Both prevention and treatment of cardiovascular diseases require a responsible and serious approach. These kinds of problems are increasingly worrying people today. Therefore, many tend to treat them somewhat frivolously. Such people often either completely ignore the need to undergo treatment, or take medications without a doctor’s prescription (on the advice of friends). However, it is important to remember: just because a drug has helped someone else does not guarantee that it will help you too. Forming a treatment regimen requires sufficient knowledge and skills that only specialists have. It is also possible to prescribe any drugs only taking into account the individual characteristics of the patient’s body, the severity of the disease, the characteristics of its course and medical history. In addition, today there are many effective medications that only specialists can select and prescribe. For example, this applies to sartans, a special group of drugs (they are also called angiotensin 2 receptor blockers). What are these drugs? How do angiotensin 2 receptor blockers work? Contraindications to the use of substances apply to which groups of patients? In what cases would it be appropriate to use them? What drugs are included in this group of substances? The answers to all these and some other questions will be discussed in detail in this article.
Angiotensin 2 receptor blockers: mechanism of action
Before you start using prescribed medications, it is important to understand exactly how they work. How do angiotensin 2 receptor blockers affect the human body? The drugs in this group bind to receptors, thus blocking a significant increase in blood pressure. This helps prevent hypertension effectively. Angiotensin 2 receptor blockers are the most effective substances in this regard. Experts pay due attention to them.
Side effects
A distinctive feature of angiotensin II receptor blockers is their good tolerability, comparable to placebo. Side effects when taking them are observed much less frequently than when using ACE inhibitors. Unlike the latter, the use of angiotensin II blockers is not accompanied by the appearance of a dry cough. Angioedema also develops much less frequently.
Like ACE inhibitors, these drugs can cause a fairly rapid decrease in blood pressure in hypertension, which is caused by increased renin activity in the blood plasma. In patients with bilateral narrowing of the renal arteries, renal function may deteriorate. The use of angiotensin II receptor blockers in pregnant women is contraindicated due to the high risk of fetal development disorders and fetal death.
Despite all these undesirable effects, sartans are considered the most well tolerated group of drugs for lowering blood pressure by patients, with the lowest incidence of adverse reactions. They go well with almost all groups of drugs that normalize blood pressure, especially with diuretics.
Angiotensin 2 receptor blockers: classification
There are several types of sartans, differing in their chemical structure. It is possible to choose angiotensin 2 receptor blockers that are suitable for the patient. The drugs, a list of which will be given below, are important to research and discuss the appropriateness of their use with your doctor.
So, there are four groups of sartans:
- Biphenyl tetrazole derivatives.
- Non-biphenyl tetrazole derivatives.
- Non-biphenyl netetrazole.
- Non-cyclic compounds.
Thus, there are several types of substances into which angiotensin 2 receptor blockers are divided. The drugs (list of main ones) are presented below:
- "Losartan."
- "Eprosartan".
- "Irbesartan".
- Telmisartan.
- "Valsartan".
- "Candesartan".
Pharmacological interactions
Angiotensin II receptor blockers may enter into pharmacodynamic interactions, changing the manifestation of the hypotensive effect, increasing the concentration of potassium in the blood serum when combined with potassium-sparing diuretics and potassium-sparing drugs. Pharmacokinetic interaction is also possible with Warfarin and Digoxin (Table 4).
Drug interactions with angiotensin II receptor blockers:
Interacting drugAngiotensin II receptor antagonistsResult of interaction
| Alcohol | Losartan, Valsartan, Eprosartan | Increased hypotensive effect |
| Antihypertensive drugs, diuretics | All | Increased hypotensive effect |
| Nonsteroidal anti-inflammatory drugs, estrogens, sympathomimetics | All | Weakening the hypotensive effect |
| Potassium-sparing diuretics, potassium-containing drugs | All | Hyperkalemia |
| Warfarin | Valsartan, Telmesartan | Decreased maximum blood concentration, increased prothrombin time |
| Digoxin | Telmisartan | Increase in maximum blood concentration |
Indications for use
You can take substances from this group only as prescribed by your doctor. There are several cases in which it would be reasonable to use angiotensin 2 receptor blockers. Clinical aspects of the use of drugs in this group are as follows:
- Hypertension. It is this disease that is considered the main indication for the use of sartans. This is due to the fact that angiotensin 2 receptor blockers do not have a negative effect on metabolism, do not provoke erectile dysfunction, or impair bronchial patency. The effect of the drug begins two to four weeks after the start of treatment.
- Heart failure. Angiotensin 2 receptor blockers inhibit the action of the renin-angiotensin-aldosterone system, whose activity provokes the development of the disease.
- Nephropathy. Due to diabetes mellitus and arterial hypertension, serious disturbances in the functioning of the kidneys occur. Angiotensin 2 receptor blockers protect these internal organs and prevent too much protein from being excreted in the urine.
Angiotensin II receptor blocking drugs
Attempts to achieve blockade of the renin-angiotensin system at the receptor level have been made for a long time. In 1972, the peptide angiotensin II antagonist saralazine was synthesized, but it did not find therapeutic use due to its short half-life, partial agonist activity, and the need for intravenous administration. The basis for the creation of the first non-peptide angiotensin receptor blocker was the research of Japanese scientists, who in 1982 obtained data on the ability of imidazole derivatives to block AT1 receptors. In 1988, a group of researchers led by R. Timmermans synthesized the non-peptide angiotensin II antagonist losartan, which became the prototype of a new group of antihypertensive drugs. Used in the clinic since 1994.
Subsequently, a number of AT1 receptor blockers were synthesized, but currently only a few drugs have found clinical use. They differ in bioavailability, level of absorption, distribution in tissues, rate of elimination, and the presence or absence of active metabolites.
"Losartan"
An effective substance belonging to the sartan group. Losartan is an angiotensin 2 receptor antagonist blocker. Its difference from other drugs is a significant increase in exercise tolerance in people suffering from heart failure. The effect of the substance becomes maximum within six hours from the moment of taking the medicine. The desired effect is achieved after three to six weeks of using the drug.
The main indications for the use of the drug in question are the following:
- heart failure;
- arterial hypertension;
- reducing the risk of stroke in those patients who have the prerequisites for this.
It is prohibited to use Losartan during pregnancy and breastfeeding, as well as in cases of individual sensitivity to individual components of the drug.
Angiotensin 2 receptor blockers, which include the drug in question, can cause certain side effects, such as dizziness, insomnia, sleep disturbances, taste disturbances, vision disturbances, tremor, depression, memory disorders, pharyngitis, cough, bronchitis, rhinitis, nausea, gastritis, toothache, diarrhea, anorexia, vomiting, cramps, arthritis, shoulder pain, back pain, leg pain, palpitations, anemia, renal dysfunction, impotence, decreased libido, erythema, alopecia, rash, itching, swelling, fever, gout, hyperkalemia .
The drug should be taken once a day, regardless of meals, in doses prescribed by your doctor.
Features of application
As a rule, drugs that block angiotensin receptors are produced in the form of tablets, which can be taken regardless of food intake. The maximum stable concentration of the drug is achieved after two weeks of regular use. The elimination period from the body is at least 9 hours.
Sartans are recommended for patients who have contraindications to the use of ACE inhibitors. The doctor selects the dose based on the individual characteristics of the patient’s body.
Angiotensin 2 blockers may differ in their spectrum of action.
Features of taking Losartan
The course of treatment for hypertension is 3 weeks or more, depending on individual characteristics.
In addition, this drug reduces the concentration of uric acid in the blood and removes sodium from the body. The dosage is adjusted by the attending physician based on the following indicators:
- Combination treatment, including the use of this drug with diuretics, involves the use of no more than 25 mg. per day.
- If side effects occur, such as headache, dizziness, decreased blood pressure, the dosage of the drug must be reduced.
- In patients with liver and kidney failure, the drug is prescribed with caution and in small doses.
Contraindications for taking Valsartan
The drug acts only on AT-1 receptors, blocking them. The effect of a single dose is achieved after 2 hours. It is prescribed only by the attending physician, as there is a risk that the drug may cause harm.
Patients who have the following pathologies should approach the use of the drug with caution:
- Obstruction of the bile ducts. The drug is excreted from the body with bile, so patients who have disturbances in the functioning of this organ are not recommended to use valsartan.
- Renovascular hypertension. In patients with this diagnosis, it is necessary to monitor serum urea levels, as well as creatinine.
- Imbalance of water-salt metabolism. In this case, correction of this violation is mandatory.
Important! When using Valsartan, the patient may experience symptoms such as cough, swelling, diarrhea, insomnia, and decreased sexual function. While taking the drug, there is a risk of developing various viral infections.
The drug should be taken with caution when performing work that requires maximum concentration.
Purpose of Ibersartan
The action of the drug is aimed at:
- reducing the load on the heart;
- elimination of the vasoconstrictor effect of angiotensin 2;
- decrease in aldosterone concentration.
The effect of taking this drug is achieved after 3 hours. After completing the course of taking Ibersartan, blood pressure gradually returns to its original value.
Ibersartan does not prevent the development of atherosclerosis, unlike most angiotensin receptor antagonists, since it does not affect lipid metabolism.
Important! The drug is to be taken daily at the same time. If you miss a dose, doubling the dose is strictly not recommended.
Adverse reactions when taking Ibersartan:
- headache;
- nausea;
- dizziness;
- weakness.
Efficacy of Eprosartan
In the treatment of hypertension, it has a mild and lasting effect throughout the day. When you stop taking it, there are no sudden increases in pressure. Eprosartan is prescribed even for diabetes mellitus, as it does not affect blood sugar levels. The drug can also be taken by patients with kidney failure.
Eprosartan has the following side effects:
- cough;
- runny nose;
- dizziness;
- headache;
- diarrhea;
- chest pain;
- dyspnea.
Adverse reactions, as a rule, are short-term and do not require dose adjustment or complete discontinuation of the drug.
The drug is not prescribed to pregnant women, during breastfeeding and to children. Eprosartan is not prescribed to patients with renal artery stenosis, as well as with primary hyperaldosteronism.
"Valsartan"
This drug effectively reduces myocardial hypertrophy, which occurs as a result of the development of arterial hypertension. Withdrawal syndrome does not appear after stopping the use of the drug, although it is caused by some angiotensin 2 receptor blockers (the description of the sartan group helps to clarify which drugs this property applies to).
The main indications for taking the substance in question are the following conditions: myocardial infarction, primary or secondary hypertension, congestive heart failure.
The tablets are taken orally. They should be swallowed without chewing. The dose of the drug is prescribed by the attending physician. But the maximum amount of the substance that can be taken during the day is six hundred and forty milligrams.
Sometimes angiotensin 2 receptor blockers can have a negative effect on the body. Side effects that Valsartan can cause: decreased libido, itching, dizziness, neutropenia, loss of consciousness, sinusitis, insomnia, myalgia, diarrhea, anemia, cough, back pain , vertigo, nausea, vasculitis, edema, rhinitis. If any of the above reactions occur, you should immediately contact a specialist.
Video on the topic
Lectures by the Doctor of Medical Sciences on drugs from the sartan group:
Thus, according to experts and patients, sartans are quite effective drugs, and side effects are very rarely observed when taken. Despite this, it is unacceptable to prescribe a certain remedy for yourself. Selecting the wrong medicine can only aggravate the disease and generally harm the condition of the patient’s body.
The information on the MyMedNews.ru website is for reference and general information, collected from publicly available sources and cannot serve as a basis for making a decision on the use of medications in the course of treatment.
MyMedNews.ru
And we also have
Fenyuls or Sorbifer - which is better?
"Candesartan"
The drug in question is prepared in the form of tablets for oral use. It should be taken once or twice a day at the same time, regardless of meals. You should carefully follow the recommendations of specialists. It is important not to stop taking the drug even when you feel better. Otherwise, this may negate the effectiveness of the drug.
When using it, caution should be exercised in patients who suffer from diabetes, kidney failure, or are pregnant. All of these conditions must be reported to specialists.
"Telmisartan"
The drug in question is absorbed from the gastrointestinal tract in a fairly short time. It can be taken regardless of meals. The main indication for use is arterial hypertension. The half-life of the drug is more than twenty hours. The drug is excreted through the intestines almost unchanged.
It is prohibited to take the drug in question during pregnancy or breastfeeding.
The drug may cause the following side effects: insomnia, dizziness, nausea, diarrhea, depression, abdominal pain, pharyngitis, rash, cough, myalgia, urinary tract infections, low blood pressure, chest pain, palpitations, anemia.
Effective drugs from the ARB group
Each drug differs in active substance and pharmacokinetics. The dosage of the medication and the duration of treatment should be selected for each patient exclusively by a doctor, based on health characteristics, concomitant pathologies, and age.
List of drugs that have proven themselves in medicine:
- Blocktran. Well tolerated by patients. Promotes the removal of excess uric acid from the body, protects the kidneys from the effects of high blood pressure, especially in patients with diabetes. Used in combination with diuretics. Improves blood circulation in the vessels of the brain, helps normalize metabolic processes, and stimulates memory. Price – about 400 rubles;
- Teveten. Effectively lowers blood pressure without affecting heart rate, plasma sugar and triglyceride levels. Improves blood circulation in the kidneys. Concomitant use with angiotensin converting enzyme inhibitors in patients with nephropathy is not recommended. Contraindications: pregnancy and breastfeeding, individual intolerance to the drug components, renal artery stenosis. Price – 1500-2000 rubles;
- Irbesartan . Absorbed from the gastrointestinal tract within the first hour. Reaches maximum plasma concentration after 2 hours. It is used in the treatment of hypertension complicated by pathological processes in the kidneys. Approved for the treatment of type 2 diabetic patients. In severe hypertension, it is permissible to combine with calcium channel blockers, beta-blockers and diuretics. In this case, the hypotensive effect of all drugs increases;
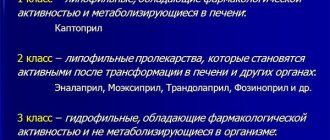
- Atakand. Tablets contain 8 or 16 mg of the active substance – candesartan. The therapeutic effect appears a couple of hours after the first dose and lasts for a day. Does not change heart rate. The big advantage of the drug is that it does not cause withdrawal symptoms. According to research results, Atacand reduces the incidence of complications in the form of heart failure and improves the contractile function of the left ventricle. Belongs to a group of prodrugs that begin to work after the transformation of the active substances in the liver. Price – 1500-2800 rubles;
- Losartan. A synthetic angiotensin 2 receptor blocker common among hypertensive patients. It is rapidly absorbed from the gastrointestinal tract, reaching maximum plasma levels after 2 hours. The drug is excreted in bile and urine. The effect of Losartan on older people is no different, therefore it is often used in their treatment. Suitable for combination therapy of arterial hypertension complicated by pathologies of the cardiovascular system, kidneys, and diabetes. Has an organoprotective effect on target organs. Under medical supervision, use in children over 12 years of age is permitted, strictly following the instructions. Price – 100 -500 rubles depending on the number of tablets in the package;
- Mikardis . In addition to a pronounced hypotensive effect, it has organoprotective properties. Protects the heart from the harmful effects of high blood pressure, relieves stress, and prevents the development of complications. Reduces the risk of mortality from cardiovascular pathologies in older patients. Contraindications: biliary tract disorders, children under 18 years of age, pregnant and lactating women. Price – 1700-2300 rubles;
- Cardosal. Contains a potent antihypertensive component – olmesartan. The therapeutic effect lasts throughout the day. When taken regularly, it gives stable results in 6-8 weeks. There is no withdrawal syndrome. Quickly relaxes blood vessels, improves blood circulation, and prevents hemorrhage in the brain. Price – about 1000 rubles;
- Lorista. A synthetic antagonist that effectively blocks angiotensin receptors. After 2-3 hours it reaches its maximum concentration in the blood and begins to act. Excreted in urine. Well tolerated by patients over 60 years of age, with complications of the urinary system, and diabetes mellitus. Taking the drug is considered prophylactic to prevent cerebral strokes and myocardial infarction.
"Eprosartan"
The drug in question should be taken once a day. The recommended amount of the drug for one-time use is six hundred milligrams. The maximum effect is achieved after two to three weeks of use. Eprosartan can be either part of complex therapy or the main component of monotherapy.
Under no circumstances should the drug in question be used during lactation or pregnancy.
What adverse reactions may occur when using Eprosartan? Among them are the following: weakness, diarrhea, dizziness, headache, rhinitis, cough, shortness of breath, swelling, chest pain.
Clinical pharmacology
All drugs are highly active in the blood, have good bioavailability and have a long-lasting effect when taken orally, so they are recommended to be taken once a day. ARBs are primarily cleared by the liver and to a small extent by the kidneys, allowing their cautious use in renal failure. Because ARBs are similar in activity to ACEIs, angiotensin II blockers should not be prescribed for stenosis of both renal arteries. Eprosartan and Telmisartan are relatively contraindicated in diseases of the liver and bile ducts, since more than 90% of their concentration is eliminated by the liver. The clinical pharmacology of the main list of drugs is presented in Table 3.
Pharmacokinetic parameters of angiotensin II receptor antagonists:
Drug Bioavailability (%) Plasma protein binding (%) Maximum concentration (h) Half-life (h) Hepatic excretion (%) Renal excretion (%)
| Valsartan | 23 | 94-97 | 2-4 | 6-7 | 70 | 30 |
| Irbesartan | 60-80 | 96 | 1,5-2 | 11-15 | More than 75 | 20 |
| Candesartan | 42 | Over 99 | 4 | 9 | 68 | 33 |
| Losartan | 33 | 99 | 1-2 | 2 (6-7) | 65 | 35 |
| Telmisartan | 42-58 | More than 98 | 0,5-1 | 24 | More than 98 | Less than 1 |
| Eprosartan | 13 | 98 | 1-2 | 5-9 | 70 | 30 |
ARBs affect neurohumoral interactions in the body, including the main regulatory systems: the RAAS and the sympathoadrenal system (SAS), which are responsible for increased blood pressure and the emergence and progression of cardiovascular pathologies.
"Irbesartan"
The drug in question is taken orally. It is absorbed from the gastrointestinal tract in a short time. The maximum concentration of the substance in the blood occurs after one and a half to two hours. Eating does not affect the effectiveness of the medicine.
If the patient is prescribed hemodialysis, this does not affect the mechanism of action of Irbesartan. This substance is not removed from the human body through hemodialysis. Likewise, patients suffering from mild to moderate liver cirrhosis can safely take the drug.
The medicine should be swallowed without chewing. Its use does not need to be combined with food intake. One hundred and fifty milligrams per day is considered the optimal starting dosage. Elderly patients are recommended to start treatment with seventy milligrams. During treatment, your doctor may decide to change the dosage (for example, increase it if the therapeutic effect on the body is insufficient). In this case, the patient may be prescribed to take three hundred milligrams of the drug or, in principle, replace the main drug. For example, for the treatment of people suffering from type 2 diabetes mellitus and arterial hypertension, the dosage should be gradually changed from one hundred and fifty milligrams per day to three hundred milligrams (this is the amount of medication that is most effective in combating nephropathy).
There are certain features of the use of the drug in question. Thus, patients suffering from water-electrolyte imbalance must eliminate some of its manifestations (hyponatremia) before starting treatment.
If a person has impaired kidney function, then his treatment regimen may be the same as if there were no such problem. The same applies to mild to moderate liver dysfunction. At the same time, when hemodialysis is carried out simultaneously, the initial amount of the drug should be halved compared to usual and amount to seventy-five milligrams per day.
Experts do not recommend the use of the drug in question by minors, since it has not been established how safe and effective it is for patients of this age.
Irbesartan is strictly contraindicated for use by women who are pregnant, as it directly affects the development of the fetus. If pregnancy occurs while undergoing therapy, the latter should be discontinued immediately. It is recommended to switch to the use of alternative drugs before planning a pregnancy. The drug in question should not be used during breastfeeding, since there is no information as to whether this substance passes into breast milk.
Main effects of AT1 receptor blockers
The effects of angiotensin II antagonists are due to their ability to bind to specific receptors of the latter. Having high specificity and preventing the action of angiotensin II at the tissue level, these drugs provide more complete blockade of the renin-angiotensin system compared to ACE inhibitors. The advantage of AT1 receptor blockers over ACE inhibitors is also the absence of an increase in the level of kinins when they are used. This avoids unwanted side effects caused by the accumulation of bradykinin, such as cough and angioedema.
Blockade of AT1 receptors by angiotensin II antagonists leads to suppression of its main physiological effects:
- vasoconstriction
- aldosterone synthesis
- release of catecholamines from the adrenal glands and presynaptic membranes
- release of vasopressin
- slowing down the process of hypertrophy and proliferation in the vascular wall and myocardium
Hemodynamic effects
The main hemodynamic effect of AT1 receptor blockers is vasodilation and, consequently, a decrease in blood pressure.
The antihypertensive effectiveness of drugs depends on the initial activity of the renin-angiotensin system: in patients with high renin activity they act more strongly.
The mechanisms through which angiotensin II antagonists reduce vascular resistance are as follows:
- suppression of vasoconstriction and hypertrophy of the vascular wall caused by angiotensin II
- decreased Na+ reabsorption due to the direct action of angiotensin II on the renal tubules and through decreased aldosterone release
- elimination of sympathetic stimulation due to angiotensin II
- regulation of baroreceptor reflexes due to inhibition of the structures of the renin-angiotensin system in brain tissue
- an increase in the content of angiotensin, which stimulates the synthesis of vasodilatory prostaglandins
- decreased vasopressin release
- modulating effect on vascular endothelium
- increased production of nitric oxide by the endothelium due to activation of AT2 receptors and bradykinin receptors by increased levels of circulating angiotensin II
All AT1 receptor blockers have a long-term antihypertensive effect that lasts for 24 hours. It manifests itself after 2-4 weeks of therapy and reaches a maximum by the 6-8th week of treatment. Most drugs have a dose-dependent reduction in blood pressure. They do not disrupt his normal daily rhythm. Available clinical observations indicate that with long-term administration of angiotensin receptor blockers (for 2 years or more), resistance to their action does not develop. Canceling treatment does not lead to a rebound increase in blood pressure. AT1 receptor blockers do not reduce blood pressure if it is within normal limits.
When compared with antihypertensive drugs of other classes, it was noted that AT1 receptor blockers, while providing a similar antihypertensive effect, cause fewer side effects and are better tolerated by patients.
Action on the myocardium
A decrease in blood pressure when using AT1 receptor blockers is not accompanied by an increase in heart rate. This may be due to both a decrease in peripheral sympathetic activity and the central effect of drugs due to inhibition of the activity of the tissue unit of the renin-angiotensin system at the level of brain structures.
Particularly important is the blockade of the activity of this system directly in the myocardium and vascular wall, which contributes to the regression of myocardial and vascular wall hypertrophy. AT1 receptor blockers not only inhibit growth factors, the action of which is mediated through activation of AT1 receptors, but also act on AT2 receptors. Suppression of AT1 receptors promotes increased stimulation of AT2 receptors due to an increase in the content of angiotensin II in the blood plasma. Stimulation of AT2 receptors slows down the processes of growth and hyperplasia of vascular smooth muscles and endothelial cells, and also suppresses collagen synthesis by fibroblasts.
The effect of AT1 receptor blockers on the processes of myocardial hypertrophy and remodeling is of therapeutic importance in the treatment of ischemic and hypertensive cardiomyopathy, as well as cardiosclerosis in patients with coronary artery disease. Experimental studies have shown that drugs of this class increase coronary reserve. This is due to the fact that fluctuations in coronary blood flow depend on coronary vascular tone, diastolic perfusion pressure, and LV end-diastolic pressure—factors modulated by angiotensin II antagonists. AT1 receptor blockers also neutralize the participation of angiotensin II in the processes of atherogenesis, reducing atherosclerotic damage to heart vessels.
Effect on the kidneys
The kidneys are a target organ for hypertension, the function of which is significantly affected by AT1 receptor blockers. Blockade of AT1 receptors in the kidneys reduces the tone of efferent arterioles and increases renal plasma flow. At the same time, the glomerular filtration rate does not change or increases.
AT1 receptor blockers, promoting dilatation of efferent renal arterioles and reducing intraglomerular pressure, as well as suppressing the renal effects of angiotensin II (increased sodium reabsorption, dysfunction of mesangial cells, activation of glomerular sclerosis), prevent the progression of renal failure. By selectively reducing the tone of efferent arterioles and, consequently, reducing intraglomerular pressure, the drugs reduce proteinuria in patients with hypertensive and diabetic nephropathy.
However, it must be remembered that in patients with unilateral renal artery stenosis, AT1 receptor blockers can cause an increase in plasma creatinine levels and acute renal failure.
Blockade of AT receptors has a moderate natriuretic effect through direct suppression of sodium reabsorption in the proximal tubule, as well as due to inhibition of aldosterone synthesis and release. A decrease in aldosterone-mediated sodium reabsorption in the distal tubule contributes to some of the diuretic effect.
Losartan, the only AT1 receptor blocker, has a dose-dependent uricosuric effect. This effect is independent of the activity of the renin-angiotensin system and the use of table salt. Its mechanism is not yet completely clear.
Nervous system
AT-receptor blockers slow down neurotransmission by inhibiting peripheral sympathetic activity through blockade of presynaptic adrenergic receptors. During experimental intracerebral administration of drugs, central sympathetic responses are suppressed at the level of the paraventricular nuclei. As a result of the effect on the central nervous system, the release of vasopressin is reduced and the feeling of thirst is reduced.
Summing up
Maintaining your health is the personal responsibility of every person. And the older you are, the more effort you will have to put into this. However, the pharmaceutical industry provides invaluable assistance in this regard, constantly working to create better and more effective drugs. The angiotensin 2 receptor blockers discussed in this article are also actively used in the fight against cardiovascular diseases. The drugs, the list of which was given and discussed in detail in this article, should be used and applied as prescribed by the attending physician who is well acquainted with the current the patient’s health condition, and only under his constant supervision. Among these drugs are Losartan, Eprosartan, Irbesartan, Telmisartan, Valsartan and Candesartan. The drugs in question are prescribed only in the following cases: in the presence of hypertension, nephropathy and heart failure.
If you want to start self-medicating, it is important to remember the dangers associated with this. Firstly, when using the medications in question, it is important to strictly follow the dosage and adjust it from time to time depending on the current condition of the patient. Only a professional can carry out all these procedures correctly. Since only the attending physician can, based on the examination and test results, prescribe appropriate dosages and accurately formulate a treatment regimen. After all, therapy will be effective only if the patient adheres to the doctor’s recommendations.
On the other hand, it is important to do your best to improve your own physical condition by following the rules of a healthy lifestyle. Such patients need to properly adjust their sleep and wakefulness patterns, maintain fluid balance, and also adjust their eating habits (after all, poor-quality nutrition that does not provide the body with a sufficient amount of essential nutrients will not allow it to recover in a normal rhythm).
Choose quality medicines. Take care of yourself and your loved ones. Be healthy!
Blockers of the renin-angiotensin-aldosterone system
Angiotensin-converting enzyme inhibitors (ACEIs), angiotensin II receptor antagonists (ARAs), and aldosterone antagonists have proven efficacy in secondary prevention in patients with myocardial infarction.
of ACE inhibitors is currently recommended
in all patients (
class of recommendations II a, level of evidence A
), especially (
class of recommendations I, level of evidence A):
1. with a left ventricular ejection fraction of 40% or less,
2. with the heart failure clinic,
3. diabetes,
4. arterial hypertension,
5. chronic kidney disease,
6. myocardial infarction in the area of the anterior wall of the left ventricle.
Before starting treatment with ACE inhibitors, it is necessary to ensure that the patient does not have:
1. intolerance to this class of drugs (cough, angioedema);
2. bilateral stenosis of the renal arteries;
3. pregnancy or planning it;
4. potassium content in the blood is more than 5.0 mmol/l;
5. renal failure: blood creatinine content more than 221 mmol/l or a decrease in glomerular filtration rate less than 30 ml/min/1.73 m²;
6. systolic blood pressure less than 90 mm Hg. Art.
Reception begins with minimal doses, which are doubled at intervals of at least 2 weeks to the so-called “target” doses that have shown effectiveness in randomized trials, or the maximum tolerated doses (Table 9).
Table 9.
Recommended doses of ACE inhibitors
| Drugs | Dose, mg | |
| Starting | Target | |
| Enalapril | 2.5×2r/d | 10–20×2 rubles/day |
| Lisinopril | 2.5–5×1r/d | 20–35×1r/d |
| Ramipril | 2.5×1r/d | 5×2r/d |
| Trandolapril | 0.5×1r/d | 4×1r/d |
Adverse reactions to ACEIs are mainly cough (causing discontinuation in approximately 3% of cases), azotemia, hyperkalemia (causing discontinuation in 1.5% of cases) and hypotension, which leads to discontinuation of the drug in 4–5% of cases even when used correctly. To prevent hypotension from developing, simultaneous administration of drugs that lower blood pressure - nitrates, calcium antagonists (verapamil, diltiazem) should be avoided. If there are indications for these drugs, you can return to them after stabilization of blood pressure and the dose of ACEI. Also, before starting a course of treatment with ACE inhibitors, heavy diuresis and dehydration should be avoided. When treating ACE inhibitors, it is necessary to consider the patient's simultaneous use of:
1. Potassium-containing food additives, including low-salt products;
2. Potassium-sparing diuretics, including their combinations with furosemide, aldosterone antagonists;
3. Renin inhibitors (not indicated for heart failure);
4. Trimethoprim (risk of hyperkalemia);
5. Non-steroidal anti-inflammatory drugs - NSAIDs (reducing the effect of ACE inhibitors).
During treatment with ACE inhibitors, it is necessary to monitor the level of creatinine and potassium in the blood: 1–2 weeks after the start of titration and after its completion, then every 4 months. It is acceptable to increase the potassium content in the blood to 5.5 mmol/l and the creatinine content in the blood to 50% of the initial level or up to 266 mmol/l.
ARA
(valsartan, candesartan) are considered as an alternative to ACE inhibitors in patients with a left ventricular ejection fraction of 40% or less or clinical heart failure, especially if ACEIs are intolerant (
class of recommendations I, level of evidence B).
The drugs are contraindicated for hyperkalemia, renal failure, renal artery stenosis and are prescribed according to the same rules as ACE inhibitors. It is mandatory to achieve the maximum tolerated dose (Table 10).
Table 10.
Recommended doses of ARAs
| Drugs | Dose, mg | |||
| Starting | Starting for hypotension | Therapeutic | Maximum | |
| Candesartan | 4×1 r/d | 2×1r/d | 16×1r/d | 32×1r/d |
| Valsartan | 40×1r/d | 20×1r/d | 80×1r/d | 160×1r/d |
Combination therapy with ACE inhibitors and ARBs has not been sufficiently studied regarding effectiveness and is limited to patients with a left ventricular ejection fraction of 40% or less ( Class IIb recommendation, Level of evidence A).
Aldosterone antagonists
(Table 11) are recommended for patients after myocardial infarction with a left ventricular ejection fraction of 40% or less with clinical heart failure or diabetes without impaired renal function and/or hyperkalemia (
class of recommendations I
,
level of evidence B),
especially those who are already receiving therapeutic doses ACE inhibitors and β-blockers (class of recommendation I,
level of evidence
A).
Table 11.
Recommended doses of aldosterone antagonists
| Drugs | Dose, mg, 1 time per day | |||
| Starting | Regular | |||
| Together with IACE/ARA | Without ACEI/ARA | Together with IACE/ARA | Without ACEI/ARA | |
| Spironolactone | 12,5–25 | 50 | 50 | 100–200 |
| Eplerenone | 12,5–25 | 50 | 50 | 100–200 |
Side effects that complicate the use of aldosterone antagonists (painful gynecomastia, increased blood creatinine and hyperkalemia) develop when high (diuretic) doses are used. As a neurohormonal modulator, aldosterone antagonists are usually prescribed in small doses: 12.5–50 mg once daily. It must be remembered that the concentration of spironolactone in the blood plasma stabilizes by the third day of prescription and after discontinuation (or reduction of the drug dose), its effect disappears after three days. Gynecomastia requires discontinuation of medications.
Before starting therapy with aldosterone antagonists, it is necessary to ensure that the potassium level in the patient’s blood is not more than 5.0 mmol/l, and the creatinine level in the blood is not more than 221 mmol/l or the glomerular filtration rate is not reduced by less than 30 ml/min/1.73 m². In such situations, it is necessary to consider treating the patient together with a cardiologist or a CHF specialist.
When treating with aldosterone antagonists, it is necessary to take into account the patient's simultaneous intake of: potassium-containing food supplements, including low-salt foods; potassium-sparing diuretics, including their combinations with furosemide; ACE inhibitors or ARAs, renin inhibitors (not indicated for heart failure); trimethoprim (risk of hyperkalemia). Eplerenone is a strong inhibitor of cytochrome P450, so it can block the metabolism of a number of drugs: ketoconazole, intraconazole, nefazodone, telithromycin, clarithromycin, ritonavir, nelfinavir.
During treatment with aldosterone antagonists, it is necessary to monitor the level of creatinine and potassium in the blood: at the 1st, 4th, 8th, 12th week, 6th, 9th, 12th month after starting therapy or increasing the dose , then every 4 months. An increase in potassium levels in the blood above 5.5 mmol/l or a blood creatinine level of more than 221 mmol/l or a decrease in glomerular filtration rate of less than 30 ml/min/1.73 m² requires a reduction in the dose of the drug by half. If the potassium content in the blood increases above 6 mmol/l; or blood creatinine level more than 310 mmol/l; or glomerular filtration rate less than 20 ml/min/1.73 m², the drug must be discontinued immediately. The patient should avoid consuming potassium-containing salt supplements and take NSAIDs (nephrotoxicity) only as directed by a physician. If symptoms such as diarrhea, nausea, vomiting develop, the patient should stop taking aldosterone antagonists and consult a doctor. Due to the high risk of developing hyperkalemia, treatment of patients with a combination of ACE inhibitors, angiotensin II receptor antagonists and aldosterone antagonists is not recommended.
Statins
The goal of cholesterol-lowering therapy after myocardial infarction is to reduce low-density lipoprotein (LDL) levels to less than 1.8 mmol/L ( grade IIa recommendation, level of evidence C
), and non-high-density lipoprotein cholesterol (total cholesterol minus high-density lipoprotein cholesterol) less than 2.6 mmol/L, if the triglyceride level is 5.2 mmol/L or more (
Class IIa recommendation, Level of evidence B).
Before starting treatment, all patients should have a lipid profile ( grade I recommendation, level of evidence B)
). It should be remembered that in the acute period of a heart attack the patient’s usual cholesterol concentration decreases, so it is necessary to evaluate the lipid profile 4–6 weeks after ACS.
In order to monitor safety during statin therapy, it is necessary to initially determine the levels of liver enzymes: AST, ALT. Start with the lowest doses (Table 12). Every 4–6 weeks of treatment, the tolerability and safety of treatment are assessed (patient complaints, including myalgia, muscle weakness, repeated blood tests for lipids, AST, ALT, CPK). When titrating doses, they are primarily focused on tolerability and safety of treatment, and secondly, on achieving target lipid levels. If the activity of liver transaminases increases more than 3 upper limits of normal, it is necessary to repeat the blood test again. After achieving target levels, laboratory parameters are monitored once every 6 months.
Statin therapy is prescribed in the absence of contraindications and documented side effects in addition to a cholesterol-lowering diet and modification of other risk factors ( grade I recommendation, level of evidence A).
In patients intolerant to statins, the use of bile acid sequestrants and/or niacin is recommended (
Class IIa, Level of Evidence B
).
These same drugs should be added if statin therapy does not achieve the goal ( class of recommendation IIa, level of evidence B
).
The prescription of drugs that interfere with the absorption of cholesterol in the small intestine (ezetimibe) may be considered if statins, bile acid sequestrants, or niacin are ineffective ( class of recommendation IIb, level of evidence C
).
Patients with triglyceride levels greater than 13 mmol/L require fibrate therapy to prevent the development of acute pancreatitis ( Grade I recommendation, Level of evidence C
).
Fibrates may also be added when there is no response (total cholesterol minus high-density lipoprotein cholesterol less than 2.6 mmol/L) from adequate statin and niacin therapy ( Class IIb, Level of Evidence C).
Table 12.
Recommended doses of statins
| Medications | Doses |
| Rosuvastatin | 10–40 mg |
| Atorvastatin | 10–80 mg |
| Simvastatin | 10–40 mg |
| Pravastatin | 10–40 mg |
| Fluvastine | 20–80 mg |
Antianginal therapy
β-blockers, nitrates and long-acting calcium antagonists prevent and/or relieve attacks of angina pectoris (myocardial ischemia), improve the well-being of patients and increase exercise tolerance.
While β-blockers have been shown to improve survival in patients after myocardial infarction and are therefore recommended for all patients as secondary prevention, nitrates and long-acting calcium antagonists are recommended only when the anti-ischemic effect of β-blockers is insufficient.
Calcium antagonists
, along with beta-blockers, are first-line drugs for controlling heart rate and ischemic symptoms (
grade I recommendation, level of evidence B
). The mechanism of the anti-ischemic action of dihydropyridine calcium antagonists (Table 13) is associated with peripheral vasodilation and, thus, a decrease in vascular resistance (afterload on the heart). Currently, it is recommended to use only long-acting dosage forms taken once a day.
Table 13.
Recommended doses of calcium antagonists
| Drugs | Daily therapeutic doses, mg |
| Dihydropyridine | |
| Nifedipine | 30–120 |
| Amlodipine | 5–10 |
| Felodipin | 5–10 |
| Isradipin | 2,5–10 |
| Lacidipine | 2–4 |
| Non-dihydropyridine | |
| Verapamil | 120–480 |
Currently, three drugs from the nitrate
- nitroglycerin, isosorbide dinitrate and isosorbide-5-mononitrate (Table 14).
There are no fundamental differences in their pharmacological action. From the point of view of practical use, nitrates are divided into drugs with short (<1 hour) ( class of recommendations I, level of evidence B
), medium (<6 hours) and long (6–24 hours) action. With regular use of nitrates, the anti-ischemic effect fades, so they should be prescribed in such a way as to ensure a period during the day free from the action of the drug: at least 8-10 hours.
If short-acting nitrates are recommended for all patients to relieve symptoms of angina pectoris ( class of recommendation I, level of evidence B
), then intermediate- and long-acting drugs should be used only as a second line, after beta-blockers and calcium antagonists, to control heart rate and ischemic symptoms (
grade IIa recommendation, level of evidence B
).
Long-acting nitrates are prescribed once a day in the morning, medium-acting nitrates are prescribed 2 times a day (morning and afternoon).
Table 14.
Recommended doses of nitrates
| Drugs | Daily therapeutic doses, mg |
| Nitroglycerine | 0.3–1.5 under the tongue |
| Isosorbide dinitrate | |
| short acting | 1.25–3.75 sublingually |
| medium action | 20–80 |
| long acting | 40–120 |
| Isosorbide-5-mononitrate | |
| medium action | 40–120 |
| long acting | 40–240 |
Nitrates often cause side effects (headache), addiction, rebound syndrome with sudden withdrawal after long-term regular use.
For angina pectoris class I, short-acting nitrates are prescribed 5–10 minutes before the expected exercise, which usually provokes an attack of angina. For class II exertional angina, you can also use intermediate-acting drugs. For class III–IV angina, long-acting isosorbide-5-mononitrate is prescribed.
Education
One of the most important aspects of successful treatment after myocardial infarction is education of the patient and his family (Class I recommendation, level of evidence
C). Its effectiveness has been demonstrated in numerous studies.
Group education of patients in a school format (“coronary clubs”) is advisable. A nurse specially trained in advanced training courses may be involved as a moderator.
The learning objectives are:
1. Informing the patient about the symptoms of the disease.
2. Overcoming bad habits and developing a healthy lifestyle.
3. Organization of physical activity and diet of patients.
4. Encouraging social activity.
5. Development of adequate stereotypes of behavior in difficult situations.
6. Automotive training and social skills training.
7. Readaptation of the patient in the family and society.
8. Changing attitudes and value orientations.
The main goal of training is to create, maintain and strengthen motivation for active participation in the rehabilitation program. During the classes, participants are encouraged to ask questions, express opinions, share experiences, that is, actively participate in the discussion of the problem. All patients should be provided with educational material; before handing it over, it is necessary to review each point of the recommendations together with the patient.
Recommendations are mandatory to avoid those types of physical activity or any other activity that provokes an attack. The patient is explained the need for prophylactic use of nitro drugs, as well as the principles of relieving a pain attack. Inform the patient about the side effects of these medications so that he or she can lie down or sit down after using them to avoid hypotension. Information about the symptoms of ACS and the duration of pain that requires immediate medical attention is required in order to reduce the time before hospitalization.
Knowledge about the disease and existing treatment methods is a common and most important factor influencing the patient's compliance with recommendations.
Employment
After a myocardial infarction, the patient is temporarily disabled. The patient's period of incapacity for work is determined depending on the depth, location of myocardial damage and the presence of complications (Table 15).
Table 15.
Approximate duration of temporary disability
| Type of heart attack | Features of the flow | Length of incapacity for work (days) |
| Acute transmural (synonyms: penetrating, large focal, with Q wave) infarction of the anterior myocardial wall | Without complications with mild anginal syndrome | 70–90 |
| With complications of the acute period | 90–130 | |
| Acute transmural infarction of the inferior wall of the myocardium | Without complications with mild anginal syndrome | 70–90 |
| With complications of the acute period | 90–130 | |
| Acute transmural myocardial infarction of other locations | Without complications with mild anginal syndrome | 70–90 |
| With complications of the acute period | 90–130 | |
| Acute subendocardial myocardial infarction | No complications | 60–70 |
| Heart failure FC I | 60–80 | |
| Heart failure FC II | 80–110 | |
| Heart failure FC III–IV | 90–120 | |
| Recurrent myocardial infarction | 90–120 | |
| Unstable angina | 10–14 | |
At the end of the period of temporary disability, based on a comprehensive assessment of the state of the cardiovascular system (EchoCG, Holter ECG monitoring), the presence of concomitant diseases and the results of assessing exercise tolerance (including stress testing), it is necessary to discuss with the patient the possibility of returning to work .
For patients after myocardial infarction, static loads are contraindicated: lifting and carrying heavy objects (the weight of the object being carried is limited by the functional class of the patient), working with arms raised up for a long time (for example, painting or washing the ceiling), working in an inclined position (washing the floor). and working in stuffy, hot conditions. physical activity after meals.
All patients with a history of MI are contraindicated in types of work related to:
1. a potential danger to people (drivers of public transport, freight transport, dispatchers at railways, power plants, airports).
2. constant walking during the working day (postal workers, couriers, salespeople, machine operators).
3. working away from populated areas in the field (geologists, builders).
4. the need to stay in unfavorable microclimatic or meteorological conditions during working hours.
5. maintenance of electrical installations.
6. work on the night shift (watchman, security guard) or daily duty.
7. a strictly set pace of work (telephone operators, work on machines and conveyors).
8. high-altitude work (crane operator, steeplejack).
9. exposure to vascular and neurotropic toxic substances, poisons (production of cigarettes, work with benzene, lead, carbon monoxide).
10. air transport (pilots, flight mechanics, flight attendants).
If there is no prospect of the patient returning to his usual work activity, it is necessary to refer him to the bureau of medical and social examination to determine the degree of restriction to work activity for the purpose of rational employment.
Dispensary observation
All patients after myocardial infarction, regardless of age and the presence of concomitant diseases, should be registered at the dispensary as a high-risk group for sudden death and the development of cardiovascular complications.
The frequency of visits to the doctor is at least once a month at the beginning of observation, and once every 6 months after stabilization of the condition and selection of adequate drug therapy. The examination includes: examination of the patient with determination of BMI and waist circumference, fundus examination, ECG, lipid profile, fasting blood glucose, creatinine and glomerular filtration rate.
6. Consultations with specialists:
Cardiac surgeon
- to resolve the issue of myocardial revascularization if indicated:
1. Transient changes of an ischemic nature, recorded on a resting ECG or according to Holter ECG monitoring.
2. Attacks of angina pectoris and rest during antianginal therapy.
3. Post-infarction angina (up to 1 month after a heart attack).
4. Ventricular tachyarrhythmias (class of recommendations I, level of evidence C).
5. Stable angina pectoris class III–IV, especially in the absence of an adequate response to drug therapy ( class of recommendations I, level of evidence C
).
6. Drug therapy does not provide satisfactory control of symptoms.
7. Non-invasive methods demonstrate the presence of a widespread area of ischemia.
8. The patient prefers invasive treatment.
9.
The occurrence of class III–IV angina after revascularization (
recommendation class I, level of evidence C).
Cardiologist
- in the presence of concomitant diseases that limit the selection of drug therapy. in the presence of severe heart failure. with concomitant severe arterial hypertension. for the selection of antiarrhythmic therapy in the presence of complications in the form of rhythm disturbances. with dyslipidemia refractory to treatment or its familial forms.
Arrhythmologist
- if coronary artery disease is complicated by rhythm disturbances requiring the installation of additional intracardial devices or invasive diagnostic procedures.
Endocrinologist
- with concomitant severe diabetes mellitus. with severe obesity.
Psychiatrist
- if correction of the psychological status is required, the patient has anxiety, depression, hostility.
Nutritionist
- if there are difficulties in choosing a diet.
7. Indications for hospitalization:
1. Post-infarction angina (developed within 1 month of myocardial infarction).
2. Progressive angina pectoris (increased frequency, intensity, duration of anginal attacks, the occurrence of attacks during lower intensity loads).
Bibliography
1.
Guide to outpatient cardiology / ed. Yu.N. Belenkova, R.G. Oganova. - M.: GEOTAR-Media, 2007. - 400 p.
2. Estimated periods of temporary disability for the most common diseases and injuries (in accordance with ICD-10). Recommendations for heads of medical institutions and attending physicians, specialist doctors of the executive bodies of the Social Insurance Fund of the Russian Federation (approved by the Ministry of Health of the Russian Federation and the Social Insurance Fund of the Russian Federation dated August 21, 2000 No. 2510/9362-34, 02-08/10- 1977P).
3.
ESC Guidelines on the management of stable coronary artery disease. Eur Heart J 2013); 34:2949–3003.
4. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2012; 33:2569–619.
5. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J 2011; 32:2999–3054.
6. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients with Coronary and other Atherosclerotic Vascular Disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation 2011; 124:2458–73.
7. ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: Executive Summary.Circulation 2013;127:529–55.
8. ACCF/AHA Focused Update Incorporated Into the ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction. Circulation 201; 123:e426–579.
9. General medical practice: national guide in 2 volumes / ed. I.N. Denisova, O.M. Lesnyak. - M.: GEOTAR-Media, 2013. - 1864 p.
10. Diagnosis and treatment of patients with acute myocardial infarction with elevation of the ST segment of the ECG // “Cardiovascular Therapy and Prevention” 2007.― No. 6 (8), Appendix 1