Our body is designed in such a way that if one organ is damaged, the whole system suffers, which ultimately leads to general exhaustion of the body. The main organ in human life is the heart, which consists of three main layers. The myocardium is considered one of the most important and susceptible to damage. This layer is muscle tissue, which consists of transverse fibers. It is this feature that allows the heart to work many times faster and more efficiently. One of the main functions is myocardial contractility, which may decrease over time. It is the causes and consequences of this physiology that should be carefully considered.
The contractility of the heart muscle decreases during cardiac ischemia or myocardial infarction.
It must be said that our cardiac organ has a fairly high potential in the sense that it can increase blood circulation if necessary. Thus, this can occur during normal sports activities, or during heavy physical labor. By the way, if we talk about the potential capabilities of the heart, the volume of blood circulation can increase up to 6 times. But it happens that myocardial contractility decreases for various reasons, this already indicates its reduced capabilities, which should be diagnosed in time and the necessary measures taken.
Reasons for the decline
For those who do not know, it should be said that the functions of the myocardium of the heart represent a whole algorithm of work that is not violated in any case. Thanks to the excitability of cells, the contractility of the heart walls and the conductivity of the blood flow, our blood vessels receive a portion of useful substances that are necessary for full performance. Myocardial contractility is considered satisfactory when its activity increases with increasing physical activity. It is then that we can talk about full health, but if this does not happen, we should first understand the reasons for this process.
It is important to know that decreased contractility of muscle tissue can be due to the following health problems:
- avitaminosis;
- myocarditis;
- cardiosclerosis;
- hyperthyroidism;
- increased metabolism;
- atherosclerosis, etc.
So, there can be a lot of reasons for a decrease in muscle tissue contractility, but the main one is one. During prolonged physical activity, our body may not receive not only the required portion of oxygen, but also the amount of nutrients that are necessary for the body’s functioning and from which energy is produced. In such cases, first of all, internal reserves that are always available in the body are used. It is worth saying that these reserves are not enough for a long time, and when they are depleted, an irreversible process occurs in the body, as a result of which cardiomyocytes are damaged (these are the cells that make up the myocardium), and the muscle tissue itself loses its contractility.
In addition to the fact of increased physical activity, reduced contractility of the left ventricular myocardium can occur as a result of the following complications:
- severe brain damage;
- consequence of unsuccessful surgery;
- heart-related diseases, such as ischemia;
- after myocardial infarction;
- a consequence of toxic effects on muscle tissue.
It must be said that this complication can greatly ruin a person’s quality of life. In addition to the general deterioration of a person's health, it can provoke heart failure, which is not a good sign. It is necessary to clarify that myocardial contractility must be preserved under any circumstances. To do this, you should limit yourself from overwork during prolonged physical activity.
Some of the most noticeable signs are the following signs of reduced contractility:
- fast fatiguability;
- general weakness of the body;
- rapid weight gain;
- rapid breathing;
- swelling;
- attacks of night suffocation.
Diagnosing decreased contractility
At the first signs mentioned above, you should consult a specialist; under no circumstances should you self-medicate or ignore this problem, as the consequences can be disastrous. Often, to determine the contractility of the left ventricular myocardium, which may be satisfactory or reduced, a conventional ECG plus echocardiography is performed.
Myocardial echocardiography allows you to measure the volume of the left ventricle of the heart in systole and diastole
It happens that after an ECG it is not possible to make an accurate diagnosis, then the patient is prescribed Holter monitoring. This method allows you to make a more accurate conclusion using constant monitoring of an electrocardiograph.
In addition to the above methods, the following are used:
- ultrasound examination (ultrasound);
- blood chemistry;
- blood pressure control.
Treatment options
In order to understand how to carry out treatment, you first need to conduct a qualified diagnosis, which will determine the degree and form of the disease. For example, global contractility of the left ventricular myocardium should be eliminated using classical treatment methods. In such cases, experts recommend taking medications that help improve blood microcirculation. In addition to this course, medications are prescribed that can be used to improve metabolism in the heart organ.
Medicinal substances are prescribed that regulate metabolism in the heart and improve blood microcirculation
Of course, in order for the therapy to have the desired result, you must get rid of the underlying disease that caused the illness. In addition, if it comes to athletes or people with increased physical activity, then for starters you can get by with a special regime that limits physical activity and recommends daytime rest. In more severe forms, bed rest is prescribed for 2-3 days. It is worth saying that this disorder can be easily corrected if diagnostic measures are carried out in a timely manner.
Myocardial contractility is the ability of the heart muscle to provide rhythmic contractions of the heart automatically in order to move blood through the cardiovascular system. The heart muscle itself has a specific structure that differs from other muscles of the body.
Features of the myocardium
The myocardium has a number of physical and physiological properties that allow it to ensure the full functioning of the cardiovascular system. These features of the heart muscle make it possible not only to maintain blood circulation, ensuring a continuous flow of blood from the ventricles into the lumen of the aorta and pulmonary trunk, but also to carry out compensatory and adaptive reactions, ensuring the body’s adaptation to increased stress.
The physiological properties of the myocardium are determined by its extensibility and elasticity. The extensibility of the heart muscle ensures its ability to significantly increase its own length without damaging or disrupting its structure.
The elastic properties of the myocardium ensure its ability to return to its original shape and position after the effect of deforming forces (contraction, relaxation) ends.
Also, the ability of the heart muscle to develop strength during myocardial contraction and perform work during systole plays an important role in maintaining adequate cardiac activity.
What is myocardial contractility?
Cardiac contractility is one of the physiological properties of the heart muscle, which realizes the pumping function of the heart due to the ability of the myocardium to contract during systole (leading to the expulsion of blood from the ventricles into the aorta and pulmonary trunk (TP)) and relax during diastole.
First, the contraction of the atrial muscles occurs, and then the papillary muscles and the subendocardial layer of the ventricular muscles. Further, the contraction spreads to the entire inner layer of the ventricular muscles. This ensures a full systole and allows you to maintain a continuous ejection of blood from the ventricles into the aorta and LS.
The contractility of the myocardium is also supported by:
- excitability, the ability to generate an action potential (get excited) in response to stimuli;
- conductivity, that is, the ability to conduct the generated action potential.
Cardiac contractility also depends on the automatism of the heart muscle, manifested by the independent generation of action potentials (excitations). Thanks to this feature of the myocardium, even a denervated heart is able to contract for some time.
What determines the contractility of the heart muscle?
The physiological characteristics of the heart muscle are regulated by the vagus and sympathetic nerves, which can influence the myocardium:
- chronotropic;
- inotropic;
- bathmotropic;
- dromotropic;
- tonotropically.
Features of the heart muscle
The excitability of the heart muscle is not the same in all parts of the heart. The most excitable is the sinusoatrial node. The excitability of the His bundle is much less. Although during contraction the heart muscle is excitable. But during this period, which almost coincides with systole, the strongest artificial irritations of the heart do not cause a new contraction due to “the conflict of two strong excitations, placed too close to each other in time in the same substrate” (A. A. Ukhtomsky). This state of complete loss of excitability during heart contraction is referred to as absolute refractoriness. After this, during relaxation of the heart muscle when the heart is irritated by a shock of inductive electric current, due to a change in the time interval between two excitations and a change in the functional state of the heart, an out-of-turn, but weaker contraction can be obtained.
This second period of incomplete excitability during cardiac relaxation is referred to as relative refractoriness. Immediately after a period of relative refractoriness, a short-term increase in excitability is observed - the exaltation phase. The duration of absolute and relative refractoriness depends on the duration of the cardiac cycle. The period of absolute refractoriness of the sinus node in humans reaches 0.3 s., the atria - from 0.06 to 0.12 s., and the ventricles - from 0.3 to 0.4 s.
Due to prolonged refractoriness, the heart responds to prolonged stimulation with rhythmic contractions and, under normal conditions, cannot enter a state of tetanus.
If irritation is applied to the ventricle of the heart of a cold-blooded animal before the arrival of the next automatic impulse, i.e., in a period of relative refractoriness, then a premature contraction of the heart occurs - an extrasystole, followed by a compensatory pause, the duration exceeding the usual one.
Extrasystoles occur when there are changes in the conduction system or in the heart muscle. The effect on changes in excitability is designated as bathmotropic.
Contraction of the heart muscle does not increase with increasing stimulation. If you directly apply irritation to the heart muscle, increasing the amount of irritation each time, the following fact is discovered. Initially, with weak irritations, the muscle does not respond by contracting, then with a slight increase in the magnitude of irritation, it contracts. This reduction is maximum. A further increase in the strength of stimulation no longer increases the contraction of the heart muscle (G. Bowdich, 1871).
However, this is only a special case, and not a rule, since the height of contraction of the heart muscle (“everything”) changes and depends on its excitability and lability, i.e., on its functional state. “Nothing” also does not exist, since with subthreshold stimulation, excitation occurs, which is summed up at a certain frequency of stimulation.
The magnitude of the greatest contraction of the heart muscle depends on the level of metabolism in it. The effect on the strength of heart contractions is referred to as inotropic.
In the process of phylogenesis, the ability of the heart muscle to increase the force of its contractions has developed depending on the increase in the amount of blood flowing to the heart and the increase in blood pressure in the arterial system.
Increased blood flow to the heart and increased blood pressure are physiologically caused by muscle activity and certain emotions.
How does the heart increase the force of its contractions under increased loads?
The force of heart contraction increases due to an increase in the initial length of muscle fibers (Starling, 1916).
Muscle fibers have a certain length during cardiac diastole during rest of the body, before the start of heart contraction (initial length). With an increase in blood flow to the heart and with outflow difficulties caused by an increase in blood pressure, the heart in diastole, from the cavity being overfilled with blood, stretches more, therefore, the initial length of the muscle fibers of the heart increases. The greater the blood flow to the heart, or the greater the blood pressure that impedes the flow of blood, the greater the initial stretch of the muscle fibers.
Using isolated muscles, it was found that the energy of contraction of skeletal and cardiac muscles is directly proportional to the length of the muscle fibers. The greater the initial fiber length, the stronger the contraction. Therefore, as the initial length of the heart fibers increases, it contracts more strongly during systole and, due to this, the amount of blood ejected increases.
Blood supply and nutrition to the heart muscle is of great importance. The better the nutrition of the muscle, the less it pre-stretches.
Under natural conditions, in the absence of additional stretching of the heart, an increase in the force of contractions is the result of increased metabolism in the heart muscle under the influence of the nervous system (trophic influence).
When the heart muscle gets tired, the pressure in the heart drops and it stretches. The ability of the heart to perform the same work during fatigue depends on the degree of stretching of its muscle fibers.
The degree of cardiac stretching is determined by the thickness and condition of the heart muscle. The heart can expand as much as possible to the pericardium, which thus determines the maximum expansion of the heart.
You might be interested in:
Neuromuscular drug
Structure of the heart
Muscle strength
Human musculoskeletal system
Blood supply to the heart
How is myocardial contractility regulated?
The influence of the vagus nerves causes a decrease in:
- myocardial contractility,
- heart rate,
- generation of action potential and its propagation,
- metabolic processes in the myocardium.
That is, it has exclusively negative inotropic, tonotropic, etc. effects.
The influence of sympathetic nerves is manifested by an increase in myocardial contractility, an increase in heart rate, acceleration of metabolic processes, as well as an increase in the excitability and conductivity of the heart muscle (positive effects).
With reduced blood pressure, the sympathetic effect on the heart muscle is stimulated, myocardial contractility increases and heart rate increases, due to which compensatory normalization of blood pressure occurs.
When pressure increases, a reflex decrease in myocardial contractility and heart rate occurs, allowing blood pressure to be lowered to an adequate level.
Myocardial contractility is also influenced by significant stimulation:
- visual,
- auditory,
- tactile,
- temperature, etc. receptors.
This causes changes in the frequency and strength of heart contractions during physical or emotional stress, being in a hot or cold room, as well as when exposed to any significant irritants.
Of the hormones, adrenaline, thyroxine and aldosterone have the greatest effect on myocardial contractility.
The role of calcium and potassium ions
Also, potassium and calcium ions can change the contractility of the heart. With hyperkalemia (excess potassium ions), there is a decrease in myocardial contractility and heart rate, as well as inhibition of the formation and conduction of the action potential (excitation).
Calcium ions, on the contrary, help to increase myocardial contractility, the frequency of its contractions, and also increase the excitability and conductivity of the heart muscle.
Drugs that affect myocardial contractility
Cardiac glycoside preparations
have a significant effect on myocardial contractility .
This group of drugs can have a negative chronotropic and positive inotropic effect (the main drug of the group, digoxin, in therapeutic doses increases myocardial contractility). Due to these properties, cardiac glycosides are one of the main groups of drugs used in the treatment of heart failure. Also, beta blockers (reduce myocardial contractility, have negative chrontropic and dromotropic effects), Ca channel blockers (have a negative inotropic effect), ACE inhibitors (improve the diastolic function of the heart, helping to increase cardiac output in systole) and etc.
Increased myocardial contractility and cardiac output
In order to increase myocardial contractility, it is advisable, first of all, to use cardiac glycosides. In practice, these drugs must be prescribed to all patients with circulatory disorders and congestion in both the small and large circles, including those patients who have rhythm and conduction disturbances and even those with increased cardiac output. Moreover, the effectiveness of glycosides varies in different diseases and even in individual patients with the same suffering. Cardiac glycosides are more effective for heart defects without signs of rheumatic activity, as well as for atherosclerotic heart disease. The effect is usually less pronounced in myocarditis and myocardial lesions in diseases such as thyrotoxicosis, anemia, myocardiopathy with amyloidosis, hemochromatosis, uremia, etc. An absolute contraindication to the use of glycosides is a condition associated with intoxication with them. However, these symptoms can often be mildly expressed, close to the manifestations of heart failure itself, and careful monitoring is required for their timely diagnosis. A slight slowdown in atrioventricular conduction is not a contraindication to the use of glycosides. However, with a blockade with 2:1 impulses and the presence of Wenckebach periods, these agents should be used with caution. With complete transverse blockade, these drugs can be administered if there is confidence that the increase in conduction disturbances and the occurrence of blockade were not associated with taking glycosides.
Indications for the prescription of glycosides are always determined clinically when signs of heart failure are detected, even at the initial stage. Typically, complex treatment is carried out, which includes rest, diuretics, and a salt-restricted diet. Therefore, the completeness of “digitalization” can be difficult to assess. The maximum dose and duration of its administration are determined in each specific case individually, taking into account the dynamics of clinical data.
The effectiveness of glycosides in patients with heart failure has attracted much attention from pharmacologists for many years. Much work has been done to study the mechanism of action of these drugs on the heart, as well as to introduce new effective substances of this series into practice and isolate active agents in chemically pure form. Cardiac glycosides are found in a large number of plants. The most commonly used preparations are those obtained from foxglove purpurea (digitoxin), foxglove woolly (digoxin, lantoside, celanide, or isolanide), adonis (adonis, strophanthin, etc.). From a chemical point of view, active glycosides consist of two main parts: genin, a structure similar to steroid hormones (based on cyclopentaneperhydrophenanthrene), and a five- or six-membered lactone ring and a carbohydrate molecule attached to genin. The pharmacological action is primarily associated with genin. The carbohydrate molecule determines to a large extent such properties of the drug as the ability to be absorbed, accumulate in the body and pass through biological membranes. A complete synthesis of cardiac glycosides has not been carried out, but their synthetic derivatives have been obtained by combining various groups with a steroid core (for example, acetyl-strophanthin, which contains an acetate group in the third position).
The positive inotropic effect with increased contractility of myocardial fibers as a result of the direct action of cardiac glycosides on them was convincingly demonstrated in experiments on isolated cat papillary muscles. When digitoxin was added to the solution in which these muscles were located, their previously depleted ability to contract under the influence of electrical impulses was quickly restored. This direct effect of glycosides on the myocardium has also been shown in the human heart during surgery using artificial circulation, when cardiac contractility was assessed using electrokymography or by the rate of change in pressure in the left ventricle. Cardiac glycosides worsen conduction in the myocardium and increase the refractory period of the atrioventricular node. However, the individual sensitivity of the heart of different people in this regard varies greatly, up to the possibility of slowing down atrioventricular conduction during treatment with therapeutic doses of the drug. The increase in the refractory period of the atrioventricular node is associated with both the direct influence of glycosides and their vagotropic effect. The refractory period of the atria and ventricles myocardium decreases under the influence of cardiac glycosides.
Toxic doses of digitalis cause arrhythmias and conduction disturbances, which are associated with various effects, including increased automaticity and decreased excitability and Purkinje fiber conduction. The susceptibility of the ventricles to fibrillation increases. Depending on the predominance of one or another toxic effect, digitalis in a lethal dose can cause ventricular fibrillation or cardiac arrest.
The exact mechanism of action of glycosides on the contractile myocardium has not yet been clarified. Using modern technology, it has been shown that cardiac glycosides provide a parallel and proportional increase in the force of contraction of muscle fibers and their oxygen absorption. At the same time, they enhance the oxidation of glucose and free fatty acids in the heart.
Toxic doses of glycosides reduce the potassium content in the heart muscle. The decrease in intracellular potassium concentration is due to inhibition of potassium influx while its outflow remains unchanged. It is assumed that a decrease in intracellular potassium content is the most significant result of the action of these drugs, ultimately responsible for their inotropic effect. However, not all researchers agree with this. It is considered very likely that the action of glycosides is related to their influence on the movement of calcium ion in myocardial cells, since it is this ion that also has a positive inotropic effect by participating in the coupling of the processes of excitation and contraction. Using modern technology, it has not yet been possible to reliably establish the nature of the movements of calcium ion in myocardial cells and changes in its content in the sarcoplasmic reticulum and mitochondria under the influence of digitalis. The effect of digitalis on adenosine triphosphatase was studied. Some authors have noted that glycosides reduce the activity of potassium- and sodium-dependent adenosine triphosphatase. Because the ion pump requires adenosine triphosphate energy, inhibition of adenosine triphosphatase can alter the intracellular ion content. It should be noted that this effect of glycosides has been shown in many cell types, with glycosides typically being added at toxic concentrations. Other studies have found that non-toxic concentrations of glycosides lead to stimulation of adenosine triphosphatase. This suggests that it is this enzyme that is the “receptor” of glycosides, through which they exert their inotropic effect.
Some metabolic effects of glycosides are close to the action of catecholamines. In this regard, the assumption that glycosides increase myocardial contractility as a result of the release of catecholamines has been discussed, but it has not been convincingly confirmed. There is also no definite evidence that glycosides directly affect myocardial proteins. Thus, the mechanism of inotropic action of glycosides requires further study.
Cardiac glycosides also have extracardiac effects. They cause, in particular, bradycardia, which is associated with their vagotropic effect. This also partially explains the tendency to atrioventricular conduction disorders.
Direct injection of cardiac glycosides into the perfused artery leads to its spasm, although relatively short-lived compared to the longer-term inotropic effect. In an experiment on dogs, a tendency to spasm of the coronary arteries under the influence of glycosides was noted. However, the clinical significance of these observations is questionable. An increase in angina attacks under the influence of glycosides is not observed. In healthy individuals, venoconstriction is observed, and in heart failure, paradoxical dilatation of the veins. Under the influence of the direct irritating effect of glycosides on the mucous membrane of the gastrointestinal tract, as well as on the central nervous system, anorexia, nausea, vomiting, and diarrhea are often observed. When strophanthin is administered into the renal artery of a dog, the excretion of sodium and water increases, indicating a direct effect of the drug on the tubules. It is associated with inhibition of adenosine triphosphatase, but a similar explanation for the diuretic effect of glycosides in patients with heart failure is considered unlikely, since in healthy people there is no diuretic effect when strophanthin is administered.
The effect of glycosides on the heart and blood circulation in healthy individuals and in patients with heart failure is somewhat different. Patients experience an increase in cardiac output with improved cardiac emptying and a decrease in pressure in the atria, veins and pulmonary artery. At the same time, renal blood flow improves, glomerular filtration increases and, apparently, aldosterone secretion decreases. All this leads to increased natriuresis with a decrease in the volume of circulating blood and, subsequently, in the size of the heart. In individuals with a healthy heart, when glycosides are administered, cardiac output does not change or even decreases. However, in this case, this indicator reflects not only myocardial contractility, but also a number of other changes in blood circulation. It has been shown that myocardial contractility increases, although at the same time there is a sharp decrease in pressure in the left atrium due to a decrease in venous inflow. These effects are practically neutralized in patients in whom the decisive factor is improvement in cardiac function. The effect of glycosides on heart size in both healthy and sick individuals also usually depends on their direct effect not only on the myocardium, but also on the autonomic nervous system and blood vessels. Bearing in mind the effect (including indirect) on the electrical activity of the heart, it is necessary to point out the possibility of the occurrence of almost any conduction disturbances and ectopic arrhythmias under the influence of glycosides.
Glycoside preparations differ from each other in absorption, speed of onset of effect and its duration. Absorption when taking the drug orally ranges from 10-20% for lantoside to 60-70% for digoxin and up to 100% for digitoxin. The speed of onset of the effect varies from 5-10 minutes with intravenous administration of strophanthin to 1 hour when taking digitoxin. The metabolism and excretion of glycosides have been studied using drugs labeled with radioactive isotopes. The half-life of digoxin is 1.5 days, and it is excreted unchanged in the urine, and therefore the maintenance dose should be reduced in chronic renal failure (with a sharp decrease in renal function to 3 times the average dose for patients with normal renal function).
Indications for use, the size of the maintenance dose and the need to discontinue cardiac glycosides due to intoxication are determined, as a rule, taking into account a comprehensive assessment of clinical manifestations and previous treatment (taking drugs that promote potassium excretion). On the ECG, changes usually appear in connection with digitalization, primarily in the terminal part of the ventricular ST-T complex, but they often do not correlate with either the optimal effect achieved or with toxic phenomena that may later occur in the form of atrioventricular conduction disorders.
Treatment of heart failure with glycosides is most often carried out long-term using maintenance doses. However, in case of many myocardial diseases, digitalization can be limited to a period of exacerbation of the underlying disease, which is sometimes stopped by the combined use of a number of drugs that eliminate the main cause of heart failure (as, for example, in thyrotoxicosis, rheumatic carditis, etc.).
- Cardiac glycoside preparations
- Intoxication with cardiac glycosides
Why is contractility disorder dangerous?
Reduced myocardial contractility is accompanied by a decrease in cardiac output and impaired blood supply to organs and tissues. As a result, ischemia develops, metabolic disorders occur in tissues, hemodynamics are disrupted and the risk of thrombosis increases, and heart failure develops.
When SM may be violated
A decrease in SM can be observed against the background of:
- myocardial hypoxia ;
- coronary heart disease ;
- severe atherosclerosis of the coronary vessels;
- myocardial infarction and post-infarction cardiosclerosis;
- cardiac aneurysm (a sharp decrease in contractility of the left ventricular myocardium is observed);
- acute myocarditis, pericarditis and endocarditis;
- cardiomyopathies (the maximum impairment of SM is observed with depletion of the adaptive capabilities of the heart and decompensation of cardiomyopathy);
- brain injuries;
- autoimmune diseases;
- strokes;
- intoxication and poisoning;
- shocks (toxic, infectious, painful, cardiogenic, etc.);
- avitaminosis;
- electrolyte imbalances;
- blood loss;
- severe infections;
- intoxication with the active growth of malignant neoplasms;
- anemia of various origins;
- endocrine diseases.
Impaired myocardial contractility - diagnosis
The most informative methods for studying SM are:
- standard electrocardiogram;
- ECG with stress tests;
- Holter monitoring;
- ECHO-K.
Also, to identify the cause of a decrease in SM, a general and biochemical blood test, a coagulogram, a lipid profile are performed, the hormonal profile is assessed, an ultrasound scan of the kidneys, adrenal glands, thyroid gland, etc. is performed.
SM on ECHO-KG
The most important and informative study is ultrasound examination of the heart (assessment of ventricular volume during systole and diastole, myocardial thickness, calculation of minute blood volume and effective cardiac output, assessment of the amplitude of the interventricular septum, etc.).
Treatment of SM disorders
All treatment should be selected by a cardiologist in accordance with the cause of the SM disorder.
To improve metabolic processes in the myocardium, drugs can be used:
- riboxin,
- mildronate,
- L-carnitine,
- phosphocreatine,
- B vitamins,
- vitamins A and E.
Potassium and magnesium preparations (Asparkam, Panangin) can also be used.
Patients with anemia are advised to take iron, folic acid, and vitamin B12 supplements (depending on the type of anemia).
If lipid balance disorders are detected, lipid-lowering therapy may be prescribed. To prevent thrombosis, antiplatelet agents and anticoagulants are prescribed according to indications.
Also, drugs that improve the rheological properties of blood (pentoxifylline) can be used.
Patients with heart failure may be prescribed cardiac glycosides, beta blockers, ACE inhibitors, diuretics, nitrate preparations, etc.
Transverse heart block
Transverse heart block is a violation of the propagation of the excitation wave coming from the sinoauricular region at the level of the atrioventricular node.
Transverse blockade can occur as a result of ischemic damage to the localization area of the atrioventricular node, with infections, intoxication, myocarditis, rheumatic lesions, thyrotoxicosis, the use of certain medications (cardiac glycosides, beta blockers, etc.),
Depending on the depth of conduction disturbance of the atrioventricular node, four degrees of transverse heart block are distinguished.
First degree block (simple prolongation of the PQ interval)
This is the mildest degree of conduction disturbance, which is characterized by only a slight slowdown in the conduction of impulses through the atrioventricular region. In this case, each impulse generated by the sinus node is conducted to the ventricles. The rhythm remains correct. On the ECG, first-degree transverse block is manifested as a prolongation of the PQ interval by more than 0.21 s.
Second degree block (periodic loss of the ventricular complex)
This type of transverse block consists of a progressive (over several cardiac cycles) decrease in the conductivity of the atrioventricular node, which ultimately ends in a temporary complete loss of its ability to conduct impulses. As a result, one ventricular contraction is lost.
Next, the properties of the atrioventricular node are restored, and a similar cycle is repeated again and again. On the ECG, second degree transverse blockade can appear in two forms: Mobitz-I and Mobitz-I. Mobitz-I is characterized by a progressive increase in the PQ interval, which, upon reaching a certain critical limit, ends with the loss of the ventricular complex (Wenckebach-Samoilov periods).
Mobitz-II is characterized by periodic loss of the ventricular complex without a previous increase in the duration of the PQ interval.
Third degree block (incomplete transverse heart block)
In this case, not all impulses coming from the sinus node are conducted through the atrioventricular node, but only every second or every third, etc. Accordingly, the ratio of contractions of the atria and ventricles is 2:1,3:1, etc.
When impulse conduction is blocked over the atrioventricular region, the function of the pacemaker can be taken over by the upper part of the atrioventricular node. In this case, the frequency of ventricular contractions becomes not much lower than normal, and cardiac hemodynamics are not very deeply disturbed. Subjectively, this is expressed in the unpleasant sensations of interruptions in the functioning of the heart.
IV degree block (complete transverse heart block)
This type of atrioventricular conduction disorder is the most severe and is characterized by the fact that not a single impulse passes from the atria to the ventricles. At the same time, the atrioventricular node itself, as a rule, does not generate impulses (for this reason, we also considered this form of pathology in the subsection devoted to the pathology of heart automaticity).
In such a situation, the coordinated work of the atria and ventricles is disrupted: the atria contract in sinus rhythm, and the ventricles contract in idioventricular rhythm, since the His bundle becomes the pacemaker for them. Moreover, the frequency of ventricular contractions decreases to 30-40 per minute. Persistent complete heart block requires implantation of an artificial pacemaker.
Often, transverse heart block is complicated by the development of a very serious pathological condition - Morgagni-Edams-Stokes syndrome, which occurs when incomplete transverse blockade transitions to complete and vice versa.
At this moment, the so-called pre-automatic pause occurs, characterized by complete cardiac arrest, which can last from several seconds to several minutes and manifests itself depending on the duration from fainting to clinical death. This syndrome can occur up to several times a day.
Forecast
With timely detection of SM disorders and further treatment, the prognosis is favorable. In the case of the development of heart failure, the prognosis depends on its severity and the presence of concomitant diseases that aggravate the patient’s condition (post-infarction cardiosclerosis, cardiac aneurysm, severe heart block, diabetes mellitus, etc.).
All materials are published under the authorship or editorship of medical professionals (about the authors), but are not a prescription for treatment. Contact the specialists!
When using materials, a link or indication of the source name is required.
Author: Sazykina Oksana Yurievna, cardiologist
The heart muscle is the most resilient in the human body. The high performance of the myocardium is due to a number of properties of myocardial cells – cardiomyocytes. These properties include automaticity (the ability to independently generate electricity), conductivity (the ability to transmit electrical impulses to nearby muscle fibers in the heart) and contractility - the ability to contract synchronously in response to electrical stimulation.
In a more global concept, contractility refers to the ability of the heart muscle as a whole to contract in order to push blood into the large main arteries - the aorta and the pulmonary trunk. They usually talk about the contractility of the left ventricular myocardium, since it is the one that does the most work of pushing out blood, and this work is assessed by the ejection fraction and stroke volume, that is, by the amount of blood that is ejected into the aorta with each cardiac cycle.
Cardiac cycle
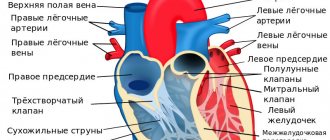
General characteristics of the structure and functioning of the heart
Animated image of the cardiac cycle
Cardiac cycle briefly
The heart contracts rhythmically and cyclically. One cycle lasts 0.8-0.85 seconds, which is approximately 72-75 contractions (beats) per minute.
Main phases:
- Systole is the contraction of the muscle layer (myocardium) and the release of blood from the cardiac cavities. First, the ears of the heart contract, then the atria and then the ventricles. Contraction runs through the heart in a wave from the ears to the ventricles. Contraction of the heart muscle is triggered by its excitation, and excitation begins from the sinoatrial node in the upper part of the atria.
- Diastole – relaxation of the heart muscle (myocardium).
At the same time, there is an increase in the own blood supply to the myocardium and metabolic processes in it. During diastole, the cavities of the heart are filled with blood: both the atria and the ventricles simultaneously. It is important to note that blood fills both the atria and the ventricles at the same time, because The valves between the atria and ventricles (atrioventricular) are open in diastole. Complete cardiac cycle
From the point of view of the movement of excitation through the heart muscle, the cycle should begin with the excitation and contraction of the atria, because It is on them that excitement comes from the main pacemaker of the heart - the sinoatrial node.
Pacemaker
The heart pacemaker is a special part of the heart muscle that independently generates electrochemical impulses that excite the heart muscle and lead to its contraction.
In humans, the leading pacemaker is the sinoatrial (sinoatrial) node. This is a section of cardiac tissue containing “pacemaker” cells , i.e. cells capable of spontaneous excitation. It is located on the fornix of the right atrium at the junction of the superior vena cava. The node consists of a small number of cardiac muscle fibers innervated by the endings of neurons from the autonomic nervous system. It is important to understand that autonomic innervation does not create an independent rhythm of heart impulses, but only regulates (changes) the rhythm that is set by the pacemaker cardiac cells themselves. Each wave of cardiac excitation originates in the sinoatrial node, which leads to contraction of the heart muscle and serves as a stimulus for the occurrence of the next wave.
Phases of the cardiac cycle
So, the wave of heart contraction, provoked by a wave of excitation, begins from the atria.
1. Systole (contraction) of the atria (together with the ears) – 0.1 s . The atria contract and push the blood already in them into the ventricles. The ventricles also already have blood, which poured into them from the veins during diastole, passing through the atria and open atrioventricular valves. Due to their contraction, the atria add additional portions of blood to the ventricles.
2. Diastole (relaxation) of the atria is the relaxation of the atria after contraction, it lasts 0.7 seconds. Thus, the rest time of the atria is much greater than the time they work, and this is important to know. From the ventricles, blood cannot return back to the atria thanks to special atrioventricular valves between the atria and ventricles (tricuspid on the right and bicuspid, or mitral, on the left). Thus, in diastole the walls of the atria are relaxed, but blood does not flow into them from the ventricles. During this period, the heart has 2 empty and 2 filled chambers. Blood from the veins begins to flow into the atria. At first, blood slowly fills the relaxed atria. Then, after the contraction of the ventricles and their relaxation, it opens the valves with its pressure and enters the ventricles. Atrial diastole has not yet ended.
And finally, a new wave of excitation is born in the sinoatrial node and, under its influence, the atria move to systole and push the blood accumulated in them into the ventricles.
3. Ventricular systole – 0.3 s . The excitation wave comes from the atria, as well as along the interventricular septum, and reaches the ventricular myocardium. The ventricles contract. Blood is pumped under pressure from the ventricles into the arteries. From the left - to the aorta, to run through the systemic circulation, and from the right - to the pulmonary trunk, to run through the pulmonary circulation. Maximum effort and maximum blood pressure are provided by the left ventricle. It has the most powerful myocardium of all the chambers of the heart.
4. Ventricular diastole - 0.5 s . Note that again rest lasts longer than work (0.5 s vs. 0.3). The ventricles have relaxed, the semilunar valves at their border with the arteries are closed, they do not allow blood to return to the ventricles. The atrioventricular (atrioventricular) valves are open at this time. The ventricles begin to fill with blood, which enters them from the atria, but so far without contraction of the atria. All 4 chambers of the heart, i.e. the ventricles and atria are relaxed.
5. Total diastole of the heart – 0.4 s . The walls of the atria and ventricles are relaxed. The ventricles are filled with blood flowing into them through the atria from the vena cava, 2/3, and the atria - completely.
6. New cycle . The next cycle begins - atrial systole .
Video: Pumping blood to the heart
To reinforce this information, look at the animated diagram of the cardiac cycle:
Animated diagram of the cardiac cycle - I highly recommend clicking and viewing the details!
Details of the work of the ventricles of the heart
1. Systole.
2. Expulsion.
3. Diastole
Ventricular systole
1. Systole period , i.e. contraction consists of two phases:
1) Asynchronous contraction phase – 0.04 s . There is an uneven contraction of the ventricular wall. At the same time, the interventricular septum contracts. Due to this, pressure increases in the ventricles, and as a result, the atrioventricular valve closes. As a result, the ventricles are isolated from the atria.
2) Isometric contraction phase . This means that the length of the muscles does not change, although their tension increases. The volume of the ventricles also does not change. All valves are closed, the walls of the ventricles contract and tend to shrink. As a result, the walls of the ventricles become tense, but the blood does not move. But at the same time, the blood pressure inside the ventricles increases, it opens the semilunar valves of the arteries and an outlet appears for the blood.
2. The period of blood expulsion is 0.25 s.
1) Rapid expulsion phase – 0.12 s.
2) Slow expulsion phase – 0.13 s.
Expulsion (ejection) of blood from the heart
Blood is forced under pressure from the left ventricle into the aorta. The pressure in the aorta increases sharply, and it expands, accepting a large portion of blood. However, due to the elasticity of its wall, the aorta immediately contracts again and drives blood through the arteries. The expansion and contraction of the aorta generates a transverse wave, which propagates at a certain speed through the vessels. This is a wave of expansion and contraction of the vascular wall - a pulse wave. Its speed does not match the speed of blood.
The pulse is a transverse wave of expansion and contraction of the arterial wall, generated by the expansion and contraction of the aorta when blood is released into it from the left ventricle of the heart.
Ventricular diastole
Protodiastolic period – 0.04 s. From the end of ventricular systole to the closure of the semilunar valves. During this period, part of the blood returns back to the ventricle from the arteries under blood pressure in the circulation.
Isometric relaxation phase – 0.25 s. All valves are closed, muscle fibers are contracted, they have not yet stretched. But their tension decreases. The pressure in the atria becomes higher than that in the ventricles, and this blood pressure opens the atrioventricular valves to allow blood to pass from the atria to the ventricles.
Filling phase . There is a general diastole of the heart, during which all its chambers are filled with blood, first quickly and then slowly. Blood transits through the atria and fills the ventricles. The ventricles are filled with blood to 2/3 of their volume. At this moment, the heart is functionally 2-chambered, because only its left and right halves are separated. Anatomically, all 4 chambers are preserved.
Presystole . The ventricles are finally filled with blood as a result of atrial systole. The ventricles are still relaxed, while the atria are already contracting.
Bioelectrical basis of myocardial contractility
heart contraction cycle
The contractility of the entire myocardium depends on the biochemical characteristics in each individual muscle fiber. The cardiomyocyte, like any cell, has a membrane and internal structures, mainly consisting of contractile proteins. These proteins (actin and myosin) can contract, but only if calcium ions enter the cell through the membrane. This is followed by a cascade of biochemical reactions, and as a result, the protein molecules in the cell contract like springs, causing contraction of the cardiomyocyte itself. In turn, the entry of calcium into the cell through special ion channels is possible only in the case of repolarization and depolarization processes, that is, sodium and potassium ion currents through the membrane.
With each incoming electrical impulse, the cardiomyocyte membrane is excited, and the flow of ions into and out of the cell is activated. Such bioelectric processes in the myocardium do not occur simultaneously in all parts of the heart, but one by one - first the atria are excited and contracted, then the ventricles themselves and the interventricular septum. The result of all processes is a synchronous, regular contraction of the heart with the ejection of a certain volume of blood into the aorta and further throughout the body. Thus, the myocardium performs its contractile function.
Video: more about the biochemistry of myocardial contractility
How does the heart contract?
Contractility is one of the properties of the myocardium, which consists in creating rhythmic movements of the atria and ventricles, allowing blood to be pumped into the vessels. The chambers of the heart constantly pass through 2 phases:
- Systole - is caused by the combination of actin and myosin under the influence of ATP energy and the release of potassium ions from the cells, while thin fibers slide over thick ones and the bundles decrease in length. The possibility of wave-like movements has been proven.
- Diastole - relaxation and separation of actin and myosin occurs, restoration of expended energy due to the synthesis of enzymes, hormones, and vitamins obtained through the “bridges”.
It has been established that the force of contraction is provided by calcium entering the myocytes.
The entire cycle of heart contraction, including systole, diastole and the general pause after them, with a normal rhythm fits into 0.8 seconds. Begins with atrial systole, the ventricles are filled with blood. Then the atria “rest”, moving into the diastole phase, and the ventricles contract (systole). Calculating the time of “work” and “rest” of the heart muscle showed that per day the state of contraction accounts for 9 hours 24 minutes, and the state of relaxation accounts for 14 hours 36 minutes.
The sequence of contractions, ensuring the physiological characteristics and needs of the body during stress and anxiety depend on the connection of the myocardium with the nervous and endocrine systems, the ability to receive and “decipher” signals, and actively adapt to human living conditions.
The spread of excitation from the sinus node can be traced by intervals and ECG waves
Why do you need to know about myocardial contractility?
Cardiac contractility is the most important ability that indicates the health of the heart itself and the entire body as a whole. In the case when a person’s myocardial contractility is within normal limits, he has nothing to worry about, since in the complete absence of cardiac complaints, we can confidently say that at the moment everything is in order with his cardiovascular system.
If the doctor suspects and confirms through examination that the patient has impaired or reduced myocardial contractility, he needs to be further examined as soon as possible and begin treatment if he has a serious myocardial disease. What diseases can cause impaired myocardial contractility will be discussed below.
What is normokinesis of myocardial contractility?
Dopamine increases myocardial contractility and reduces total pulmonary and total peripheral vascular resistance.
Inotropic drugs increase myocardial oxygen consumption, which in turn requires an increase in coronary blood flow. The purpose of the study was to study the contractile function of the myocardium of the left and right ventricles using radioventriculographic methods.
LVEF in patients on the waiting list for heart transplantation is significantly reduced (Ј 40% in 78% and € 20% in 18% of patients). 13. Kapelko V.I. The importance of assessing ventricular diastole in the diagnosis of heart diseases.
Myocardial contractility according to ECG
The contractility of the heart muscle can be assessed already by performing an electrocardiogram (ECG), since this research method allows you to record the electrical activity of the myocardium. With normal contractility, the heart rhythm on the cardiogram is sinus and regular, and the complexes reflecting contractions of the atria and ventricles (PQRST) have the correct appearance, without changes in individual teeth. The nature of the PQRST complexes in different leads (standard or chest) is also assessed, and with changes in different leads, one can judge the impairment of contractility of the corresponding sections of the left ventricle (lower wall, high-lateral sections, anterior, septal, apical-lateral walls of the LV). Due to its high information content and ease of use, an ECG is a routine research method that allows timely identification of certain disorders in the contractility of the heart muscle.
Longitudinal heart block
Longitudinal heart block is understood as a violation of impulse conduction at the level of the left or right bundle branch. Most often, the cause of the development of this type of pathology is focal ischemia of the corresponding area of the myocardium of the interventricular septum.
Depending on the depth of damage to the conduction system of the heart, longitudinal blockade can be accompanied by various disorders of cardiac activity, up to pronounced dissociation in the activity of the ventricles, consisting in their asynchronous contraction.
With complete blockade of the right bundle branch, excitation to the right ventricle spreads from the left. The ECG shows a tall and wide R wave in the right precordial leads.
With complete blockade of the left bundle branch, excitation of the left ventricle occurs when it spreads from the right. In this case, on the ECG in the right chest leads, the R wave will have a small amplitude, the S wave will be wide and deep; in the left chest leads the R wave is wide and jagged (M-shaped).
Normal cardiac contractility and abnormal myocardial contractility
Whether the patient has preserved contractility of the heart muscle or not can be reliably judged only after an ultrasound of the heart. Thus, based on the calculation of the total wall mobility index, as well as determining the thickness of the LV wall during systole, it is possible to identify a normal type of contractility or deviations from the norm. Thickening of the studied myocardial segments of more than 40% is considered normal. An increase in myocardial thickness by 10-30% indicates hypokinesia, and a thickening of less than 10% of the original thickness indicates severe hypokinesia.
Based on this, the following concepts can be distinguished:
- Normal type of contractility - all segments of the LV contract in full force, regularly and synchronously, myocardial contractility is preserved,
- Hypokinesia – decreased local contractility of the LV,
- Akinesia is the complete absence of contraction of a given segment of the LV,
- Dyskinesia – myocardial contraction in the segment under study is incorrect,
- An aneurysm is a “protrusion” of the left ventricular wall, consisting of scar tissue, completely lacking the ability to contract.
In addition to this classification, disorders of global or local contractility are distinguished. In the first case, the myocardium of all parts of the heart is not able to contract with such force to achieve a full cardiac output. In case of disturbance of local myocardial contractility, the activity of those segments that are directly susceptible to pathological processes and in which signs of dys-, hypo- or akinesia are visualized decreases.
What diseases cause myocardial contractility disorders?
graphs of changes in myocardial contractility in various situations
Disturbances in global or local myocardial contractility can be caused by diseases characterized by the presence of inflammatory or necrotic processes in the heart muscle, as well as the formation of scar tissue instead of normal muscle fibers. The category of pathological processes that provoke a violation of local myocardial contractility includes the following:
- Myocardial hypoxia in coronary heart disease,
- Necrosis (death) of cardiomyocytes during acute myocardial infarction,
- Scar formation in post-infarction cardiosclerosis and LV aneurysm,
- Acute myocarditis is an inflammation of the heart muscle caused by infectious agents (bacteria, viruses, fungi) or autoimmune processes (systemic lupus erythematosus, rheumatoid arthritis, etc.),
- Postmyocardial cardiosclerosis,
- Dilated, hypertrophic and restrictive types of cardiomyopathy.
In addition to pathology of the heart muscle itself, pathological processes in the pericardial cavity (in the outer lining of the heart, or in the heart sac) can lead to disruption of global myocardial contractility, which prevent the myocardium from fully contracting and relaxing - pericarditis, cardiac tamponade.
In acute stroke and brain injury, a short-term decrease in the contractility of cardiomyocytes is also possible.
More harmless causes of decreased myocardial contractility include vitamin deficiency, myocardial dystrophy (with general exhaustion of the body, dystrophy, anemia), as well as acute infectious diseases.
Are clinical manifestations of impaired contractility possible?
Changes in myocardial contractility are not isolated, and, as a rule, are accompanied by one or another myocardial pathology. Therefore, among the patient’s clinical symptoms, those that are characteristic of a specific pathology are noted. Thus, with acute myocardial infarction, intense pain in the heart region is observed, with myocarditis and cardiosclerosis - shortness of breath, and with increasing systolic dysfunction of the LV - edema. Heart rhythm disturbances (usually atrial fibrillation and ventricular extrasystole) are common, as well as syncope (fainting) conditions caused by low cardiac output and, as a consequence, low blood flow to the brain.
How to treat hypertrophy?
Typically, prolonged increased load causes hypertrophy. The thickness of the left ventricular wall increases by more than 15 mm. An important point in the formation mechanism is the lag in the growth of capillaries deep into the muscle. In a healthy heart, the number of capillaries per mm2 of cardiac muscle tissue is about 4000, and with hypertrophy the figure decreases to 2400.
Therefore, the condition is considered compensatory up to a certain point, but with significant thickening of the wall it leads to pathology. It usually develops in the part of the heart that must work hard to push blood through a narrowed hole or overcome a vascular obstruction.
Hypertrophied muscle is able to maintain blood flow for a long time in case of heart defects.
The muscle of the right ventricle is less developed; it works against a pressure of 15–25 mm Hg. Art. Therefore, compensation for mitral stenosis and cor pulmonale does not last long. But right ventricular hypertrophy is of great importance in acute myocardial infarction, cardiac aneurysm in the left ventricular area, and relieves overload. The significant capabilities of the right sections in training during physical exercises have been proven.
Thickening of the left ventricle compensates for aortic valve defects and mitral insufficiency
Do contractility disorders need to be treated?
Treatment of impaired contractility of the heart muscle is mandatory. However, when diagnosing such a condition, it is necessary to establish the cause that led to impaired contractility and treat this disease. Against the background of timely, adequate treatment of the causative disease, myocardial contractility returns to normal levels. For example, in the treatment of acute myocardial infarction, areas subject to akinesia or hypokinesia begin to normally perform their contractile function 4-6 weeks after the onset of the infarction.
How is reduced contractility treated?
The most accurate assessment of myocardial contractility is possible by performing ventriculography with simultaneous recording of intraventricular pressure. Many formulas and coefficients proposed for clinical practice only indirectly reflect myocardial contractility.
Further improvement in myocardial pumping function can be achieved by using several drugs that improve contractile function (eg, dopamine).
The ideal inotropic agent would appear to increase myocardial contractility without affecting heart rate. Unfortunately, there is currently no such tool. However, the doctor already has several drugs, each of which increases the inotropic properties of the myocardium.
Are there possible consequences?
If we talk about the consequences of this condition, then you should know that possible complications are caused by the underlying disease. They can be represented by sudden cardiac death, pulmonary edema, cardiogenic shock during a heart attack, acute heart failure during myocarditis, etc. Regarding the prognosis of impaired local contractility, it should be noted that zones of akinesia in the area of necrosis worsen the prognosis in acute cardiac pathology and increase the risk of sudden later cardiac death. Timely treatment of the causative disease significantly improves the prognosis, and patient survival increases.