the injury in children or adults is open, there is a possibility of infection through contact. Statistics show that post-traumatic meningoencephalitis is diagnosed in approximately 1-3.5% of people with TBI.
- After vaccination has been carried out. If the immune system is weakened and a live vaccine was administered, an infectious process may develop. Pathogens penetrate the blood-brain barrier.
However, it is important to understand that this terrible disease does not always develop after infectious agents enter the body. The following factors contribute to its manifestation:
- weakened body;
- immature immune system;
- immunodeficiency;
- autoimmune reactions;
- massive infection.
Meningoencephalitis diagnosed in newborns
The cause of the disease that develops in newborns is, as a rule, a viral attack or intrauterine damage. For example, if the expectant mother suffered an acute infectious disease in the early stages of pregnancy, the fetus may develop inflammation of the brain (as one of the consequences).
The child does not always survive until the moment of birth; in principle, he is not always born alive if the infection was serious. For example, if a mother has suffered from rubella, the consequences are almost always irreversible.
Meningoencephalitis in infants is accompanied by the following symptoms:
- Hyperthermia;
- General serious condition;
- Refusal to feed;
- Vomit;
- Diarrhea;
- Involuntary eye twitching;
- Strabismus;
- Cyanosis of the skin;
- Cardiopalmus.
During diagnostic measures, the eloquent Kerning symptoms and muscle rigidity are difficult to diagnose. A positive Pandey reaction is detected in the cerebrospinal fluid by a laboratory method. Moderate lymphocytic pleocytosis, peripheral blood tests may not reveal pathologies, ESR is accelerated, but weakly.
Drug treatment includes broad-spectrum antibiotics, the use of gamma globulin, and high doses of vitamin formulations. If a child has prolonged vomiting, then dextrose and so-called saline solution are administered intravenously.
The prognosis for such patients is assessed as doubtful; every third baby, unfortunately, dies. Most surviving children show signs of brain damage.
Encephalitic meningitis - description
Encephalitic meningitis is an infectious disease characterized by the formation of pathogenic changes in the cellular structures of the brain along with the membranes. This pathology is dangerous due to the development of severe complications that can lead to disability or death of the patient. If there is a suspicion of an encephalitic form of meningitis, the patient is urgently hospitalized in a medical facility for further detection of the cause of the pathogenic processes and treatment.
Unlike encephalitic meningitis, the pathogenesis of which is accompanied by the development of pathogenic processes in the membranes and tissues of the brain, encephalitis is characterized by damage only to brain structures. Different forms of meningitis and encephalitis can occur in one patient at the same time. In this case, the diagnosis will be established as meningoencephalitis.
Rehabilitation after meningitis: recovery of the body and possible complications
Rehabilitation after meningitis: recovery of the body and possible complications
Meningitis is an inflammatory disease affecting the brain and spinal cord.
The causative agents of the disease can be microorganisms of a viral, bacterial or fungal environment.
Depending on the severity of the disease, prevalence, nature and speed of progression, it is divided into separate types.
The disease develops rapidly. Rehabilitation after meningitis is an important part of the treatment process.
Description of the disease
An infectious-inflammatory disease develops against the background of the penetration of pathogenic organisms into the human body.
The disease can be independent or develop as a complication after severe pathology.
The course of the disease is always rapid and requires emergency care. It is important to contact specialists who will tell you how to recover from meningitis.
The causative agents are bacteria - meningococci, viruses - enterovirus, protozoa (in the case of malaria or toxoplasmosis), fungi.
Meningitis of fungal origin is rare, only in cases of low immunity.
Treatment must be comprehensive, rehabilitation after meningitis is mandatory.
The bacterial type of disease spreads:
- during childbirth (from mother to baby);
- through microparticles in the air - from a carrier of the pathogen through sneezing or coughing;
- through close contact;
- through food or drinks;
- through general hygiene items.
Various types of bacteria can cause bacterial meningitis.
Development of serous meningitis
An infected person may not get sick himself, however, he will pose a threat to others as a source of the disease. The viral type of disease is more common.
It is distributed:
There are many viruses that can cause meningitis. This type of illness is more mild. The best prevention of viral meningitis is frequent hand washing - after using the toilet, performing hygiene procedures with a child, before preparing food. Treatment and recovery after meningitis in adults includes a mandatory course of rehabilitation.
Classification of meningitis
In accordance with the nature of inflammation, serous meningitis is distinguished.
In this case, many lymphocytes are formed in the cerebrospinal fluid. In the case of a purulent type of disease, many neutrophils are present in the cerebrospinal fluid, and purulent fluid is released.
Based on localization, generalized and organic (affecting the hemispheres or base of the brain) types of the disease are distinguished. Depending on the speed of the pathology, it is divided into fulminant, acute, subacute and chronic.
Diagnosis of meningitis by a doctor
The chronic type in most cases is a consequence of an infection in the body that has moved to the brain area. In terms of severity, meningitis can be mild, severe, moderate, or extremely severe.
Treatment and rehabilitation after meningitis in adults include a number of drugs and measures aimed at restoring the normal functioning of the brain and tissues of the nervous system.
Symptoms of the disease
Meningitis has the following manifestations:
- intoxication – chills, fever, myalgia, malaise, weakness, skin rash, arthralgia;
- irritation of the membranes of the brain - severe headache, photophobia, severe tension in the neck muscles;
- general symptoms – vomiting and nausea, convulsions, loss of consciousness and coma, hallucinations, delirium;
- damage to the nerves of the head - impaired hearing and vision;
- The characteristic position of the body in a serious condition is that the patient lies on his side, his legs are pulled up to his chest, his head is laid back.
In childhood or in older people, symptoms may be mild or absent altogether.
Meningitis is characterized by a rapid onset of high fever, headache and vomiting. Unlike ordinary poisoning, vomiting does not bring relief.
After this, the main symptom of the disease appears - stiffness of the neck muscles. The patient is unable to lower his chin to his chest.
Fever and severe headache are some of the symptoms of meningitis
Dizziness, drowsiness, and photophobia occur. Sometimes convulsions occur and the patient may lose consciousness. The meningococcal form of the disease is characterized by the appearance of skin rashes.
With other types of disease, this sign may not be present. Viral meningitis most often affects children under 18 years of age. Tuberculous meningitis is the most common chronic type of the disease.
Rehabilitation after meningitis
Recovery from meningitis in adults is complex, complex and multifaceted.
After treatment, the patient must visit a neurologist for two years.
The doctor selects an individual rehabilitation program for viral meningitis, which includes several components.
Diet
Nutrition after meningitis should restore strength and not disrupt the functioning of the digestive organs.
Food is steamed, boiled, baked or stewed. Lean meat is suitable - veal, rabbit, chicken. For children, lean fish or meat is pre-chopped.
Lean meat is indicated after meningitis.
Porridge is suitable for dietary nutrition. Fruits and vegetables are subjected to heat treatment, since fiber can be irritating to the mucous membrane of the digestive organs.
The diet should include baked or stewed vegetables, soups, fruit purees, and dairy products. Drinks include jelly, compotes, and tea.
Physiotherapy
Rehabilitation after meningitis at this stage includes massage and hardware procedures.
Electrophoresis using drugs or vitamins stimulates certain muscles and helps relax them in the right places.
Electrophoresis to restore the body after meningitis
Magnetotherapy, electrosleep and magnetic laser therapy are used for cognitive and coordination types of complications. These procedures are aimed at restoring the functions of the central nervous system.
Physiotherapy
This type of rehabilitation procedures includes various exercises that the doctor selects for each patient individually.
The main task of exercise therapy is the restoration of motor functions. Exercises consistently train individual areas, moving from one link to another.
In modern rehabilitation centers, in addition to gymnastics, special exercise equipment, clothing and other methods of influencing the patient’s body are used.
Meningitis leaves consequences in the form of a changed lifestyle. In this regard, the patient needs adaptation that will help fully or partially restore his lost capabilities.
Conclusion
Meningitis is a dangerous, serious disease that threatens human health and life.
Only early treatment can be most effective.
Self-medication in the case of such an illness is unacceptable. The basis for success is the selection of adequate restoration measures.
A positive treatment result directly depends on timely rehabilitation.
: Meningitis: how to protect yourself from it
Source: https://noalone.ru/infocentr/psikhologiya/reabilitaciya-posle-meningita/