© Author: Sazykina Oksana Yuryevna, cardiologist, especially for SosudInfo.ru (about the authors)
Currently, medicine is actively developing, and invasive diagnostic and treatment methods are widespread and accessible to any patient population. One such technique is stenting of neck vessels – the carotid arteries.
The carotid arteries are the main vessels bringing blood to the brain. The common carotid arteries (right and left) run along the neck and at the level of the base of the skull are divided into internal and external parts. The outer part supplies blood to the soft tissues of the skull, but the inner part penetrates the cranial cavity and takes part in the formation of the Circle of Willis - this is the main link in the blood circulation of the brain.
Thus, the carotid artery is a vital vessel, because if its lumen is blocked, even on just one side, irreversible consequences occur in the brain, often leading to death. The lumen of the artery is blocked either by a blood clot or an unstable atherosclerotic plaque, then certain areas of the brain experience acute hypoxia, its tissues die - brain necrosis is formed. This condition is called acute cerebrovascular accident (ACVA, stroke) of the ischemic type. Even if the patient survives the stroke (which most often happens), then in most cases he remains deeply disabled with impaired motor, speech, swallowing and other body functions. That is why it is so important to prevent blockage of the carotid artery and to perform an operation to clear the lumen in time if atherosclerosis has already affected the carotid arteries.
Briefly about atherosclerosis
Atherosclerosis, in principle, is not strictly localized, since the deposition of plaques consisting of harmful cholesterol can occur in any part of the bloodstream. But the most dangerous localizations are considered to be the arteries of the brain, coronary (“heart”) arteries and arteries of the lower extremities. It is problems in these vessels that lead to strokes, heart attacks and gangrene of the lower extremities with subsequent amputation.
atherosclerotic plaque of the carotid artery, obstructing blood supply to the brain
The development of atherosclerosis is caused by excess cholesterol in the blood, followed by its deposition in the form of plaques on the inner lining of the artery. Based on this, doctors prescribe lipid-lowering drugs (statins, fibrates) in combination with diet to patients with high cholesterol levels. However, what to do if the plaque has already blocked the lumen of the artery completely or partially? In this case, medications alone cannot be used, and the doctor, based on the examination results, decides on the need for surgical intervention.
Recovery after
The patient must be under constant medical supervision for the first time after completion of the operation. Blood pressure indicators, the state of the central nervous system, and the site of arterial catheterization are monitored. Strict bed rest is required for several hours. Restriction of physical activity usually lasts about a day, then the patient is transferred to the general ward and discharged after stabilization of the condition.
At home you need:
- take medications to reduce blood clotting - Aspirin, Deplatte;
- dosed physical activity in the first two months;
- avoid lifting heavy objects and stressful situations;
- stop smoking and drinking alcohol;
- limit your diet to table salt, fatty meat, butter, cottage cheese above 5% fat, confectionery, coffee and strong tea;
- drink about 1.5 liters of water per day if there is no swelling;
- maintain normal body weight;
- do not take a hot shower or bath, or visit a bathhouse or sauna.
It is necessary to regularly undergo examinations for glucose and cholesterol levels in the blood, determine coagulation parameters, and measure blood pressure and pulse daily.
Such alarming symptoms include:
- sudden numbness of the arm and/or leg;
- visual impairment;
- attack of headache with nausea and vomiting;
- unsteady gait;
- dizziness;
- severe weakness;
- fainting;
- slurred speech;
- change in facial expressions.
The essence of the method, its advantages and disadvantages
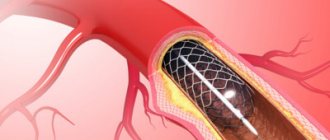
A technique such as stenting has proven itself to be a minimally invasive vascular intervention that can reduce the risk of strokes in patients with atherosclerosis. The essence of this operation is that a miniature stent is placed through endovascular (intravascular) access to the area of the carotid artery affected by the plaque, which mechanically affects the soft plaque, partially destroying it and eliminating the obstruction to blood flow.
installation of a stent in the carotid artery
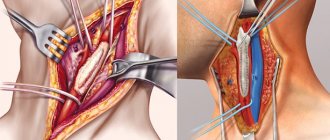
There is another intervention on the carotid artery - carotid endarterectomy. This treatment method is also common as a treatment for atherosclerosis of the carotid arteries, but it is a more invasive intervention, since the affected part of the vessel is removed from the side of the neck, with dissection of its soft tissue. Recently, preference has been given to endovascular stenting, since this technique has significant advantages.
First of all, stenting is a virtually “bloodless” operation and can be performed under local anesthesia only at the site where the catheter is inserted into the vascular bed (usually the femoral artery). In this regard, operational stress on the body is minimized. After such an intervention, the patient’s rehabilitation occurs faster, and there is no need for a long stay in the hospital. In addition, during the operation the carotid artery is not compressed, as in the case of open surgery, and accordingly, the risk of complications from intraoperative brain hypoxia is greatly reduced.
On the other hand, this technique, being relatively new, does not have a sufficient evidence base for long-term favorable results of the operation. In some cases, complications are possible, and some patients may require repeated intervention several years later. Repeated surgery, in turn, is often accompanied by complications and may not always lead to complete restoration of the lumen of the carotid artery.
However, it is intravascular intervention that is currently recognized as a well-tolerated method of treating carotid atherosclerosis, since complications after it are very rare.
Video: animation of the carotid artery stenting process
Risks of Angioplasty and Stenting
Complications can occur with any medical procedure. Here are some of the possible complications of carotid angioplasty and stenting:
- Stroke or mini-stroke (transient ischemic attack or TIA) . During angioplasty, blood clots that may form on the catheters can break free and travel to your brain. You will receive blood thinners during the procedure to reduce this risk. A special trap filter is used for these procedures, but the risk is associated with placing it after the catheter has passed the narrowing site.
- New narrowing of the carotid artery (restenosis) . The main disadvantage of carotid angioplasty is the likelihood that your artery will narrow again within a few months of the procedure. Special drug-eluting stents have been developed to reduce the risk of restenosis.
- Blood clots . Blood clots can form in stents even weeks or months after angioplasty. These clots can cause stroke or death. It is important to take aspirin, clopidogrel (Plavix), and other medications exactly as prescribed to reduce the chance of clots forming in your stent.
- Bleeding . You may have bleeding at the injection site. Usually this simply results in a hematoma, but sometimes serious bleeding occurs and blood transfusions or surgical procedures may be required.
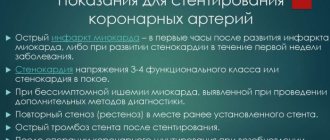
Indications for carotid artery stenting surgery
Carotid stenting is indicated for patients with arterial stenosis greater than 60%. This means that more than half the lumen of the vessel is blocked by a plaque, which at any moment can become unstable, detach from the inner lining of the vessel and migrate into a vessel with a narrower lumen, blocking it completely. In addition, blood clots easily settle on such a plaque, and even if the plaque does not come off, a large blood clot forms on it, which can also completely block the blood flow.
Indications for surgery are determined based on the results of instrumental diagnostic methods - carotid ultrasound with Doppler, angiography, CT and MRI with contrast of the vascular bed of the neck. Usually, for accurate visualization of a plaque in the lumen of an artery, ultrasound and Doppler examination in combination with angiography of neck vessels is sufficient (the first method assesses the location and size of the plaque, the second - the degree of disturbance of blood flow in the lumen of the vessel).
How is cerebral stenting performed?
The operation is most often performed under local anesthesia to maintain contact with the patient. Monitoring the progress of stenting is carried out using Doppler ultrasound and measuring blood pressure.
Through a puncture of the femoral artery, a catheter is inserted into the vascular bed, at the end of which a balloon is attached. Contrast is pumped into it and the vessels are examined on a monitor. After reaching the desired area, the balloon is expanded, and a special trap is placed above it, which will protect the brain vessels from emboli during stenting.
The main stage is the installation of a frame, which independently straightens and presses the plaque. At this time, blood flow is restored. The stent holds the artery in an expanded position, which improves the supply of arterial blood to the brain and prevents the development of ischemia. The average duration of the operation is two hours.
When is carotid stenting contraindicated?
Like any surgical intervention, this technique is contraindicated in the following categories of patients:
- With severe chronic diseases in the decompensation stage (bronchial asthma, diabetes mellitus, chronic heart failure),
- With acute illnesses suffered in the previous two months - myocardial infarction, stroke, acute infectious diseases),
- With total stenosis of the carotid artery,
- If you have an existing allergy to a radiocontrast agent used for vascular interventions,
- With existing contraindications for taking anticoagulants and antiplatelet agents (warfarin, aspirin), since these are the drugs prescribed to prevent complications after the intervention.
All indications and contraindications should be interpreted only by the attending physician, and not by the patient himself, because in each specific case the risk/benefit ratio for a particular patient must be correctly assessed.
Risk factors for complications of carotid stenting
These factors include:
- High blood pressure;
- Allergy to X-ray contrast agents;
- Calcification (impregnation with lime) and large-scale narrowing of the carotid arteries;
- Sharp bends and other anatomical features leading to difficulties in stent placement;
- Plaques of significant size, or atherosclerosis of the aorta in the area of the beginning of the carotid arteries;
- Age over 80 years;
- Concomitant blockages of the arteries of the vessels of the arms and legs.
Preparing for surgery
Carotid stenting is always performed only as planned, after a thorough examination of the patient. Within two weeks before surgery, the patient needs to undergo the following studies (except for the main examination of the carotid arteries - Doppler and angiography):
- General and biochemical blood test,
- Blood tests for HIV, syphilis and viral hepatitis,
- X-rays of the chest organs,
- Electrocardiograms,
- Analysis of the blood coagulation system (with determination of MCV, PTI, APTT and PTT),
- If necessary, echocardioscopy (ultrasound of the heart).
5-7 days before the operation, the patient is prescribed antiplatelet agents (to prevent thrombus formation in the bloodstream) - aspirin Cardio, Cardiomagnyl, acecardol, ThromboAss, etc.
Planned hospitalization is carried out two to three days before surgery. The evening before and on the day of surgery, the patient is prohibited from eating. Before entering the operating room, the patient may be given light premedication with intravenous sedatives.
Rehabilitation
Rehabilitation after carotid artery stenting requires compliance with certain rules:
- It is necessary to give up physical activity.
- You should not lift heavy objects.
- See a doctor immediately if you suspect an ischemic stroke. This pathological condition is characterized by an unsteady gait, numbness on one side of the body, and headache.
- Quit smoking and alcohol.
- Take drugs from the group of antiplatelet drugs.
- Drink enough liquid.
- Avoid thermal procedures.
Proper nutrition plays an important role in the recovery process after surgery. It is necessary to balance your diet by eliminating all foods that can increase cholesterol. To do this, you should give preference to vegetable fiber and dishes with a minimum amount of fat and give up fast food, processed foods, etc. It is necessary to avoid stress and emotional turmoil.
After surgery, patients must take medications that affect blood clotting throughout their lives. This measure is necessary in order to reduce the risk of recurrent thrombosis. Additionally, after recovery, people who have undergone stenting are recommended to engage in physical therapy that does not involve heavy loads.
Operation technique
After the patient is admitted to the cath lab, he is placed on the operating room table. First, the femoral artery is accessed under local anesthesia in the groin area. To do this, make a thin incision or puncture in the skin of the specified area. Then an introducer is inserted into the artery - a conductor, through which access to the carotid artery will be provided.
introducer
A radiopaque substance is injected into the vascular bed and an X-ray of the neck area is taken to clarify the location of the stenosis. After this, a kind of basket is brought to the carotid artery through an introducer, closer to the brain, that is, further than the stenosis. This is necessary to protect the brain from pieces of plaque or blood clots that appear during the operation entering its vessels.
After installing the brain protection system, a stent is inserted into the lumen of the vessel under X-ray control in real time. It resembles a compressed spring, which then straightens out and is firmly pressed into the vascular wall. In order for the stent to fit more firmly into the place of the stenosis, a miniature balloon is brought to it, which is inflated in the lumen of the stent. This is the stage of balloon angioplasty.
angioplasty (1) and stent placement (2)
After a control X-ray of the neck is taken, it is checked whether the stent is installed in the correct place, and if everything is in order, the introducer and brain protection system are removed. The entire procedure takes no more than 1-2 hours, without causing significant pain in the patient. The patient is conscious and able to follow the doctor's commands. More often, the patient is given a rubber ball, which he squeezes at the surgeon’s request. This is necessary so that the doctor can notice in time if the patient has a violation of motor functions.
Video: progress of carotid artery stenting operations
What alternative methods of treating atherosclerosis of the carotid arteries without anesthesia exist?
First of all, this is the operation of carotid endarterectomy under local anesthesia. Currently, experience in the use of this type of treatment is still accumulating, but several shortcomings are obvious, which do not yet allow it to gain a strong foothold in the arsenal of vascular surgeons.
First, and most importantly, patients are afraid of performing carotid endarterectomy itself under local anesthesia. When performing local anesthesia, there are complaints of discomfort and a feeling of fullness and even pain in the neck during conduction anesthesia. Based on the fear of experiencing such sensations, patients have a natural psychological reaction of rejection of this intervention as a type of treatment.
The second is that when performing an operation, a non-standard situation may arise that requires an increase in the duration of the operation, spending time on repeated local anesthesia or switching to intubation anesthesia. As a result, both the patient and the surgeon operating on him become “nervous.”
Constantly being conscious, the patient, when the carotid arteries are compressed, may feel quite unpleasant sensations, in the form of paresthesia in the limbs, blurred vision, and even loss of consciousness. This may be perceived by the patient as something wrong or bad. This is the third drawback.
However, there are undeniable advantages of this method, which you can read about in the article: “ Carotid endarterectomy under local anesthesia .”
A situation has arisen when the patient refuses open surgery, and the surgeon is not ready to take responsibility due to the high risk of complications and death of the patient with severe concomitant pathology. This gave impetus to the development of a new direction in carotid artery surgery, its name is Endovascular balloon angioplasty and carotid artery stenting.
What types of stents are there?
A stent is a thin metal frame structure capable of opening and taking the shape of the vessel in which it is installed. Currently, there are more than 300 stent models, but they all have a number of features:
- spring mechanism,
- Mesh design,
- shape memory,
- Coating with a medicinal substance that prevents the formation of blood clots (anticoagulant) or a cytostatic agent that prevents the proliferation of connective tissue,
- No deformation,
- No inflammation at the implantation site.
Stenting - what is it?
The essence of the intervention comes down to the introduction of a special frame (stent) into the lumen of a narrowed vessel, which no longer allows it to change its size. Stents are made of a special metal or plastic that does not attract blood clotting factors and cannot be complicated by thrombosis. This is a kind of cylinder with a solid, mesh, or wall made of rings. It is straightened with the help of an inflated balloon, on which, in fact, it is brought to the place of narrowing. But there are also self-expanding stents.
In addition, implants with medicinal spraying have been developed. Antiplatelet agents and immunosuppressants are used as medicine. They further reduce the risk of thrombus formation on the inner surface of the stent and inhibit the immune response to a foreign body. But the most recent innovation is biodegradable frames, which begin to gradually dissolve six months after installation. Nevertheless, specialists from Switzerland, who closely study the long-term results of stenting with different materials, have recognized drug-eluting intravascular stents as the best to date.
Arterial stenting is a fairly simple procedure for trained angiosurgeons. They all perform the same algorithm of actions.
- First, a peripheral vessel is selected through which the stent will be inserted. Usually this is the femoral, brachial or radial artery.
- The place in its projection is treated with an antiseptic. A local anesthetic is injected, for which an allergy test was previously carried out.
- Then the vessel is punctured, a catheter is installed into it, into which a conductor with a balloon is inserted.
- An antiplatelet agent is injected before it, usually Heparin. Then - a contrast agent. Both drugs are picked up by the blood and outpace the balloon, thinning the blood and filling the lumen of the artery, which becomes visible under fluoroscopy.
- The balloon, under the control of an X-ray machine, is brought to the narrowed area, and a temporary filter emerges from it to catch accidentally detached elements of the atherosclerotic plaque and blood clots. The balloon then inflates, compressing atherosclerotic plaques and expanding the lumen of the artery.
- After dilation of the vessel, the balloon is deflated, and the conductor with it and the temporary filter are removed.
- Then a second conductor with a stent fixed on a balloon is brought to the mechanically expanded vascular segment.
- The balloon slowly inflates, straightening the metal frame, pressing the plaque against the vascular wall, and expanding the lumen. The frame fixes atheromatous masses, preventing them from entering the general bloodstream.
- After fixing the implant to finally strengthen it in place, the balloon is deflated and inflated several times and removed from the vascular bed.
- The catheter is also removed.
- The surgical site is treated with an antiseptic, and a pressure bandage is applied to the wound. Sometimes a single interrupted suture may be required.
The implant remains in the human body forever, its shape does not change, and it promotes normal blood supply to the corresponding tissues for life. Gradually, the inner surface of the stent becomes covered with proliferating cells of the vascular lining, and the immune system does not recognize the foreign body. In arteries prone to excessive growth of the inner lining, and, consequently, to the re-emergence of atherosclerotic plaque, an implant with an appropriate drug coating is inserted. It prevents the growth and new formation of endothelium. Without the use of such new generation scaffolds, relapse would occur in 20% of cases, and the lumen of the artery would narrow again.
The number of stents, their size and type are determined by the angiosurgeon depending on the specific situation:
- number of affected vessels requiring stenting;
- length of the stenotic area;
- degree of narrowing of the arterial lumen;
- the ability of the inner membrane to hyperplasia.
The condition after stenting has found its place in the International Classification of Diseases and has its own code according to the ICD 10 revision - Z 95.5. This suggests that it plays an important role in medicine, preventing the fatal complications of atherosclerosis, and increasing the life expectancy of operated patients. Thanks to percutaneous coronary intervention (PCI), stenting of the precerebral, renal arteries, vessels of the lower extremities, and aorta, the mortality rate from myocardial infarction, stroke, gangrene and aneurysm rupture has decreased significantly.
There are cases when stenting is not necessary and only balloon angioplasty is indicated for patients. This is a similar method of surgical intervention in which the vascular lumen is enlarged by inflating a balloon without subsequent implantation of a stent. But in this situation, without the patient following the doctor’s instructions, there is a risk of relapse. Then doctors perform angioplasty again, or, if there are no contraindications, prescribe stenting.
Installing another frame in the place of an existing one is impossible: the implant is designed to perform its functions throughout life. Repeated stenting is indicated when atherosclerosis progresses in other areas of the vascular bed, including those located far from the site of the first surgical intervention. In case of advanced changes in the vascular wall and the impossibility of implanting a frame, a more traumatic operation is performed - bypass surgery.
Are there any complications?
Complications after this technique develop extremely rarely, in approximately 0.5% of cases. In this case, all complications can be divided into complications in the early postoperative period and long-term adverse consequences.
So, the first group includes:
- Embolism of cerebral vessels due to destroyed plaque particles or blood clots. Complications of this kind can be prevented by taking antiplatelet agents and anticoagulants before and after surgery, as well as installing a brain protection system (like a blood clot trap).
- An allergic reaction to a radiopaque substance, up to anaphylactic shock and acute renal failure. Prevention includes a thorough collection of allergy history from the patient before surgery, as well as an allergy test with a substance.
From the second group of complications, the following should be noted:
- Formation of restenosis. Repeated narrowing of the lumen of the carotid artery is due to the fact that over time, the stretched wall of the vessel, due to its elastic properties, tends to take its original position in a narrowed form. If this condition occurs, repeat surgery to replace the stent may be required.
- Stent thrombosis. It is also rare, and its prevention is the constant use of anticoagulants and antiplatelet agents (if there are no contraindications).
Indications
Carotid artery stenting is required for patients who may experience serious complications from endarterectomy. The high risk of side effects forces us to resort to stenting techniques, as they are safer. The procedure is indicated for patients with significant narrowing of the lumen of the carotid arteries, with signs of microstroke and stroke. The operation is also performed in cases where there are no symptoms of cerebrovascular accident, but a significant narrowing is detected (more than 80%) and there is a high risk of complications after endartectomy.
Stenting is also performed in patients who have relapsed stenosis after a previous endartectomy.
Rehabilitation after surgery
carotid artery before and after stenting
After the intervention, the patient remains in the hospital for three days under the supervision of doctors. If the postoperative period proceeds without complications, the patient is discharged under the supervision of the outpatient service. In the first week after surgery, any physical activity is prohibited. In the future, the patient will need a diet that excludes foods that can increase blood cholesterol (fatty, fried foods, animal fats).
In the clinic at the place of residence, the patient needs to undergo an ultrasound of the neck vessels once a year to assess the patency of the stent. In addition, it is necessary to constantly take blood-thinning drugs, and depending on the level of blood cholesterol, lipid-lowering drugs.
Postoperative period
The patient is discharged on the 2nd day after surgery with a mandatory follow-up ultrasound scan.
After carotid artery stenting, combination antiplatelet therapy with clopidogrel 75 mg/day and aspirin 100 mg/day is prescribed for up to 12 months. Subsequently, aspirin and anti-cholesterol drugs - statins remain.
A control ultrasound scan is performed one month after stenting surgery. The patency of stented segments should be assessed at intervals of 6 months. If signs of restenosis are detected, the patient is prescribed a multislice computed tomography scan with contrast.
Forecast
The labor prognosis is determined based on the presence of concomitant diseases, as well as previous strokes. In the absence of previous strokes, the patient is not assigned disability after stenting, but a pronounced limitation of body functions after previous strokes is the basis for assigning the first or second disability group. In any case, the labor forecast is determined individually in each specific case.
The prognosis for life and health after surgery is favorable - complications develop extremely rarely, and the risk of strokes is minimized. However, the prognosis may be unfavorable if long-term consequences develop, since repeated surgery will be required, which is less tolerated by patients.
The image below shows a remote section of the carotid artery with a stent, on which an atherosclerotic plaque has re-formed, already six months after the stenting operation.
Methods
The analysis included 2544 individuals with carotid artery stenosis of 70% or more. Patients were randomized to receive stenting or endarterectomy in addition to standard therapy for cardiovascular risk factors.
The CREST study included 1091 patients (548 stenting, 543 endarterectomy), and the ACT I study included 1453 patients (1089 stenting, 364 endarterectomy). All patients were <80 years of age (the upper limit in the ACT I study) and were asymptomatic.
The researchers used the Kaplan-Meier method to evaluate the effect of age on treatment outcomes. Patients were divided into 3 age groups: <65 years, 65-74 years and 75+.
As a primary endpoint
We considered a composite of stroke, myocardial infarction, and death during the perioperative period or development of ipsilateral (same side as the stenosis) stroke within 4 years after randomization.
Cost of the operation
This intervention, like any X-ray surgical method of treating blood vessels, is possible under a quota within the compulsory medical insurance system. To do this, after establishing the indications for surgery, the attending physician refers the patient for a consultation with a vascular surgeon. If the decision about the operation is made, the doctor collects the necessary documents (examination results, discharge from the hospital, certificates of disability, if any) and sends a request to the regional divisions of the Ministry of Health. After receiving a positive decision from the nearest city or from a health care facility in the patient’s city that they are ready to accept the patient for surgery, the patient awaits a quota. The wait may last for several months, so if he has the opportunity to pay for treatment and stay in this health facility, it makes sense to use paid treatment.
The operation is possible in a multidisciplinary hospital in any large city, provided that this health care facility includes a department of x-ray surgical treatment methods and a department of vascular surgery, and also meets the standards of personnel and technical equipment. The cost of the operation varies from 60 thousand rubles to 200 thousand rubles. The patient must take into account not only the cost of the operation itself, but also the cost of bed days spent in the hospital. The attending physician will advise the patient on a more accurate cost for stenting neck vessels.
Indications for stenting of cerebral vessels
Expansion (balloon dilatation) and stenting are indicated in the presence of:
- narrowing of the artery lumen by more than half;
- contraindications to open or eversion plaque removal (endarterectomy), general anesthesia;
- repeated narrowing after surgery;
- frequent transient ischemic attacks;
- severe discirculatory encephalopathy;
- signs of stroke;
- radiation therapy or surgery in the neck area.
This method is more effective in middle age, and after 65 years, surgeons more often choose endarterectomy if there are no restrictions on its implementation.
And here is more information about atherosclerosis of the neck vessels.