The heart is a muscular hollow organ of the circulatory system that performs a pumping function. It is located in the chest in the mediastinal cavity. The organ is adjacent to numerous veins, arteries and lymphatic vessels, borders the esophagus, stomach, left hepatic lobe and both lungs. The place where the human heart is located is called the pericardium. This is a membrane (a two-layer “bag”) surrounding the organ and the mouths of large blood vessels.
General description of the anatomy of the chest
The chest is where the heart is located in humans, mammals and birds. This is the musculoskeletal reservoir of all organs responsible for breathing and blood circulation. Also located in the chest is the esophagus and a number of large arteries and veins of the body. The chest itself is formed by the vertebral column, costal arches and sternum. It communicates with other cavities and areas of the body and provides mechanical protection to the vital organs of the body.
Whole chest and its cavities
Due to the attachment of the ribs by cartilage to the sternum, the cell is formed as a closed osteochondral container. Due to the intercostal muscles, external and internal fascia, as well as the muscle-tendon diaphragm, a closed chest cavity is formed. It has several openings: the superior aperture, the esophageal opening, the aortic opening of the diaphragm, and the opening of the inferior vena cava. The chest cavity itself contains a number of vital enclosed spaces: the mediastinum (the place where the heart is located), the pericardial cavity, and the pleural cavities surrounding the lungs.
Projection of the heart onto the chest
The place where the human heart is located is called the mediastinum. Here is the pericardium, which contains the heart with the mouths of the main blood vessels. In this case, the heart has three borders, which are projected onto the chest. Their change makes it possible to determine deviations from the norm and specific physical symptoms of organic heart lesions. Normally, the heart is located to the left of the sternum from the third intercostal space to the fifth intercostal space. The right ventricle of the heart is turned slightly forward. The direction of the longitudinal axis of the heart from the basal (upper) sections to the lower (apical) is as follows: the heart is oriented from top to bottom, from back to front, from right to left.
Projection of the borders of the heart onto the chest
The upper border of the heart is located at the level of the upper edges of the third right and left costal cartilages.
The lower border goes from the lower edge of the body of the sternum and the cartilage of the right rib to the apex of the heart.
The apex of the heart is located in the left intercostal space 1.5 cm medially from the midclavicular line.
The left border of the heart looks like a convex line running from top to bottom in an oblique direction: from the upper edge of the third (left) rib to the apex of the heart.
The one who says that the heart is on the left side will not be entirely right. Sometimes the muscular organ is located in the right chest area. But not only doctors are required to know where this organ is usually located. Each individual should be aware of their anatomical features
.
Boundaries of the heart
The right cardiac border is determined by percussion and is located 1 cm to the right of the right edge of the sternum along the fourth intercostal space. The left border corresponds to the apical impulse: 1.5 cm to the left of the left midclavicular line. The upper border, corresponding to the entire width of the vascular bundle, is located in the third intercostal space. By connecting the point of the extreme right and extreme left borders with the extreme points of the width of the vascular bundle, the basic configuration of the pericardium is determined. This is the projection of the place where a person’s heart is located.
Online consultations with doctorsAll about coronavirus
October 18, 2020, 7:27 pm doctor001 · October 18, 2020, 7:27 pm Thank Reply
Hello!
ARVI is a viral disease and most often proceeds without any complications at all and ends with recovery! But depending on the state of a person’s immunity, the treatment being carried out and many other factors, complications can sometimes arise in various organs and systems! PULMONARY COMPLICATIONS OF ARVI. 1. Primary viral (influenza) pneumonia - develops in the first 24-72 hours from the onset of the disease (on days 1-3 it occurs as acute hemorrhagic toxic pulmonary edema, from days 4-6 as polysegmental, often bilateral pneumonia, which is based on ARDS ). 2. Late viral-bacterial pneumonia - signs of involvement of the lung parenchyma appear 5-6 days or later from the onset of the influenza clinic. 3. Acute laryngotracheitis with laryngeal stenosis (false croup syndrome) is a rapidly developing (over hours or days) breathing difficulty associated with a narrowing of the lumen of the larynx. Three leading symptoms are characteristic: a change in the timbre of the voice, a rough “barking cough”, and sonorous difficulty breathing (stenotic breathing). B. EXTRAPULMONARY COMPLICATIONS OF ARVI: 1. Myositis - sharp muscle pain that appears at the height of the flu clinic; Severe rhabdomyolysis can lead to the development of renal failure. It is necessary to differentiate influenza myositis from acute muscle pain in staphylococcal sepsis. 2. Cardiac complications – myocarditis, less often pericarditis; Patients with chronic cardiac pathology may experience rhythm disturbances and progression of congestive heart failure. 3. Acute toxic encephalopathy - observed rarely, more often in children, is the result of microcirculation disorders in the vessels of the brain with the formation of multiple ischemic and hemorrhagic lesions. It is characterized by high mortality and the formation of severe neurological deficits in survivors. 4. Guillain-Barré syndrome is a form of acute inflammatory polyradiculoneuropathy, manifested by flaccid paresis, sensory disturbances and autonomic disorders. It develops as a complication of a wide variety of viral infections, including influenza, and, extremely rarely, vaccinations. It is based on the development of autoimmune processes. 5. Reye's syndrome (Reyo) is a rare pathology of the liver and central nervous system with high mortality. Most often, Reye's syndrome develops in children and adolescents against the background of influenza and chickenpox when treated with acetylsalicylic acid. In this regard, drugs containing salicylates should not be prescribed to relieve fever in this age group. 6. Acute otitis media, sinusitis, bronchitis, occurring against the background of an acute respiratory viral infection. The etiological factors are not only viruses, but also many bacterial agents - Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, Streptococcus pyogenes, Moraxella catarrhalis, less often chlamydia and mycoplasma. Properly initiated treatment, prevention and timely treatment in the case of a secondary bacterial infection almost always allows for recovery! Good luck to you ! Thank Reply
The concept of the mediastinum
The mediastinum is the place where the human heart is located. This is a limited cavity that includes all the organs located between both lungs. The anterior border of the cavity is the intrathoracic fascia and the sternum, the posterior border is the neck of the ribs, the prevertebral fascia and the thoracic spinal column. The lower wall is the diaphragm, and the upper wall is a collection of fascial sheets connected to form a suprapleural membrane. The lateral walls of the mediastinum are areas of the parietal pleura and intrathoracic fascia. Also, for the convenience of studying the elements located here, the mediastinum is conventionally divided into upper and lower. The latter is divided into posterior, central and anterior mediastinum. The place where the human heart is located is the lower central mediastinum.
Syntopy of the heart
Syntopy is a topographical concept that reflects the proximity of a certain organ to other anatomical formations. It is advisable to disassemble it along with the location of the mediastinal organs. So, the heart is not directly adjacent to any of the anatomical structures, except the pericardium and blood vessels. But the outer pericardial layer, by which the organ is separated from the rest of the anatomical formations, is adjacent to them. Anterior to the pericardium are the anteromedial, prepericardial, intrathoracic lymph nodes and vessels, surrounded by fatty tissue. At the back, the pericardium and the heart are bordered by the esophagus, azygos and semi-gypsy veins, the aorta, the vagus nerve, the sympathetic trunk and the thoracic lymphatic duct.
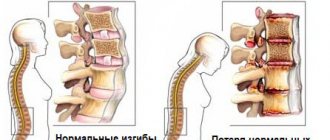
The diaphragm is the second heart
You can only fill an empty cup. Striving for knowledge, always remember: A person’s consciousness is a cup, And knowledge is the desired water. Funakoshi Gichin * * * * * Many people like heart disease. They strive for them. But there are people who don't like heart attacks. It is for them that I write. And for myself, of course. * * * * * The heart is a pump that pumps blood throughout the body. The heart is located in the center of the chest. First, it supplies blood to the right and left - to the lungs, to both halves. Pumping blood through the lungs, the heart receives oxygenated scarlet blood. He leaves as much as necessary for his own needs, and supplies the rest of the scarlet blood to all organs, throughout the body. The heart pumps red blood into the organs through the arteries. And blood returns to the heart through the venous system (blue blood) and through the lymphatic system (light liquid). It is supplied through one pipe and returned through two pipes. Like any pump, the heart pumps well, but sucks poorly. The country pump easily lifts water to the tenth floor - 30m, but only sucks from 6 - 7 meters. Blue blood and lymph flow in only one direction - towards the heart. For this purpose, many valves (check valves) are installed on the vessels. The veins and lymph vessels of the heart itself are especially important. Blue blood flows through small veins and collects in a large vein - the inferior vena cava and the superior vena cava. They are as thick as a water pipe, but the walls are thin. When the diaphragm moves (inhale-exhale), the vena cava contracts and unclenches, and blood is energetically pumped to the heart. Few people know this. It’s about the same with lymph. They even say that the diaphragm plays a major role in the movement of lymph. The diaphragm not only “breathes”, but also “pumps”. When a person with a large belly (fat or pregnancy) lies on his back, the heavy belly compresses the vena cava, and the “heart” becomes heavy, arrhythmia, shortness of breath. This is, in brief, in general terms, the mechanics of blood circulation. All necessary information is mentioned here, and unnecessary information is omitted. All that remains is to think about it and apply it. * * * * * The ease of pumping blood throughout the body, of course, also depends on other conditions. For example, from the thickness of the blood. The blood thickens from sugar, from grub, and her heart pumps with difficulty. I drank a glass of water, the blood became thinner and flowed through my veins more easily. You can also take pills to thin your blood. It's more luxurious. But this is for aristocrats, for gentlemen. But we are from peasants, from comrades, and we like health and longevity more than chic. Therefore, water is more reliable for us. Or else, he raised his hands up while sitting at the computer, and the flow of venous blood to the heart increased. And it’s easier for the heart. Do you feel it? * * * * * The power of the diaphragm, as a pump for blue blood and lymph, is comparable to the power of the heart, and perhaps even exceeds it. Therefore, if the diaphragm is weak, then the heart is overloaded, and problems are inevitable. The heart works independently, and the work of the diaphragm is adjusted by consciousness. In a healthy body, the rhythm of movement of the diaphragm is usually consistent with the rhythm of the heartbeat. For example, for one breath (inhale-exhale) there are four heartbeats. The diaphragm is the second heart. This knowledge is secret and must be treated with care. * * * * * On the topic of “diaphragm” there is still a question of how to learn to breathe with the diaphragm. But to do this you need to have an idea of how to use attention. See related articles.
The heart, cor, is located in the chest cavity as part of the organs of the middle mediastinum; The apex of the heart, apex cordis, is directed downwards, to the left and forward, and the wider base of the heart, basis cordis, is directed upwards and backwards.
The sternocostal (anterior) surface of the heart, fdcies sternocostalis (anterior), faces the posterior surface of the sternum and ribs; the lower one is adjacent to the diaphragm and is called the diaphragmatic surface, fdcies diaphragmdtica (inferior). The lateral surfaces of the heart face the lungs, each of them is called pulmonary, fdcies pulmondlis.
On the surface of the heart there is a transversely located coronary groove, sulcus corondrius, which is the boundary between the atria and ventricles. In front, the groove is covered by the pulmonary trunk and the ascending aorta, behind which the atria are located. On the anterior, sternocostal, surface of the heart, the anterior interventricular groove (heart), sulcus interventriculdris anterior, is visible, and on the bottom - the posterior (lower) interventricular groove (heart), sulcus interventriculdris posterior. The longitudinal anterior interventricular groove divides the sternocostal surface of the heart into the right part, corresponding to the right ventricle, and the smaller left part, belonging to the left ventricle. The posterior (lower) interventricular groove begins on the posterior surface of the heart at the confluence of the coronary sinus into the right atrium, reaches the apex of the heart, where, with the help of the notch of the apex of the heart, incisura dpicis cordis, it connects with the anterior groove.
The heart consists of 4 chambers: two atria and two ventricles - right and left. The atria receive blood from the veins and push it into the ventricles; the ventricles eject blood into the arteries: the right one through the pulmonary trunk into the pulmonary arteries, and the left one into the aorta, from which numerous arteries extend to the organs and walls of the body. The right half of the heart contains venous blood, the left half contains arterial blood. They do not communicate with each other. Each atrium is connected to the corresponding ventricle by an atrioventricular orifice (right or left), each of which is closed by leaflet valves. The pulmonary trunk and aorta have semilunar valves at their origin.
The structure of the heart wall. The heart wall consists of 3 layers:
a thin inner layer is the endocardium, a thick muscular layer is the myocardium and a thin outer layer is the epicardium, which is the visceral layer of the serous membrane of the heart - the pericardium (pericardial sac).
Topography of the heart.
The upper border of the heart runs along the line connecting the upper edges of the right and left third costal cartilages. The right border descends from the level of the upper edge of the third right costal cartilage (1-2 cm to the right of the edge of the sternum) vertically down to the fifth right costal cartilage. The lower border is drawn along a line that runs from the fifth right costal cartilage to the apex of the heart; it is projected in the left fifth intercostal space 1.0-1.5 cm medially from the midclavicular line. The left border of the heart extends from the upper edge of the cartilage of the third left rib, starting at the level of the middle of the distance between the left edge of the sternum and the left midclavicular line, and continues to the apex of the heart.
X-ray anatomy of the heart. When examined with X-rays, the heart of a living person appears as an intense shadow located between the light lung fields. This shadow has the shape of an irregular triangle, the base of which faces the diaphragm. The shadow of the heart and its large vessels are also superimposed on the shadows of the organs. The contours of the shadow of the heart have a series of convexities called arcs. The smoothed superior arch is clearly visible on the right contour of the heart. The left contour of the heart forms 4 arches: a) lower; b) the arch of the protruding appendage of the left atrium; c) arch of the pulmonary trunk and d) superior arch.
Syntopy of the heart in the lower central mediastinum
The place where the human heart is as close as possible to other vital organs and vessels is called the lower central mediastinum. Here is the pericardial sac, which consists of two layers of mesothelium, between which there is a small cavity. Behind the visceral pericardial layer is the heart itself. Outside the pericardium are the roots of the lung: the pulmonary veins and arteries, the main bronchi located below the bifurcation of the trachea. The phrenic nerves and intrathoracic vessels with lymph nodes are also present here. As long as the main vessels (aorta, vena cava, pulmonary trunk and pulmonary veins) are covered by the pericardium, they are also located in the central mediastinum. Once they leave the pericardial sac, they are found in other areas of the mediastinum. All these anatomical features are extremely important, because they determine surgical tactics for chest injuries penetrating into its cavity, and during planned operations.
Rules for cardiac auscultation.
1. The heart must be listened to in various positions: lying down, standing, after physical activity (for example, after repeated squats).
2. It is better to listen to the heart while holding your breath after a deep inhalation and subsequent deep exhalation (so that breathing noises do not interfere). It is recommended to make commands while listening to each point: “Inhale and exhale,” “hold your breath.”
3. Auscultation of the heart must be carried out in strict sequence (from the 1st to the 5th points sequentially). The sound of the second tone must be compared at the 2nd and 3rd points of auscultation.
4. If any changes are detected at auscultation points, carefully listen to the entire area of the heart.
3. To improve auscultation of sound phenomena associated with mitral valve pathology, it is necessary to place the patient on the left side, when the apex of the heart approaches the chest wall; lesions of the aortic valve are better detected by auscultation of the patient in an upright position with arms crossed and raised above the head and in a lying position on the right side.
The heart is located asymmetrically in the anterior mediastinum. Most of it is to the left of the midline, leaving only the right atrium and both vena cavae on the right. The long axis of the heart is located obliquely from top to bottom, from right to left, from back to front, forming an angle of approximately 40 degrees with the axis of the entire body. In this case, the heart seems to be rotated in such a way that its right venous section lies more anteriorly, and the left arterial section lies more posteriorly.
The heart, together with the pericardium, in most of its anterior surface (facies sternocostalis) is covered by the lungs, the anterior edges of which, together with the corresponding parts of both pleurae, reaching in front of the heart, separate it from the anterior chest wall, with the exception of one place where the anterior surface of the heart, through the pericardium, is adjacent to the sternum and cartilages of the 5th and 6th ribs. The boundaries of the heart are projected onto the chest wall as follows. The impulse of the apex of the heart can be felt 1 cm medially from the linea mamillaris sinistra in the fifth left intercostal space. The upper limit of the cardiac projection is at the level of the upper edge of the third costal cartilages. The right border of the heart runs 2 - 3 cm to the right from the right edge of the sternum, from the III to V ribs; the lower border runs transversely from the fifth right costal cartilage to the apex of the heart, the left - from the cartilage of the third rib to the apex of the heart.
The ventricular outlets (aorta and pulmonary trunk) lie at the level of the third left costal cartilage; pulmonary trunk (ostium trunci pulmonalis) - at the sternal end of this cartilage, aorta (ostium aortae) - behind the sternum slightly to the right. Both ostia atrioventricularia are projected on a straight line running along the sternum from the third left to the fifth right intercostal space.
When auscultating the heart (listening to the sounds of the valves using a phonendoscope), the sounds of the heart valves are heard in certain places: mitral - at the apex of the heart; tricuspid - on the sternum on the right against the costal cartilage; tone of the aortic valves - at the edge of the sternum in the second intercostal space on the right; the tone of the pulmonary valves is in the second intercostal space to the left of the sternum.
X-ray anatomy of the heart. X-ray examination of the heart of a living person is carried out mainly by fluoroscopy of the chest in its various positions. Thanks to this, it is possible to examine the heart from all sides and get an idea of its shape, size and position, as well as the state of its parts (ventricles and atria) and the large vessels associated with them (aorta, pulmonary artery, vena cava).
The main position for the study is the anterior position of the subject (the course of the rays is sagittal, dorsoventral). In this position, two light pulmonary fields are visible, between which there is an intense dark, so-called median, shadow. It is formed by the shadows of the thoracic spinal column and sternum layered on top of each other and the heart, large vessels and organs of the posterior mediastinum located between them. However, this median shadow is considered only as a silhouette of the heart and large vessels, because the other mentioned formations (spine, sternum, etc.) usually do not appear within the cardiovascular shadow. The latter in normal cases, both on the right and on the left, extends beyond the edges of the spinal column and sternum, which become visible in the anterior position only in pathological cases (curvature of the spine, displacement of the cardiovascular shadow, etc.).
The named median shadow has the shape of a wide strip in the upper part, which expands downwards and to the left in the form of an irregular triangle, with the base facing downwards. The lateral contours of this shadow have the form of protrusions separated from each other by depressions. These projections are called arcs. They correspond to those parts of the heart and the large vessels associated with it that form the edges of the cardiovascular silhouette.
In the anterior position, the lateral contours of the cardiovascular shadow have two arcs on the right and four on the left. On the right contour, the lower arch is well grown, which corresponds to the right atrium; the upper, weakly convex arch is located medial to the lower and is formed by the ascending aorta and the superior vena cava. This arch is called the vascular arch. Above the vascular arch, another small arch is visible, heading upward and outward, towards the collarbone; it corresponds to the brachiocephalic vein. Below, the arch of the right atrium forms an acute angle with the diaphragm. In this angle, when the diaphragm is low at the height of a deep inspiration, it is possible to see a vertical shadow stripe, which corresponds to the inferior vena cava.
On the left contour, the uppermost (first) arch corresponds to the arch and the beginning of the descending aorta, the second to the pulmonary trunk, the third to the left ear and the fourth to the left ventricle. The left atrium, located for the most part on the posterior surface, is not edge-forming during the dorsoventral course of the rays and therefore is not visible in the anterior position. For the same reason, the right ventricle located on the anterior surface, which also merges below with the shadow of the liver and diaphragm, is not contoured. The place of transition of the left ventricular arch into the lower contour of the cardiac silhouette is marked radiographically as the apex of the heart.
In the area of the second and third arches, the left contour of the cardiac silhouette has the character of an indentation or interception, which is called the “waist” of the heart. The latter, as it were, separates the heart itself from the vessels associated with it, constituting the so-called vascular bundle.
By turning the subject around the vertical axis, you can see in oblique positions those segments that are not visible in the anterior position (right ventricle, left atrium, most of the left ventricle). The most widely used are the so-called first (right nipple) and second (left nipple) oblique positions.
When examining in the left nipple position (the subject stands obliquely, adjacent to the screen with the area of the left nipple), four pulmonary fields are visible, separated from each other by the sternum, cardiovascular shadow and spinal column: 1) presternal, lying in front of the shadow of the sternum and formed by the outer part of the sternum above by the ascending part of the aorta, then by the left atrium and below by the right atrium and the inferior vena cava; anterior contour of the ascending aorta, pulmonary trunk and left ventricle.
- Mitral (mitralis; anat. valva mitralis mitral valve, from Greek mitra miter, headdress) - related to the atrioventricular (mitral) valve of the heart….
- Chest 1 (thorax, pectus, PNA, BNA, JNA) - the upper part of the body, the border of which is drawn above from the jugular notch of the sternum along the clavicles and from the acromioclavicular joints to the apex of the spinous process of the VII cervical vertebra, and below from the xiphoid process of the sternum...
News about Diagram of the projection of heart valves onto the anterior chest wall and the main points for listening to heart murmurs
- Vladimir Ivanovich Makolkin Corresponding member. RAMS, professor, head. Department of Internal Diseases of the 1st Medical Faculty of MMA named after. THEM. Sechenov As is known, among the causes of the development of chronic heart failure (CHF), the leading place is occupied by coronary heart disease (CHD), while
- Despite antibiotic treatment and advances in cardiac surgery, infective endocarditis remains a serious pathology, potentially fatal, the incidence of which may increase due to improved survival of patients with congenital cardiopathy. The frequency is 1.35 cases per 1000 per
Discussion Scheme of the projection of the heart valves onto the anterior chest wall and the main points for listening to heart murmurs
- I had an echocardiogram 2 years ago. Mitral valve prolapse 3.5 mm 1st grade was discovered. , MR 1st, TR1st. Open oval window. And an unstable flow from left to right. I gave birth a year ago and am now worried about palpitations and tachycardia. Today I did another echocardiogram. Aorta - 3.0 cm Left atrium - 2.8 cm Gender
- Dear doctor! Regarding the issue of mitral valve prolapse in a 12 year old boy, I am sending the results of the examination: ECHO-CG study: Project of the aortic root – 21 mm Left atrium – 23 mm Systolic divergence of the leaflets – 13 mm Left ventricle EDC – 43 mm Left ventricle CSP – 28 mm Prej