History of auscultation
René Laennec - first proposed the method of auscultation
Today it is difficult to imagine that back in the 19th century the heart was listened directly to the ear. A revolution in the history of diagnosing cardiovascular diseases was made by Rene Laennec, who had the idea of rolling a sheet of music into a tube. Having applied the newly created structure to the chest of a young patient, Rene Laennec was pleasantly surprised by the results of his work. Heart sounds were heard much better.
From this time on, the method of heart auscultation began. The sheet of music was replaced by a single-tube stethoscope, gradually changing its shape. Then Pyotr Nikolaevich Korotkov invented a phonendoscope, which makes it possible to differentiate high-frequency noises. Today, combined stethophonendoscopes are readily available, allowing for more accurate assessment of the functioning of the cardiovascular system.
Stethoscope device
Double-head neonatal stethophonendoscope
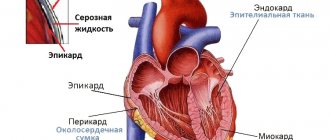
Before moving on to the topic of listening points, it would be appropriate to refer to the structure of the stethoscope and phonendoscope. Recently, the most common combined version is the stethophonendoscope. This option is very convenient and more informative in assessing the functioning of the cardiovascular system. A stethoscope consists of a bell-shaped head, a tube and tips (olives). The phonendoscope is also equipped with a membrane and also has tubes and olives.
A stethoscope during auscultation helps to listen to low-frequency noises. The phonendoscope allows you to evaluate high-frequency noise, since the built-in membrane reduces the audibility of low-frequency sounds. A stethoscope is convenient for listening to the lungs and blood vessels, a phonendoscope is used for auscultation of the heart. However, in each specific case, the specialist, when performing auscultation, gives preference to a stethoscope or phonendoscope.
Auscultation rules
The doctor listens to the heartbeat with a stethoscope
Preparation for auscultation is no less important than the process itself. We know that once we find ourselves in a dark room, we do not immediately begin to distinguish the objects located there. In the same way, our hearing requires adaptation. This is a very important point, which allows the specialist not to miss possible signs of the disease. So, let's pay attention to the following rules for preparing for cardiac auscultation.
- The room should be warm, since to carry out auscultation it is necessary to free the torso above the waist from clothing.
- In the room, it is necessary to try to exclude extraneous sounds that may interfere with the specialist’s auscultation.
- When listening to the heart, the head of the stethoscope or phonendoscope should fit snugly against the surface of the patient’s chest.
- It is recommended to evaluate cardiac function through auscultation in different phases of the respiratory cycle in order to exclude the side effects of respiratory sounds. Therefore, the patient will have to inhale and exhale, as well as hold his breath, if necessary.
- If a murmur is detected at a certain point, auscultation can be performed over the entire cardiac region. With valve defects, heart murmurs tend to spread along the flow of blood. Therefore, in addition to the heart area, the entire surface of the chest, the interscapular space, and the area of the carotid arteries in the neck can be auscultated.
Listening points for the cardiovascular system
The procedure for listening to the heart
Before applying a stethoscope or phonendoscope to the surface of the patient's chest, it is necessary to know the auscultation points of the heart valves. These points of listening to the heart do not coincide with their anatomical projection, which is important to remember. Auscultation of the heart should be carried out in descending order of damage to the heart valves. To make it easier to remember the order of heart listening points, you can mentally draw a figure eight, connecting the points in the correct order.
- The mitral valve is auscultated at the apex of the heart.
- The aortic valve is heard in the second intercostal space to the right of the sternum.
- The pulmonary valve is heard in the second intercostal space to the left of the sternal border.
- The site of auscultation of the tricuspid valve is the base of the xiphoid process of the sternum.
- There is also a fifth auscultation point - the Botkin-Erb point. Auscultation of the heart at this point helps to identify aortic valve insufficiency.
Listening points for heart valves, order of heart auscultation.
Page 1 of 15Next ⇒Heart listening points:
- 1st - point of apex impulse (point of listening to the mitral valve and the left atrioventricular orifice);
- 2nd - point in the 2nd intercostal space directly at the right edge of the sternum (the point of listening to the aortic valves and the aortic orifice);
- 3rd - point in the 2nd intercostal space directly at the left edge of the sternum (point of listening to the pulmonary valves);
- 4th - the lower third of the sternum at the base of the xiphoid process and the place of attachment of the 5th rib to the right edge of the sternum (the point of listening to the tricuspid valve and the right atrioventricular orifice);
- 5th - at the level of the third intercostal space at the left edge of the sternum (an additional point for listening to the aortic valves).
The sequence of listening to the heart is performed in the above order. Auscultation of the heart at the 1st point: the examiner palpably determines the localization of the apex beat and places the phonendoscope on the beat zone. In cases where the apex beat is not palpable, the left border of the relative dullness of the heart is determined by percussion, after which the phonendoscope is installed on a certain border. The subject is given the command to inhale and exhale and hold his breath. Now the doctor, listening to the sounds of the heart, identifies and evaluates them. The first is the tone that follows a long pause, the second is the tone after a short pause. In addition, the first sound coincides with the apical impulse or pulse impulse of the carotid artery. This is checked by palpation of the right carotid artery with the tips of the II-IV fingers of the left hand, installed at the angle of the lower jaw at the inner edge of m. sternocleidomastoideus. In a healthy person, the ratio of tones I and II in volume at this point is such that tone I is louder than tone II, but not more than 2 times. If the sonority of the first tone is more than 2 times higher than the loudness of the second tone, then the amplification of the first tone (clacking first tone) at this point is stated. If the ratio of the first tone and the second tone is such that the volume of the first tone is equal to or weaker than the sound of the second tone, then a weakening of the first tone at this point is stated. In some cases, a rhythm consisting of 3 tones is heard at the apex. The third sound of a healthy heart is often heard in children; it disappears with age. In approximately 3% of healthy people aged 20 to 30 years, the third sound can still be heard; at older ages, it is heard very rarely. In adults, the clinic more often has to deal with a split tone or additional tones that form a three-member heart rhythm (quail rhythm, gallop rhythm, split first tone). Ri) is caused by the appearance of an additional sound in diastole (the sound of the mitral valve opening) and is usually combined with a flapping sound. With the gallop rhythm, tone I is weakened; if the gallop tone precedes the first tone, a presystolic gallop is detected; if the gallop tone follows the second tone, a diastolic gallop is stated. With tachycardia, the sounds that form the presystolic and diastolic gallops can merge, giving a single additional sound in the middle of diastole; such a gallop is called summed. When the first tone is bifurcated, both systolic tones are equal or close to each other in volume.
Auscultation of the heart at the 2nd point: the examiner palpates (with his left hand) finds the point (in the 2nd intercostal space at the right edge of the sternum) and places the phonendoscope on the chest wall in this area. The subject is given the command to inhale and exhale and hold his breath. Now the doctor, listening to the sounds of the heart, identifies and evaluates them. As a rule, a melody of two tones is heard. Identification of tones I and II is carried out according to the method described above. In a healthy person, at this point the second tone is louder than the first. If the ratio of tones I and II is such that the volume of tone II is equal to or weaker than the sound of tone I, then a weakening of tone II at this point is stated. In the case when, instead of the second tone, two fuzzy tones are heard, the splitting of the second tone at this point is stated, and if they are heard clearly, then the splitting of the second tone.
Auscultation at the 3rd point: the examiner palpates (with his left hand) finds the point (in the 2nd intercostal space at the left edge of the sternum) and places the phonendoscope on the chest wall in this area. The subject is given the command to inhale and exhale and hold his breath. Now the doctor, listening to the sounds of the heart, identifies and evaluates them. As a rule, a melody of two tones is heard. Identification of tones I and II is carried out according to the method described above. In a healthy person, at this point, tone II is louder than tone I. In pathology, changes in the ratio of tones and the melody of tones can be the same as at the 2nd point of auscultation. After finishing listening to the heart at the 3rd point, the heart is listened to again at the 2nd and 3rd points in order to compare the volume of the second tone at these two points. In healthy people, the volume of tone II at these points is the same. If the volume of the second tone predominates at one of these points (provided that at each point the second tone is louder than the first, i.e. there is no weakening of it), the emphasis of the second tone is stated over the aorta or pulmonary artery, respectively.
Auscultation of the heart at the 4th point: the examiner palpably (with his left hand) finds the base of the xiphoid process and places the phonendoscope over the right edge of the lower third of the sternum. The subject is given the command to inhale and exhale and hold his breath. Now the doctor, listening to the sounds of the heart, identifies and evaluates them. As a rule, a melody of two tones is heard. In a healthy person, at this point, tone I is louder than tone II. In pathology, changes in the ratio of tones and melody of tones can be the same as at the 1st point of auscultation.
Auscultation of the heart at the 5th point: the examiner palpates (with his left hand) finds the point (in the third intercostal space at the left edge of the sternum) and places the phonendoscope on the chest wall in this area. The subject is given the command to inhale and exhale and hold his breath. Now the doctor, listening to the sounds of the heart, identifies and evaluates them. As a rule, a melody of two tones is heard. The volume of both tones at this point in a healthy person is approximately the same. A change in the ratio of the sonority of the first and second tones during auscultation at the 5th point has no independent diagnostic value. If, in addition to the tones, a prolonged sound is heard between them, then this is noise. In the case when the murmur is heard in the interval between the first and second sounds, it is called systolic; if the noise is determined between the II and I sounds, then it is called diastolic.
16. The vascular bundle of the heart: what is formed, technique and methods for determining the width of the vascular bundle. Reasons for changes in the width of the vascular bundle.
The boundaries of the vascular bundle are determined in the 2nd intercostal space as follows. A pessimeter finger is placed on the 2nd intercostal space on the right along the midclavicular line parallel to the expected dullness and, quietly percussing, it is gradually moved inward towards the sternum until a dull sound appears. The boundaries are marked along the outer edge of the finger, facing the clear percussion sound. Then, in the same way, quiet percussion is performed on the left. A mark is also made along the outer edge of the pessimeter finger. Normally, the diameter of the vascular bundle is 4.5-6 cm.
The vascular bundle is formed by the superior vena cava and the aortic arch on the right, and the pulmonary artery on the left.
Expansion of dullness of the vascular bundle can be observed with a mediastinal tumor. An increase in dullness in the second intercostal space on the right occurs with expansion or aneurysm of the aorta, on the left - with expansion of the pulmonary artery.
The right contour of the relative dullness of the heart in the II and III intercostal spaces is formed by the superior vena cava; in IV - the right atrium. The left contour in the II intercostal space from above is the left part of the aortic arch, then the trunk of the pulmonary artery, at the level of the III rib - the appendage of the left atrium, and down to the IV-V rib - a narrow strip of the left ventricle. The anterior surface of the heart is formed by the right ventricle.
17. Heart sounds: mechanism of formation of the first and second sounds, places of best listening.
The places of best detection of heart sounds - tones, as well as murmurs - do not always coincide with the anatomical localization of their sources - valves and the openings they close. Thus, the mitral valve is projected at the site of attachment of the third rib to the sternum on the left; aortic - in the middle of the sternum at the level of the third costal cartilage; pulmonary artery - in the second intercostal space on the left at the edge of the sternum; tricuspid valve - in the middle of the line connecting the places of attachment to the sternum of the cartilages of the third left and fifth right ribs. Such proximity of the valve openings to each other makes it difficult to isolate sound phenomena at the place of their true projection onto the chest. In this regard, the locations of the best conduction of sound phenomena from each of the valves have been determined.
The place for listening to the bicuspid valve is the area of the apical impulse, i.e., the 5th intercostal space at a distance of 1-1.5 cm inward from the left midclavicular line; aortic valve - II intercostal space on the right at the edge of the sternum, as well as the 5th Botkin-Erb point (place of attachment of the III-IV rib to the left edge of the sternum; pulmonary valve - II intercostal space on the left at the edge of the sternum; tricuspid valve - lower third of the sternum, at base of the xiphoid process.
Listening is carried out in a certain sequence: the area of the apex beat; II intercostal space on the right at the edge of the sternum; II intercostal space on the left at the edge of the sternum; lower third of the sternum (at the base of the xiphoid process); Botkin-Erb point. This sequence is due to the frequency of damage to the heart valves.
In practically healthy individuals, when listening to the heart, two tones are usually detected - the first and second, sometimes the third (physiological) and even the fourth.
The first tone is the sum of sound phenomena occurring in the heart during systole. That's why it's called systolic. It occurs as a result of vibrations of the tense muscle of the ventricles (muscular component), closed leaflets of the bicuspid and tricuspid valves (valve component), the walls of the aorta and pulmonary artery during the initial period of blood entering them from the ventricles (vascular component), the atria during their contraction (atrial component).
The second tone is caused by the slamming and resulting vibrations of the aortic and pulmonary artery valves. Its appearance coincides with the beginning of diastole. That's why it's called diastolic.
Between the first and second tones there is a short pause (no sound phenomena are heard), and the second tone is followed by a long pause, after which the tone appears again. However, students beginning their studies often have great difficulty distinguishing between the first and second tones. To make this task easier, it is recommended to first listen to healthy people with slow heart rates. Normally, the first sound is heard louder at the apex of the heart and in the lower part of the sternum. This is explained by the fact that sound phenomena from the mitral valve are better transmitted to the apex of the heart and the systolic tension of the left ventricle is more pronounced than that of the right. The second tone is heard louder at the base of the heart (at the sites where the aorta and pulmonary artery are heard. The first tone is longer and lower than the second.
1Next ⇒
Heart sounds are normal
In medicine, tone is understood as the result of the work of the valves, chambers of the heart and blood vessels. The place where the first sound is heard is the apex of the heart and the base of the xiphoid process. The second sound is heard in the second intercostal space to the right and left of the sternum. Normally, the volume of the second tone both to the right and to the left of the edge of the sternum should be the same. When listening to the first tone at the apex and base of the xiphoid process of the sternum, its volume is higher in comparison with the first tone. In young and healthy patients, physiological 3rd and 4th tones may be heard. Their difference from pathological ones is listening against the background of the first and second tones. This phenomenon can be explained by the good tone and elasticity of the muscular wall of the heart chambers in young people.
Weakening and strengthening of heart sounds
Causes of weakened heart sounds
During auscultation, the first and second sounds can either weaken or intensify. This can be due to heart-related or non-heart-related reasons. Weakening of the first and second tones can be observed with an increase in the thickness of the subcutaneous fat in the chest area, in persons with developed muscles of the upper shoulder girdle, with exudative pleurisy, inflammation of the heart muscle, myocardial infarction, cardiosclerosis, myocardial dystrophy, pericarditis, etc. Strengthening of both tones observed in persons of asthenic physique, in the presence of an air-containing cavity in the lungs, anemia, tachycardia, emotional stress, increased thyroid function, during physical exertion, etc.
A number of diseases and syndromes can play a role in changing the sonority of one of the tones, which is very important to take into account in the diagnostic process. The first tone can be enhanced with tachycardia, mitral valve stenosis, extrasystole, increased thyroid function, sclerotic processes in the lung tissue, etc. A weakened first tone can be caused by insufficiency of the mitral valve, aortic or other heart valves, myocardial infarction, inflammation of the heart muscle, aortic stenosis, left ventricular myocardial hypertrophy.
When it comes to the second, its amplification (emphasis) is determined based on a comparison of its volume above the aorta and the pulmonary trunk. The emphasis of the second tone on the aorta in adults can be heard with arterial hypertension, as well as with atherosclerotic changes in the aortic valve. An accent or intensification of the second tone over the pulmonary trunk can be heard with mitral valve stenosis, proliferation of connective tissue in the lungs, emphysema (increased airiness of the lung tissue). Weakening of the second tone can be caused by hypotension, insufficiency of the aortic valve, pulmonary valve, and valve stenosis.
What does percussion reveal?
Tapping the borders of the heart helps determine the following indicators:
- the size of the organ
- outlines,
- location in the chest,
- the size of the bundle, consisting of the aortic and pulmonary trunks.
Most often, the patient stands with his arms hanging freely. In severe conditions and in small children, it is possible to perform percussion while lying down, but it should be taken into account that the size will be reduced. In infants, tapping is performed with the middle finger, and for adults, the middle finger-pessimeter of the left hand is needed. It is moved parallel to the expected boundaries. With the middle finger of the right hand, jerky blows are applied to the 2nd phalanx of the plessimeter.
In order to determine the size and outline of the heart, two types of diagnostics are used - determination of relative and absolute dullness.
Due to the fact that next to the heart sac there are lungs filled with air, when moving from them to the dense myocardium, the sound of percussion becomes dull.
The part of the heart that is not covered by lung tissue is projected onto the anterior region of the chest. It is called absolute dullness of the heart (ATC), and all true boundaries are called relative dullness (RTD).
With expansion of the cavities of the heart or myocardial hypertrophy, a displacement of the normal outlines occurs. In healthy people they are:
- ATS - the right line is located along the left edge of the sternum, the left - about 1 cm inward from the apical impulse, the lower - on the 4th rib, the upper - 2nd intercostal space.
- OTS - 1 cm outside the right edge of the sternum, on the left - the area of the apical impulse, below - the 3rd rib, above - the 2nd intercostal space.
Watch the video about performing cardiac percussion:
Split heart sounds
Right bundle branch block
Asynchronous operation of the valves can lead to split and bifurcated heart sounds being heard. Split tones are heard as two separate short sounds. Physiological splitting can be heard in young people and is associated with the inspiratory and expiratory phases. Pathological splitting or splitting of tones can be observed with blockade of the bundle branches (I tone), increased pressure in the aorta and pulmonary artery.
IV tone
IV tone
- atrial - associated with contraction of the atria. When recording synchronously with an ECG, it is recorded at the end of the P wave. This is a weak, low-frequency, rarely heard tone, recorded on the low-frequency channel of the PCG in children and athletes. The pathological IV tone causes a presystolic gallop rhythm during auscultation. The fusion of III and IV pathological tones during tachycardia is defined as a “summation gallop.”
A number of additional systolic and diastolic sounds (clicks) are detected in pericarditis (see), pleuropericardial adhesions, mitral valve prolapse.
Bibliography:
Kassirsky G.I. Phonocardiography for congenital and acquired heart defects, Tashkent, 1972, bibliogr.; Soloviev V.V. and Kassirsky G.I. Atlas of clinical phonocardiography, M., 1983; Fitileva L. M. Clinical phonocardiography, M., 1968; Holldak K. and Wolf D. Atlas and guide to phonocardiography and related mechanocardiographic research methods, trans. from German, M., 1964; Llan S. Phonocardiographie, R., 1961; Schmidt-Voigt J. Atlas der klinischen Phonocardiographie, Miinchen - B., 1955; Zuckermann R. Herzauskultation, Lpz., 1965.
G. I. Kassirsky.
Heart murmurs
Mitral regurgitation
In addition to heart sounds, murmurs in the heart area may also be heard during auscultation. Heart murmurs can be heard in healthy patients, and in such situations we are talking about functional murmurs. Pathological murmurs can be caused by changes in the valvular or muscular apparatus of the heart. But the heart is not always the only culprit of murmurs detected by auscultation. Inflammation of the pleural layers, pericardial layers and other pathologies can cause the appearance of the so-called extracardiac murmur.
Heart murmurs can be systolic, associated with the systolic phase, and diastolic, associated with diastole. Systolic murmurs can be heard if the patient has stenosis (narrowing) of the aortic orifice, pulmonary trunk, mitral or tricuspid valve insufficiency. Diastolic murmurs are heard with stenosis of the mitral and tricuspid valves, as well as with insufficiency of the aortic and pulmonary valves.
Inspection and palpation of the heart area
In healthy people, the apical impulse is palpated 1 cm closer to the center than the line running in the middle of the left clavicle in the 5th intercostal space.
The displacement of this zone occurs:
- upward – with increased intra-abdominal pressure (pregnancy, tumor process, accumulation of fluid, gases);
- down and to the right - with a low position of the diaphragmatic septum (sharp weight loss, prolapse of internal organs, emphysematosis;
- to the left - with hypertrophy of the ventricular myocardium, a sign of aortic, mitral defects, hypertension, sclerotic processes.
If the apex beat is not in the typical place, then this is a sign of dextrocardia (right-sided heart) or accumulation of fluid in the pericardial cavity.
If the patient is healthy, then apart from the apical impulse in the precordial region there should be no other vibrations of the chest wall. When diseases are detected:
- Heart beat. It is felt throughout the palm as an intense shaking. Indicates hypertrophy of the right sections.
- Trembling, similar to a cat's purring. Appears when the aorta, pulmonary artery, mitral orifice narrows, or the aortic duct is not closed.