The heart is an airless organ surrounded by air-rich lung tissue. As an airless organ, the heart produces a dull sound when percussed. But due to the fact that it is partially covered along the periphery by the lungs, the dull sound is not uniform. Therefore, relative and absolute dullness are distinguished. When percussing the area of the heart covered by the lungs, relative, or deep, dullness is determined, which corresponds to the true boundaries of the heart. Absolute, or superficial, dullness is determined over the area of the heart not covered by lung tissue.
Technique and rules of cardiac percussion
Percussion is performed in a vertical position of the patient (standing or sitting on a chair) with his arms down along the body. In this position, due to the descent of the diaphragm, the diameter of the heart is 15-20% smaller than in a horizontal position. In severely ill patients, percussion should be limited only in a horizontal position. A person sitting on a bed with his legs horizontally positioned and not lowered down has a high position of the dome of the diaphragm, maximum displacement of the heart and the least accurate results of cardiac percussion. Percussion is performed while the patient is breathing calmly. The position of the doctor should be comfortable for the correct placement of the pessimeter finger on the chest of the person being examined and the free application of percussion strikes with a hammer finger. When the patient is in a horizontal position, the doctor is on the right; in a vertical position, he is opposite him. Percussion of the heart is performed according to the following scheme: • determination of the boundaries of relative dullness of the heart, • determination of the contours of the cardiovascular bundle, configuration of the heart, size of the heart and vascular bundle, • determination of the boundaries of absolute dullness of the heart. Percussion of the heart is performed in compliance with all the “classical” rules of topographic percussion: 1) the direction of percussion from a clearer sound to a dull one; 2) the finger-pessimeter is installed parallel to the expected border of the organ; 3) the boundary is marked along the edge of the pessimeter finger facing the clear percussion sound; 4) quiet (to determine the boundaries of the relative dullness of the heart and the contours of the cardiovascular bundle) and the quietest (to determine the boundaries of the absolute dullness of the heart) percussion is performed.
Determination of the boundaries of relative cardiac dullness
The relative dullness of the heart is a projection of its anterior surface onto the chest. First, the right, then the upper, and then the left boundaries of the relative dullness of the heart are determined. However, before determining the boundaries of the relative dullness of the heart, it is necessary to establish the upper limit of the liver, i.e., the height of the right dome of the diaphragm, above which the right part of the heart is located. It should be taken into account that the upper border of the liver, corresponding to the height of the dome of the diaphragm, is covered by the right lung and upon percussion gives a dull sound (relative dullness of the liver), which cannot always be clearly determined. Therefore, in practice, it is customary to determine the upper limit of absolute dullness of the liver, corresponding to the lower limit of the right lung, which is oriented towards when finding the right border of the heart. To determine the location of the upper edge of the liver using percussion, a finger-pessimeter is placed in the second intercostal space to the right of the sternum, parallel to the ribs, along the midclavicular line and, changing the position of the finger-pessimeter downwards, percussion blows of medium strength are applied until dullness appears (lower edge lung, which in healthy people is located at the level of the VI rib). Determination of the right border of relative cardiac dullness. The pessimeter finger is placed one rib above the hepatic dullness, i.e., in the fourth intercostal space. Its position changes to vertical - parallel to the expected border of the heart. Tap from the right midclavicular line in the direction from the lungs to the heart until a clear sound transitions into dullness. The appearance of a shortened sound determines the most distant point of the right contour of the heart. Normally, the right border of the relative dullness of the heart is located in the fourth intercostal space 1-1.5 cm outward from the right edge of the sternum and is formed by the right atrium. Determination of the upper limit of the relative dullness of the heart is carried out 1 cm outward from the left edge of the sternum with the pessimeter finger in a horizontal position, moving from the first intercostal space down until dullness of the percussion sound appears. Normally, the upper limit of the relative dullness of the heart is at the level of the third rib or in the third intercostal space; in persons with an asthenic constitution, it is above the upper edge of the fourth rib, which is largely determined by the height of the dome of the diaphragm. The initial part of the pulmonary artery and the left atrial appendage participate in the formation of the upper limit of the relative dullness of the heart. Determination of the left border of relative dullness of the heart. The most distant point of the left contour of the heart is the apical impulse, which coincides with the left border of the relative dullness of the heart. Therefore, before you begin to determine the left border of the relative dullness of the heart, you need to find the apical impulse, which is necessary as a guide. In cases where the apex beat is not visible or palpable, the left border of the relative dullness of the heart is determined by percussion along the V and, in addition, along the VI intercostal spaces, in the direction from the anterior axillary line to the heart. The plessimeter finger is placed vertically, i.e., parallel to the supposed left border of the relative dullness of the heart, and percussed until dullness appears. Normally, the left border of the relative dullness of the heart is located in the 5th intercostal space 1-2 cm medially from the left midclavicular line and is formed by the left ventricle.
Determination of the right and left contour of the cardiovascular bundle, the size of the heart and vascular bundle, the configuration of the heart
Determining the boundaries of the contours of the cardiovascular bundle allows you to find the size of the heart and vascular bundle and get an idea of the configuration of the heart. The right contour of the cardiovascular bundle runs to the right of the sternum from the I to IV intercostal space. In the I, II, III intercostal spaces it is formed by the superior vena cava and is 2.5-3 cm from the anterior midline. In the IV intercostal space, the right contour is formed by the right atrium, is 4-4.5 cm from the anterior midline and corresponds to the right borderline of relative dullness of the heart. The place of transition of the vascular contour into the contour of the heart (right atrium) is called the “right cardiovascular (atriovasal) angle.”
Left contour of the cardiovascular bundle
passes to the left of the sternum from I to V intercostal space. In the 1st intercostal space it is formed by the aorta, in the 2nd by the pulmonary artery, in the 3rd by the left atrial appendage, in the 4th and 5th by the left ventricle. The distance from the anterior midline in the I-II intercostal spaces is 2.5-3 cm, in the III - 4.5 cm, in the IV-V - 6-7 cm and 8-9 cm, respectively. The border of the left contour in the V intercostal space corresponds to the left border of the relative dullness of the heart. The place where the vascular contour transitions to the left atrium contour represents an obtuse angle and is called the “left cardiovascular (atriovasal) angle,” or the waist of the heart. Methodically, percussion of the boundaries of the contours of the cardiovascular bundle (first the right, then the left) is carried out in each intercostal space from the midclavicular line towards the corresponding edge of the sternum with the pessimeter finger in a vertical position. In the first intercostal space (in the subclavian fossa), percussion is performed along the first (nail) phalanx of the plessimeter finger.
According to M.G. Kurlov, there are 4 heart sizes: length, diameter, height and width.
Percussion of the heart area
It is performed to determine the size, configuration and position of the heart, as well as the size of the vascular bundle.
The heart is a dense, airless body, over which a dull sound occurs when percussed. But due to the fact that it borders on the lungs and is partially covered by them, the sound can be absolutely dull or dull, that is, relatively dull. In this regard, a distinction is made between relative and absolute dullness of the heart.
Relative cardiac dullness corresponds to the true boundaries of the heart, absolute dullness corresponds to its anterior surface, not covered by the lungs (the anterior wall of the right ventricle). These boundaries are established by percussion, and thus the relative and absolute dullness of the heart is determined, respectively.
When determining the true boundaries of the heart, significant percussion force is required, since it is located deep and covered by the lungs. In addition, the thickness of the chest wall should also be taken into account. The thicker it is, the greater the force of the percussion blow should be. However, in all cases it should not be excessive. When moving the pessimeter finger from the lung to the location of the edge of the heart, the clear sound becomes dull. This dullness is called relative dullness of the heart, which speaks of its true boundaries, and therefore its size.
However, it should be noted that if the organ lies superficially, then the best results are obtained with a weak percussion strike. Therefore, when determining the boundaries of the area of the heart not covered by the lungs, it is necessary to use weak (quiet and even the quietest) percussion. Moreover, whenever the pessimeter finger, moving in the direction from the lungs to the heart, crosses the border between the anterior edges of the lungs and the uncovered area of the heart, the pulmonary sound is replaced by an absolutely dull sound. Therefore, the dullness obtained over this area will be absolute dullness of the heart.
When percussing the heart, the following rules are observed.
Percussion should be carried out in horizontal and vertical (if the patient's condition allows) positions of the patient. In the first case, the subject lies with his arms extended along his body, and the doctor is to his right. In the second, the examinee stands with his hands down, the doctor can sit or stand. Usually they use mediocre percussion - finger on finger. The pessimeter finger should fit snugly to the chest and be parallel to the desired boundary. You need to move it a short distance so as not to miss the desired boundary.
When determining the boundaries of relative dullness, percussion should be carried out in the direction from the lungs to the heart, i.e., from a clear pulmonary sound to dullness.
In the case of determining the boundaries of absolute dullness, it is better to percussion from a dull sound to a dull one, i.e. from the boundaries of the relative dullness of the heart to the boundaries of absolute dullness, but it is also possible in the opposite direction: from the heart to the lungs, i.e. from a dull sound to a dull one (choice method depends on hearing characteristics and skills). The border of the determined dullness is marked along the outer edge of the finger-pessimeter, facing the organ that produces a louder percussion sound, i.e., from the side of the clear pulmonary sound.
When percussing the heart, the boundaries of its relative dullness are first determined, and then its absolute dullness.
When determining the boundaries of relative dullness of the heart, the right boundary is first established, then the left, and then the upper.
To identify the right border of relative dullness of the heart along the right midclavicular line, the upper limit of absolute dullness of the liver (or the lower limit of the lung) is established, which is normally located in the VI intercostal space. After this, having risen up to the IV intercostal space (to get away from hepatic dullness masking cardiac dullness), the pessimeter finger is placed parallel to the desired border and moved towards the heart along the IV intercostal space. A change in percussion sound from clear pulmonary to dull will indicate reaching the limit of relative dullness of the heart. It should be noted that the pessimeter finger should be moved a short distance each time so as not to miss the boundaries of cardiac dullness. The first appearance of dullness indicates that the inner edge of the finger has crossed the border and is already within the location of the heart. The right border is marked along the outer edge of the finger, facing the clear percussion sound. It is formed by the right atrium and is normally located in the fourth intercostal space, protruding 1-1.5 cm beyond the right edge of the sternum.
Before establishing the left border of the relative dullness of the heart, it is necessary to determine the apical impulse, which serves as a guide. If it cannot be detected, percussion is performed in the 5th intercostal space starting from the anterior axillary line towards the sternum. The plessimeter finger is placed parallel to the desired boundary and, moving it, percussion blows of medium strength are applied until dullness appears. The mark of the left border of relative dullness is placed along the outer edge of the pessimeter finger, facing the clear percussion sound. Normally, it is formed by the left ventricle, is located in the 5th intercostal space at a distance of 1-1.5 cm medially from the left midclavicular line and coincides with the apical impulse.
When determining the upper limit of the relative dullness of the heart, a finger-pessimeter is placed near the left edge of the sternum parallel to the ribs and, moving it down along the intercostal spaces, blows of medium force are applied until dullness appears. A mark is placed along the upper edge of the pessimeter finger, facing the clear percussion sound. The upper limit of the relative dullness of the heart is formed by the contour of the pulmonary artery and the appendage of the left atrium and is normally located on the third rib along the left parasternal line.
Normally, the distance from the right border of relative dullness to the anterior midline is 3-4 cm, and from the left - 8-9 cm. The sum of these distances (11-13 cm) represents the diameter of the relative dullness of the heart.
To determine the configuration of the heart, percussion is performed sequentially in each intercostal space: to the right of IV and. higher. II, to the left of V and above—to II. In this case, the pessimeter finger is positioned, as usual, parallel to the expected dullness. The percussion blow should be of medium strength. The points obtained during percussion are connected to each other and, thus, the configuration of the heart is revealed. It may vary depending on the nature of his pathology. Thus, with mitral heart defects (mitral valve insufficiency, mitral stenosis), the heart acquires a “mitral configuration”. Due to the expansion of the left atrium and left ventricle, the waist of the heart is flattened due to an increase in the size of the left atrium. With aortic defects (aortic valve insufficiency, narrowing of the aortic opening), with pronounced forms of hypertension, the heart, as a result of isolated expansion of the left ventricle, acquires an “aortic configuration” - the appearance of a “boot” or “sitting duck”. In the case of combined and combined defects, all parts of the heart may enlarge. When there is a very sharp displacement of the boundaries of the heart in all directions, it is called “bull”.
To determine the boundaries of absolute cardiac dullness, quiet percussion should be used. The pessimeter finger is placed parallel to the desired boundary. Percussion is carried out from the boundaries of relative dullness to the boundaries of absolute dullness until an absolutely dull sound is obtained. First, the right, then the left, and finally the upper limit of absolute cardiac dullness are determined.
In order to determine the right border of absolute dullness of the heart, a finger-pessimeter is placed on the right border of relative dullness of the heart parallel to the right edge of the sternum and, applying a quiet percussion blow, it is gradually moved inward until an absolutely dull sound appears. At this point, a mark is made along the outer edge of the finger, facing the border of relative dullness. Normally, the right border of absolute cardiac dullness runs along the left edge of the sternum.
When determining the left border of absolute dullness of the heart, the pessimeter finger is placed parallel to the left border of relative dullness, slightly moving outward from it. A quiet percussion blow is applied, gradually moving the finger inward until a dull sound appears. The left border of absolute cardiac dullness is drawn along the outer edge of the pessimeter finger. Normally, it is located in the 5th intercostal space and is displaced medially from the left midclavicular line by 1.5-2 cm.
To establish the upper limit of the absolute dullness of the heart, a finger-pessimeter is placed on the upper limit of the relative dullness of the heart at the edge of the sternum parallel to the ribs and, performing quiet percussion, go down until a dull sound appears (in order to better differentiate the percussion sound, percussion begins at the 1st intercostal space above the relative dullness) . The upper limit of absolute dullness is marked along the edge of the finger facing upward. Normally, it is located on the IV rib along the left parasternal line.
Sometimes it is difficult to distinguish absolute dullness from relative dullness (if you percussion from the lungs to the heart). In such cases, the pessimeter finger is placed in the center of absolute dullness, and then it is moved towards the boundaries of relative dullness (i.e., from dull to dull sound). The first addition of a pulmonary tone to the percussion sound will indicate a transition from the area of absolute dullness to the area of relative dullness. In this case, it is advisable to use the quietest percussion: the plessimeter finger is placed on the percussed surface not straight, but bent at a right angle at the first interphalangeal joint. Place it perpendicular to the percussed area and make very quiet blows at the bend with the percussing finger of the right hand. Normally, the entire area of absolute cardiac dullness is formed by the anterior surface of the right ventricle.
The boundaries of the vascular bundle are determined in the second intercostal space as follows. The pessimeter finger is placed on the second intercostal space on the right along the midclavicular line parallel to the expected dullness and, quietly percussing, it is gradually moved inward towards the sternum until a dull sound appears. The boundaries are marked along the outer edge of the finger, facing the clear percussion sound. Then, in the same way, quiet percussion is performed on the left. A mark is also made along the outer edge of the pessimeter finger. Normally, the diameter of the vascular bundle is 4.5-6 cm.
The vascular bundle is formed by the superior vena cava and the aortic arch on the right, and the pulmonary artery on the left.
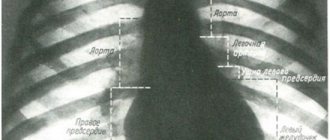
Normal contours of the heart. The right contour of the relative dullness of the heart in the II and III intercostal spaces is formed by the superior vena cava; in IV—right atrium. The left contour in the II intercostal space from above is the left part of the aortic arch, then the trunk of the pulmonary artery, at the level of the III rib is the appendage of the left atrium, and down to the IV-V rib is a narrow strip of the left ventricle. The anterior surface of the heart is formed by the right ventricle.
Auscultation of the heart. When listening to the heart, it is necessary to follow general and specific rules. The general rules are the same as when listening to the lungs. The private rules are as follows.
The doctor is positioned on the right side of the patient so that the phonendoscope (stethoscope) can be freely and correctly applied to the listening areas.
Listening is performed in the horizontal (lying on the back, on the left side) and vertical (if the condition allows) positions of the patient. This makes it possible to better listen to sound phenomena occurring in the heart with various valve defects.
To eliminate sound phenomena from the lungs, which can distort the examination result, the patient must hold his breath during auscultation. However, he cannot do this for long; the procedure has to be repeated.
Sometimes heart sounds change dramatically after physical activity. Therefore, during auscultation, the patient (if his condition allows) is asked to do several squats, climb the stairs, walk around the office, ward, etc. This often helps to detect changes in the sound phenomena of the heart that are important for diagnostic purposes.
The heart should not be listened to hastily. With a hasty examination, it is rarely possible to obtain a reliable auscultatory picture. However, too long auscultation leads to hearing fatigue and reduced listening efficiency. Listening should be done with periodic pauses, which gives the optimal effect.
The first stage of listening should always be analytical, dividing auscultatory symptoms into fragments. First, you need to focus on the heart sounds (on the first, then on the second), then on the systolic and finally on the diastolic pauses. Based on the data obtained, it is necessary to give a comprehensive assessment of the heart melody.
The places of best detection of heart sounds - tones, as well as murmurs - do not always coincide with the anatomical localization of their sources - valves and the openings they close. Thus, the mitral valve is projected at the site of attachment of the third rib to the sternum on the left; aortic - in the middle of the sternum at the level of the third costal cartilage; pulmonary artery—in the second intercostal space on the left at the edge of the sternum; tricuspid valve - in the middle of the line connecting the places of attachment to the sternum of the cartilages of the third left and fifth right ribs. Such proximity of the valve openings to each other makes it difficult to isolate sound phenomena at the place of their true projection onto the chest. In this regard, the locations of the best conduction of sound phenomena from each of the valves have been determined.
The place for listening to the bicuspid valve is the area of the apical impulse, i.e., the 5th intercostal space at a distance of 1-1.5 cm inward from the left midclavicular line; aortic valve—II intercostal space on the right at the edge of the sternum, as well as the 5th Botkin-Erb point (place of attachment of the III—IV rib to the left edge of the sternum; a); pulmonary valve—II intercostal space on the left at the edge of the sternum; tricuspid valve - the lower third of the sternum, at the base of the xiphoid process.
Listening is carried out in a certain sequence: the area of the apical impulse, the second intercostal space on the right at the edge of the sternum; II intercostal space on the left at the edge of the sternum; lower third of the sternum (at the base of the xiphoid process); Botkin-Erb point. This sequence is due to the frequency of damage to the heart valves.
In practically healthy individuals, when listening to the heart, two tones are usually detected - the first and second, sometimes the third (physiological) and even the fourth.
The first tone is the sum of sound phenomena occurring in the heart during systole. That's why it's called systolic. It occurs as a result of vibrations of the tense muscle of the ventricles (muscular component), closed leaflets of the bicuspid and tricuspid valves (valve component), the walls of the aorta and pulmonary artery during the initial period of blood entering them from the ventricles (vascular component), the atria during their contraction (atrial component).
The second tone is caused by the slamming and resulting vibrations of the aortic and pulmonary artery valves. Its appearance coincides with the beginning of diastole. That's why it's called diastolic. Between the first and second tones there is a short pause (no sound phenomena are heard), and the second tone is followed by a long pause, after which the tone appears again. However, students beginning their studies often have great difficulty distinguishing between the first and second tones. To make this task easier, it is recommended to first listen to healthy people with slow heart rates. Normally, the first sound is heard louder at the apex of the heart and in the lower part of the sternum. This is explained by the fact that sound phenomena from the mitral valve are better transmitted to the apex of the heart and the systolic tension of the left ventricle is more pronounced than that of the right. The second tone is heard louder at the base of the heart (at the sites where the aorta and pulmonary artery are heard. The first tone is longer and lower than the second.
A change in heart sounds can primarily be expressed in a weakening or strengthening of the sonority of one or both of them, in a change in timbre, duration, in their splitting or bifurcation, in some cases - in the appearance of additional tones. In this case, determining the place of best listening to pathological sound phenomena is of diagnostic importance. Strengthening the second tone in the second intercostal space on the left indicates its emphasis on the pulmonary artery (determined by comparing its volume and timbre on the pulmonary artery and aorta). This indicates an increase in pressure in the pulmonary circulation, which can be observed in diseases of the heart, as well as the respiratory system (mitral defects, emphysema, pneumosclerosis, chronic pneumonia). The intensification of the second tone in the second intercostal space on the right indicates its emphasis on the aorta, which is observed with an increase in blood pressure in the systemic circulation (arterial hypertension), as well as in the case of hardening of the wall and valve of the aorta in atherosclerosis and a number of other diseases.
Strengthening the first sound at the apex of the heart most often occurs with narrowing of the left atrioventricular orifice (mitral stenosis), tachycardia. This is due to the fact that with this defect, during diastole, less blood flows into the left ventricle than normal, and it contracts more quickly (transition from a relaxed to a tense state). In addition, with mitral stenosis, the timbre of the first tone changes due to vibrations of the sclerotic cusps of the mitral valve. It takes on a crackling tone, reminiscent of the sound of a flag flapping in the wind. This sound at the apex of the heart with mitral stenosis is called “popping”.
Weakening of the first tone at the apex of the heart can be observed during inflammatory processes of its muscle (myocarditis), cardiosclerosis (scar changes in the heart muscle), and damage to the valve apparatus (bicuspid and tricuspid, as well as aortic).
Weakening of the second sound in the aorta is possible with aortic defects (aortic valve insufficiency or stenosis of its mouth).
Weakening of the second sound in the pulmonary artery occurs when the valve is insufficient or its mouth is narrowed (stenosis).
If during auscultation of the heart, instead of one of the tones, two short ones are heard, following each other after a short period of time, then this indicates a split tone. If the difference in the time of occurrence of these components is insignificant and the impression of splitting is not created, we are talking about splitting the tone. Thus, there is no fundamental qualitative difference between bifurcation and splitting of tones. There is only some quantitative difference: splitting is the initial phase, and bifurcation is a more pronounced degree of disruption of the unity of tones.
Bifurcation and splitting of tones can be physiological and pathological.
In case of severe heart damage, a three-part rhythm can be heard. It is caused by weakening of the myocardium (inflammation, degenerative changes, toxic lesions) of the left ventricle and occurs as a result of rapid stretching of its walls under the pressure of blood flowing from the atrium. This creates a melody of a three-part rhythm (first, second and additional third tones), reminiscent of the clatter of a galloping horse—the “gallop rhythm.” It is also figuratively called the “cry of the heart for help,” since it is a sign of severe heart damage. The rhythm of the gallop is best heard directly by the ear (along with the sound, a slight impulse is perceived, transmitted from the heart to the chest in the diastole phase) in the area of the apex of the heart or the third-fourth intercostal space on the left. It can be heard especially clearly when the patient is lying on his left side. But this creates inconvenience for direct listening with the ear. In such cases, a phonendoscope is used.
Much more common are bifurcation and splitting of the second tone, caused by non-simultaneous closure of the pulmonary artery and aortic valves due to increased pressure in the pulmonary or systemic circulation. Bifurcation and splitting of the second tone can also be physiological and pathological.
Physiological splitting of the second tone is heard exclusively at the base of the heart during inhalation and exhalation or during physical activity. At the end of a deep inhalation, when the chest expands due to a decrease in pressure in it, the blood is somewhat retained in the dilated vessels of the small circle and therefore flows in smaller quantities into the left atrium, and from there into the left ventricle. The latter, due to less blood filling, ends systole earlier than the right one, and the closure of the aortic valve precedes the closure of the pulmonary valve. During exhalation, the opposite conditions are created. In the case of increased pressure in the chest, blood, as if squeezed out of the vessels of the pulmonary circle, enters in large quantities into the left part of the heart, and the systole of the left ventricle, and therefore the beginning of its diastole, occurs later than the right.
At the same time, a split second tone may be a sign of serious pathological changes in the heart and its valves. Thus, a bifurcation of the second sound at the base of the heart (second intercostal space on the left) is heard with mitral stenosis. This is due to the fact that the hypertrophied and blood-filled right ventricle ends systole later than the left. Therefore, the aortic component of the second sound occurs earlier than the pulmonary one. Bifurcation or splitting of the second sound in bicuspid valve insufficiency is associated with greater blood filling of the left ventricle than normal, which leads to prolongation of its systole, and the diastole of the left ventricle begins later than the right. Because of this, the aortic valve closes later than the pulmonary valve.
One should distinguish from the true splitting of the second tone its sound melody, which only superficially resembles splitting. An example is the additional tone that occurs during the opening of the bicuspid (mitral) valve with mitral stenosis. It has a high clicking timbre and is perceived as a loud echo following the second tone. The additional tone, together with the clapping first and second, form a peculiar melody, reminiscent of the cry of a quail. Hence the name of this sound phenomenon, heard during mitral stenosis at the apex of the heart, “quail rhythm.” Its distribution area is extensive - from the apex of the heart up and into the axillary fossa.
Sometimes, when listening to the heart, against the background of rare and dull tones, a lonely, very loud tone appears, the so-called “cannon tone” of Strazhesko. It is caused by the simultaneous contraction of the atria and ventricles, which is observed with complete atrioventricular block, i.e. when impulses from the atria do not reach the ventricles and they each contract in their own rhythm (the atria contract more often), but in some cycle their contractions coincide.
In pathology, and sometimes in healthy people, in addition to heart sounds, auscultation of the heart makes it possible to detect other sound phenomena called murmurs. They occur when the opening through which blood flows narrows and the speed of blood flow increases. Such phenomena may be caused by an increase in heart rate or a decrease in blood viscosity.
Heart murmurs are divided into murmurs that occur inside the heart itself (intracardiac) and murmurs that occur outside the heart (extracardiac, or extracardiac).
Intracardiac murmurs most often arise as a result of damage to the heart valves, when their valves are not completely closed during the closure of the corresponding hole, or when the lumen of the latter narrows. They can also be caused by damage to the heart muscle.
Intracardiac murmurs can be organic or inorganic. The first ones are most important from a diagnostic point of view. They indicate anatomical lesions of the heart valves or the openings they close.
The noise that occurs during systole, that is, between the first and second sound, is called systolic, and during diastole, that is, between the second and the next first sound, it is called diastolic. Consequently, the systolic murmur coincides in time with the apical impulse and the pulse in the carotid artery, and the diastolic murmur coincides with the long pause of the heart.
It is better to start learning the technique of listening to murmurs with systolic (with normal heart rhythm). These noises can be soft, blowing, rough, scraping, musical, short and long, quiet and loud. The intensity of any of them can gradually decrease or increase. Accordingly, they are called decreasing or increasing. Systolic murmurs are usually decreasing. They can be heard during all or part of systole.
Listening to a diastolic murmur requires special skill and attention. This noise is much weaker in volume than systolic and has a low timbre, difficult to hear with tachycardia (heart rate more than 90 per minute) and atrial fibrillation (random contractions of the heart). In the latter case, long pauses between individual systoles should be used to listen to the diastolic murmur. Diastolic murmur, depending on what phase of diastole it occurs, is divided into three types: protodiastolic (decreasing; occurs at the very beginning of diastole, immediately after the second sound), mesodiastolic (decreasing; appears in the middle of diastole, somewhat later after the second sound) and presystolic (increasing; formed at the end of diastole before the first sound). Diastolic murmur may last throughout diastole.
Organic intracardiac murmur caused by acquired heart defects can be systolic (with insufficiency of the bicuspid and tricuspid valves, narrowing of the aortic mouth) and diastolic (with narrowing of the left and right atrioventricular orifices, insufficiency of the aortic valve). A type of diastolic murmur is presystolic murmur. It occurs with mitral stenosis due to increased blood flow through the narrowed opening at the end of diastole during contraction of the left atrium. If two murmurs (systolic and diastolic) are heard above one of the valves or orifices, this indicates a combined defect, i.e., valve insufficiency and narrowing of the orifice.
The localization of any noise corresponds to the place of best auscultation of the valve in the area in which the noise originated. However, it can be carried out through the blood flow and through the dense heart muscle during its contraction.
Systolic murmur due to bicuspid valve insufficiency is best heard at the apex of the heart. It is carried out towards the left atrium (II-III intercostal space on the left) and into the axillary region. This noise becomes clearer when holding the breath during the exhalation phase and when the patient is lying down, especially on the left side, as well as after physical activity.
Systolic murmur with tricuspid valve insufficiency can be heard well at the base of the xiphoid process of the sternum. From here it is carried up and to the right, towards the right atrium. This noise is better heard when the patient is positioned on the right side while holding the breath at the height of inspiration.
Systolic murmur with narrowing of the aortic mouth is best heard in the second intercostal space to the right of the sternum, as well as in the interscapular space. It, as a rule, has a sawing, scraping character and is carried along the blood flow upward to the carotid arteries. This noise intensifies when the patient is lying on the right side with breath holding in the forced expiration phase.
Diastolic murmur with mitral stenosis, occurring at the beginning or middle of diastole, is often better heard in the area of the projection of the bicuspid valve (the place where the third rib attaches to the sternum on the left) than at the apex. Presystolic, on the contrary, is better heard in the apex region. It is carried out almost nowhere and is especially well heard in the vertical position of the patient, as well as after physical activity.
Diastolic murmur with aortic valve insufficiency is also heard in the second intercostal space to the right of the sternum and is carried along the blood flow down to the left ventricle. It is often better heard at the 5th Botkin-Erb point and intensifies when the patient is in an upright position.
Organic intracardiac murmurs, as already noted, can be the result of congenital heart defects (patent closure of the interatrial foramen ovale, ventricular septal defect - Tolochinov-Roger disease, patent ductus arteriosus, narrowing of the pulmonary artery).
When the interatrial foramen is not closed, systolic and dastolic murmurs are observed, the maximum audibility of which is detected in the area of attachment of the third rib to the sternum on the left.
With a ventricular septal defect, a grinding systolic murmur occurs. It is heard along the left edge of the sternum, at the level of the III-IV intercostal space and is carried into the interscapular space.
When the ductus arteriosus is patent (the aorta is connected to the pulmonary artery), a systolic murmur (sometimes with diastolic) is heard in the second intercostal space on the left. It is less audible over the aorta. This noise is carried out to the interscapular region closer to the spine and to the carotid arteries. Its peculiarity is that it is combined with an enhanced second sound on the pulmonary artery.
When the mouth of the pulmonary artery is narrowed, a rough systolic murmur is heard in the second intercostal space on the left at the edge of the sternum, which is little transmitted to other places; the second tone in this place is weakened or absent.
Murmurs may also occur as a result of dilatation of the heart chambers
In case of aortic valve insufficiency, a functional diastolic (presystolic) murmur—Flint's murmur—is often heard at the apex of the heart. It appears when the mitral valve leaflets are lifted by a strong stream of blood flowing from the aorta during diastole into the left ventricle, thereby causing a transient narrowing of the left atrioventricular orifice. Flint's murmur is heard at the apex of the heart. Its volume and duration are inconsistent.
Functional noises, as a rule, are heard in a limited area (best at the apex and more often on the pulmonary artery) and have a low volume and soft timbre. They are not constant and can appear and disappear with different body positions, after physical activity, and in different phases of breathing.
Extracardiac murmurs include pericardial friction rub and pleuropericardial murmur. Pericardial friction noise occurs during inflammatory processes in it. It is heard during both systole and diastole, is better detected in the area of absolute dullness of the heart and is not carried out anywhere. Pleuropericardial murmur occurs when there is inflammation in the area of the pleura adjacent to the heart. It resembles a pericardial friction noise, but unlike it, it intensifies during inhalation and exhalation, and when holding the breath it decreases or disappears altogether. A pleuropericardial murmur is heard along the left edge of the relative dullness of the heart.
Auscultation of blood vessels. When auscultating arteries close to the heart (carotid arteries), two quiet tones can be heard. One of them occurs as a result of tension in the arterial wall during ventricular systole. The second is carried out from the aortic valve leaflets when they close. When auscultating arteries located far from the heart, no sounds are heard.
With slight compression of large arteries, you can normally listen with a phonendoscope to the noise that occurs when blood passes through the narrowed lumen of the vessel. With stenosis of the aortic mouth, a systolic murmur is heard in the carotid arteries (without their compression). This is a conductive noise from the aorta.
With anemia, a systolic murmur is heard in large arteries without compressing them, which is explained by a decrease in blood viscosity, and therefore an increase in blood flow speed.
With thyrotoxicosis, the noise can be heard over the thyroid gland. It occurs as a result of increased blood flow with increased heart rate.
In case of insufficiency of the aortic valve on the femoral artery, when it is slightly compressed, using a phonendoscope or stethoscope, you can listen to the double Vinogradov-Durozier murmur - in the systole and diastole phase (the first is stronger). In addition, with this defect on the femoral and other large arteries, without compressing them, you can listen to the double Traube sound.
With anemia, a blowing or buzzing noise is sometimes heard on the jugular vein - “the sound of a top.” It intensifies with a deep breath or when turning the head in the opposite direction.
Heart Length
- the distance in centimeters from the right cardiovascular angle to the apex of the heart, i.e. to the left border of the relative dullness of the heart. It coincides with the anatomical axis of the heart and is normally 12-13 cm. To characterize the position of the heart, it is of known importance to determine the angle of inclination of the heart, enclosed between the anatomical axis of the heart and the anterior midline. Normally, this angle corresponds to 45-46°; in asthenics it increases.
Diameter of the heart
- the sum of 2 perpendiculars to the anterior midline from the points of the right and left boundaries of the relative dullness of the heart. Normally, it is 11 - 13 cm ± 1 - 1.5 cm, adjusted for constitution - in asthenics it decreases (“hanging”, “drip” heart), in hypersthenics it increases (“lying” heart).
Heart width
- the sum of 2 perpendiculars lowered onto the length of the heart: the first - from the point of the upper border of the relative dullness of the heart, the second - from the apex of the cardiohepatic angle formed by the right border of the relative dullness of the heart and the liver (practically - V intercostal space, at the right edge of the sternum). Normally, the width of the heart is 10-10.5 cm.
Heart height
- the distance from the point of the upper limit of the relative dullness of the heart to the base of the xiphoid process (first segment) and from the base of the xiphoid process to the lower contour of the heart (second segment). However, due to the fact that the lower contour of the heart is almost impossible to determine by percussion due to the adjacency of the liver and stomach, it is believed that the second segment is equal to one third of the first, and the sum of both segments normally averages 9-9.5 cm.
Oblique heart size
(quercus) is determined from the right border of the relative dullness of the heart (right atrium) to the upper border of the relative dullness of the heart (left atrium), normally equal to 9-11 cm.
Vascular bundle width
determined by the second intercostal space, normally 5-6 cm.
Determination of heart configuration.
There are normal, mitral, aortic and trapezoidal configurations of the heart with a wide base. With a normal configuration of the heart, the dimensions of the heart and cardiovascular bundle are not changed, the waist of the heart along the left contour represents an obtuse angle.
The mitral configuration of the heart is characterized by smoothness and even bulging of the waist of the heart along the left contour due to hypertrophy and dilatation of the left atrium, which is characteristic of mitral heart defects. In this case, in the presence of isolated mitral stenosis, the boundaries of the relative dullness of the heart expand upward and to the right due to an increase in the left atrium and right ventricle, and in the case of mitral valve insufficiency - upward and to the left due to hypertrophy of the left atrium and left ventricle.
The aortic configuration of the heart is observed with aortic defects and is characterized by an outward and downward displacement of the left border of the relative dullness of the heart due to an increase in the size of the left ventricle without changing the left atrium. In this regard, the waist of the heart along the left contour is emphasized, approaching a right angle. The length and diameter of the heart increase without changing its vertical dimensions. This configuration of the heart is traditionally compared to the outline of a duck sitting on the water.
The configuration of the heart in the form of a trapezoid with a wide base is observed due to the accumulation of a large amount of fluid in the pericardial cavity (hydropericardium, exudative pericarditis), while the diameter of the heart increases significantly. Severe cardiomegaly with enlargement of all chambers of the heart - “bull heart” (cor bovinum) - is observed with decompensation of complex heart defects, dilated cardiomyopathy.
Special pathological forms of the heart
Special pathological forms of the heart include pulmonary and bovine.
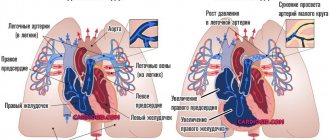
Pulmonary heart
With cor pulmonale, the load on the right side increases, which leads to dilation of the atrium and ventricle. The X-ray shows an expansion of the shadow to the right (2nd arc) and a displacement of the left contour due to the large right ventricle, a mitral configuration appears.
Chronic diseases of the bronchi and lungs, which last for several years, are accompanied by cor pulmonale in 25% of cases. It can also occur acutely when the chest and diaphragm are damaged within a few hours.
If the patient is severely obese, then excess fat raises the diaphragmatic dome upward, which makes breathing difficult and causes changes in the heart shadow. Subacute cor pulmonale (develops up to 3-7 days) occurs when a pulmonary artery is blocked by a blood clot, severe pneumonia, tumor metastases, poliomyelitis, muscle weakness (myasthenia gravis).
Bull's heart
Enlargement of the chambers of the heart (dilated cardiomyopathy) or thickening of the heart muscle (hypertrophic cardiomegaly) leads to the fact that the cardiac shadow increases in all directions and a “large” or “bull” heart is formed.
Its configuration will be close to trapezoidal or spherical, less often the waist will be preserved.
The causes of large heart syndrome may be:
- atherosclerosis, angina pectoris, heart attack and its complications: aneurysm, post-infarction cardiosclerosis;
- vices;
- hypertonic disease;
- inflammation of the myocardium, immune or due to rheumatism, bacterial, viral, fungal infections;
- cardiomyopathy due to alcoholism, contact with chemicals, metals, industrial dust;
- severe hypovitaminosis, nutritional deficiency, especially lack of protein, when the heart muscle is weakened and stretched.
The expansion of the chambers of the heart leads to poor circulation, stagnation of blood in the lungs, edema, and enlargement of the liver.
We recommend reading the article about x-rays of the heart. From it you will learn what an x-ray of the heart shows, why x-rays are needed in three projections, with contrast of the esophagus, as well as how to prepare for x-rays of the heart and what the results will tell you. And here is more information about the structure of the human heart.
The configuration of the heart can be normal: 2 arches on the right, 4 on the left, there is a waist. With defects of the heart, large vessels, diseases of the lungs, myocardium, a mitral, aortic, trapezoidal shape appears, and pulmonary and “bull” hearts can be detected on an x-ray. Just a change in configuration does not indicate the presence of a disease.
Determination of the boundaries of absolute cardiac dullness
Absolute dullness of the heart is the part of the heart not covered by the edges of the lungs, adjacent directly to the anterior wall of the chest and giving an absolutely dull sound upon percussion. Absolute cardiac dullness is formed by the anterior surface of the right ventricle. To determine the boundaries of absolute dullness of the heart, the quietest, or threshold, percussion is used. There are right, top and left borders. The determination is carried out according to the general rules of topographic percussion from the boundaries of relative dullness of the heart (right, upper, left) towards the zone of absolute dullness. The right border of absolute cardiac dullness runs along the left edge of the sternum; upper - along the lower edge of the IV rib; left - 1 cm medially from the left border of the relative dullness of the heart or coincides with it.
Norm and deviations in readings
Data obtained during physical diagnostic methods, which include inspection, palpation, percussion and auscultation, should only be assessed by a doctor in combination with a survey and other diagnostic methods.
Percussion of absolute dullness of the heart
Narrowing of the boundaries, as a rule, is not associated with heart pathologies; it occurs with emphysema, pneumothorax and a low position of the diaphragm in thin patients. The boundaries have been expanded for the following diseases:
- mitral stenosis,
- pulmonary heart,
- tricuspid valve insufficiency,
- mediastinal tumors,
- cicatricial changes along the edges of the lungs.
Deviations from the norm of relative dullness of the heart
If the right border is shifted to the right, then this is evidence of mitral or pulmonary stenosis, accumulation of fluid or air in the chest.
A shift to the left is possible with asthenia, emaciation, right-sided pneumo- or hydrothorax.
Shift of the left OTS line more often occurs to the left side in the following diseases:
- aortic insufficiency,
- non-closure of the mitral valve,
- decompensated aortic stenosis,
- hypertension,
- acute myocardial ischemia,
- circulatory failure,
- high position of the diaphragm due to flatulence, obesity.
Auscultation of adults and children
Heart sounds are heard during the movement of vascular walls, valves, and blood flow during myocardial contractions. The norm is to listen to the first and second tones.
The first is the systolic tone. It includes the following components:
- valvular - closing of the valves between the atria and ventricles;
- muscular - contraction of the cardiac muscle of the ventricles;
- vascular – passage of blood into large vessels;
- atrial – pushing blood into the ventricles.
The second sound is diastolic, it is heard when the valves of the aorta and pulmonary artery close and the subsequent flow of blood through them.
The third tone occurs in adolescents and patients with malnutrition. It is caused by the movement of the ventricles during the phase of their filling and diastolic relaxation. The fourth sound is also diastolic and is heard before the first, when the chambers of the heart are completely filled with blood.
Tones are weakened in myocarditis, myocardial dystrophy. The first tone weakens with mitral and aortic insufficiency, narrowing of the aorta.
Strengthening 1 tone is associated with the formation of a cavity inside the lung with tuberculosis, pneumothorax, as well as mitral and tricuspid stenosis, tachycardia.
The second tone becomes muffled when the valves are not closed, since its valve part is missing, and there is low arterial and pulmonary pressure. Strengthening of the 2nd tone occurs with arterial hypertension over the aorta, and pathology of the mitral valve leads to an accentuation of the 2nd tone over the pulmonary trunk.
Auscultation of the heart
Cardiac auscultation is the most valuable method for examining the heart. During the work of the heart, sound phenomena occur, which are called heart sounds. Analysis of these tones by auscultation or graphic recording (phonocardiography) gives an idea of the functional state of the heart as a whole, the functioning of the valve apparatus, and the activity of the myocardium. The objectives of cardiac auscultation are: 1) determination of heart sounds and their characteristics: a) strength; b) solidity; c) timbre; d) rhythm; e) frequency; 2) determination of the number of heart contractions (based on the frequency of sounds); 3) determination of the presence or absence of noise with a description of their main properties.
When performing cardiac auscultation, the following rules are observed. 1. The doctor’s position is opposite or to the right of the patient, which makes it possible to freely listen to all the necessary auscultation points. 2. Position of the patient: a) vertical; b) horizontal, lying on your back; c) on the left, sometimes on the right side. 3. Certain techniques for auscultation of the heart are used: a) listening after dosed physical activity, if the patient’s condition allows; b) listening in different phases of breathing, as well as when holding the breath after maximum inhalation or exhalation. The specified provisions and techniques are used to create conditions for amplification of noise and their differential diagnosis, which will be discussed below.