The phrase “heart failure” is heard by many. However, it is often used not entirely correctly, meaning most heart pathologies. Understanding the causes and mechanism of heart failure helps to identify problems in a timely manner and increase the patient’s life expectancy.
CHF 2nd degree FC 2
Decoding the concept
Heart failure (HF) is a collection of symptoms that may include:
- shortness of breath;
- orthopnea;
- weakness;
- increased fatigue;
- heartbeat;
- night cough;
- the appearance of edema;
- swelling of the neck veins.
Thus, it is not an independent disease. Doctors understand heart failure as a set of symptoms that are associated with inadequate perfusion of organs and tissues at rest or during exercise and often with fluid retention in the body.
Important: effective treatment of HF symptoms is only possible if the underlying disease is eliminated.
What is chronic heart failure
What causes heart failure
In the mechanism of occurrence of the above symptoms, the following sequence can be distinguished:
- Some diseases lead to damage and weakening of the myocardium, the main muscle of the heart.
- Myocardial pathologies cause the organ to be unable to fully meet the body's blood supply needs.
- Poor blood supply leads to insufficient nutrition of internal organs and tissues.
- Blood stagnation occurs in the body, which provokes pathological processes at the site of their formation.
Causes leading to chronic heart failure
The main and less common reasons are shown in the table:
| Main reasons | Less common causes |
| Cardiac ischemia | Previous myocarditis |
| Previous myocardial infarction or acute coronary syndrome | Cardiomyopathies |
| Diabetes | Toxic myocardial damage of various etiologies, including iatrogenic nature (chemotherapy, radiation damage to the myocardium, etc.) |
| Arterial hypertension | Anemia |
| Heart defects | |
| COPD | |
| Chronic and paroxysmal atrial fibrillation | |
| Acute cerebrovascular accident |
With any variant of the disorder, acidosis, hypoxia of tissues and internal organs, and metabolic disorders appear.
Other causes of CHF
Risk factors for angina pectoris
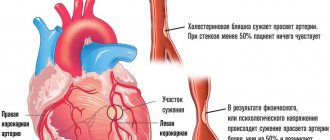
The occurrence of chest pain, even in isolated cases, is an alarming symptom indicating a problem in the body. There can be several risk factors for heart problems at the same time. Most often their appearance is influenced by:
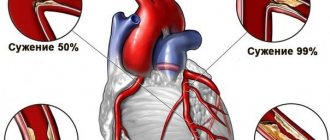
- atherosclerosis of the coronary arteries;
- high blood cholesterol levels;
- arterial hypertension;
- sedentary lifestyle;
- smoking;
- obesity;
- increased level of blood clotting;
- diabetes;
- thrombosis;
- thrombophlebitis;
- phlebothrombosis.
Doctors note, and this is confirmed by numerous observations and studies, that stress has a significant impact on the development of angina. And it doesn’t matter at all whether it’s an emotional outburst or a chronic stressful situation. In both cases, chest pain may appear, indicating serious problems, one of which may be exertional angina FC 2 (we will look at what this is in this article).
Features of the course of heart failure
Over the years, symptoms progress, signaling the emergence of new problems in the body. The lack of adequate treatment leads to deterioration of the patient's health and aggravation of pathological processes. Heart failure can occur acutely or as a chronic process. The acute form is a consequence of problems with myocardial contraction, which are accompanied by a decrease in minute and systolic blood volume. The acute form can occur due to the ingestion of toxins, the presence of cardiac diseases, or injuries. It manifests itself in critical conditions: cardiogenic shock, cardiac asthma, acute kidney failure, pulmonary edema. Left untreated can lead to death.
Pathogenesis of CHF
The chronic form develops over a long period of time and is explained by the presence of an underlying cause that caused myocardial pathology. Symptoms appear gradually, intensifying over time. The severity of the process and the number of symptoms determine the stage of chronic heart failure.
Important: treatment of the chronic form is usually long-term and complex. Often patients have to completely change their lifestyle.
Classification
Classification of CHF according to Strazhesko
There are two classifications that give a clear understanding of how advanced the pathological process is and how serious the patient’s condition is. In general, they are very similar and are often equivalent. However, the first evaluates the stage of heart failure from the point of view of the doctor and visible symptoms, while the second takes into account complaints and functional limitations in the patient’s life. For clarity, they are presented in table form:
| Classification of the All-Union Congress of Therapists (by stages) | New York Heart Association classification (by functional classes) | Symptoms |
| Clinical manifestations and morphological changes are assessed | Functional states are assessed | |
| 1 | I FC | Patient: does not experience discomfort during any physical activity. During exercise, nausea, shortness of breath, tachycardia, and heart pain do not appear. The stage is asymptomatic, there are no complaints. Doctor: there are no hemodynamic changes. During physical activity, studies may reveal a reduced ejection fraction or slight enlargements of the walls of the ventricles of the heart |
| 2a | II FC | The patient: at rest he feels absolutely normal. However, moderate activity loads cause nausea, palpitations, and unusual shortness of breath. The patient tries to control or eliminate such physical activity. Doctor: hemodynamic disorders affect one circle of blood circulation. Cyanosis can be visually detected. A dry pulmonary cough appears and congestive wheezing is heard in the lungs. |
| 2b | III FC | Patient: good health only in a calm state. Difficulties and deterioration of the condition are caused by the slightest physical exercise, which is accompanied by anginal aching pain, loss of strength, lack of air, and palpitations. The patient notices less frequent and less abundant urination. Doctor: cyanosis and swelling of the extremities are very noticeable, wheezing in the lungs and heart murmurs are heard, palpation reveals a pathological enlargement of the liver, ascites. The patient becomes incapacitated |
| 3 | IV FC | Patient: shortness of breath at rest, any exertion causes severe discomfort. The patient tries to avoid any unnecessary activity. Doctor: notes pronounced changes in hemodynamics and severe (irreversible) structural changes in target organs (heart, lungs, blood vessels, brain, kidneys). |
To describe the patient’s condition as accurately as possible, doctors combine both models, indicating both the stage and functional class.
Functional classification of CHF
Next, chronic heart failure will be considered using the example of stage 2 of functional class II.
Classification and degrees of CHF
When classifying pathology, the indicators of the organ’s ability to accept venous blood and transmit arterial blood, saturated with oxygen cells, into the circulatory system are taken into account. There are three types of heart failure (HF):
- HF with preserved left ventricular (LV) ejection fraction (HFpEF) ≥50%. Patients with normal EF typically do not have LV dilatation, but instead often have LV wall thickening and/or left atrial (LA) dilatation as a sign of increased filling pressure.
- HF with reduced LV systolic function <40% (HFrEF). Myocardial damage, in which the muscle cannot cope with the pumping function (is not able to push out a certain volume of blood).
- HF with average LVEF 40-49% (HFmEF). The ejection fraction is not within normal limits, but there is no significant decrease in it.
In 1965, the New York Heart Association (NYHA) developed a classification of heart failure consisting of four groups (functional classes). Russian doctors have a domestic method for dividing CHF into types (Strazhesko/Vasilenko), consisting of three pathology groups.
Clinical portrait of a patient with congestive heart failure
Unlike their American colleagues, Russian doctors take into account (in addition to the symptoms of the disease) the degree of scarification (impairment) of hemodynamics, metabolism, individual sensitivity to the therapy and other diagnostic indicators. Russian cardiologists take into account the NYHA classification, therefore, when diagnosing, they indicate the indicators of both methods:
| Classification of CHF by functional classes and stages | NYHA (FC) | Strazhesko/Vasilenko (stages) |
| 1/1FC | There are no restrictions on physical activity. Normal physical activity does not cause shortness of breath, fatigue, or palpitations. | Initial, or latent failure, which manifests itself in the form of shortness of breath and palpitations only with significant physical activity that has not previously caused it. At rest, hemodynamics and organ functions are not impaired, work capacity is slightly reduced. |
| 2A /2FC | Light limitation of physical activity. Feeling comfortable at rest, but ordinary physical activity causes shortness of breath, fatigue, and palpitations. | Signs of circulatory failure at rest are moderate, exercise tolerance is reduced. There are hemodynamic disturbances in the systemic or pulmonary circulation, their severity is moderate. |
| 2B/3FC | Significant limitation of physical activity. Feeling comfortable at rest, but light exertion causes shortness of breath, fatigue, and palpitations. | Severe signs of heart failure at rest, severe hemodynamic disturbances in both the systemic and pulmonary circulation. |
| 3/4FC | Inability to perform any physical activity without feeling discomfort. Symptoms may also be present at rest. With any load, the discomfort increases. | Final: diastolic stage with pronounced hemodynamic disturbances, metabolic disorders and reversible changes in the structure of organs and tissues. |
Chronic heart failure
The peculiarity of chronic heart failure is its hidden manifestations. The pathology develops slowly, without clear manifestations of symptoms. There is a high risk of not detecting heart failure in time. Doctors often note cases where older people with the first stage of pathology literally go to the terminal level within a couple of years after the diagnosis is made, when therapy in the vast majority of cases is already powerless.
Important. Without proper competent treatment of CHF, the disease provokes the appearance of pulmonary edema, attacks of suffocation and the development of cardiogenic shock (a rapid decrease in myocardial function). There is a high risk of death.
Heart with myocardial damage
If in the initial stage of CHF (stage 1) the symptoms are difficult to determine, then, starting from the second stage of the disease, the patient is already able to understand that disturbances are occurring in the body. If alarming symptoms appear, especially if they worsen, you should immediately visit a doctor.
Symptoms
Based on the circulation in which problems appear, the symptoms of the second stage may differ slightly. Symptoms that appear with pathologies of the small circle of blood flow:
- increased fatigue, irritability;
- increased heart rate after physical activity;
- orthopnea;
- nocturnal attacks of suffocation;
- dyspnea;
- orthopnea;
- weakness;
- heartbeat;
- night cough;
- the appearance of edema;
- swelling of the neck veins;
- cyanosis.
Symptoms of chronic left ventricular failure
Symptoms that appear in pathologies of the pulmonary circulation:
- shortness of breath after exercise or a heavy meal;
- pallor of the skin, acrocyanosis, cyanosis of the mucous membranes;
- loss of appetite;
- wheezing in the lungs (symmetrical from the lower parts to the entire surface of the lungs);
- weakening of the first sound at the apex of the heart, the presence of a gallop rhythm, the presence of murmurs of relative insufficiency of the atrioventricular valves.
At stage 2a, disturbances are noticeable in only one of the blood circulation circles. At the last stage of the second stage, which is classified as stage 2b, problems affect both blood circulation. Symptoms become serious and significantly worsen the patient’s quality of life. According to the foreign classification, degree 2b corresponds not to the second, but to the third functional class due to the severity of the disease.
Symptoms of chronic right ventricular failure
The second stage is decisive for the outcome of the disease. During this period, the symptoms are already quite clearly visible and should alert the patient. Timely contact with a doctor at the second stage allows you to begin proper treatment, which is likely to lead to full compensation. If treatment is not started, then the symptoms will begin to worsen and go into the third stage, the treatment of which is impossible for modern medicine.
Important: the patient must be mentally prepared for treatment and want to get better. This will help you strictly follow your doctor’s recommendations and not skip taking medications. A frivolous approach to treatment makes it practically useless.
Symptoms of second class CHF
When the chambers of the heart organ are stretched and weakened, the heart is unable to fully contract and send blood through the bloodstream. As a result, it accumulates in a large hemodynamic circle. When the accumulated blood encounters the natural flow of the circulation, it “overflows,” returning to the pulmonary vessels. If a similar situation occurs with a small hemodynamic circle, swelling and shortness of breath develop. Less and less blood enters and exits the heart organ, causing the heart to beat faster. The main distinguishing signs of CHF are shortness of breath, rapid heartbeat (tachycardia) and swelling.
Causes of CHF
Dyspnea
One of the first and most common symptoms of CHF. At the first stage of heart failure, attacks of shortness of breath are hardly noticeable, they practically do not happen, and breathing becomes more frequent only with strong physical exertion. As the pathology develops, shortness of breath occurs to the patient even in a state of complete rest. Many patients are even forced to sleep in a semi-sitting position - cardiac asthma manifests itself especially strongly at night, when it is harder for the heart to cope with stress. A paroxysmal hacking cough develops.
Important. Dyspnea is a specific indicator for diagnosing CHF by type. Dyspnea indicates the patient's functional potential and serves as the basis for disease classification.
Shortness of breath occurs due to problems with blood flow through the vascular system of the pulmonary organs (venous stagnation develops in the vessels). This leads to the development of a dry, hacking cough and swelling of the lungs. In severe situations, cough syndrome and shortness of breath combine into a severe attack of suffocation, which indicates the transition of CHF to the acute stage.
Complaints of patients with CHF
Tachycardia
In the initial stages of development of CHF, an increase in heart rate develops only with severe overexertion. With the development of pathology, tachycardia manifests itself constantly and increases even with minor physical effort.
Important. CHF is characterized by a “gallop rhythm,” that is, when listening to the heart rhythm, the heartbeat is clear and fast.
When resting at night, heart rate increases from 120 beats/minute. Such a heart rhythm does not allow the patient to sleep and rest normally. With stage 2 CHF, the pulse returns to normal 10-12 minutes after physical activity. As the disease progresses, the time frame increases.
Swelling
Distribution of patients by stages of CHF and FC
One of the most striking and noticeable signs of CHF is the appearance of peripheral edema. The appearance of edema may indicate the degree of development of the pathology:
- Beginning of the disease. There is no swelling.
- CHF from stage 2 B. Swelling covers the area of the lower leg and thighs, spreading to other parts of the body. In bedridden patients, swelling is concentrated in the sacral area. By the evening there is a strong dynamics of the symptom, in the morning the manifestation of the pathology remains.
- Last stage CHF. Severe swelling in the lower back and hips. Possible development of ascites (abdominal dropsy).
Video - Heart failure
Other signs
In addition to tachycardia, swelling and shortness of breath, a number of other signs are observed in patients with CHF. The possibility of their manifestation depends on the condition of the patient’s body. The following symptoms may occur:
- swelling of the jugular veins;
- hair loss (alopecia);
- deformation of the nail plates;
- blueness of the tip of the nose, lips and fingers;
- dull aching pain in the area of the right hypochondrium;
- hydrothorax (chest dropsy: accumulation of fluid in the pleural cavities);
- skin problems (pigmentation, trophic changes, ulcers, non-healing wounds);
- disruption of the liver (enlargement of the organ, its compaction, yellowness of the epidermal and mucous tissues).
Another main sign of early stage CHF is pronounced muscle weakness and high fatigue. This symptom develops due to insufficient blood supply to the muscles.
Treatment
Heart failure is difficult to completely cure. In most cases, doctors manage to improve the patient’s condition and return to the first stage. It is much easier to prevent the occurrence of heart failure, so it is very important to take specific preventive measures, take care of heart health and treat other diseases in a timely manner.
Treatment of CHF
At the second stage of FC II, drug therapy is prescribed:
- diuretics (diuretics);
- ACEI;
- statins;
- beta blockers;
- cardiac glycosides;
- omega-3 PUFAs;
- APA;
- anticoagulants and antiplatelet agents;
- antiarrhythmics, etc.
Important: only a doctor can select the correct group, generation and brand of the drug. If you have heart problems, taking medications that someone else recommended could cost you your life!
In addition to drug therapy, much attention is paid to:
- Physical activity regimen. The doctor adjusts the dose and frequency of exercise.
- Diet. The diet includes heart-healthy ingredients and eliminates all junk food and drinks. For stage 2 CHF, recommendations for salt intake are no more than 1.5 g per day.
- Quitting smoking.
- The psychological state of the patient. This will allow you to be more conscious about your treatment and reduce the level of daily stress that has a negative impact on your heart health.
Drug treatment of CHF
An important point at all stages, especially the second, is the treatment regimen. This concept includes medical recommendations and patient adherence to treatment. Doctors teach the patient and his family to monitor the course of heart failure, identify severe conditions and provide first aid. The patient receives complete information about the disease. The treatment becomes clearer to him, and the symptoms become less frightening. Doctors create a recommended daily routine for the patient, which includes hours of activity, physical activity, daytime and nighttime sleep.
Video - Chronic heart failure: epidemiology, diagnosis, treatment
Treatment of the disease
Therapeutic measures for CHF are aimed at removing excess fluid from the body, normalizing myocardial function and stabilizing blood pressure. Treatment with medications is carried out simultaneously with a diet that limits fluid and salt intake and moderate physical activity.
Treatment of heart failure
When treating CHF, the following medications are prescribed: ACE inhibitors . The medicinal group of these drugs significantly reduces the risk of unexpected death from respiratory arrest, slows down the manifestations of CSH and alleviates unpleasant symptoms. The therapeutic result appears after 2-3 days. ACE inhibitors include: Benazepril, Captopril, Zofenopril, Cilazapril, Enalapril, Lisinopril, Perindopril, Quinapril, Ramipril, Spirapril, Trandolapril and Fosinopril. Cardiac glycosides . Medicines in this group are aimed at improving myocardial function, stabilizing hemodynamics and reducing the load on the heart muscle. Glycosides slow down the pulse and restore kidney function, having a moderate diuretic effect. This group of drugs includes: Digoxin, Novodigal, Lanatozid, Dilacor, Korglykon, Cordigit, Tsedigalan, Strophanthin, Digitoxin. Antiarrhythmic drugs . Medicines in this category lower pulse and blood pressure, preventing the occurrence of arrhythmia. They also significantly reduce the likelihood of cardiac (sudden) death in people with CHF.
Drugs for the treatment of CHF
Antiarrhythmic drugs include Amiodarone, Quinidine, Lidocaine, Disopyramide, Mexiletine, Flecainide, Etatsizin, Esmolol, Ivabradine, Adenosine, Panangin, Atenolol, Procainamide. Diuretics. Medicines that reduce the load on the myocardium and relieve swelling. These are Triamterene, Lasix, Diuver, Veroshpiron and Diakarb. Anticoagulants . Medicines that prevent blood clots and thin the blood. This group of drugs includes: Warfarin, Heparin, Nadroparin, Reviparin, Tinzaparin, Parnaparin, Enoxaparin, Acenocoumarol, Deltaparin, Neodicoumarin. In case of stage 1 CHF, in addition to drug treatment, the patient is prescribed sanatorium-resort therapy, regular walks and vitamin therapy. Success in the treatment of CHF largely depends on the participation of the patient himself in the process, his attitude towards his own health and strict compliance with all doctor’s instructions.
Heart and vascular diseases - general information on News4Health.ru
Cardiology is a field of medicine that studies the vital system of the human body - the cardiovascular system: the structural features and functions of the heart and blood vessels, the causes and mechanisms of pathology; develops and improves methods for diagnosing, preventing and treating cardiovascular diseases. Considerable attention in cardiology is paid to the rehabilitation of patients with cardiovascular pathology. Unfortunately, heart and vascular diseases have an increasing tendency to affect young people and represent one of the most important problems of modern health care.
Practical cardiology is developing in two directions: therapeutic cardiology and cardiac surgery. Therapeutic cardiology uses conservative methods (medicines, sanatorium treatment) for the treatment of cardiovascular diseases: bradycardia, tachycardia, arrhythmia, extrasystole, vegetative-vascular dystonia, vascular atherosclerosis, arterial hypertension, angina pectoris, myocardial infarction, coronary heart disease, heart failure, myocarditis, pericarditis, endocarditis.
Surgical cardiology surgically eliminates congenital and acquired heart defects and other lesions of the heart and blood vessels, and performs prosthetics of heart valves and vessels.
Cardiovascular diseases are currently considered the most common cause of disability and early mortality in economically prosperous Western countries. According to statistics, the mortality rate due to cardiovascular diseases is 40-60% annually of the total number of deaths.
The main symptoms that allow one to suspect the development of cardiovascular diseases are pain arising behind the sternum and radiating to the left shoulder or scapula, shortness of breath, persistently elevated blood pressure (BP over 140/90 mm Hg), tachycardia (heart rate more than 100 beats per minute) or bradycardia (pulse less than 50 beats per minute), interruptions in heart rhythm, edema. When the first signs of heart and vascular diseases appear, in order to avoid the development of persistent disorders and complications, you must immediately contact a cardiologist. In the initial period of disease development, restoration of functions is achieved more easily and with smaller doses of drugs.
Currently, cardiology has reached a new level in terms of being equipped with the most modern equipment for quick and early diagnosis and timely treatment of cardiovascular pathology. The main diagnostic methods in cardiology are: phonocardiography, electrocardiography (ECG), echocardiography (ultrasound of the heart), daily ECG monitoring. They allow you to assess the contractile function and condition of the heart muscle, cavities, valves and blood vessels of the heart. Over the past few decades, new methods for examining patients with cardiac pathology have been actively developed: probing of the heart cavities and angiocardiography, which allow diagnosing and planning operations on the heart and coronary vessels.
Modern technologies and methods of treating cardiac pathology make it possible to cope with heart diseases that were considered incurable just yesterday. With the help of heart transplantation, cardiology today saves the lives of many desperate patients.
The main directions in the complex of preventive measures to prevent heart disease are optimal physical activity, giving up bad habits, eliminating nervous overload and stress, healthy eating and proper rest.
Prevention of coronary artery disease is the best medicine
If a person is diagnosed with coronary artery disease, angina pectoris FC 2, the lifestyle must be structured in such a way as to minimize the possibility of an attack and complications in the form of stroke, heart attack and death.
Doctors advise using the principle with the same abbreviation as the disease itself - IHD. The letter “I” here means: “get rid of tobacco smoke,” the letter “B” means “move more,” and the letter “C” means “lose excess weight.”
You also need a rational, balanced diet, rich in components that regulate the functioning of the whole body: vitamins, micro- and macroelements, amino acids, fiber.
Answering the question of what angina pectoris FC 2 is - what it is, doctors talk about a symptom complex of problems in the functioning of the heart and cardiovascular system, manifested in attacks of pain in the chest and are a harbinger of serious health problems.