Let's find out in detail what hyperkalemia is, how it is dangerous for the human body, for what reasons this condition appears, and also find out its symptoms, treatment, possible consequences and preventive measures.
What is hyperkalemia
This is an excess of potassium in the extracellular environments of the body.
Potassium is the main intracellular cation of the human body, which takes part in the conduction of nerve impulses. Its concentration in cells is approximately 140 mmol/l, which is almost 98% of the total content in the body. Extracellular concentration is 3.3–5.0 mmol/l, which corresponds to the normal level of potassium in the blood serum. The upper limit is 5.0–5.5 mmol/l.
Hyperkalemia is considered to be an excess potassium concentration in the blood of more than 5.5 mmol/l.
The code for hyperkalemia according to the International Classification of Diseases, Tenth Revision ICD-10, is E87.5. Belongs to the category “Other disorders of water-salt metabolism or acid-base balance.”
What does potassium and magnesium deficiency lead to?
The content of microelements in the body is one of the parameters of the constancy of the internal environment. Therefore, any deviation, more or less, leads to metabolic pathology. A lack of potassium and magnesium causes an increase in the concentration of sodium and calcium ions, which have opposite properties. Therefore, the following violations develop:
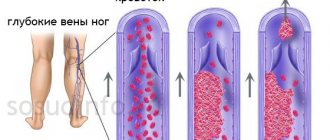
- Spasm of the muscular layer of the heart - contracts during systole, and is not sufficiently restored during diastole.
- Reduced filling of the myocardium with blood leads to ischemia and dystrophy.
- The conduction of cardiac impulses is disrupted.
- Vascular tone increases as the ability to relax decreases.
All this contributes to the development of coronary disease, arterial hypertension, insufficient functioning of the heart, blood stagnation, and arrhythmia.
Why is hyperkalemia dangerous?
With an increase in the extracellular potassium content, its transmembrane ratio changes. At the same time, the resting potential of cells decreases and the functional excitability of tissues increases.
First of all, hyperkalemia affects the conduction system of the heart. Developing atrioventricular block is manifested by severe bradycardia, up to cardiac arrest. This condition is more typical of progressive chronic hyperkalemia.
The rate of increase in blood potassium also matters. Acute situations associated with its excess in the body are more dangerous than a gradual increase in level. A large one-time overdose can cause ventricular tachycardia and fibrillation, which can cause sudden death.
Causes of hyperkalemia
Excess potassium in the body occurs for the following reasons:
- increased consumption with food and medications;
- impaired movement of potassium into the intracellular space or excessive release from it;
- impaired renal excretion.
Combinations of these reasons are also possible. Let's take a closer look at them.
Excessive potassium intake
Potassium enters the body with food. Since its biological digestibility is very high - up to 90–95%, it is therefore easily absorbed through the mucous membrane of the small intestine.
The body's daily need for potassium is from 2.5 to 5 grams.
Excess dietary potassium intake rarely causes clinically significant electrolyte imbalance.
The exception is patients with initially elevated potassium in the blood. A lot of this macronutrient is found in porcini mushrooms, wheat bran, soybeans and dried fruits such as peaches, apricots and dried apricots. Slightly less - in pears, prunes, raisins. Excessive content of such products in the diet can lead to the development of hyperkalemia against the background of renal kidney disease. Potassium preparations are widely used in medicine. Medicines combined with magnesium (Panangin, Asparkam) are indicated for cardiac pathology accompanied by tachycardias and arrhythmias. If there is insufficient intake of potassium from food, confirmed by laboratory tests, doctors prescribe vitamin and mineral complexes. Potassium salts are used as antiseptics, to improve anabolic processes and treat thyroid diseases. Excessive use of these drugs can also cause hyperkalemia.
Disturbances in the movement of potassium in the body
The cause of hyperkalemia can also be an increase in potassium content in the extracellular space:
- due to a slowdown in the transition of cations into the intracellular space - due to a lack of insulin or in a state of acidosis (a shift in the acid-base balance of the body towards increasing acidity);
- as a result of increased release of electrolytes from cells during their massive breakdown.
More common causes of hyperkalemia are disturbances in the processes of removing potassium from the body:
- decreased excretory function of the kidneys due to acute or chronic renal failure;
- lack of adrenal hormones;
- the use of potassium-sparing diuretics - aldosterone inhibitors;
- side effects of medications such as non-steroidal anti-inflammatory drugs, antihypertensive drugs.
The most common cause of hyperkalemia is a disorder of renal excretory function.
Conditions associated with disruption of the transmembrane movement of potassium or its removal from the body, which cause hyperkalemia, are observed in the following pathologies.
- Kidney disease is the most common cause of excess potassium in the blood. Among them are glomerulonephritis, amyloidosis, nephrosclerosis, and diabetic nephropathy. Violation of the processes of glomerular filtration and potassium secretion in the renal tubules leads to the fact that this cation is not excreted from the body.
- Some hormonal conditions can also cause hyperkalemia. Thus, in Addison's disease, a decrease in the level of glucocorticoids and aldosterone leads to reduced excretion of potassium from the body.
- In diabetes mellitus, hyperkalemia occurs due to insufficient insulin, which promotes the passage of potassium into the cell.
- Diseases accompanied by massive breakdown of body cells - trauma, extensive burns, prolonged compartment syndrome, malignant hyperthermia. From destroyed cells, potassium moves into the interstitial space. Large hematomas resolve over time due to hemolysis of red blood cells. This process is also accompanied by hyperkalemia.
- Poisoning with drugs containing potassium or their overdose. In this case, an excess supply of cation from the outside occurs. Cases of poisoning with long-acting potassium tablets, saltpeter, and sodium bichromate (found in match heads) have been described.
- Diseases accompanied by acute metabolic acidosis. An example is acetic acid poisoning. With this pathology, hydrogen ions prevent the entry of potassium into the intracellular space. That is, hyperkalemia will be expected in all diseases accompanied by a decrease in blood pH. Pathological redistribution of potassium between cells and interstitial fluid is also observed during hypoxia, hyperthermia and increased osmolarity.
Features of the symptoms, treatment and prognosis of these diseases are associated with their etiology. The similarity lies only in the syndrome of electrolyte imbalance associated with excess potassium that occurs at a certain stage of the disease, that is, in the appearance of hyperkalemia.
Calcium antagonist abilities
Calcium channel antagonists are represented by various chemical compounds that, in addition to lowering blood pressure, have a number of other capabilities:
- They are able to regulate the rhythm of heart contractions , so they are often used as antiarrhythmic drugs.
- It has been noted that drugs of this pharmaceutical group have a positive effect on cerebral blood flow during the atherosclerotic process in the vessels of the head and for this purpose are used to treat patients after a stroke.
- By blocking the path of ionized calcium into cells, these drugs reduce mechanical tension in the myocardium and reduce its contractility. Thanks to the antispastic effect on the walls of the coronary arteries, the latter expand, which helps to increase blood circulation in the heart. The effect on peripheral arterial vessels is reduced to a decrease in upper (systolic) blood pressure and, of course, peripheral resistance. Thus, as a result of the influence of these pharmaceuticals, the need of the heart muscle for oxygen decreases, and the supply of nutrients to the myocardium and, first of all, oxygen increases.
- Calcium antagonists, by inhibiting Ca++ metabolism in cells, inhibit platelet aggregation, that is, they prevent the formation of blood clots.
- Drugs in this group have antiatherogenic properties, reduce pressure in the pulmonary artery and cause dilatation of the bronchi, which makes it possible to use them not only as antihypertensive drugs.
Scheme: mechanism of action and capabilities of AK 1-2 generations
Symptoms
Excess potassium in the human body is manifested by heart rhythm disturbances, muscle weakness and neurological disorders.
In acutely developed hyperkalemia, its main signs are:
- chest pain;
- increased heart rate;
- a feeling of interruptions in the work of the heart;
- cold sweat;
- nausea;
- weakness;
- dizziness.
Similar symptoms are observed not only with chronic hyperkalemia, but also with an overdose of potassium preparations. Often, patients with such symptoms are admitted to the cardiology department with suspected acute myocardial infarction. However, laboratory tests reveal hyperkalemia.
Gradually developing chronic hyperkalemia is characterized by:
- symptoms of neurological disorders - irritability, anxiety, apathy, confusion, paresthesia, paresis;
- changes in muscle tone - increasing weakness, myoplegia (temporary paralysis of the limbs);
- gastrointestinal disorders - diarrhea, abdominal cramps.
With chronic hyperkalemia, signs of damage to the nervous system - central and peripheral - are clearly visible. A gradual increase in the level of potassium in the blood is accompanied by cardiac conduction disturbances in the form of bradyarrhythmias. Restlessness, irritability and drowsiness may be the first signs of hyperkalemia in a patient with chronic renal failure, indicating decompensation of his condition.
Symptoms of excess potassium in the body are the same for both men and women. The only difference is in the frequency of occurrence of pathological conditions accompanied by hyperkalemia. Thus, women are more prone to kidney diseases of inflammatory etiology and diabetes mellitus. Malignant kidney tumors and Addison's disease are more common in men.
Diagnostics
If hyperkalemia develops, hospitalization in the intensive care unit is indicated. Diagnostics takes into account the patient’s complaints, medical history, electrocardiography (ECG) results and laboratory blood parameters.
Complaints are usually nonspecific. The anamnesis is not always complete and reliable. Therefore, the first stage of diagnosis is based on the results of an ECG and biochemical blood tests. Changes in the shape of the T and P waves on the ECG are the primary signs of hyperkalemia.
Blood tests confirm the presence of elevated potassium levels. With a further increase in its concentration, the electrocardiogram registers disturbances in heart rhythm and conduction.
Data on a decrease in diuresis and the results of urine tests (if the electrolyte disturbances are renal) are informative.
A more detailed examination of the patient, allowing to identify the cause of the electrolyte imbalance, is carried out after relief of hyperkalemia.
First aid for an overdose of potassium preparations
In case of acute hyperkalemia, the hospital administers intravenous medications that reduce the level of potassium in the blood, under the control of laboratory parameters.
First-line drugs include calcium gluconate, which is an antidote to potassium.
Another drug that can relieve acute hyperkalemia is insulin. It is administered intravenously with glucose solution. However, infusion should be withheld when hyperkalemia is associated with the development of renal failure.
If a potassium overdose occurs outside the hospital, emergency treatment is provided by emergency medical personnel. The administration of potassium antidote is permissible if the following conditions are met:
- availability of accurate information about the fact of poisoning with a substance that contains potassium, or about its overdose;
- the victim's complaints and ECG data correspond to the symptoms of hyperkalemia;
- the risk of transporting the patient to the hospital without administering an antidote exceeds the risk of using this drug in the absence of laboratory confirmation of hyperkalemia.
The urgency of treatment measures is associated with the likelihood of life-threatening cardiac arrhythmias. For emergency correction of hyperkalemia, calcium salts are used. They prevent the possibility of sudden cardiac arrest by acting on the myocardium as potassium antagonists.
Classification
Full article: classification of drugs for hypertension.
Calcium antagonists are divided into derivatives:
- phenylalkylamine;
- benzothiazepine;
- dehydropyridine.
Another classification involves dividing calcium antagonists into two groups:
- non-dihydropyridine;
- dihydropyridine.
Classification by generation divides drugs into groups:
- first generation (Nifedipine, Diltiazem, Verapamil);
- second IIA generation (Nifedipine SR, Nicardipine SR, Felodipine SR, Dlitiazem SR, Verapamil SR);
- second IIB generation (Benidipin, Felodipin and others);
- third generation (Amlodipine, Lacidipine, Lecarnidipine).
First generation drugs have several properties that limit their use:
- low bioavailability;
- short action;
- frequent occurrence of side effects (headache, tachycardia, redness of the skin);
- decreased heart rate and strength (diltiazem and verapamil).
Second generation drugs have a better effect than the first. Some of them act for a short time, and peak concentrations of active substances in the blood are reached at different times.
Third generation drugs were developed taking into account the shortcomings of first and second generation drugs, therefore they have:
- high bioavailability;
- high tissue selectivity;
- long half-life from the body.
Treatment
Therapy for hyperkalemia includes measures to eliminate electrolyte imbalance, establish a diagnosis and etiotropic treatment of the underlying disease. If medications are ineffective, hemodialysis is used.
Drug treatment of hyperkalemia is carried out with the following drugs:
- if there is a persistent increase in blood potassium, repeated administration of calcium gluconate is required;
- intravenous administration of insulin in a glucose solution (contraindicated in anuria, when urine output stops);
- the use of sodium bicarbonate to correct acidosis;
- administration of beta-agonists (salbutamol) intravenously or inhaled as an aerosol;
- administration of diuretics to enhance potassium excretion by the kidneys (ineffective in the oliguric stage of acute renal failure, when diuresis decreases);
- removing excess potassium from the body by using orally or rectally cation exchange resins.
Extracorporeal detoxification methods are used, as well as implantation of an artificial pacemaker.
- Conducting hemodialysis for the treatment of hyperkalemia in chronic renal failure, accompanied by symptoms of oliguria or anuria and resistant to other drugs.
- If complete atrioventricular block develops, a pacemaker must be installed.
Causal therapy prevents the possibility of relapse. Treatment of the disease that causes hyperkalemia is based on the following measures:
- establishing a diagnosis;
- carrying out therapy according to etiology;
- involvement of specialized specialists in the process.
Which doctor treats hyperkalemia? Ideally, this is an anesthesiologist-resuscitator in the intensive care unit. However, more often it happens that emergency care for hyperkalemia is provided by the doctor on duty who admits the patient to the hospital. After the diagnosis has been established, treatment will be continued by a specialized specialist - a nephrologist, urologist, toxicologist or endocrinologist.
Treatment of hyperkalemia with folk remedies can only be used as an addition to the main therapy. It is acceptable to use traditional medicine when potassium values do not exceed 5.0–6.0 mmol/l. However, it must be taken into account that when combining drug therapy and folk therapy, undesirable effects may occur. Therefore, constant interaction between the patient, his attending physician and herbalist is required. As well as periodic monitoring of potassium in the blood.
Diet for hyperkalemia
What foods should you not eat if blood tests reveal hyperkalemia? Many dried fruits, grains and legumes become forbidden foods. Fruits, vegetables and herbs are included in the blacklist.
However, with a complete exclusion of all of the above from food, hypovitaminosis may occur. Therefore, meat products, fish, apples, currants, garlic and onions will help restore the lack of microelements. Due to the low potassium content, they reduce its concentration in the blood, replenishing the lack of other vitamins.
Mode of application
Let's get acquainted with the method of using some drugs.
- Nifedipine . It is used orally in a dose of 5 to 10 mg after meals 3 to 4 times throughout the day, and to stop a hypertensive crisis - 5 to 10 mg sublingually.
- Nifedipine retard (Corinfar retard). Prescribed 10–20 mg twice a day after meals.
- Nifedipine GITS (continuous release). Use 60 - 90 mg once per day.
- Felodipine . Prescribed after meals, 2.5–10 mg once a day. The tablets should be washed down with water; they should not be crushed or chewed, but should be taken whole. The dose is increased gradually if necessary.
- Amlodipine . Used after meals, 2.5–10 mg once daily. If necessary, the dose is increased gradually. The maximum permissible daily dose is 10 mg.
- Lacidipine. The starting dose for adults is 2 mg per day. If possible, you should take the drug at the same time, preferably in the morning. The full effect develops after 3-4 weeks of regular use.
- Nisoldipine . At the beginning of treatment, the dosage is 5–10 mg twice a day. According to indications, after 3–4 weeks it can be increased to 20 mg per dose. The drug is taken with meals in the morning and evening. Do not chew, you need to drink enough water.
- Gallopamil . Prescribed 50 mg 2 times a day. It should be taken either during meals or immediately after it, the maximum permissible dose per day is 200 mg.
- Diltiazem . Take 60–90 mg three times a day. The tablets should not be chewed, they should be taken before meals and washed down with plenty of water. The daily maximum dosage is 360 mg (4 times 90 mg).
- Diltiazem SR . Used one to two times a day, 120–180 mg with meals.
Hyperkalemia in children
The mechanism of development of electrolyte imbalance in patients of different age groups is the same. The causes of hyperkalemia in children and adults are also basically the same. However, there is a hereditary disease that manifests itself already in the first weeks of a child’s life. It is associated with the absence of the enzyme steroid 21-hydroxylase in the newborn’s body. As a result, the synthesis of progesterone and adrenal hormones, which are responsible for water and electrolyte balance, is disrupted. The pathological condition is called adrenogenital salt loss syndrome.
Clinical manifestations of the disease are abnormal development of the genital organs and severe dehydration, accompanied by a decrease in blood pressure. Laboratory testing reveals elevated potassium levels. Treatment of hyperkalemia in young children with this hereditary pathology is carried out with adrenal hormones. Replacement therapy is carried out intravenously or intramuscularly, with a gradual transition to oral administration of drugs.
Hyperkalemia during pregnancy
Women during pregnancy also face problems with electrolyte imbalance. However, hyperkalemia is not typical for this period. On the contrary, physiological pregnancy is accompanied by hypervolemia and a decrease in blood osmolarity due to a decrease in the concentration of electrolytes, including potassium.
With a pathological course of pregnancy, the severity of these manifestations increases, aggravating hypokalemia. A decrease in blood potassium levels is an electrolyte imbalance typical of pregnancy.
Consequences of hyperkalemia
Acutely developed electrolyte imbalance is easier to treat than chronic hyperkalemia. The outcome of the disease depends on the severity of the injury or poisoning that caused a sharp increase in potassium levels in the blood.
Most complications of hyperkalemia are observed in chronic progressive diseases. A gradual increase in potassium in the blood is accompanied by conduction disturbances, up to complete atrioventricular block. The rapid increase in electrolyte causes clinically significant rhythm disturbances. The cause of death from treatment-resistant hyperkalemia is asystole or ventricular fibrillation.
Reasons why the level of potassium and magnesium in the body decreases
The main reason for the reduced intake of potassium and magnesium is an unbalanced diet, which contains little dietary fiber from vegetables, nuts, bran, legumes, and leafy greens. Increased amounts of table salt and sugar, as well as caffeine, lead to a drop in the level of potassium and magnesium in the blood. A relative deficiency of microelements may occur when the need is high:
- exercise stress;
- stress;
- loss of fluid - high ambient temperature (climate, at work, sauna), vomiting, diarrhea, forced diuresis with diuretics;
- laxative abuse;
- taking birth control pills;
- surgeries, injuries and burns;
- diabetes;
- impaired absorption from the intestine in diseases of the digestive system (enteritis, gastritis, cholecystitis, pancreatitis, peptic ulcer).
Prevention measures
Many diseases accompanied by hyperkalemia are chronic and progressive. Therefore, in order to prevent relapses, the following preventive measures are effective:
- taking medications selected for the treatment of the underlying disease;
- discontinuation of medications that can cause hyperkalemia;
- avoiding consumption of foods with high potassium content;
- periodic monitoring of blood electrolytes;
- observation by a local therapist.
Compliance with the basic principles of prevention ensures long-term remission of chronic diseases, resulting in an improvement in the quality of life of patients.
Let's summarize. Hyperkalemia is an excess of potassium in the blood. It is a life-threatening condition, as it is accompanied by disturbances in the conduction and rhythm of the heart. The most common cause of hyperkalemia is a disorder of the excretory function of the kidneys. Diagnosis is based on medical history, blood electrolyte studies and electrocardiography. Therapy is carried out with medications including potassium antidote. If drug treatment is ineffective, dialysis is used. Rapid elimination of hyperkalemia and etiotropic treatment are the basis of the patient’s recovery.
Hyperkalemia
Literature
- I.V. Davydova, N.A. Perepelchenko, L.V. Klimenko. Calcium channel blockers: mechanisms of action, classification, indications and contraindications for use, 2009
- Giuseppe Mancia, Robert Fagard et al. Guidelines for the treatment of arterial hypertension ESH/ESC 2013, 2014
- Yu. Shtrygol. Calcium channel blockers in cardiology, 2004
Irina Kostyleva
Higher medical education. Kirov State Medical Academy (KSMA). Local therapist. More about the author
All articles by the author