Indications for stenting of coronary arteries
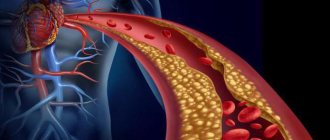
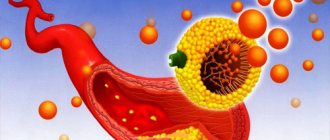
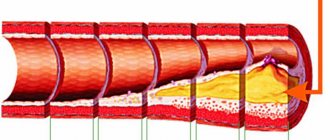
The main indications for endovascular intervention are narrowing of blood vessels due to atherosclerosis associated with atheromatous deposits on their internal walls. This leads to insufficient blood supply to the myocardium and oxygen starvation of its cells, ischemia.
To solve this problem, arterial stenting is performed when:
- ischemic disease and stable angina;
- atherosclerosis of the coronary arteries of the heart;
- atherosclerotic lesions of the coronary vessels;
- systemic vasculitis.
Installation of a stent in the vessels of the heart is carried out if the severity of ischemic symptoms does not decrease with the help of drug therapy and the condition cannot be stabilized.
Preparation and performance of the operation
Stenting can be performed urgently or routinely. In emergency surgery, coronary angiography (CAG) is first performed, based on the results of which a decision is immediately made to introduce a stent into the vessels. Preoperative preparation in this case comes down to the introduction of antiplatelet agents and anticoagulants into the patient’s body - drugs that prevent increased blood clotting (to avoid thrombosis). As a rule, heparin and/or clopidogrel (warfarin, Xarelto, etc.) are used.
Before a planned operation, the patient must perform the necessary research methods to clarify the degree of vascular damage, as well as assess the contractile activity of the myocardium, the ischemic zone, etc. For this, the patient is prescribed CAG, ultrasound of the heart (echocardioscopy), standard and stress ECG, transesophageal electrical stimulation myocardium (TEFI - transesophageal electrophysiological study). After all diagnostic methods have been completed, the patient is hospitalized in the clinic where the operation will be performed.
The evening before the operation, a light dinner is allowed. It is likely that some cardiac medications will need to be discontinued, but only as directed by the attending physician. Breakfast before surgery is not allowed.
Stenting itself is performed under local anesthesia. General anesthesia, dissection of the chest and sternum, and connection of the heart to a heart-lung machine (ACB) are not required. At the beginning of the operation, local anesthesia of the skin is performed in the projection of the femoral artery, which is accessed through a small incision. An introducer is inserted into the artery - a conductor, through which a catheter with a stent installed at the end is brought to the affected coronary artery. Under the control of X-ray equipment, the exact position of the stent at the site of stenosis is monitored.
Next, the balloon, which is always inside the stent in a compressed state, is inflated using air injection, and the stent, being a spring structure, is straightened out, tightly fixed in the lumen of the artery.
After this, the catheter with the balloon is removed, a tight aseptic dressing is applied to the skin incision, and the patient is transferred to the intensive care unit for further observation. The entire procedure lasts about three hours and is painless.
After stenting, the patient is observed for the first day in the intensive care unit, then transferred to a regular ward, where he remains for about 5-7 days until discharge from the hospital.
Video: stenting, medical animation
Contraindications
Coronary stenting of heart vessels is contraindicated in:
- acute cerebrovascular accident (stroke);
- diffuse cardiosclerosis;
- congestive (decompensated) heart failure of various etiologies;
- the presence of acute infectious diseases, including bacterial endocarditis;
- severe functional failure of the liver, kidneys or lungs;
- in the presence of extensive diffuse stenoses in one vessel.
In case of local internal bleeding with a bleeding disorder, stent placement is also contraindicated.
Types of stents. Features and Benefits
Stents are small, spring-loaded, expandable wire mesh tubes used to treat narrowed or weakened arteries in the body. In patients with coronary artery disease (CAD), the devices are used to open narrowed arteries and reduce symptoms such as chest pain from angina or to treat a heart attack.
Stents help prevent the artery from becoming blocked again (restenosis). The device is a tiny expandable coil of metal mesh. It is injected into the area of the artery to prevent the artery from narrowing or re-closing.
Once the stent is in place, tissue will begin to cover it like a layer of skin. Full tissue coverage will be completed within 3–12 months, depending on whether the stent is drug-eluting or not.
Metal stent for coronary arteries, uncovered
Pure metal springs do not have a special coating. They act as a scaffold to support open blood vessels after they are dilated with angioplasty.
As the artery heals, the tissue around the stent grows, holding it in place. However, sometimes excessive growth of scar tissue on the lining of the artery increases the risk of another blockage.
These intravascular devices do not require long-term use of antiplatelet drugs and are preferred for people at high risk of bleeding.
Drug coated
In these devices, the surface of a cylindrical frame is coated with a medicinal substance that is slowly released into the arterial wall. This helps the artery stay smooth and open, allowing good blood flow.
However, such stents require longer treatment with blood thinners, making them less desirable for people with bleeding problems or those who will need some kind of surgery within a year of the stent placement.
Other passive coatings
Installation of a stent in the vessels of the heart is currently carried out using the latest type of coronary devices.
This is a first-of-its-kind stent therapy designed to not only reduce the likelihood of the artery narrowing again or the need for a repeat procedure, but also to facilitate the healing process of the artery. This stent contains a drug for active healing.
The expandable tube has a coating on both the inside and outside that reduces the likelihood of blood clots, inflammation, and aids the healing process of the artery.
The surface of the design, facing the artery wall, contains a drug that is released to help stop the artery from re-blocking without worrying about swelling or an inflammatory reaction. The drug is delivered by a biovascular scaffold that degrades over time.
Innovative
A bioresorbable vascular scaffold, also known as an antibody-coated stent, is under active development. This type is different from others because it does not contain polymer and does not use medication. As a result, it helps speed up the lining of artery cells (endothelialization), promoting natural healing.
The antibody on the surface of the stent attracts circulating endothelial progenitor cells that come from human bone marrow and help accelerate the formation of healthy endothelium. This provides rapid coverage of the stent surface, helping to reduce the risk of early and late thrombosis.
Possible risks of coronary angioplasty
Although angioplasty is less invasive than bypass surgery, the procedure still carries some risks. Risks may be associated with the procedure itself and its long-term outcomes.
Early risks:
- Bleeding. There may be bleeding in the leg or arm where the vessel was accessed. Usually it just develops as a bruise, but sometimes there is serious bleeding that may require a blood transfusion or surgery.
- Heart attack. Coronary circulation disorders develop very rarely during surgery, but sometimes, due to technical reasons, a rupture or dissection of the coronary artery may develop. These complications may require emergency coronary artery bypass surgery.
- Kidney problems. The contrast agent used in angioplasty and stent placement can cause kidney damage, especially in people who already have kidney problems. If you are at higher risk, your doctor may take steps to protect your kidneys, such as limiting the amount of contrast material and increasing fluid intake to dilute the contrast.
- Ischemic stroke. During angioplasty, a stroke can occur if pieces of plaque break off as the catheter is passed through the aorta. Stroke is an extremely rare complication of coronary angioplasty. To prevent it, drugs that reduce blood clotting are prescribed.
- Heart arythmy. During the procedure, the heart may beat too fast or too slow. Such arrhythmias are usually short-lived, but sometimes a temporary pacemaker is required.
Late complications
- Repeated narrowing of the artery (restenosis). With angioplasty without stenting, the rate of restenosis is approximately 30% of cases. Stents have been developed to reduce restenosis. The use of plain metal stents reduces the risk of restenosis to 15%, and the use of drug-eluting stents reduces the risk to less than 10%.
- Stent thrombosis. Blood clots (thrombi) can block an artery, causing a heart attack. To reduce the risk of thrombosis, it is important to take aspirin, clopidogrel (Plavix), which helps reduce the risk of blood clots forming in the stent. Never stop taking these medications without talking to your doctor.
Diagnostics before stenting
Before the procedure:
- general and biochemical blood test;
- ECG;
- coronary angiography.
The patient needs to prepare for coronary angioplasty and stenting as follows:
- 4 weeks before the procedure, take a blood test;
- Talk to your doctor about taking your regular medications, especially diabetes medications or blood thinners. Diabetic medications should be stopped at least 3 days before surgery;
- 6 hours before the start of the procedure you should not smoke, eat or drink alcohol;
- It is not recommended to drink tea or milk 2 hours before the procedure.
How is cardiac stenting performed?
The stent supports the walls of the artery and is placed after the heart vessels are dilated with an inflated balloon.
How the procedure works:
- A stent mounted on a balloon is guided by a catheter through the artery to the site of the blockage.
- The balloon is inflated and the stent is expanded and secured inside the artery.
- Once the stent is in place, the balloon catheter is removed and an angiogram is performed to see how well blood is flowing through the dilated artery.
- The puncture site of the vessel is treated with antiseptics and a pressure bandage is applied. The entire process of coronary stenting of the heart vessels can last from one and a half to 3 hours.
After the procedure, the doctor will prescribe treatment with “blood thinning” drugs called anticoagulants.
Relevance of the operation
Coronary arteries are the arteries that supply the heart muscle.
There are 2 main vessels:
- Arteria coronaria dextra. This artery (blood, nutrients passing through the branches) supplies the right wall of the right ventricle, the septum, and the posterior wall. The vessel is small.
- Arteria coronaria sinistra. It supplies blood to the left parts of the myocardium, the anterior wall (almost all), most of the septum and the apical region.
Each artery has a large number of connections. Due to this, when the branches narrow, blood flows to the muscle from the pool of another vessel (in a smaller volume). This provides protection against coronary syndrome and acute heart attack. When small branches are blocked, muscle damage will be moderate. Coronary blood flow does not decrease significantly.
| Type of intervention | Price |
| Stenting of coronary arteries | 110,000 - 220,000 rub. |
However, it is important to understand that the coronary arteries play a major role in the functioning of the heart muscle. It is thanks to them that the blood supply to the heart is ensured. Blood flowing through the arteries supplies all heart cells with oxygen and essential nutrients, so that the organ functions properly. If the vessels narrow due to atherosclerosis or myocardium, the heart stops working at full capacity. Because of this, changes occur in tissues at the biochemical level. The consequence of obstruction of the coronary vessels is coronary artery disease. Ischemic disease involves damage to the myocardium.
Request a call back Get a free consultation
Rehabilitation after cardiac stenting
Each patient is given specific instructions, but in general:
- Do not lift anything heavier than 2-3 kg for the first week.
- Do not climb stairs more than 2-3 times a day and move slowly when going up and down.
- Avoid most sports or physical activities at first.
- Try not to overexert yourself during bowel movements. In case of constipation, take special medications
- Do not drive for the first 2 days.
- Do not engage in sexual activity during the first week after the procedure.
During recovery, you should walk on level ground as often as possible. This will help prevent blood clots in your legs and increase your endurance.
Basic recommendations
A stent is inserted into the heart vessels through an incision in the thigh or arm. After the procedure, the area may become infected or bleed, so it is important to keep it clean and not strained.
To care for your incision you will need:
- Wash the incision site daily with mild soap and water.
- As directed by your doctor, apply a healing antibiotic ointment to the wound.
- Every day after washing and applying ointment, apply a small bandage to the incision site.
- Do not take a bath for a week after the procedure as this may slow down the healing of the wounds.
- At first, the incision site may be swollen and bruised, but this should improve over time. If the incision site gradually becomes very swollen, hot, red, or if the temperature rises, you should consult a doctor. This may be a sign that the wound is infected.
- If bleeding begins from the incision, you should lie down and apply pressure to the wound, holding it in this position for at least 30 minutes. If the wound does not stop bleeding, you should call a doctor.
Diet
After the procedure, in the following days, it is advisable to prevent an increase in blood cholesterol levels. For this reason, you should follow a special diet.
Lifelong dietary restrictions should concern total caloric intake (toward its reduction in order to avoid obesity), as well as the consumption of animal fats, table salt and fermented milk products. The main diet after stenting corresponds to the dietary tables for high cholesterol and atherosclerosis.
Physical exercise
Moderate physical activity and exercise after cardiac stenting should become an integral part of your lifestyle.
Experts say aerobic exercise is best: regular walking or cycling, which requires little effort but works most muscles and promotes circulation. In this case, it is necessary to monitor the state of the pulse and prevent tachycardia.
A healthy lifestyle will speed up recovery:
- Drink plenty of fluids.
- Eat a healthy diet rich in vegetables, fruits, lean meats and whole grains.
- Increase your physical activity level at least 3 times a week. Once you return to normal activity, you can start with a half-hour walk every day.
Consequences after stenting of cardiac vessels and possible complications
Installing a stent in the heart vessels has some risks:
- Bleeding or hematoma where the catheter entered the groin or arm.
- Repeated narrowing of the coronary artery, called restenosis.
- Blood clots inside the stent (thrombosis).
Serious problems with stenting rarely occur:
- coronary artery damage;
- stroke;
- acute cardiovascular disease;
- heart rhythm disturbance;
- death.
Possible complications after the procedure:
- formation of a hematoma in the area of puncture of the vessel;
- bleeding after removing the catheter from the artery - in the first 12-15 hours after installation of the device;
- temporary, during the first 48 hours, disturbance of heart rhythm
- dissection of the intima (inner lining) of the vessel;
- severe renal failure.
Lethal consequences after the procedure are associated with the development of myocardial infarction. One of the main complications of stenting is restenosis – repeated narrowing of the lumen several months after coronary intervention.
This is due to the fact that after its installation, pressure develops on the vessel wall and an inflammatory reaction. In this case, blood platelets can accumulate on the inner surface of the structure, causing the formation of a blood clot, which subsequently leads to fibrosis of the intima, the inner wall of the vessel.
Heart attack after stent placement
The key factor in the possible risk of developing a heart attack after stent installation remains that the patient does not comply with doctors’ recommendations. After unauthorized cessation of taking special medications, especially in the first few months, the risk of death increases.
Temperature
If medications are poorly tolerated, signs of intoxication may appear:
- vomit;
- weakness;
- nausea;
- temperature increase.
All symptoms are corrected by prescribing other drugs and changing the patient’s behavior tactics.
Other complications after surgery
There are risks of stenting, which are associated with damage to the vascular wall, infection, improper implantation of the device, the development of a heart attack and cardiac arrest.
Possible complications
Due to the fact that stenting of the coronary arteries is an invasive method of treating ischemia, that is, it is introduced into the body tissue, the development of postoperative complications is quite possible. But thanks to modern materials and intervention techniques, the risk of complications is minimized.
Thus, intraoperative (during surgery) complications are the occurrence of life-threatening arrhythmias (ventricular fibrillation, ventricular tachycardia), incision of the coronary artery (dissection), and extensive myocardial infarction.
Early postoperative complications are acute thrombosis (sedimentation of blood clots at the site of stent installation), aneurysms of the vascular wall with the possibility of rupture, and cardiac arrhythmias.
A late complication after surgery is restenosis, the growth of the inner lining of the vessel onto the surface of the stent from the inside with the appearance of new atherosclerotic plaques and blood clots.
Prevention of complications consists of careful X-ray monitoring of stent installation, the use of the highest quality materials, as well as taking the necessary medications after surgery to treat atherosclerosis and reduce blood clots. The correct attitude of the patient also plays a significant role here, because in any field of surgery it is known that in positively minded patients the postoperative period proceeds more favorably than in persons predisposed to anxiety and restlessness. Moreover, complications develop in less than 10% of cases.
Post-op pills and other medications
After the procedure, antiplatelet drugs are prescribed to reduce the “stickiness” of platelets. Platelets are special blood cells that clump together to stop bleeding. The medicine may also prevent blood clots from forming inside the stent.
| Combination of drugs | Duration of treatment after metal stent placement | Duration of treatment after installation of a stent coated with cytostatics |
| Aspirin + Clopidogrel | 3-4 weeks of double treatment | Minimum 1 year |
| Aspirin-cardio + Plavix | 3-4 months |
The duration often depends on the blockage, the type of stent, and the individual's risk of bleeding. You should not stop taking aspirin or other medications without consulting your cardiologist because the medications not only minimize the risk of thrombosis, but also reduce the risk of stroke or heart attack.